
Pharmacogenetic Interventions Improve the Clinical Outcome of Treatment-Resistant Autistic Spectrum Disorder Sufferers

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Pharmacogenetic Intervention
2.3. Clinical Assessment of Response
2.4. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baxter, A.J.; Brugha, T.S.; Erskine, H.; Scheurer, R.W.; Vos, T.; Scott, J. The epidemiology and global burden of autism spectrum disorders. Psychol. Med. 2015, 45, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Henneberry, E.; Lamy, M.; Dominick, K.C.; Erickson, C.A. Decades of Progress in the Psychopharmacology of Autism Spectrum Disorder. J. Autism Dev. Disord. 2021, 51, 4370–4394. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.T.; Eum, S.; Cook, E.H.; Bishop, J.R. Pharmacogenomics of autism spectrum disorder. Pharmacogenomics 2017, 18, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.S.; Nasir, M.; Farhat, L.C.; Kook, M.; Artukoglu, B.B.; Bloch, M.H. Meta-analysis: Pharmacologic Treatment of Restricted and Repetitive Behaviors in Autism Spectrum Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2020, 60, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.T.; Campo-Soria, C.; Bishop, J.R. Current strategies for predicting side effects from second generation antipsychotics in youth. Expert Opin. Drug Metab. Toxicol. 2021, 17, 655–664. [Google Scholar] [CrossRef]
- Mano-Sousa, B.J.; Pedrosa, A.M.; Alves, B.C.; Galduróz, J.C.F.; Belo, V.S.; Chaves, V.E.; Duarte-Almeida, J.M. Effects of Risperidone in Autistic Children and Young Adults: A Systematic Review and Meta-Analysis. Curr. Neuropharmacol. 2021, 19, 538–552. [Google Scholar] [CrossRef]
- Libowitz, M.R.; Nurmi, E.L. The Burden of Antipsychotic-Induced Weight Gain and Metabolic Syndrome in Children. Front. Psychiatry 2021, 12, 623681. [Google Scholar] [CrossRef]
- Dodsworth, T.; Kim, D.D.; Procyshyn, R.M.; Ross, C.J.; Honer, W.G.; Barr, A.M. A systematic review of the effects of CYP2D6 phenotypes on risperidone treatment in children and adolescents. Child Adolesc. Psychiatry Ment. Health 2018, 12, 37. [Google Scholar] [CrossRef] [Green Version]
- Dragioti, E.; Solmi, M.; Favaro, A.; Fusar-Poli, P.; Dazzan, P.; Thompson, T.; Stubbs, B.; Firth, J.; Fornaro, M.; Tsartsalis, D.; et al. Association of Antidepressant Use with Adverse Health Outcomes: A Systematic Umbrella Review. JAMA Psychiatry 2019, 76, 1241–1255. [Google Scholar] [CrossRef]
- Fabbri, C.; Serretti, A. Pharmacogenetics of the efficacy and side-effects of antidepressant drugs. In Genetic Influences on Response to Drug Treatment for Major Psychiatric Disorders; Rybakowski, J.K., Serretti, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Altar, C.A.; Hornberger, J.; Shewade, A.; Cruz, V.; Garrison, J.; Mrazek, D. Clinical validity of cytochrome P450 metabolism and serotonin gene variants in psychiatric pharmacotherapy. Int. Rev. Psychiatry 2013, 25, 509–533. [Google Scholar] [CrossRef]
- Zhou, Y.; Ingelman-Sundberg, M.; Lauschke, V.M. Worldwide Distribution of Cytochrome P450 Alleles: A Meta-analysis of Population-scale Sequencing Projects. Clin. Pharmacol. Ther. 2017, 102, 688–700. [Google Scholar] [CrossRef] [Green Version]
- Altar, C.A.; Carhart, J.M.; Allen, J.D.; Hall-Flavin, D.K.; Dechairo, B.M.; Winner, J.G. Clinical validity: Combinatorial pharmacogenomics predicts antidepressant responses and healthcare utilizations better than single gene phenotypes. Pharm. J. 2015, 15, 443–451. [Google Scholar] [CrossRef]
- Hall-Flavin, D.K.; Winner, J.G.; Allen, J.D.; Carhart, J.M.; Proctor, B.; Snyder, K.A.; Drews, M.S.; Eisterhold, L.L.; Geske, J.; Mrazek, D.A. Utility of integrated pharmacogenomic testing to support the treatment of major depressive disorder in a psychiatric outpatient setting. Pharm. Genom. 2013, 23, 535–548. [Google Scholar] [CrossRef] [Green Version]
- Pérez, V.; AB-GEN Collaborative Group; Salavert, A.; Espadaler, J.; Tuson, M.; Saiz-Ruiz, J.; Sáez-Navarro, C.; Bobes, J.; Baca-García, E.; Vieta, E.; et al. Efficacy of prospective pharmacogenetic testing in the treatment of major depressive disorder: Results of a randomized, double-blind clinical trial. BMC Psychiatry 2017, 17, 250. [Google Scholar] [CrossRef] [Green Version]
- Winner, J.G.; Carhart, J.M.; Altar, C.A.; Goldfarb, S.; Allen, J.D.; Lavezzari, G.; Parsons, K.K.; Marshak, A.G.; Garavaglia, S.; DeChairo, B.M. Combinatorial pharmacogenomic guidance for psychiatric medications reduces overall pharmacy costs in a 1 year prospective evaluation. Curr. Med. Res. Opin. 2015, 31, 1633–1643. [Google Scholar] [CrossRef]
- Fagerness, J.; Fonseca, E.; Hess, G.P.; Scott, R.; Gardner, K.R.; Koffler, M.; Fava, M.; Perlis, R.H.; Brennan, F.X.; Lombard, J. Pharmacogenetic-guided psychiatric intervention associated with increased adherence and cost savings. Am. J. Manag. Care 2014, 20, e146–e156. [Google Scholar]
- Arranz, M.J.; Gonzalez-Rodriguez, A.; Perez-Blanco, J.; Penadés, R.; Gutierrez, B.; Ibañez, L.; Arias, B.; Brunet, M.; Cervilla, J.; Salazar, J.; et al. A pharmacogenetic intervention for the improvement of the safety profile of antipsychotic treatments. Transl. Psychiatry 2019, 9, 177. [Google Scholar] [CrossRef]
- Yoshida, K.; Koyama, E.; Zai, C.C.; Beitchman, J.H.; Kennedy, J.L.; Lunsky, Y.; Desarkar, P.; Müller, D.J. Pharmacogenomic Studies in Intellectual Disabilities and Autism Spectrum Disorder: A Systematic Review. Can. J. Psychiatry 2021, 66, 1019–1041. [Google Scholar] [CrossRef]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Ambrosini, P.; Fisher, P.; Bird, H.; Aluwahlia, S. A children’s global assessment scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228–1231. [Google Scholar] [CrossRef]
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry 2007, 4, 28–37. [Google Scholar]
- Komaryk, A.; Elbe, D.; Burgess, L. Retrospective Review of Clozapine Use in Children and Adolescents. J. Can. Acad. Child Adolesc. Psychiatry 2021, 30, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, M.E.; de Andrés, F.; Delgado, A.; Cobaleda, J.; Peñas-Lledó, E.M.; LLerena, A. High frequency of CYP2D6 ultrarapid metabolizers in Spain: Controversy about their misclassification in worldwide population studies. Pharm. J. 2016, 16, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, B.; Arranz, M.J.; A Collier, D.; Vallès, V.; Guillamat, R.; Bertranpetit, J.; Murray, R.M.; Fañanás, L. Serotonin Transporter Gene and Risk for Bipolar Affective Disorder: An Association Study in a Spanish Population. Biol. Psychiatry 1998, 43, 843–847. [Google Scholar] [CrossRef]
- Thummler, S.; Dor, E.; David, R.; Leali, G.; Battista, M.; David, A.; Askenazy, F.; Verstuyft, C. Pharmacoresistant Severe Mental Health Disorders in Children and Adolescents: Functional Abnormalities of Cytochrome P450 2D6. Front. Psychiatry 2018, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Vanwong, N.; Ngamsamut, N.; Medhasi, S.; Puangpetch, A.; Chamnanphon, M.; Tan-Kam, T.; Hongkaew, Y.; Limsila, P.; Sukasem, C. Impact of CYP2D6 Polymorphism on Steady-State Plasma Levels of Risperidone and 9-Hydroxyrisperidone in Thai Children and Adolescents with Autism Spectrum Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 185–191. [Google Scholar] [CrossRef]
- Correia, C.T.; Almeida, J.P.; E Santos, P.; Sequeira, A.F.; Marques, C.; Miguel, T.S.; Abreu, R.L.; Oliveira, G.G.; Vicente, A.M. Pharmacogenetics of risperidone therapy in autism: Association analysis of eight candidate genes with drug efficacy and adverse drug reactions. Pharm. J. 2009, 10, 418–430. [Google Scholar] [CrossRef]
- Bishop, J.R.; Najjar, F.; Rubin, L.H.; Guter, S.J.; Owley, T.; Mosconi, M.W.; Jacob, S.; Cook, E.H. Escitalopram pharmacogenetics: CYP2C19 relationships with dosing and clinical outcomes in autism spectrum disorder. Pharmacogenet. Genomics. 2015, 25, 548–554. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.; Sharp, S.; Manzardo, A.M.; Butler, M.G. Pharmacogenetics Informed Decision Making in Adolescent Psychiatric Treatment: A Clinical Case Report. Int. J. Mol. Sci. 2015, 16, 4416–4428. [Google Scholar] [CrossRef] [Green Version]
- Shindler, A.E.; Hill-Yardin, E.L.; Petrovski, S.; Bishop, N.; Franks, A.E. Towards Identifying Genetic Biomarkers for Gastrointestinal Dysfunction in Autism. J. Autism Dev. Disord. 2019, 50, 76–86. [Google Scholar] [CrossRef]
- Porcelli, S.; Fabbri, C.; Serretti, A. Meta-analysis of serotonin transporter gene promoter polymorphism (5-HTTLPR) association with antidepressant efficacy. Eur. Neuropsychopharmacol. 2012, 22, 239–258. [Google Scholar] [CrossRef]
- Owley, T.; Brune, C.W.; Salt, J.; Walton, L.; Guter, S.; Ayuyao, N.; Gibbons, R.D.; Leventhal, B.L.; Cook, E.H. A pharmacogenetic study of escitalopram in autism spectrum disorders. Autism Res. 2009, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Clinical and Demographic Data | ||
| Total N = 104 | ||
| Treatment-resistant cohort | N | 42 |
| age | 18·79 ± 8.3 SD 3 | |
| Gender | 74% male 4 | |
| Basal CGI | 6 ± 0.99 | |
| Basal CGAS | 30.02 ± 13.28 | |
| Control | N | 62 |
| age | 13.83 ± 3.8 | |
| Gender | 92% male | |
| Basal CGI | 4.33 ± 0.80 | |
| Basal CGAS | 44.32 ± 9 | |
| Medication | ||
| Treatment resistant | Control | |
| Antipsychotics 1 | 28 (67%) | 29 (32%) |
| Antidepressants 2 | 20 (48%) | 10 (11%) |
| Anxiolytics, anticonvulsants and others | 21 (26%) | 50 (56%) |
| No current medication | 3 (7%) | 0 |
| Gene | Variants Studied | |
|---|---|---|
| CYP1A2 | rs762551 (*1F) | A > C |
| CYP2C19 | rs4244285 (*2) | G > A |
| rs12248560 (*17) | C > T | |
| CYP2D6 | rs35742686 (*3) | delA |
| rs3892097 (*4) | G > A | |
| rs5030655 (*6) | delT | |
| rs5030656 (*9) | delAAG | |
| rs1065852 (*10) | C > T | |
| rs28371706 (*17) | C > T | |
| rs28371725 (*41) | G > A | |
| Gene deletion (*5) | - | |
| Gene duplication (*XN) | - | |
| SLC6A4 | LPR | L/S |
| rs25331 | A > G | |
| STin2 | 12/10/9 | |
| Drug | Type | CYP Enzymes | Targets |
|---|---|---|---|
| Amitriptiline | TCA | CYP2C19, CYP2D6 | 5HTT, 5-HT2A |
| Aripiprazole | SGA | CYP2D6 | |
| Atomoxetine | NRI | CYP2D6 | |
| Citalopram | SSRI | CYP2C19 | 5-HTT |
| Clomipramine | TCA | CYP2C19, CYP2D6 | 5-HTT, 5-HT2A |
| Clozapine | SGA | CYP1A2, CYP2C19 | |
| Desvenlafaxine | SNRI | 5-HTT | |
| Duloxetine | SNRI | CYP2D6 & CYP1A2 | 5-HTT |
| Escitalopram | SSRI | CYP2C19, | 5-HTT |
| Fluoxetine | SSRI | CYP2D6 | 5-HTT |
| Fluvoxamine | SSRI | CYP2D6 | 5-HTT |
| Haloperidol | FGA | CYP2D6 | |
| Imipramine | TCA | CYP2C19, CYP2D6 | 5-HTT |
| Maprotiline | TCA | CYP2D6 | |
| Mirtazapine | TCA | CYP2D6, CYP1A2 | 5-HT2A |
| Nortriptyline | TCA | CYP2D6 | 5-HTT, 5-HT2A |
| Olanzapine | SGA | CYP1A2 | |
| Paroxetine | SSRI | CYP2D6 | 5-HTT |
| Risperidone | SGA | CYP2D6 | |
| Sertraline | SSRI | CYP2C19 | 5-HTT |
| Venlafaxine | SNRI | CYP2D6 | 5-HTT |
| Vortioxetine | SMS | CYP2D6 | 5-HTT |
| Gene | CYP1A2 | CYP2C19 | CYP2D6 |
| Phenotype | |||
| Normal metaboliser | 56% | 34% | 81% |
| Intermediate metaboliser | - | 32% | 5% |
| Poor metaboliser | - | - | 7% |
| Rapid or ultra-rapid metaboliser | 44% | 34% | 7% |
| Gene | SLC6A4 | ||
| Phenotype | |||
| Normal expression or activity | 20% | ||
| Intermediate expression or activity | 51% | ||
| Reduced expression or activity | 29% | ||
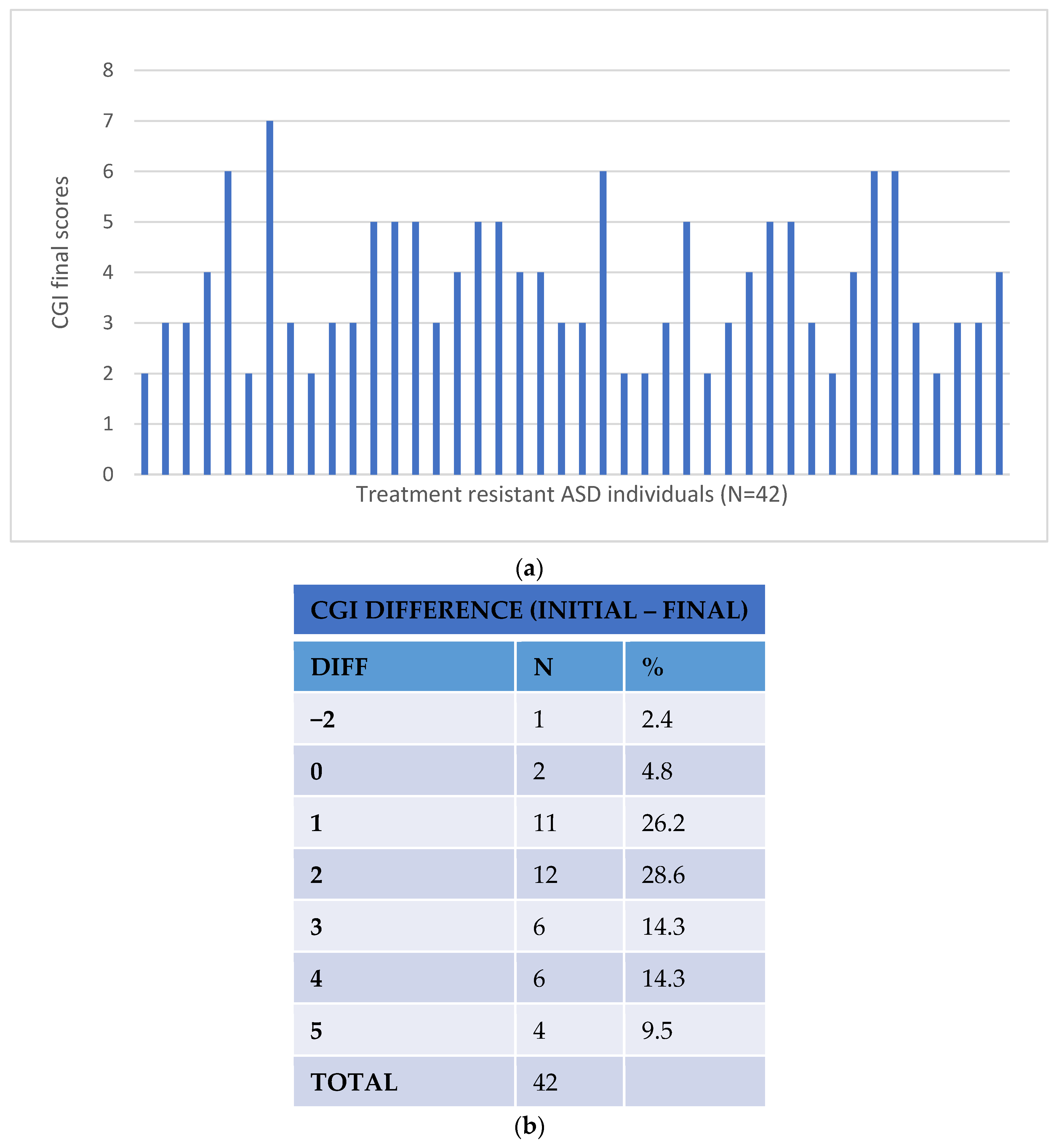
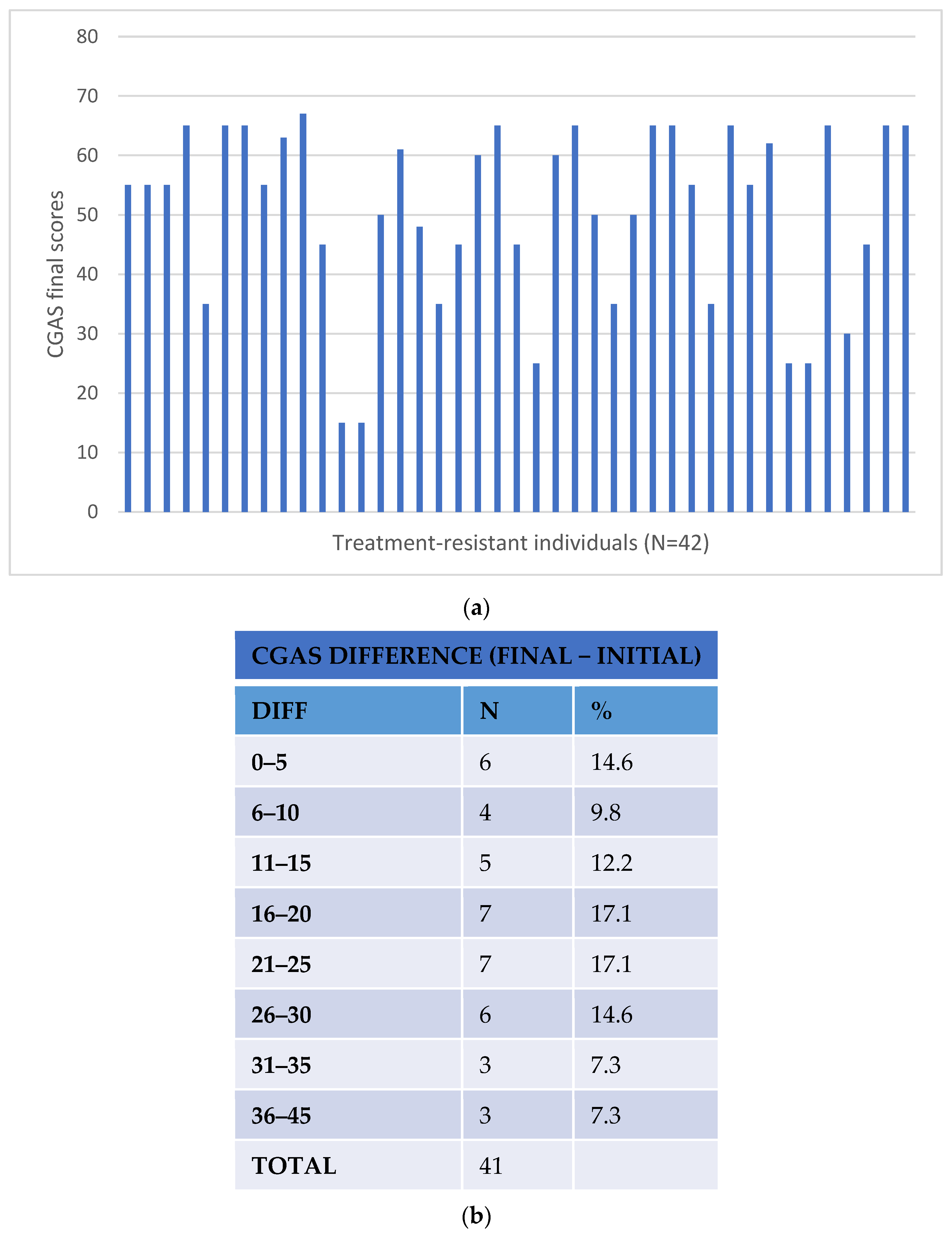
| Treatment-Resistant ASD Subjects (N = 42) (with Pharmacogenetic Intervention) | |
| Improvement in CGI scores (basal–final scores) | 2.26 ± 1.55 |
| Improvement in CGA scores (final–basal scores) | 20.29 ± 11.85 |
| Control subjects (N = 62) | |
| Improvement in CGI scores (basal–final scores) | −0.87 ± 9.44 |
| Improvement in CGA scores (final–basal scores) | 6.59 ± 7.76 |
| Non-Responders (N = 21) (no improvement in CGI or CGA scores) | |
| Improvement in CGI scores (basal–final scores) | 0.10 ± 0.63 |
| Improvement in CGA scores (final–basal scores) | 0.48 ± 2.18 |
| Responders (N = 41) (Improvement in CGI and CGA scores) | |
| Improvement in CGI scores (basal-final scores) | 1.54 ± 0.588 |
| Improvement in CGA scores (final-basal scores) | 11.74 ± 7.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arranz, M.J.; Salazar, J.; Bote, V.; Artigas-Baleri, A.; Serra-LLovich, A.; Triviño, E.; Roige, J.; Lombardia, C.; Cancino, M.; Hernandez, M.; et al. Pharmacogenetic Interventions Improve the Clinical Outcome of Treatment-Resistant Autistic Spectrum Disorder Sufferers. Pharmaceutics 2022, 14, 999. https://doi.org/10.3390/pharmaceutics14050999
Arranz MJ, Salazar J, Bote V, Artigas-Baleri A, Serra-LLovich A, Triviño E, Roige J, Lombardia C, Cancino M, Hernandez M, et al. Pharmacogenetic Interventions Improve the Clinical Outcome of Treatment-Resistant Autistic Spectrum Disorder Sufferers. Pharmaceutics. 2022; 14(5):999. https://doi.org/10.3390/pharmaceutics14050999
Chicago/Turabian StyleArranz, Maria J., Juliana Salazar, Valentin Bote, Alicia Artigas-Baleri, Alexandre Serra-LLovich, Emma Triviño, Jordi Roige, Carlos Lombardia, Martha Cancino, Marta Hernandez, and et al. 2022. "Pharmacogenetic Interventions Improve the Clinical Outcome of Treatment-Resistant Autistic Spectrum Disorder Sufferers" Pharmaceutics 14, no. 5: 999. https://doi.org/10.3390/pharmaceutics14050999