
Effects of Flow Hydrodynamics and Eye Movements on Intraocular Drug Clearance

 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials and Instrumentation
2.2. Methods
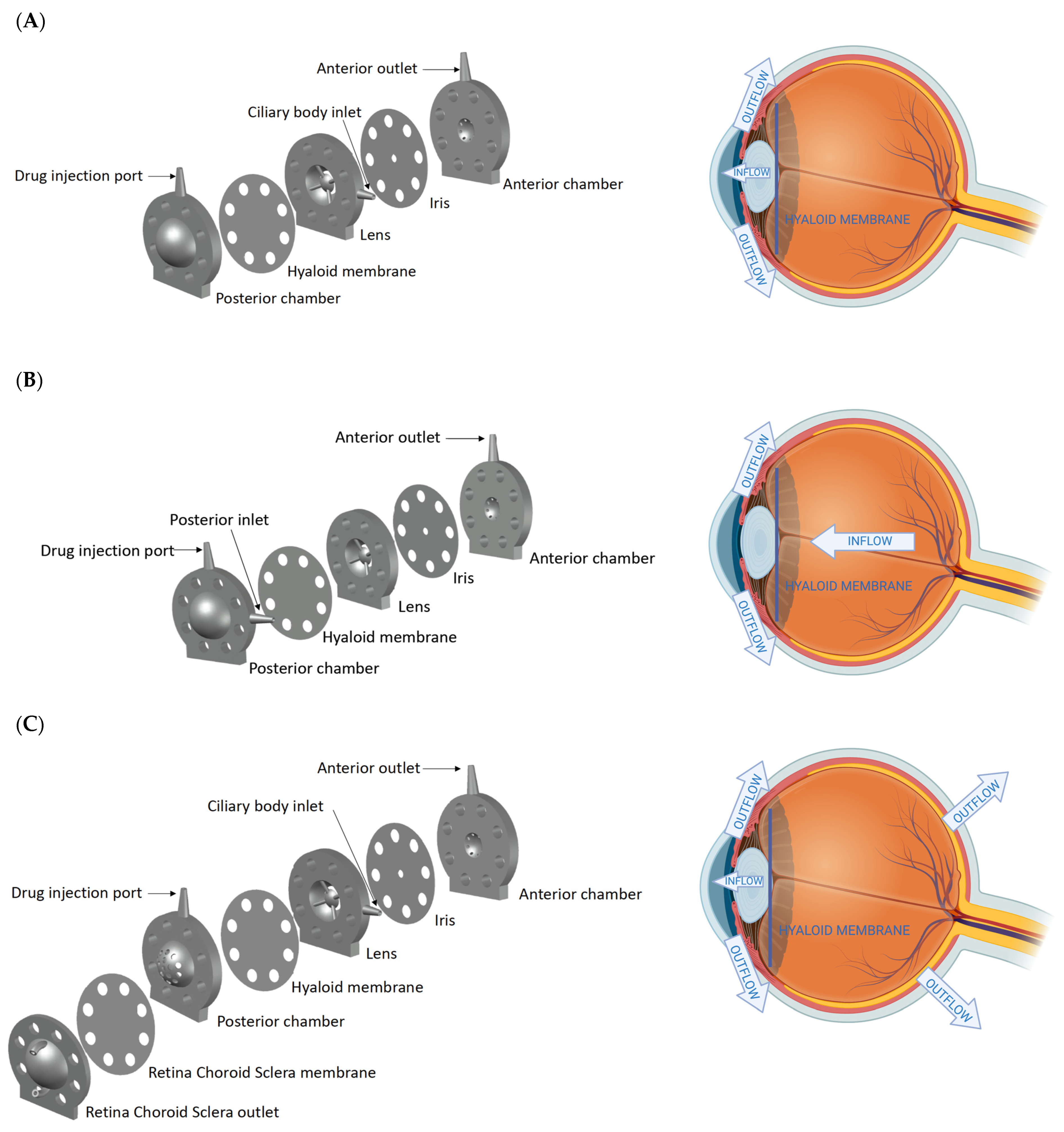
2.2.1. Design of the Models
2.2.2. Eye Movement Platform
2.2.3. Intraocular Clearance Studies
2.2.4. Drug Quantification
Bevacizumab Analysis with microBCA
Dexamethasone Analysis with HPLC
Data Analysis
3. Results
3.1. Design of the Models
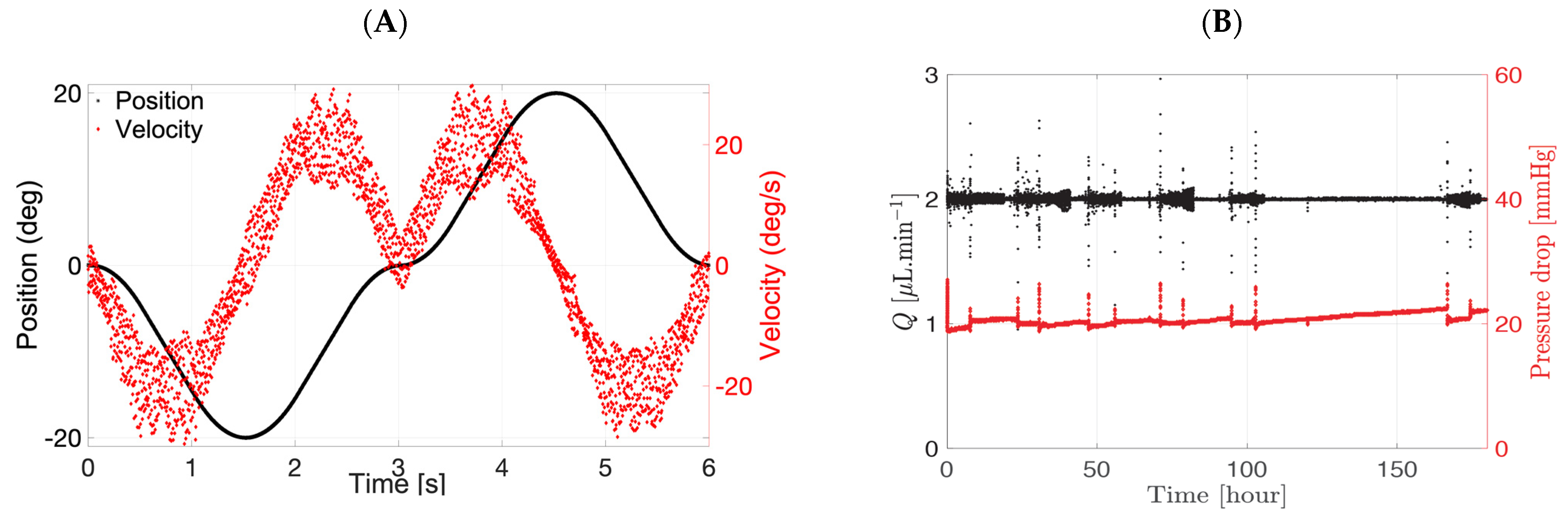
3.2. Eye Movement Platform
3.3. Intraocular Clearance Studies
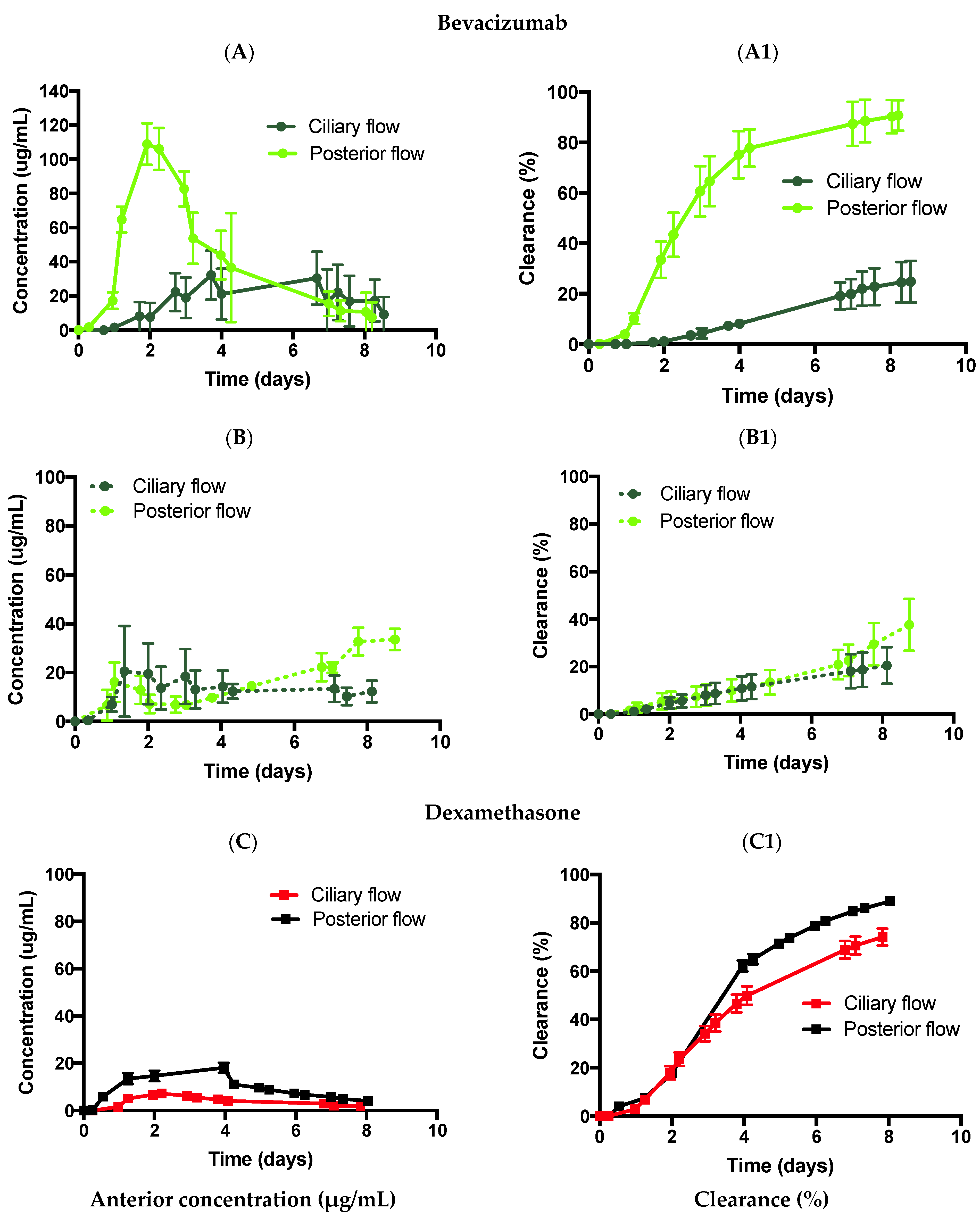
3.3.1. Effect of Diffusion
3.3.2. Flow Convection
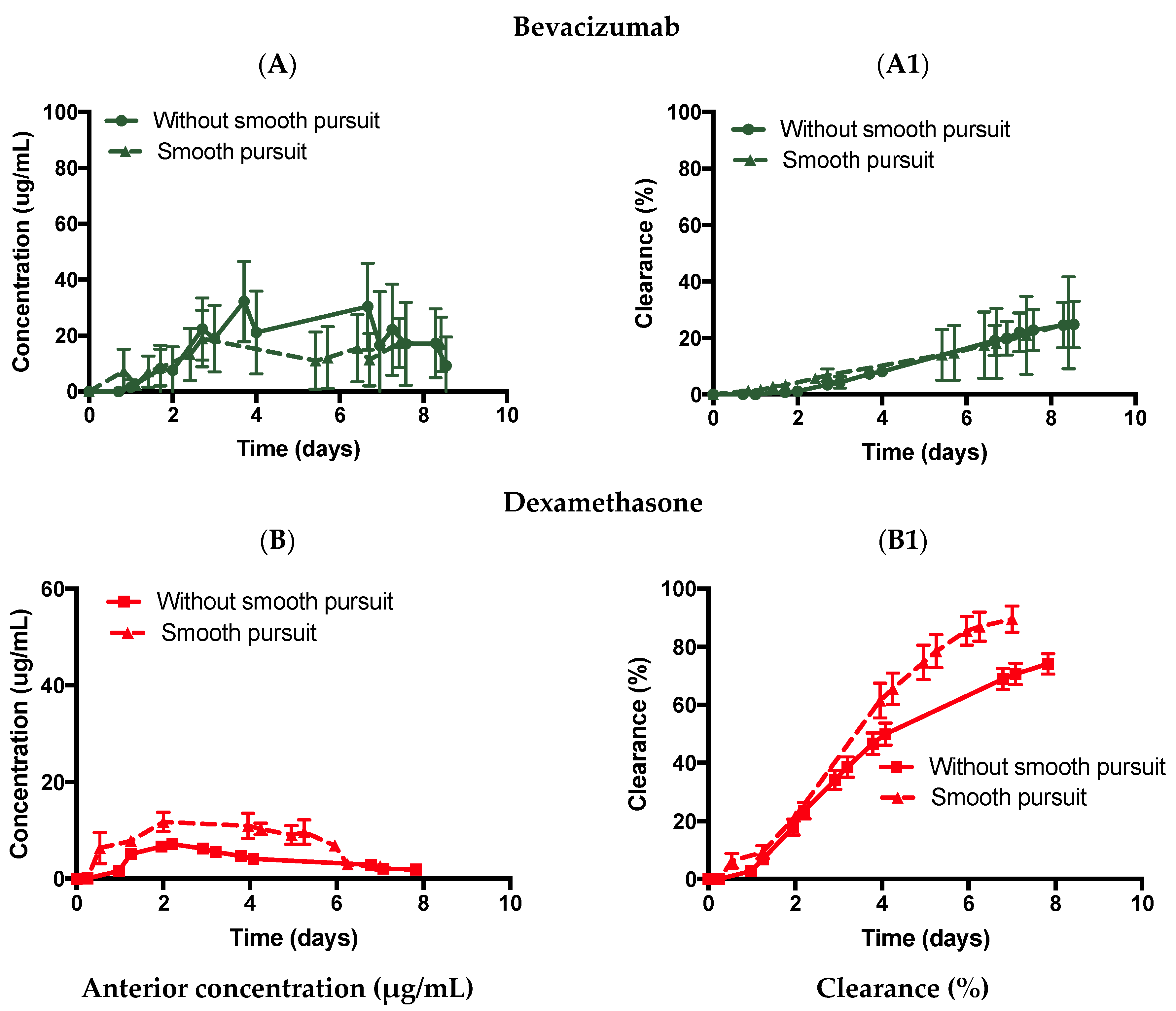
3.3.3. Introduction of Eye Movement
3.3.4. Introduction of the RCS Pathway
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Conflicts of Interest
References
- Joseph, R.R.; Venkatraman, S.S. Drug delivery to the eye: What benefits do nanocarriers offer? Nanomedicine 2017, 12, 683–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jager, R.D.; Aiello, L.P.; Patel, S.C.; Cunningham, E.T. Risks of intravitreous injection: A comprehensive review. Retina 2004, 24, 676–698. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kumar, N.; Parachuri, N.; Regillo, C.D.; Bandello, F.; Kuppermann, B.D. Retina: A unique subspecialty in the biosimilar landscape. Eye 2022, 36, 1145–1146. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Reddy, P.; Kuppermann, B.D.; Bandello, F.; Lowenstein, A. Biosimilars in ophthalmology: “is there a big change on the horizon”? Clin. Ophthalmol. 2018, 12, 2137–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Kumar, N.; Parachuri, N.; Bandello, F.; Kuppermann, B.D.; Loewenstein, A. Biosimilars for Retinal Diseases: An Update. Am. J. Ophthalmol. 2021, 224, 36–42. [Google Scholar] [CrossRef]
- Strohl, W.R. Fusion Proteins for Half-Life Extension of Biologics as a Strategy to Make Biobetters. BioDrugs 2015, 29, 215–239. [Google Scholar] [CrossRef] [Green Version]
- Awwad, S.; Henein, C.; Ibeanu, N.; Khaw, P.T.; Brocchini, S. Preclinical challenges for developing long acting intravitreal medicines. Eur. J. Pharm. Biopharm. 2020, 153, 130–149. [Google Scholar] [CrossRef]
- Laude, A.; Tan, L.E.; Wilson, C.G.; Lascaratos, G.; Elashry, M.; Aslam, T.; Patton, N.; Dhillon, B. Intravitreal therapy for neovascular age-related macular degeneration and inter-individual variations in vitreous pharmacokinetics. Prog. Retin. Eye Res. 2010, 29, 466–475. [Google Scholar] [CrossRef]
- Shankar, G.; Shores, E.; Wagner, C.; Mire-Sluis, A. Scientific and regulatory considerations on the immunogenicity of biologics. Trends Biotechnol. 2006, 24, 274–280. [Google Scholar] [CrossRef]
- Adrianto, M.F.; Annuryanti, F.; Wilson, C.G.; Sheshala, R.; Thakur, R.R.S. In vitro dissolution testing models of ocular implants for posterior segment drug delivery. Drug Deliv. Transl. Res. 2021. [Google Scholar] [CrossRef]
- Patel, S.; Müller, G.; Stracke, J.O.; Altenburger, U.; Mahler, H.-C.; Jere, D. Evaluation of protein drug stability with vitreous humor in a novel ex-vivo intraocular model. Eur. J. Pharm. Biopharm. 2015, 95, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Auel, T.; Großmann, L.; Schulig, L.; Weitschies, W.; Seidlitz, A. The EyeFlowCell: Development of a 3D-Printed Dissolution Test Setup for Intravitreal Dosage Forms. Pharmaceutics 2021, 13, 1394. [Google Scholar] [CrossRef] [PubMed]
- Awwad, S.; Lockwood, A.; Brocchini, S.; Khaw, P.T. The PK-Eye: A Novel In Vitro Ocular Flow Model for Use in Preclinical Drug Development. J. Pharm. Sci. 2015, 104, 3330–3342. [Google Scholar] [CrossRef] [Green Version]
- Thakur, S.S.; Shenoy, S.K.; Suk, J.S.; Hanes, J.S.; Rupenthal, I.D. Validation of hyaluronic acid-agar-based hydrogels as vitreous humor mimetics for in vitro drug and particle migration evaluations. Eur. J. Pharm. Biopharm. 2020, 148, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Repetto, R.; Siggers, J.H.; Stocchino, A. Mathematical model of flow in the vitreous humor induced by saccadic eye rotations: Effect of geometry. Biomech. Model Mechanobiol. 2010, 9, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Loch, C.; Nagel, S.; Guthoff, R.; Seidlitz, A.; Weitschies, W. The Vitreous Model—A new in vitro test method simulating the vitreous body Model characterization. Biomed. Eng./Biomed. Tech. 2012, 57, 281–284. [Google Scholar] [CrossRef]
- Loch, C.; Bogdahn, M.; Stein, S.; Nagel, S.; Guthoff, R.; Weitschies, W.; Seidlitz, A. Simulation of drug distribution in the vitreous body after local drug application into intact vitreous body and in progress of posterior vitreous detachment. J. Pharm Sci. 2013, 103, 517–526. [Google Scholar] [CrossRef]
- Egbu, R.; Brocchini, S.; Khaw, P.T.; Awwad, S. Antibody loaded collapsible hyaluronic acid hydrogels for intraocular delivery. Eur. J. Pharm. Biopharm. 2018, 124, 95–103. [Google Scholar] [CrossRef]
- Awwad, S.; Al-Shohani, A.; Khaw, P.T.; Brocchini, S. Comparative Study of In Situ Loaded Antibody and PEG-Fab NIPAAM Gels. Macromol. Biosci. 2018, 18, 1700255. [Google Scholar] [CrossRef] [Green Version]
- Awwad, S.; Abubakre, A.; Angkawinitwong, U.; Khaw, P.T.; Brocchini, S. In situ antibody-loaded hydrogel for intravitreal delivery. Eur. J. Pharm. Sci. 2019, 137, 104993. [Google Scholar] [CrossRef]
- Awwad, S.; Day, R.M.; Khaw, P.T.; Brocchini, S.; Fadda, H.M. Sustained release ophthalmic dexamethasone: In vitro in vivo correlations derived from the PK-Eye. Int. J. Pharm. 2017, 522, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modareszadeh, A.; Abouali, O.; Ghaffarieh, A.; Ahmadi, G. Saccade movements effect on the intravitreal drug delivery in vitreous substitutes: A numerical study. Biomech. Model Mechanobiol. 2013, 12, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Stay, M.S.; Xu, J.; Randolph, T.W.; Barocas, V.H. Computer simulation of convective and diffusive transport of controlled-release drugs in the vitreous humor. Pharm. Res. 2003, 20, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Ferroni, M.; Cereda, M.G.; Boschetti, F. A Combined Approach for the Analysis of Ocular Fluid Dynamics in the Presence of Saccadic Movements. Ann. Biomed. Eng. 2018, 46, 2091–2101. [Google Scholar] [CrossRef] [PubMed]
- Abouali, O.; Modareszadeh, A.; Ghaffariyeh, A.; Tu, J. Numerical simulation of the fluid dynamics in vitreous cavity due to saccadic eye movement. Med. Eng. Phys. 2012, 34, 681–692. [Google Scholar] [CrossRef]
- Stocchino, A.; Repetto, R.; Siggers, J.H. Mixing processes in the vitreous chamber induced by eye rotations. Phys. Med. Biol. 2010, 55, 453–467. [Google Scholar] [CrossRef] [Green Version]
- Stocchino, A.; Repetto, R.; Cafferata, C. Eye rotation induced dynamics of a Newtonian fluid within the vitreous cavity: The effect of the chamber shape. Phys. Med. Biol. 2007, 52, 2021–2034. [Google Scholar] [CrossRef]
- Silva, A.F.; Pimenta, F.; Alves, M.A.; Oliveira, M.S.N. Flow dynamics of vitreous humour during saccadic eye movements. J. Mech. Behav. Biomed. Mater. 2020, 110, 103860. [Google Scholar] [CrossRef]
- Balachandran, R.; Barocas, V. Contribution of Saccadic Motion to Intravitreal Drug Transport: Theoretical Analysis. Pharm Res. 2011, 28, 1049–1064. [Google Scholar] [CrossRef]
- Ferroni, M.; de Gaetano, F.; Cereda, M.G.; Boschetti, F. A drug delivery analysis of large molecules in ocular vitreous chamber: Dependency on saccadic movements after intravitreal injection. Med. Eng. Phys. 2020, 82, 49–57. [Google Scholar] [CrossRef]
- Maurice, D. Review: Practical issues in intravitreal drug delivery. J. Ocul. Pharmacol. 2001, 17, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Siggers, J.H.; Ethier, C.R. Fluid Mechanics of the Eye. Annu. Rev. Fluid Mech. 2012, 44, 347–372. [Google Scholar] [CrossRef]
- Hayreh, S.S. Posterior Drainage of the Intraocular Fluid from the Vitreous. Exp. Eye Res. 1966, 5, 123–144. [Google Scholar] [CrossRef]
- Haghjou, N.; Abdekhodaie, M.J.; Cheng, Y.-L. Retina-choroid-sclera permeability for ophthalmic drugs in the vitreous to blood direction: Quantitative assessment. Pharm Res. 2013, 30, 41–59. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.W.; Amico, D.J.D. Evaluation of the Retinal Toxicity and Pharmacokinetics of Dexamethasone after Intravitreal Injection. Arch Ophthalmol. 1992, 110, 259–266. [Google Scholar] [CrossRef]
- Gisladottir, S.; Loftsson, T.; Stefansson, E. Diffusion characteristics of vitreous humour and saline solution follow the Stokes Einstein equation. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 1677–1684. [Google Scholar] [CrossRef]
- Hutton-Smith, L.A.; Gaffney, E.A.; Byrne, H.M.; Maini, P.K.; Schwab, D.; Mazer, N.A. A mechanistic model of the intravitreal pharmacokinetics of large molecules and the pharmacodynamic suppression of ocular vascular endothelial growth factor levels by ranibizumab in patients with neovascular age-related macular degeneration. Mol. Pharm. 2016, 13, 2941–2950. [Google Scholar] [CrossRef]
- Penkova, A.N.; Martinez, J.C.; Humayun, M.; Tadle, A.; Galesic, A.; Calle, A.; Pratt, M.; Sadhal, S.S. Bevacizumab diffusion coefficient in vivo measurment of rabbit vitreous humor with fluorescein labeling. Investig. Ophthalmol. Vis. Sci. 2022, 60, 6103. [Google Scholar]
- Henein, C.; Awwad, S.; Ibeanu, N.; Vlatakis, S.; Brocchini, S.; Tee Khaw, P.; Bouremel, Y. Hydrodynamics of intravitreal injections into liquid vitreous substitutes. Pharmaceutics 2019, 11, 371. [Google Scholar] [CrossRef] [Green Version]
- Castro-Balado, A.; Mondelo-García, C.; González-Barcia, M.; Zarra-Ferro, I.; Otero-Espinar, F.J.; Ruibal-Morell, Á.; Aguiar, P.; Fernández-Ferreiro, A. Ocular Biodistribution Studies Using Molecular Imaging. Pharmaceutics 2019, 11, 237. [Google Scholar] [CrossRef] [Green Version]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamoorthy, M.K.; Park, J.; Augsburger, J.J.; Banerjee, R.K. Effect of retinal permeability, diffusivity, and aqueous humor hydrodynamics on pharmacokinetics of drugs in the eye. J. Ocul. Pharmacol. Ther. 2008, 24, 255–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Bungay, P.; Lutz, R. Evaluation of coupled convective–diffusive transport of drugs administered by intravitreal injection and controlled release implant. J. Control. Release 2005, 105, 279–295. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.G.; Tan, L.E. Principles of Retinal Drug Delivery from within the Vitreous. In Drug Product Development for the Back of the Eye; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2011; pp. 125–158. [Google Scholar]
- Xu, J.; Heys, J.J.; Barocas, V.H.; Randolph, T.W. Permeability and diffusion in vitreous humor: Implications for drug delivery. Pharm Res. 2000, 17, 664–669. [Google Scholar] [CrossRef]
- Brubaker, R.F. The flow of aqueous humor in the human eye. Trans. Am. Ophthalmol Soc. 1982, 80, 391–474. [Google Scholar]
- Cunha-Vaz, J.G. The blood-ocular barriers: Past, present, and future. Doc. Ophthalmol. 1997, 93, 149–157. [Google Scholar] [CrossRef]
- Pitkanen, L. Permeability of Retinal Pigment Epithelium: Effects of Permeant Molecular Weight and Lipophilicity. Investig. Ophthalmol. Vis. Sci. 2005, 46, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.W.; Song, Y.; Kim, J.H.; Shin, Y.U.; Hwang, S.J.; Hon, S. Normal Range of Eye Movement and Its Relationship to Age. Investig. Opthalmol. Vis. Sci. 2017, 58, 747. [Google Scholar]
- Rayner, K. Eye movements in reading and information processing: 20 years of research. Psychol. Bull. 1998, 124, 372–422. [Google Scholar] [CrossRef]
- Otero-Millan, J.; Troncoso, X.G.; Macknik, S.L.; Serrano-Pedraza, I.; Martinez-Conde, S. Saccades and microsaccades during visual fixation, exploration, and search: Foundations for a common saccadic generator. J. Vis. 2008, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Meyer, C.H.; Lasker, A.G.; Robinson, D.A. The upper limit of human smooth pursuit velocity. Vis. Res. 1985, 25, 561–563. [Google Scholar] [CrossRef]
- Erkelens, C.J. Coordination of smooth pursuit and saccades. Vis. Res. 2006, 46, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foulsham, T.; Kingstone, A.; Underwood, G. Turning the world around: Patterns in saccade direction vary with picture orientation. Vis. Res. 2008, 48, 1777–1790. [Google Scholar] [CrossRef] [PubMed]
- Higgins, E.; Leinenger, M.; Rayner, K. Eye movements when viewing advertisements. Front. Psychol. 2014, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsby, B.; Thell, J.; Moller, C.; Odkvist, L. The effect of stimulus predictability and age on human tracking eye movements. Acta Otolaryngol. 1988, 105, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Awwad, S.; Bouremel, Y.; Ibeanu, N.; Brocchini, S.J.; Khaw, P.T. Artificial Eye Assembly for Studying Ocular Pharmacokinetics. WO2021186191. 2020. Available online: https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2021186191&tab=PCTBIBLIO&_cid=P20-KTWYO1-27725-1 (accessed on 11 June 2022).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time (minutes) | Mobile Phase (%) | |
|---|---|---|
| A | B | |
| 0 | 80 | 20 |
| 7.5 | 80 | 20 |
| 8.5 | 50 | 50 |
| 15 | 60 | 40 |
| 17 | 80 | 20 |
| 20 | 80 | 20 |
| Model | Media | Drug | SP | Cmax (µg/mL) | t1/2 (days) | k (days−1) | R2 |
|---|---|---|---|---|---|---|---|
| Effect of diffusion | |||||||
| Ciliary inflow | PBS | Bevacizumab | No | 32.2 ± 14.4 | 20.4 | 0.0340 | 0.833 |
| Dexamethasone | 7.2 ± 0.5 | 4.7 | 0.1478 | 0.972 | |||
| SVF | Bevacizumab | 20.5 ± 18.6 | 19.2 | 0.0361 | 0.750 | ||
| Dexamethasone | 5.8 ± 0.8 | 4.9 | 0.1409 | 0.933 | |||
| Introduction of flow convection | |||||||
| Posterior inflow | PBS | Bevacizumab | No | 108.9 ± 12.1 | 2.4 | 0.2902 | 0.930 |
| SVF | 37.6 ± 10.9 | 10.8 | 0.0410 | 0.810 | |||
| PBS | Dexamethasone | 18.1 ± 2.1 | 4.8 | 0.1439 | 0.976 | ||
| Introduction of eye movement | |||||||
| Ciliary inflow | PBS | Bevacizumab | Yes | 19.0 ± 10.1 | 20.4 | 0.0340 | 0.650 |
| Dexamethasone | 11.8 ± 2.0 | 2.3 | 0.2960 | 0.955 | |||
| SVF | Bevacizumab | 20.8 ± 12.6 | 18.8 | 0.0368 | 0.940 | ||
| Dexamethasone | 21.9 ± 1.0 | 2.6 | 0.2702 | 0.907 | |||
| Introduction of RCS pathway | |||||||
| Ciliary RCS flow | PBS | Dexamethasone | No | 9.3 ± 2.1 | 1.0 | 0.7040 | 0.864 |
| Yes | 10.3 ± 2.0 | 2.1 | 0.328 | 0.962 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velentza-Almpani, A.; Ibeanu, N.; Liu, T.; Redhead, C.; Tee Khaw, P.; Brocchini, S.; Awwad, S.; Bouremel, Y. Effects of Flow Hydrodynamics and Eye Movements on Intraocular Drug Clearance. Pharmaceutics 2022, 14, 1267. https://doi.org/10.3390/pharmaceutics14061267
Velentza-Almpani A, Ibeanu N, Liu T, Redhead C, Tee Khaw P, Brocchini S, Awwad S, Bouremel Y. Effects of Flow Hydrodynamics and Eye Movements on Intraocular Drug Clearance. Pharmaceutics. 2022; 14(6):1267. https://doi.org/10.3390/pharmaceutics14061267
Chicago/Turabian StyleVelentza-Almpani, Angeliki, Nkiruka Ibeanu, Tianyang Liu, Christopher Redhead, Peng Tee Khaw, Steve Brocchini, Sahar Awwad, and Yann Bouremel. 2022. "Effects of Flow Hydrodynamics and Eye Movements on Intraocular Drug Clearance" Pharmaceutics 14, no. 6: 1267. https://doi.org/10.3390/pharmaceutics14061267