
Pharmacokinetics of Haloperidol in Critically Ill Patients: Is There an Association with Inflammation?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Data Analysis
2.4. Model Simulation
3. Results
3.1. Study Population
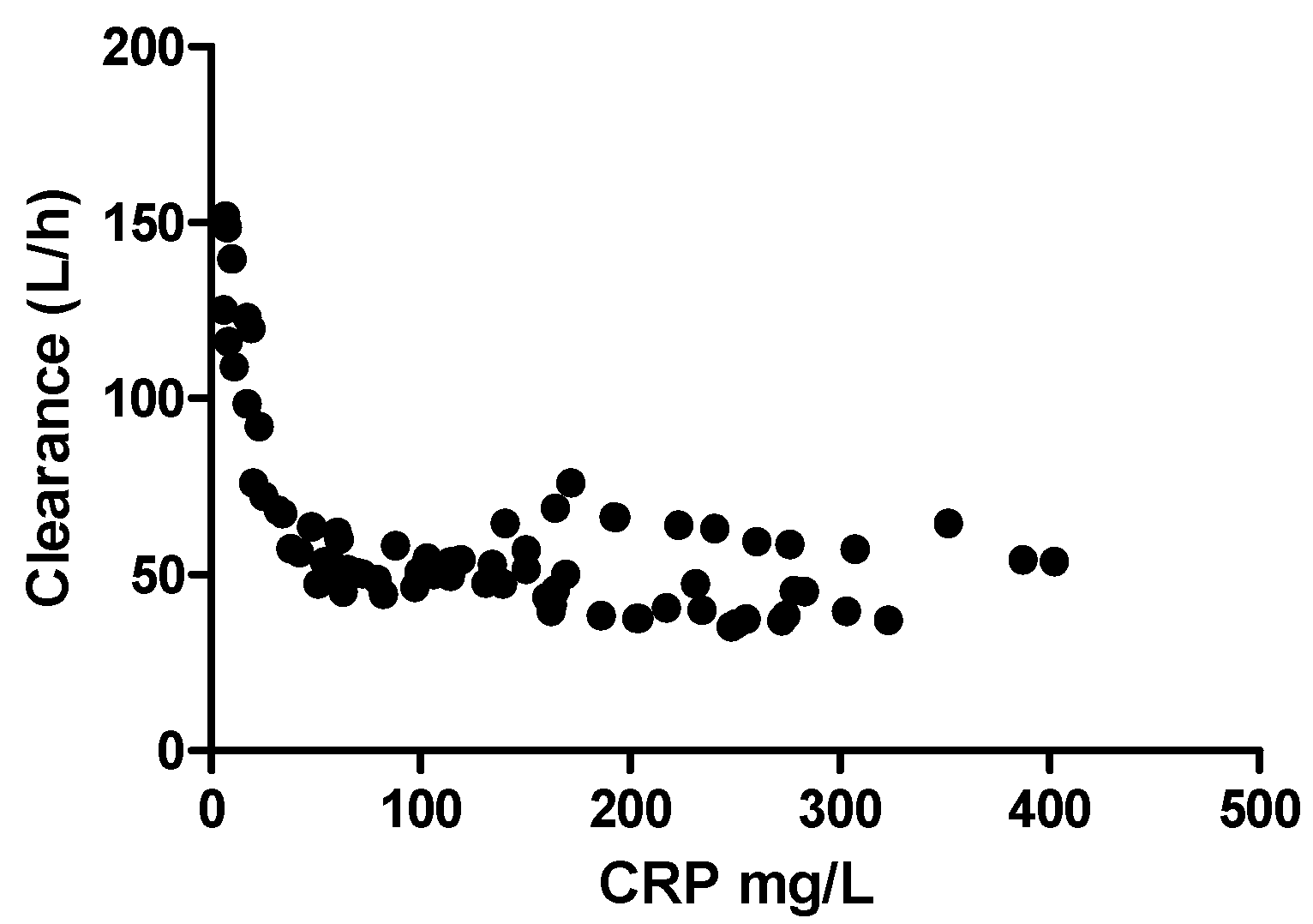
3.2. Structural Model
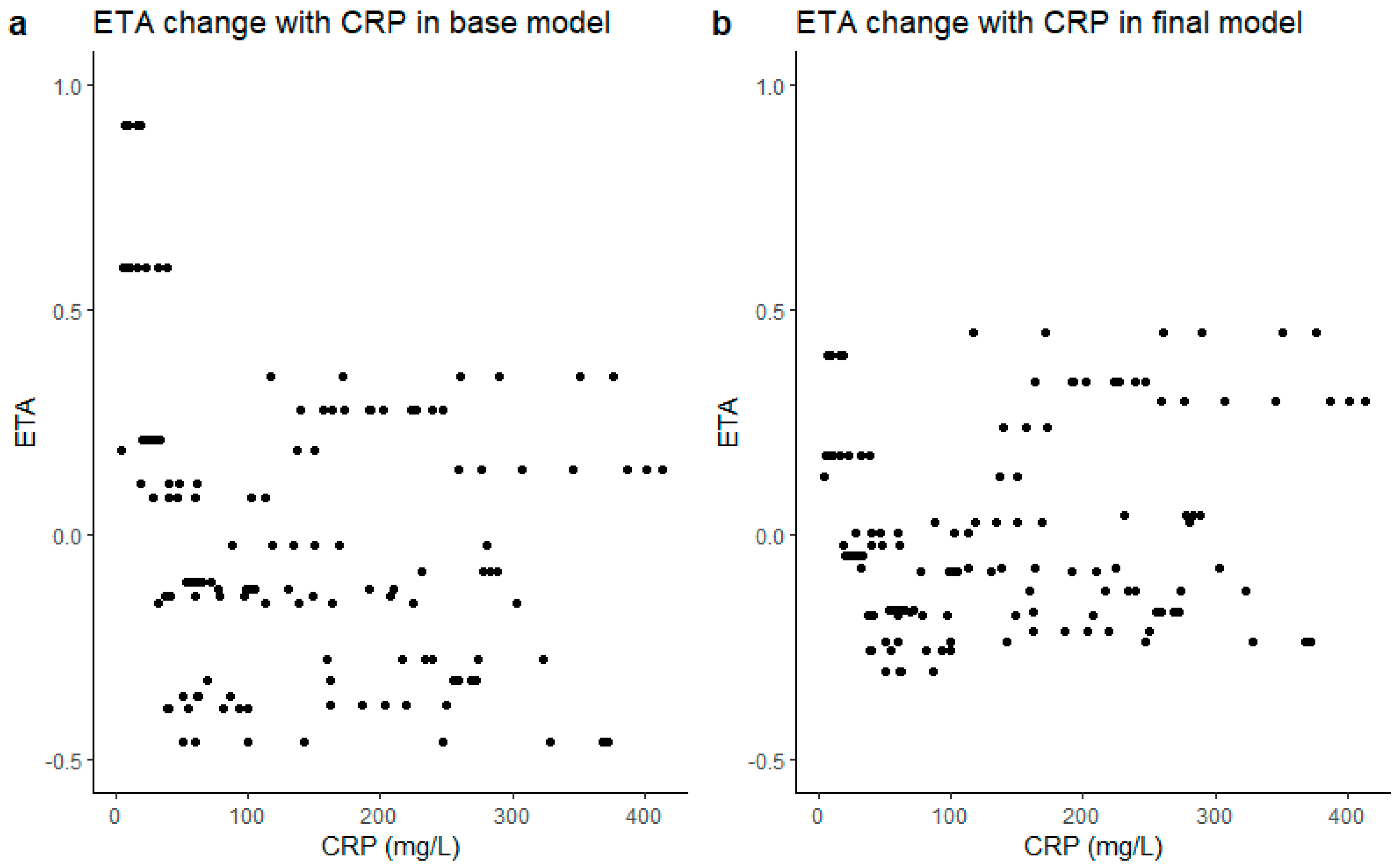
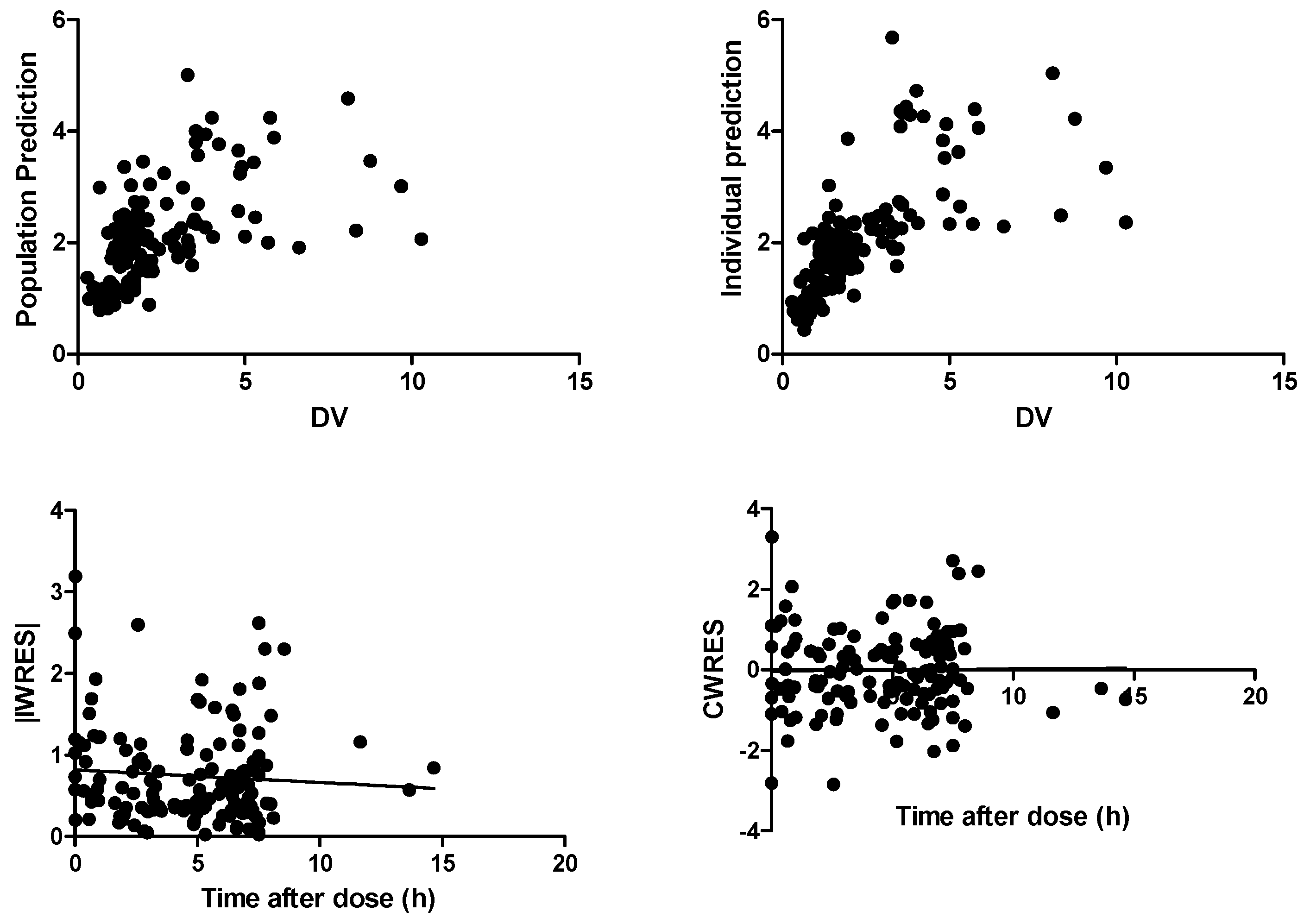
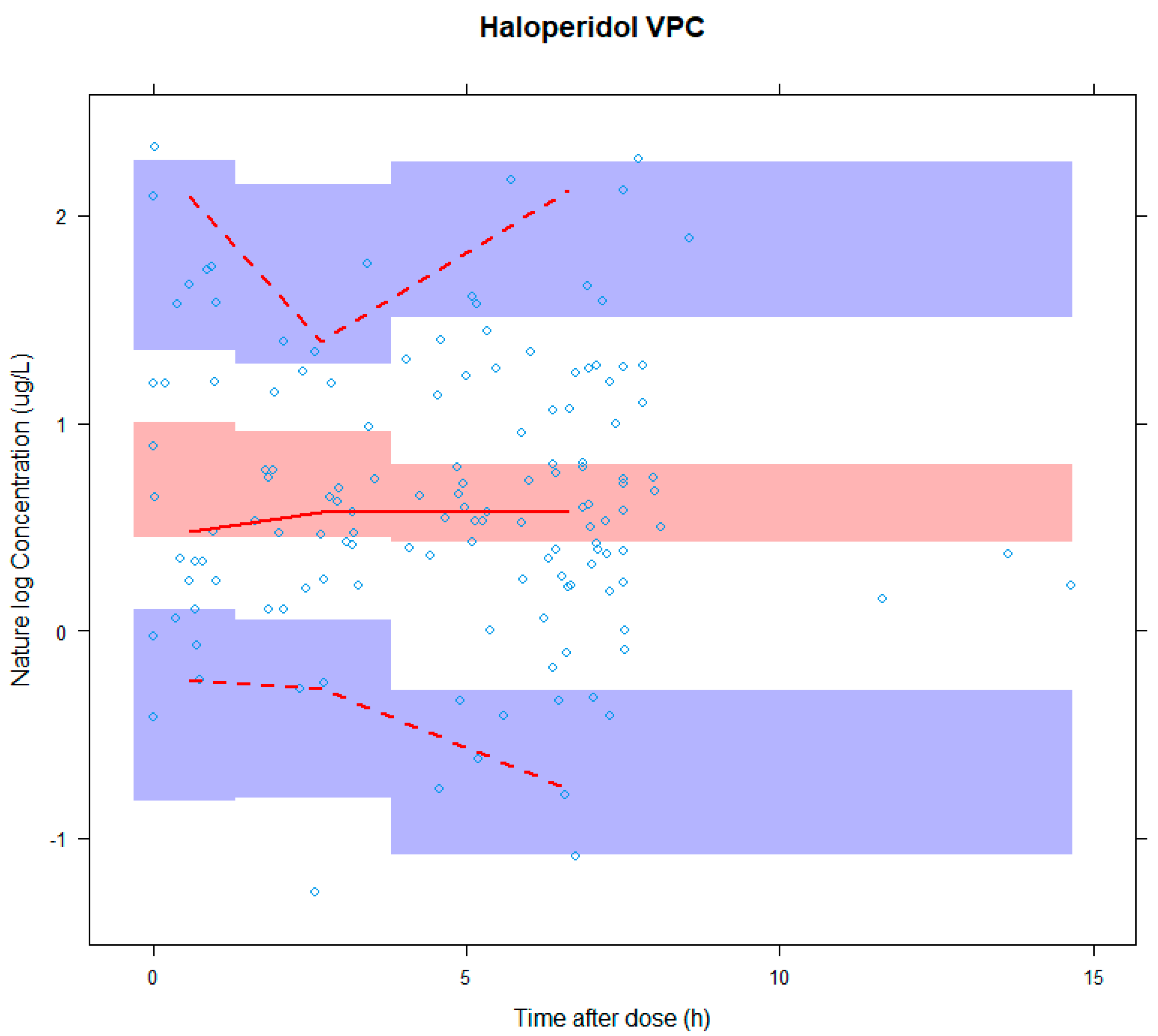
3.3. Model Evaluation
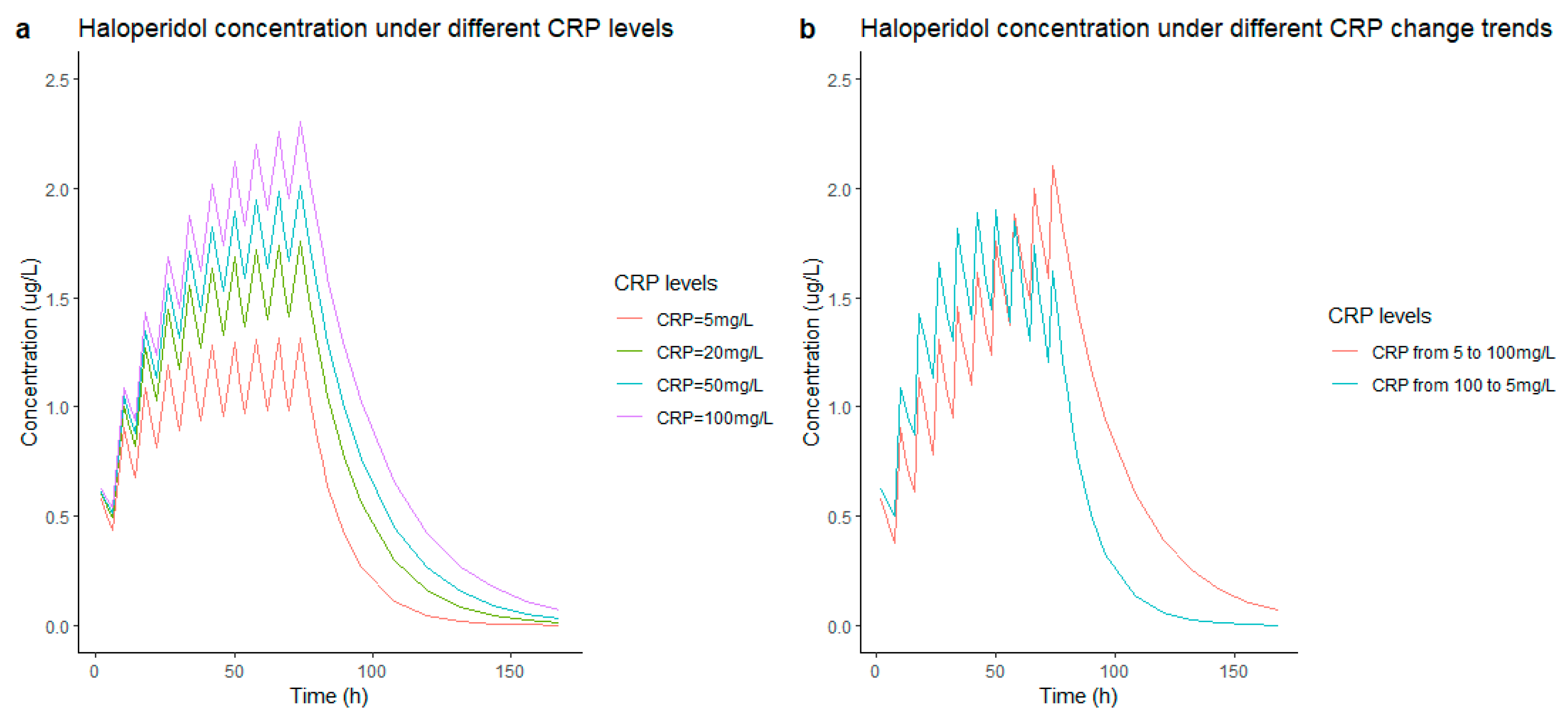
3.4. Simulations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kotfis, K.; Marra, A.; Ely, E.W. ICU delirium—A diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol. Intensive Ther. 2018, 50, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Adamis, D.; Treloar, A.; Martin, F.C.; Macdonald, A.J. A brief review of the history of delirium as a mental disorder. Hist. Psychiatry 2007, 18, 459–469. [Google Scholar] [CrossRef]
- Jayaswal, A.K.; Sampath, H.; Soohinda, G.; Dutta, S. Delirium in medical intensive care units: Incidence, subtypes, risk factors, and outcome. Indian J. Psychiatry 2019, 61, 352. [Google Scholar]
- Tilouche, N.; Hassen, M.F.; Ali, H.B.S.; Jaoued, O.; Gharbi, R.; El Atrous, S.S. Delirium in the intensive care unit: Incidence, risk factors, and impact on outcome. Indian J. Crit. Care Med. Peer-Rev. Off. Publ. Indian Soc. Crit. Care Med. 2018, 22, 144. [Google Scholar] [CrossRef]
- Herling, S.F.; Greve, I.E.; Vasilevskis, E.E.; Egerod, I.; Bekker Mortensen, C.; Møller, A.M.; Svenningsen, H.; Thomsen, T. Interventions for preventing intensive care unit delirium in adults. Cochrane Database Syst. Rev. 2018, 11, CD009783. [Google Scholar] [CrossRef]
- Reznik, M.E.; Slooter, A.J.C. Delirium Management in the ICU. Curr. Treat. Options Neurol. 2019, 21, 59. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [Green Version]
- Smit, L.; Dijkstra-Kersten, S.M.A.; Zaal, I.J.; van der Jagt, M.; Slooter, A.J.C. Haloperidol, clonidine and resolution of delirium in critically ill patients: A prospective cohort study. Intensive Care Med. 2021, 47, 316–324. [Google Scholar] [CrossRef]
- van den Boogaard, M.; Slooter, A.J.C.; Brüggemann, R.J.M.; Schoonhoven, L.; Beishuizen, A.; Vermeijden, J.W.; Pretorius, D.; de Koning, J.; Simons, K.S.; Dennesen, P.J.W.; et al. Effect of Haloperidol on Survival Among Critically Ill Adults With a High Risk of Delirium: The REDUCE Randomized Clinical Trial. JAMA 2018, 319, 680–690. [Google Scholar] [CrossRef]
- Girard, T.D.; Exline, M.C.; Carson, S.S.; Hough, C.L.; Rock, P.; Gong, M.N.; Douglas, I.S.; Malhotra, A.; Owens, R.L.; Feinstein, D.J.; et al. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N. Engl. J. Med. 2018, 379, 2506–2516. [Google Scholar] [CrossRef] [PubMed]
- Khan, B.A.; Perkins, A.J.; Campbell, N.L.; Gao, S.; Farber, M.O.; Wang, S.; Khan, S.H.; Zarzaur, B.L.; Boustani, M.A. Pharmacological Management of Delirium in the Intensive Care Unit: A Randomized Pragmatic Clinical Trial. J. Am. Geriatr. Soc. 2019, 67, 1057–1065. [Google Scholar] [CrossRef]
- Smith, B.S.; Yogaratnam, D.; Levasseur-Franklin, K.E.; Forni, A.; Fong, J. Introduction to drug pharmacokinetics in the critically ill patient. Chest 2012, 141, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient--concepts appraised by the example of antimicrobial agents. Adv. Drug Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.H.; Mabasa, V.H.; Loh, G.W.; Ensom, M.H. Haloperidol dosing strategies in the treatment of delirium in the critically ill. Neurocrit. Care 2012, 16, 170–183. [Google Scholar] [CrossRef]
- Franken, L.G.; de Winter, B.C.; van Esch, H.J.; van Zuylen, L.; Baar, F.P.; Tibboel, D.; Mathôt, R.A.; van Gelder, T.; Koch, B.C. Pharmacokinetic considerations and recommendations in palliative care, with focus on morphine, midazolam and haloperidol. Expert Opin. Drug Metab. Toxicol. 2016, 12, 669–680. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.F.; Paalzow, L.K.; Bondesson, U.; Ekblom, B.; Eriksson, K.; Eriksson, S.O.; Lindberg, A.; Lindström, L. Pharmacokinetics of haloperidol in psychotic patients. Psychopharmacology 1987, 91, 410–414. [Google Scholar] [CrossRef]
- Prommer, E. Role of haloperidol in palliative medicine: An update. Am. J. Hosp. Palliat. Care 2012, 29, 295–301. [Google Scholar] [CrossRef]
- Blaschke, T.F. Protein binding and kinetics of drugs in liver diseases. Clin. Pharm. 1977, 2, 32–44. [Google Scholar] [CrossRef] [PubMed]
- Sychev, D.A.; Zastrozhin, M.S.; Miroshnichenko, I.I.; Baymeeva, N.V.; Smirnov, V.V.; Grishina, E.A.; Ryzhikova, K.A.; Mirzaev, K.B.; Markov, D.D.; Skryabin, V.Y.; et al. Genotyping and phenotyping of CYP2D6 and CYP3A isoenzymes in patients with alcohol use disorder: Correlation with haloperidol plasma concentration. Drug Metab. Pers. Ther. 2017, 32, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Sychev, D.A.; Zastrozhin, M.S.; Smirnov, V.V.; Grishina, E.A.; Savchenko, L.M.; Bryun, E.A. The correlation between CYP2D6 isoenzyme activity and haloperidol efficacy and safety profile in patients with alcohol addiction during the exacerbation of the addiction. Pharmgenomics Pers. Med. 2016, 9, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Zastrozhin, M.S.; Smirnov, V.V.; Sychev, D.A.; Savchenko, L.M.; Bryun, E.A.; Matis, O.A. CYP3A4 activity and haloperidol effects in alcohol addicts. Int. J. Risk Saf. Med. 2015, 27 (Suppl. S1), S23–S24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Someya, T.; Shibasaki, M.; Noguchi, T.; Takahashi, S.; Inaba, T. Haloperidol metabolism in psychiatric patients: Importance of glucuronidation and carbonyl reduction. J. Clin. Psychopharmacol. 1992, 12, 169–174. [Google Scholar] [CrossRef]
- Kato, Y.; Nakajima, M.; Oda, S.; Fukami, T.; Yokoi, T. Human UDP-glucuronosyltransferase isoforms involved in haloperidol glucuronidation and quantitative estimation of their contribution. Drug Metab. Dispos. 2012, 40, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Chang, W.H.; Lam, Y.W.; Jann, M.W.; Chen, H. Pharmacokinetics of haloperidol and reduced haloperidol in Chinese schizophrenic patients after intravenous and oral administration of haloperidol. Psychopharmacology 1992, 106, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Forsman, A.; Ohman, R. Pharmacokinetic studies on haloperidol in man. Curr. Ther. Res. Clin. Exp. 1976, 20, 319–336. [Google Scholar]
- Holley, F.O.; Magliozzi, J.R.; Stanski, D.R.; Lombrozo, L.; Hollister, L.E. Haloperidol kinetics after oral and intravenous doses. Clin. Pharmacol. Ther. 1983, 33, 477–484. [Google Scholar] [CrossRef]
- Magliozzi, J.R.; Hollister, L.E. Elimination half-life and bioavailability of haloperidol in schizophrenic patients. J. Clin. Psychiatry 1985, 46, 20–21. [Google Scholar]
- Franken, L.G.; Mathot, R.A.A.; Masman, A.D.; Baar, F.P.M.; Tibboel, D.; van Gelder, T.; Koch, B.C.P.; de Winter, B.C.M. Population pharmacokinetics of haloperidol in terminally ill adult patients. Eur. J. Clin. Pharmacol. 2017, 73, 1271–1277. [Google Scholar] [CrossRef]
- Yukawa, E.; Hokazono, T.; Yukawa, M.; Ichimaru, R.; Maki, T.; Matsunaga, K.; Ohdo, S.; Anai, M.; Higuchi, S.; Goto, Y. Population pharmacokinetics of haloperidol using routine clinical pharmacokinetic data in Japanese patients. Clin. Pharmacokinet 2002, 41, 153–159. [Google Scholar] [CrossRef]
- Trogrlić, Z.; van der Jagt, M.; Osse, R.J.; Devlin, J.W.; Nieboer, D.; Koch, B.C.P.; van Schaik, R.H.N.; Hunfeld, N.G.M. Pharmacogenomic response of low dose haloperidol in critically ill adults with delirium. J. Crit. Care 2020, 57, 203–207. [Google Scholar] [CrossRef]
- FDA. Guidance for Industry Process Validation: General Principles and Practices: Food and Drug Administration. 2011. Available online: https://www.fda.gov/downloads/drugs/guidances/ucm070336.pdf (accessed on 1 January 2011).
- Agency, E.E.M. Guideline on Bioanalytical Method Validation. 2011. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-bioanalytical-method-validation_en.pdf (accessed on 21 July 2011).
- Jonsson, E.N.; Karlsson, M.O. Automated covariate model building within NONMEM. Pharm. Res. 1998, 15, 1463–1468. [Google Scholar] [CrossRef] [PubMed]
- Bergstrand, M.; Hooker, A.C.; Wallin, J.E.; Karlsson, M.O. Prediction-corrected visual predictive checks for diagnosing nonlinear mixed-effects models. Aaps. J. 2011, 13, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chityala, P.K.; Wu, L.; Chow, D.S.; Ghose, R. Effects of inflammation on irinotecan pharmacokinetics and development of a best-fit PK model. Chem. Biol. Interact 2020, 316, 108933. [Google Scholar] [CrossRef] [PubMed]
- Ternant, D.; Ducourau, E.; Perdriger, A.; Corondan, A.; Le Goff, B.; Devauchelle-Pensec, V.; Solau-Gervais, E.; Watier, H.; Goupille, P.; Paintaud, G.; et al. Relationship between inflammation and infliximab pharmacokinetics in rheumatoid arthritis. Br. J. Clin. Pharmacol. 2014, 78, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, Y.; Takahashi, Y.; Horino, A.; Usui, N.; Nishida, T.; Imai, K.; Kagawa, Y.; Inoue, Y.I. nfluence of Inflammation on the Pharmacokinetics of Perampanel. Ther. Drug Monit. 2018, 40, 725–729. [Google Scholar] [CrossRef]
- Veringa, A.; Ter Avest, M.; Span, L.F.; van den Heuvel, E.R.; Touw, D.J.; Zijlstra, J.G.; Kosterink, J.G.; van der Werf, T.S.; Alffenaar, J.C. Voriconazole metabolism is influenced by severe inflammation: A prospective study. J. Antimicrob. Chemother. 2017, 72, 261–267. [Google Scholar] [CrossRef]
- van Wanrooy, M.J.; Span, L.F.; Rodgers, M.G.; van den Heuvel, E.R.; Uges, D.R.; van der Werf, T.S.; Kosterink, J.G.; Alffenaar, J.W. Inflammation is associated with voriconazole trough concentrations. Antimicrob. Agents Chemother. 2014, 58, 7098–7101. [Google Scholar] [CrossRef] [Green Version]
- Franken, L.G.; Masman, A.D.; de Winter, B.C.M.; Baar, F.P.M.; Tibboel, D.; van Gelder, T.; Koch, B.C.P.; Mathot, R.A.A. Hypoalbuminaemia and decreased midazolam clearance in terminally ill adult patients, an inflammatory effect? Br. J. Clin. Pharmacol. 2017, 83, 1701–1712. [Google Scholar] [CrossRef]
- Vet, N.J.; Brussee, J.M.; de Hoog, M.; Mooij, M.G.; Verlaat, C.W.; Jerchel, I.S.; van Schaik, R.H.; Koch, B.C.; Tibboel, D.; Knibbe, C.A.; et al. Inflammation and Organ Failure Severely Affect Midazolam Clearance in Critically Ill Children. Am. J. Respir. Crit. Care Med. 2016, 194, 58–66. [Google Scholar] [CrossRef]
- Hefner, G.; Shams, M.E.; Unterecker, S.; Falter, T.; Hiemke, C. Inflammation and psychotropic drugs: The relationship between C-reactive protein and antipsychotic drug levels. Psychopharmacology 2016, 233, 1695–1705. [Google Scholar] [CrossRef]
- Pilla Reddy, V.; Kozielska, M.; Johnson, M.; Mafirakureva, N.; Vermeulen, A.; Liu, J.; de Greef, R.; Rujescu, D.; Groothuis, G.M.; Danhof, M.; et al. Population pharmacokinetic-pharmacodynamic modeling of haloperidol in patients with schizophrenia using positive and negative syndrome rating scale. J. Clin. Psychopharmacol. 2013, 33, 731–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, B.J.; Holford, N.H. Mechanism-based concepts of size and maturity in pharmacokinetics. Annu. Rev. Pharmacol. Toxicol. 2008, 48, 303–332. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 22 |
|---|---|
| Age, years (median, range) | 67 (48–77) |
| Male, n(%) | 12 (54.5) |
| Female, n(%) | 10 (45.5) |
| Weight, kg (median, range) | 80 (52–137) |
| Ethnic origin, n (%) | |
| Caucasian | 22 (100) |
| BMI (median, range) | 27 (18–39) |
| Primary reason for ICU admission, n (%) | |
| Surgery | 7 (32%) |
| Respiratory failure | 3 (14%) |
| Sepsis | 3 (14%) |
| Vascular aneurysm | 2 (9%) |
| Blood chemistry, serum levels at admission (median, range) | |
| Albumin, g/L | 26 (6–47) |
| Creatinine, μmol/L | 130 (32–401) |
| Urea, mmol/L | 13(4–46) |
| Bilirubin, μmol/L | 14 (3–754) |
| CRP, mg/L | 171 (4.1–368) |
| CYP2D6 n (%) | |
| Extensive metabolizers | 12 (54%) |
| Intermediate metabolizers | 7 (32%) |
| Poor metabolizers | 3 (14%) |
| CYP3A4 n (%) | |
| Extensive metabolizers | 18 (82%) |
| Intermediate metabolizers | 4 (12%) |
| Quetiapine exposure n(%) | 5 (22.7%) |
| APACHE III score median (range) | 81 (76–99) |
| ICDSC baseline median (range) | 4 (1–6) |
| Duration of stay (during using halo), days (median, range) | 6.5 (3–8) |
| Died in ICU, n (%) | 11 (50) |
| Cause of death | |
| Respiratory failure (During ICU) | 1 |
| Sepsis with multiple organ failure (During ICU) | 4 |
| Cardiac causes (after ICU) | 2 |
| Gastrointestinal causes (after ICU) | 2 |
| Respiratory insufficiency (transferred to another hospital) | 1 |
| Unknown (transferred to another hospital) | 1 |
| Blood samples collected, median (range) | 7.5 (3–8) |
| Parameter | Base Model | RSE% | Shrinkage% | Final Model | RSE% | Shrinkage% | Bootstrap of the Final Model | ||
|---|---|---|---|---|---|---|---|---|---|
| Median | 90% Percentile (Lower) | 90% Percentile (Upper) | |||||||
| CL (L/h) | 54.6 | 11 | 51.7 | 12 | 50.64 | 39.65 | 63.74 | ||
| Vd (L) | 1450 | 29 | 1490 | 31 | 1522.05 | 893.6 | 2305.2 | ||
| CRP | −0.23 | 50 | −0.21 | −0.02 | −0.42 | ||||
| IIV-CL (%) | 40.4% | 31 | 15 | 29.9% | 27 | 24 | |||
| Residual variability | 0.457 | 9 | 6 | 0.461 | 9 | 5 | 0.446 | 0.382 | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Sassen, S.D.T.; van der Jagt, M.; Endeman, H.; Koch, B.C.P.; Hunfeld, N.G.M. Pharmacokinetics of Haloperidol in Critically Ill Patients: Is There an Association with Inflammation? Pharmaceutics 2022, 14, 549. https://doi.org/10.3390/pharmaceutics14030549
Li L, Sassen SDT, van der Jagt M, Endeman H, Koch BCP, Hunfeld NGM. Pharmacokinetics of Haloperidol in Critically Ill Patients: Is There an Association with Inflammation? Pharmaceutics. 2022; 14(3):549. https://doi.org/10.3390/pharmaceutics14030549
Chicago/Turabian StyleLi, Letao, Sebastiaan D. T. Sassen, Mathieu van der Jagt, Henrik Endeman, Birgit C. P. Koch, and Nicole G. M. Hunfeld. 2022. "Pharmacokinetics of Haloperidol in Critically Ill Patients: Is There an Association with Inflammation?" Pharmaceutics 14, no. 3: 549. https://doi.org/10.3390/pharmaceutics14030549