
Ultrasound-Responsive Liposomes for Targeted Drug Delivery Combined with Focused Ultrasound

 ,
,
Abstract
:1. Introduction
2. Materials and Method
2.1. Materials
2.2. Preparation of DOX-Loaded Liposomes
2.3. Characterization of IMP301
2.4. Analysis of In Vitro Release under Ultrasound Exposure
2.5. Determination of the Ideal FUS Parameters for DOX Release
2.6. IMP301 Stability Test
2.7. In Vitro Cellular Uptake and Cytotoxicity of IMP301
2.8. Pharmacokinetics of Ultrasound-Sensitive Liposomal DOX
2.9. In Vivo DOX Release under Ultrasound Irradiation
2.10. In Vivo Anticancer Efficacy
3. Results and Discussion
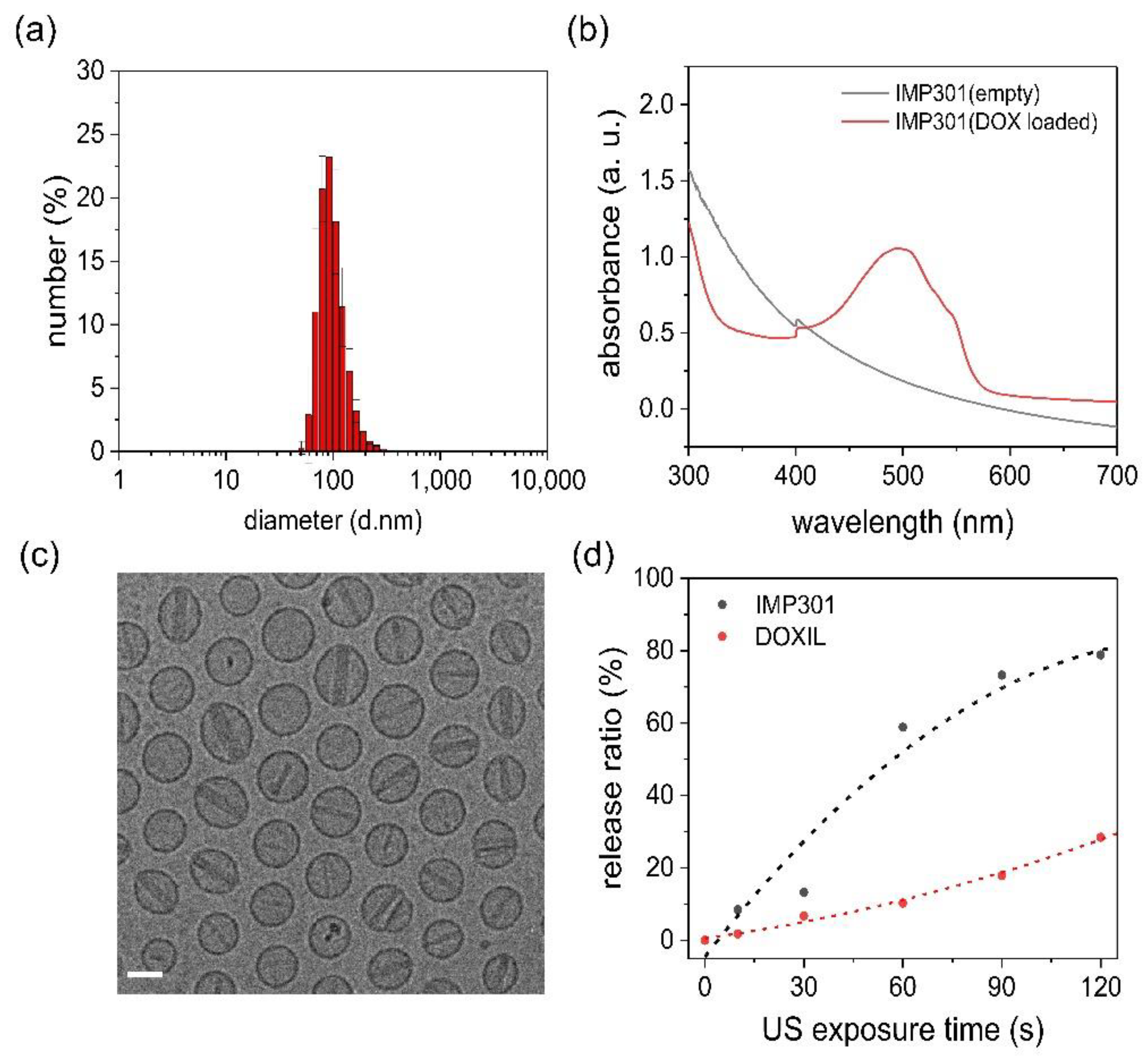
3.1. Characterization of IMP301
3.2. In Vitro Release of DOX under the FUS Exposure
3.3. In Vitro Release Depends on FUS Parameters
3.4. Long-Term Stability of IMP301
3.5. Cellular Uptake of Liposomes
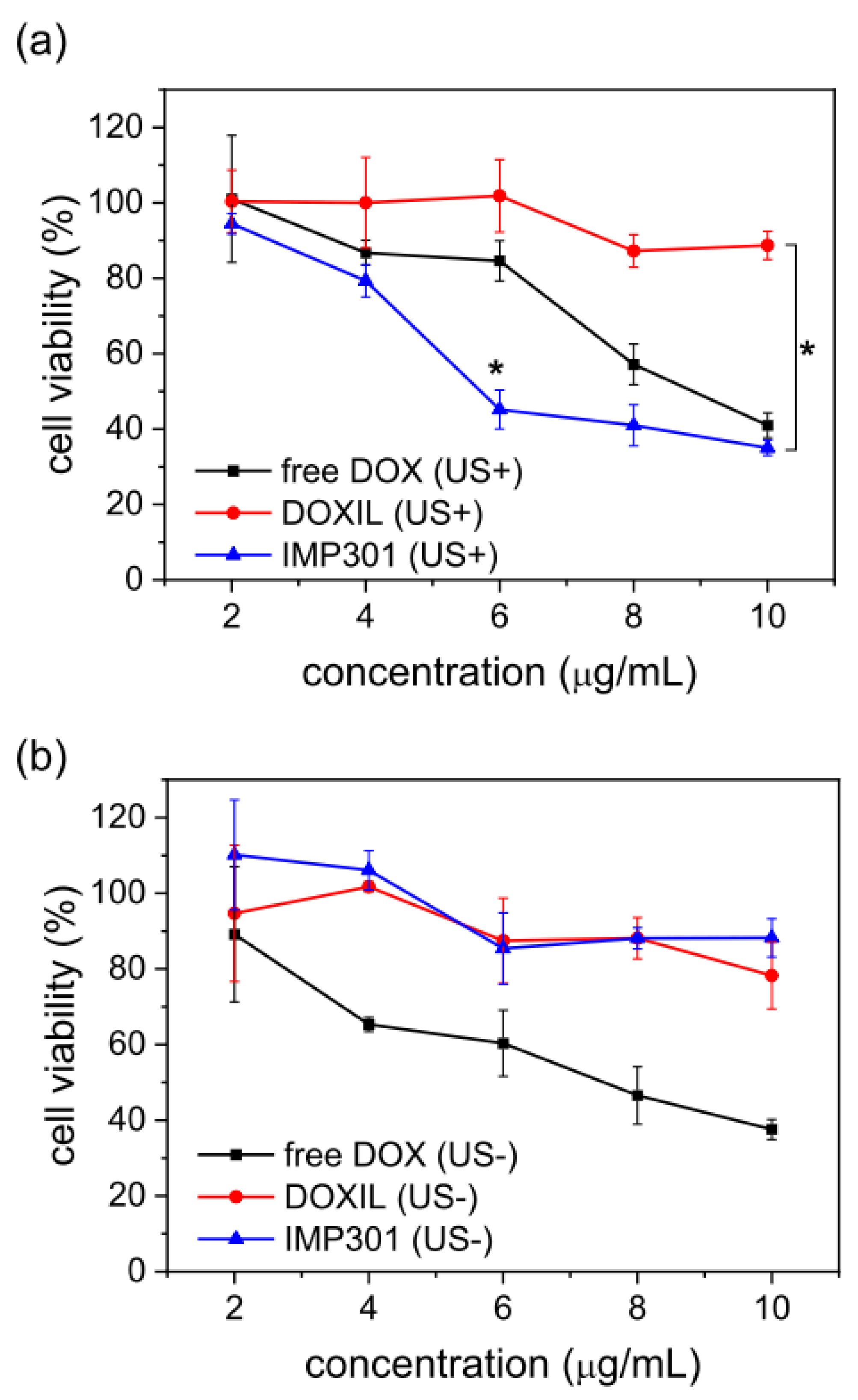
3.6. Cytotoxicity of IMP301 with Ultrasound-Triggered DOX Release
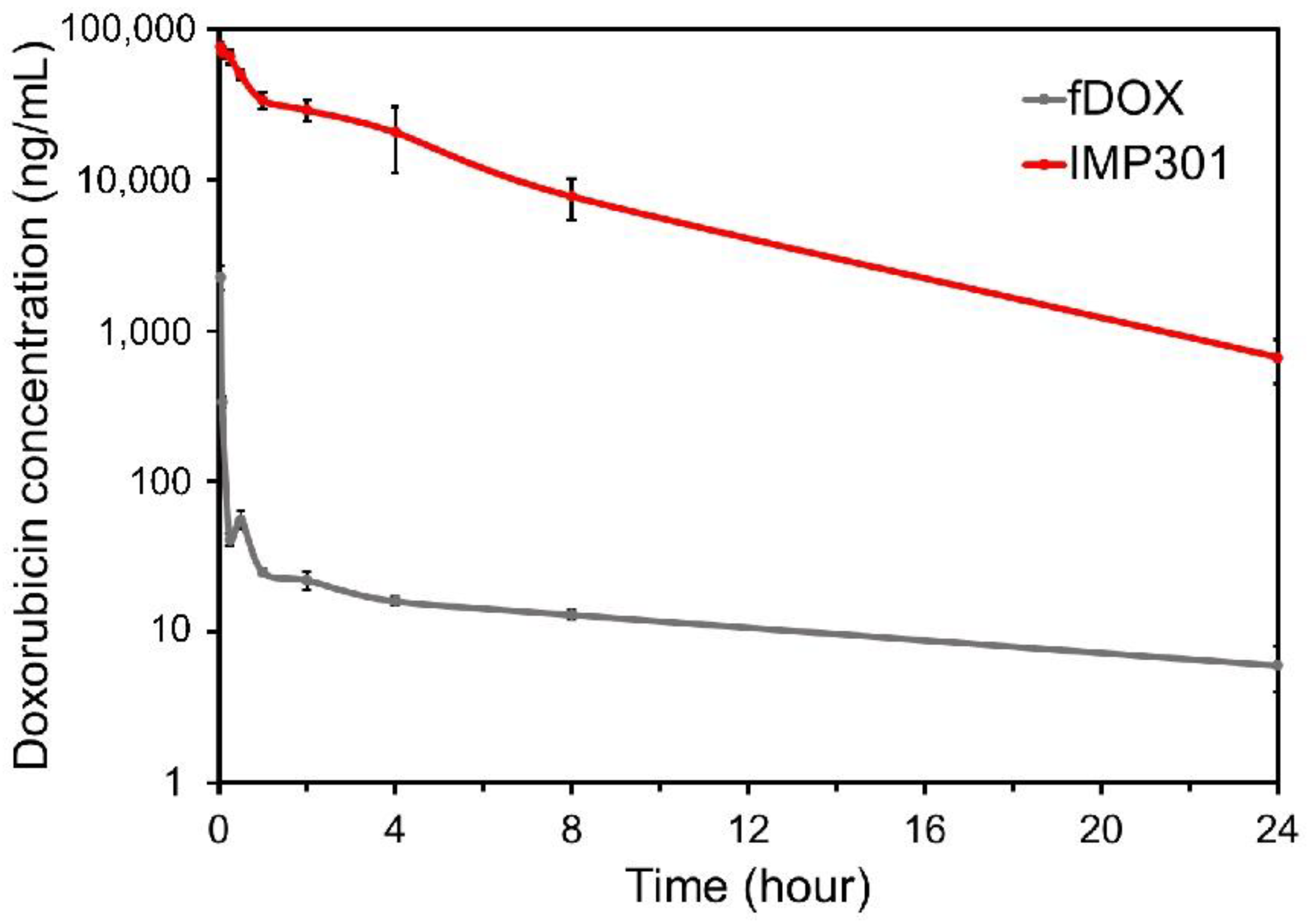
3.7. Pharmacokinetic Study
3.8. In Vivo Release Test of IMP301 at the Tumor
3.9. Therapeutic Effect of Ultrasound-Responsive Liposomes In Vivo
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Readi, M.Z.; Althubiti, M.A. Cancer Nanomedicine: A New Era of Successful Targeted Therapy. J. Nanomater. 2019, 2019, 4927312. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.L.; Bendayan, R.; Rauth, A.M.; Li, Y.; Wu, X.Y. Chemotherapy with anticancer drugs encapsulated in solid lipid nanoparticles. Adv. Drug Deliv. Rev. 2007, 59, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; del Pilar Rodriguez-Torres, M.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.-S. Nanoparticles of biodegradable polymers for new-concept chemotherapy. Expert Rev. Med Devices 2004, 1, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Nakamura, H.; Maeda, H. The EPR effect: Unique features of tumor blood vessels for drug delivery, factors involved, and limitations and augmentation of the effect. Adv. Drug Deliv. Rev. 2011, 63, 136–151. [Google Scholar] [CrossRef]
- Nakamura, Y.; Mochida, A.; Choyke, P.L.; Kobayashi, H. Nanodrug Delivery: Is the Enhanced Permeability and Retention Effect Sufficient for Curing Cancer? Bioconjug. Chem. 2016, 27, 2225–2238. [Google Scholar] [CrossRef]
- Fang, J.; Sawa, T.; Maeda, H. Factors and Mechanism of “EPR” Effect and the Enhanced Antitumor Effects of Macromolecular Drugs Including SMANCS. Adv. Exp. Med. Biol. 2003, 519, 29–49. [Google Scholar] [CrossRef]
- Huang, S.-L.; MacDonald, R.C. Acoustically active liposomes for drug encapsulation and ultrasound-triggered release. Biochim. Et Biophys. Acta 2004, 1665, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Regenold, M.; Bannigan, P.; Evans, J.C.; Waspe, A.; Temple, M.J.; Allen, C. Turning down the heat: The case for mild hyperthermia and thermosensitive liposomes. Nanomed. Nanotechnol. Biol. Med. 2022, 40, 102484. [Google Scholar] [CrossRef]
- Maruyama, M.; Tojo, H.; Toi, K.; Ienaka, Y.; Hyodo, K.; Kikuchi, H.; Ogawara, K.-I.; Higaki, K. Effect of Doxorubicin Release Rate from Polyethylene Glycol-Modified Liposome on Anti-tumor Activity in B16-BL6 Tumor-Bearing Mice. J. Pharm. Sci. 2021, 111, 293–297. [Google Scholar] [CrossRef]
- Sercombe, L.; Veerati, T.; Moheimani, F.; Wu, S.Y.; Sood, A.K.; Hua, S. Advances and Challenges of Liposome Assisted Drug Delivery. Front. Pharmacol. 2015, 6, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barenholz, Y. Liposome application: Problems and prospects. Curr. Opin. Colloid Interface Sci. 2001, 6, 66–77. [Google Scholar] [CrossRef]
- Guimarães, D.; Cavaco-Paulo, A.; Nogueira, E. Design of liposomes as drug delivery system for therapeutic applications. Int. J. Pharm. 2021, 601, 120571. [Google Scholar] [CrossRef] [PubMed]
- Akbarzadeh, A.; Rezaei-Sadabady, R.; Davaran, S.; Joo, S.W.; Zarghami, N.; Hanifehpour, Y.; Samiei, M.; Kouhi, M.; Nejati-Koshki, K. Liposome: Classification, preparation, and applications. Nanoscale Res. Lett. 2013, 8, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verpalen, I.M.; Anneveldt, K.J.; Nijholt, I.M.; Schutte, J.M.; Dijkstra, J.R.; Franx, A.; Bartels, L.W.; Moonen, C.T.; Edens, M.A.; Boomsma, M.F. Magnetic resonance-high intensity focused ultrasound (MR-HIFU) therapy of symptomatic uterine fibroids with unrestrictive treatment protocols: A systematic review and meta-analysis. Eur. J. Radiol. 2019, 120, 108700. [Google Scholar] [CrossRef]
- Malon, E.; Hwang, J.H. Emerging HIFU applications in cancer therapy. Int. J. Hyperth. 2015, 31, 302–309. [Google Scholar] [CrossRef]
- Khokhlova, T.D.; Hwang, J.H. HIFU for palliative treatment of pancreatic cancer. J. Gastrointest. Oncol. 2011, 2, 175–184. [Google Scholar] [CrossRef]
- Qiu, W.; Bouakaz, A.; Konofagou, E.E.; Zheng, H. Ultrasound for the Brain: A Review of Physical and Engineering Principles, and Clinical Applications. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 68, 6–20. [Google Scholar] [CrossRef]
- Frenkel, V. Ultrasound-Induced Cavitation Damage to External Epithelia of fish skin. Ultrasound Med. Biol. 1999, 25, 1295–1303. [Google Scholar] [CrossRef]
- Han, H.; Lee, H.; Kim, K.; Kim, H. Effect of high intensity focused ultrasound (HIFU) in conjunction with a nanomedicines-microbubble complex for enhanced drug delivery. J. Control. Release 2017, 266, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Evjen, T.J.; Nilssen, E.A.; Barnert, S.; Schubert, R.; Brandl, M.; Fossheim, S.L. Ultrasound-mediated destabilization and drug release from liposomes comprising dioleoylphosphatidylethanolamine. Eur. J. Pharm. Sci. 2011, 42, 380–386. [Google Scholar] [CrossRef] [Green Version]
- Cheng, M.; Li, F.; Han, T.; Yu, A.C.; Qin, P. Effects of ultrasound pulse parameters on cavitation properties of flowing microbubbles under physiologically relevant conditions. Ultrason. Sonochem. 2018, 52, 512–521. [Google Scholar] [CrossRef]
- Mohan, P.; Rapoport, N. Doxorubicin as a Molecular Nanotheranostic Agent: Effect of Doxorubicin Encapsulation in Micelles or Nanoemulsions on the Ultrasound-Mediated Intracellular Delivery and Nuclear Trafficking. Mol. Pharm. 2010, 7, 1959–1973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tharkar, P.; Varanasi, R.; Wong, W.S.F.; Jin, C.; Chrzanowski, W. Nano-Enhanced Drug Delivery and Therapeutic Ultrasound for Cancer Treatment and Beyond. Front. Bioeng. Biotechnol. 2019, 7, 324. [Google Scholar] [CrossRef] [Green Version]
- Mitragotri, S. Healing sound: The use of ultrasound in drug delivery and other therapeutic applications. Nat. Rev. Drug Discov. 2005, 4, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Joshi, B.; Joshi, A. 10—Ultrasound-based drug delivery systems. In Bioelectronics and Medical Devices; Pal, K., Kraatz, H.-B., Khasnobish, A., Bag, S., Banerjee, I., Kuruganti, U., Eds.; Woodhead Publishing: Sawston, UK, 2019; pp. 241–260. [Google Scholar]
- Yang, F.-Y.; Lin, Y.-S.; Kang, K.-H.; Chao, T.-K. Reversible blood–brain barrier disruption by repeated transcranial focused ultrasound allows enhanced extravasation. J. Control. Release 2011, 150, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Hynynen, K.; McDannold, N.; Sheikov, N.A.; Jolesz, F.A.; Vykhodtseva, N. Local and reversible blood–brain barrier disruption by noninvasive focused ultrasound at frequencies suitable for trans-skull sonications. NeuroImage 2005, 24, 12–20. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Month | DOX (%) | DSPC (%) | DSPC-mPEG2k (%) | Cholesterol (%) | DOPE (%) | MSPC (%) | Entrapment (%) | Size (d·nm) | PDI |
|---|---|---|---|---|---|---|---|---|---|
| 0 | 97.5 | 99.2 | 106.5 | 101.5 | 109.0 | 108.7 | 97.8 | 83.5 | 0.08 |
| 1 | 97.4 | 96.4 | 98.1 | 101.2 | 109.2 | 94.7 | 98.3 | 86.4 | 0.10 |
| 3 | 96.5 | 96.5 | 92.8 | 96.1 | 96.1 | 89.2 | 96.7 | 81.2 | 0.06 |
| 6 | 94.4 | 94.1 | 93.9 | 97.1 | 98.3 | 91.0 | 98.6 | 78.6 | 0.07 |
| 9 | 94.8 | 94.5 | 93.2 | 97.3 | 98.5 | 90.0 | 98.2 | 83.5 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-S.; Ko, M.J.; Moon, H.; Sim, W.; Cho, A.S.; Gil, G.; Kim, H.R. Ultrasound-Responsive Liposomes for Targeted Drug Delivery Combined with Focused Ultrasound. Pharmaceutics 2022, 14, 1314. https://doi.org/10.3390/pharmaceutics14071314
Kim Y-S, Ko MJ, Moon H, Sim W, Cho AS, Gil G, Kim HR. Ultrasound-Responsive Liposomes for Targeted Drug Delivery Combined with Focused Ultrasound. Pharmaceutics. 2022; 14(7):1314. https://doi.org/10.3390/pharmaceutics14071314
Chicago/Turabian StyleKim, Yoon-Seok, Min Jung Ko, Hyungwon Moon, Wonchul Sim, Ae Shin Cho, Gio Gil, and Hyun Ryoung Kim. 2022. "Ultrasound-Responsive Liposomes for Targeted Drug Delivery Combined with Focused Ultrasound" Pharmaceutics 14, no. 7: 1314. https://doi.org/10.3390/pharmaceutics14071314