
General Characteristics, Biomedical and Dental Application, and Usage of Chitosan in the Treatment of Temporomandibular Joint Disorders: A Narrative Review

 , , and
, , and
Abstract
:1. Introduction
2. Methodology of the Literature Search Strategy
2.1. Clinical Question
2.2. Inclusion and Exclusion Criteria
2.3. The PICO Approach
- Population:
- Intervention:
- Comparison:
- Outcome:
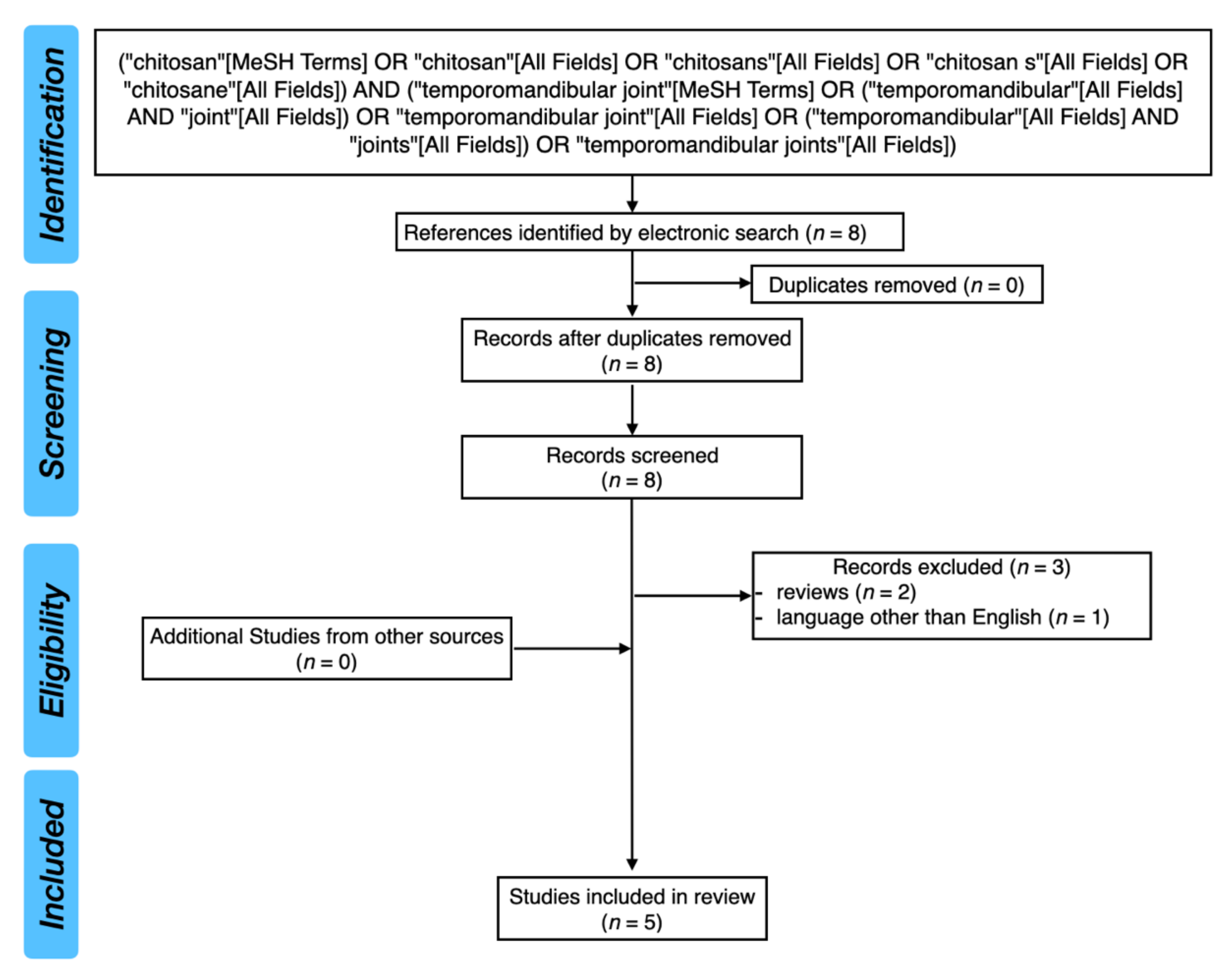
2.4. Search Strategy
2.5. Cohen’s Kappa Coefficient
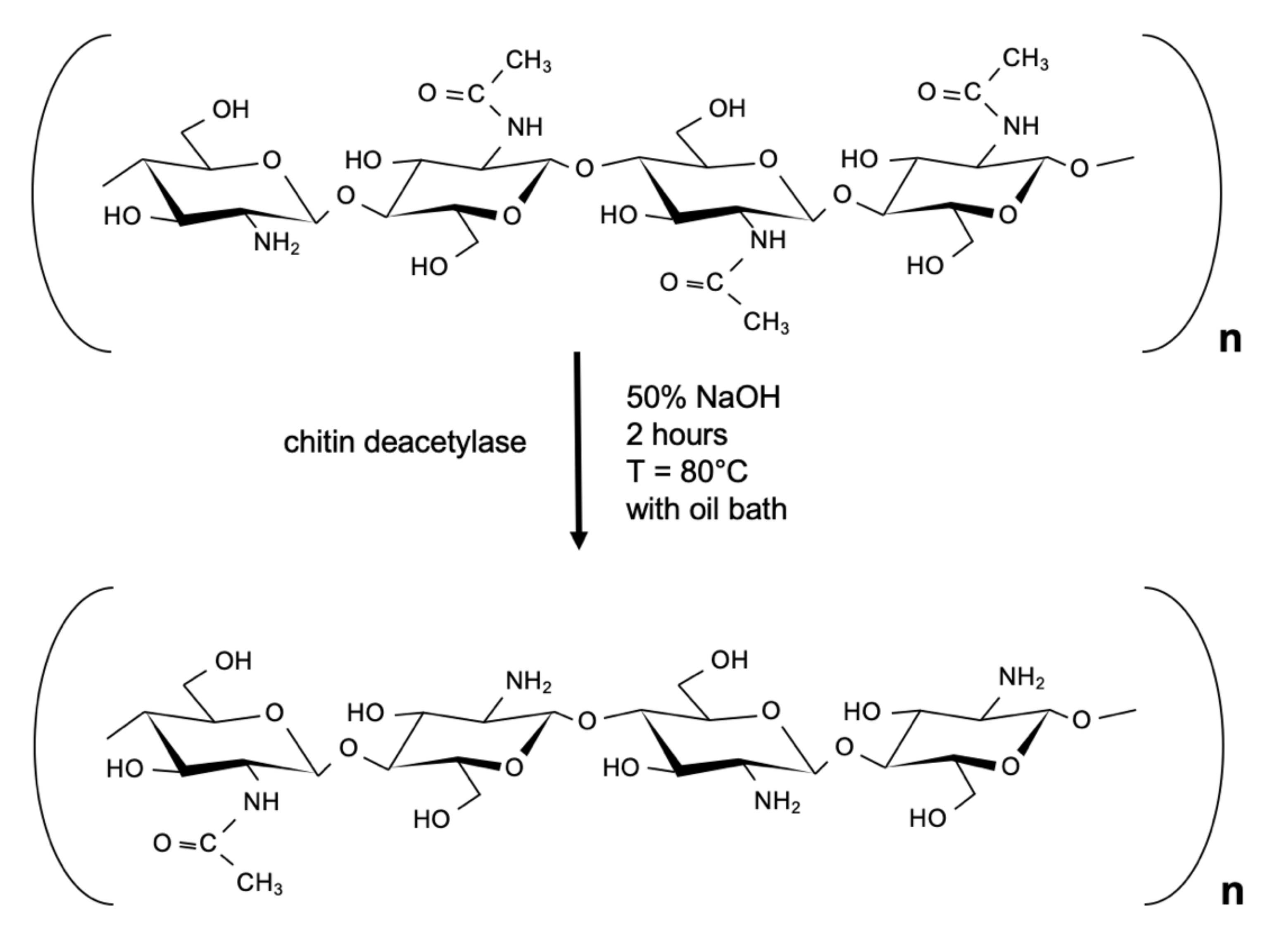
3. Chitosan: General Characteristics
4. Chitosan in Comparison to Hyaluronic Acid
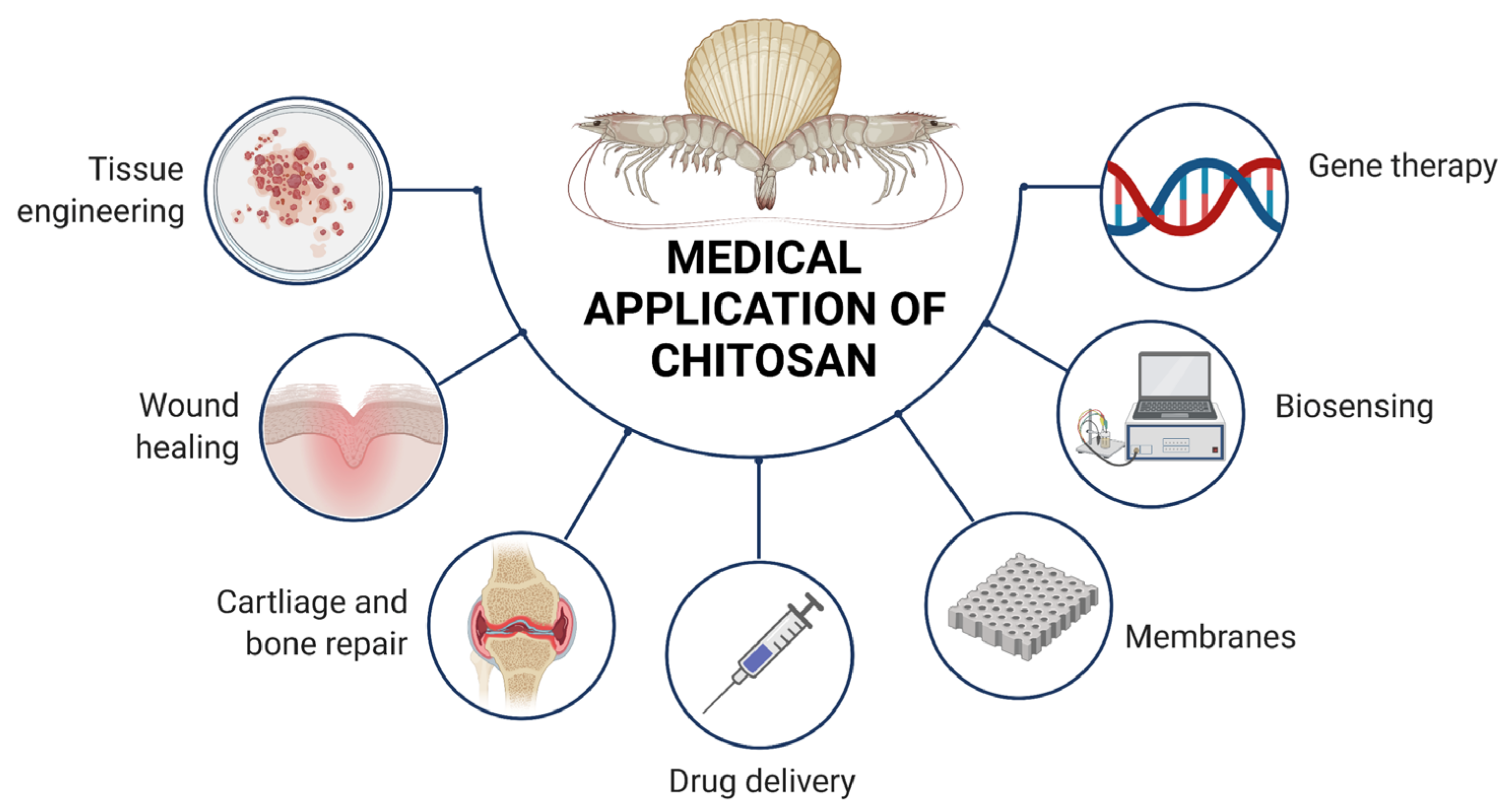
5. Properties of Chitosan and its Biomedical Application
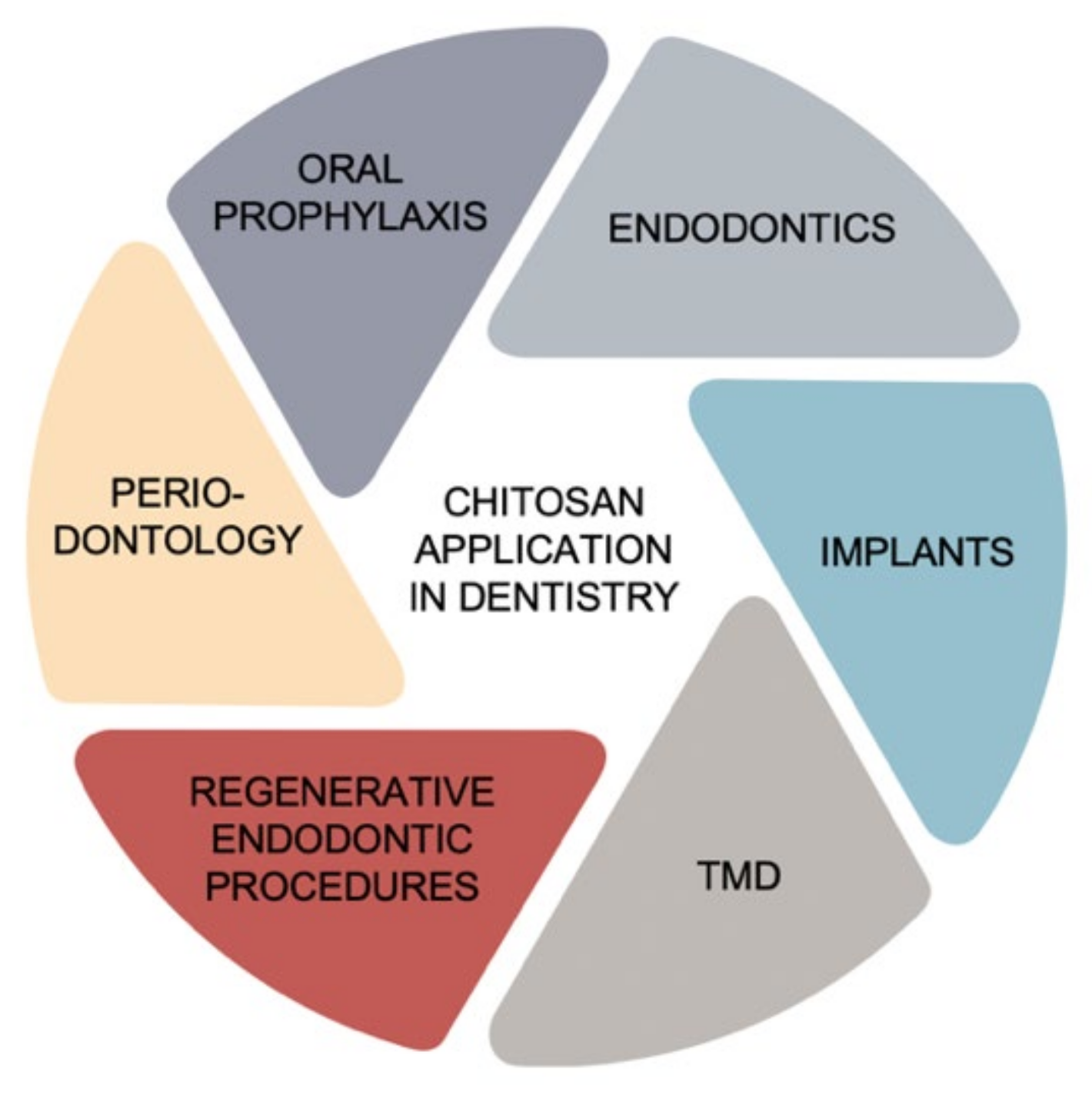
6. Chitosan Application in Dentistry
6.1. Oral Prophylaxis
6.2. Endodontics
6.3. Periodontology
6.4. Implantology
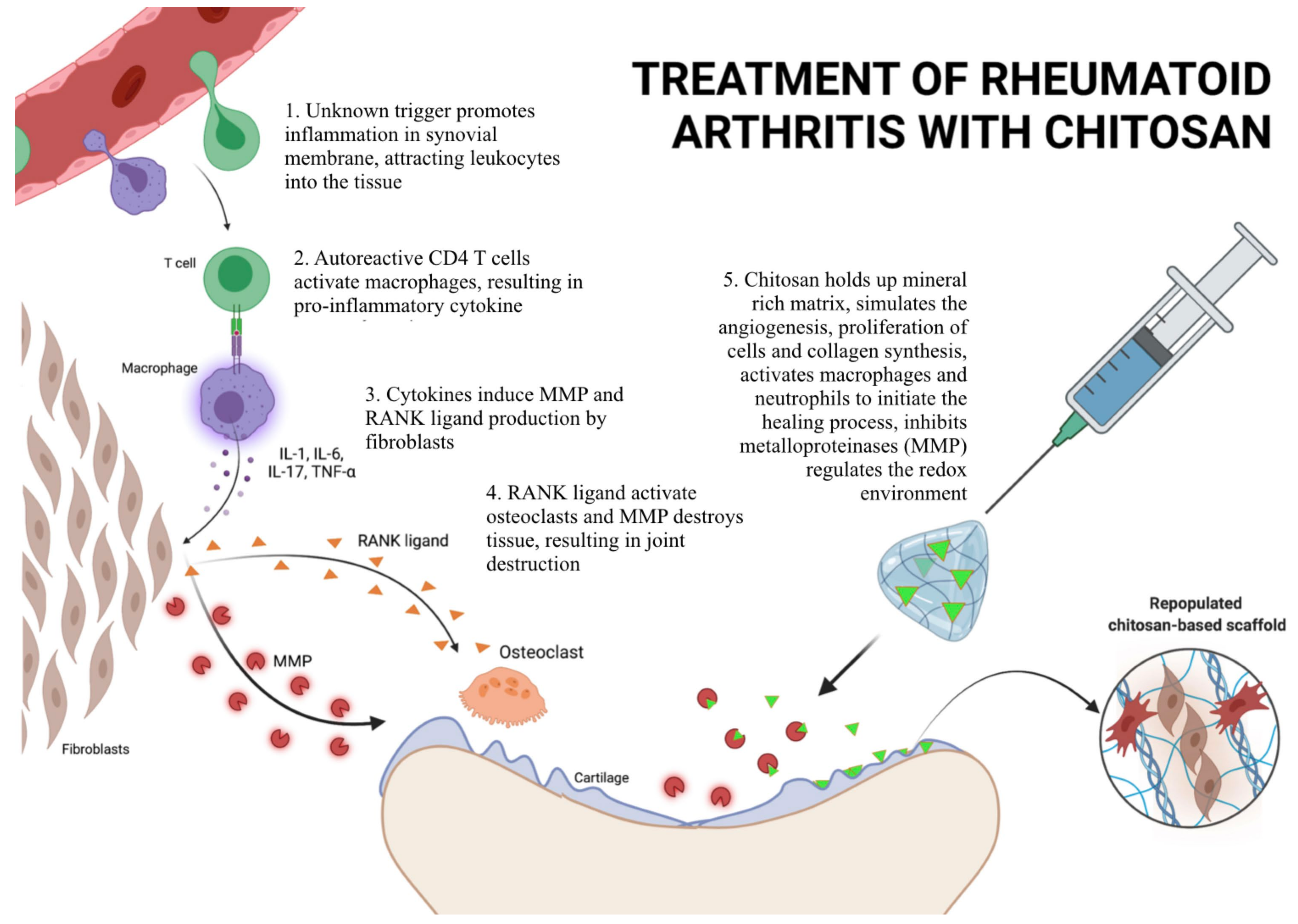
7. Chitosan in the Treatment of TMD
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ohrbach, R.; Bair, E.; Fillingim, R.B.; Gonzalez, Y.; Gordon, S.M.; Lim, P.F.; Ribeiro-Dasilva, M.; Diatchenko, L.; Dubner, R.; Greenspan, J.D.; et al. Clinical orofacial characteristics associated with risk of first-onset TMD: The OPPERA prospective cohort study. J. Pain 2013, 14 (Suppl. 12), T33–T50. [Google Scholar] [CrossRef] [Green Version]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, S.F.; Von Korff, M.; LeResche, L. Multiple pains and psychiatric disturbance. An epidemiologic investigation. Arch. Gen. Psychiatry. 1990, 47, 239–244. [Google Scholar] [CrossRef] [PubMed]
- List, T.; Dworkin, S.F. Comparing TMD diagnoses and clinical findings at Swedish and US TMD centers using research diagnostic criteria for temporomandibular disorders. J. Orofac. Pain 1996, 10, 240–253. [Google Scholar]
- John, M.T.; Reissmann, D.R.; Schierz, O.; Wassell, R.W. Oral health-related quality of life in patients with temporomandibular disorders. J. Orofac. Pain 2007, 21, 46–54. [Google Scholar] [PubMed]
- Türp, J.C.; Motschall, E.; Schindler, H.J.; Heydecke, G. In patients with temporomandibular disorders, do particular interventions influence oral health-related quality of life? A qualitative systematic review of the literature. Clin. Oral Implant. Res. 2007, 18 (Suppl. 3), 127–137. [Google Scholar] [CrossRef]
- Suvinen, T.I.; Reade, P.C.; Kemppainen, P.; Könönen, M.; Dworkin, S.F. Review of aetiological concepts of temporomandibular pain disorders: Towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur. J. Pain 2005, 9, 613–633. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Detamore, M.S.; Mercuri, L.G. Degenerative disorders of the temporomandibular joint: Etiology, diagnosis, and treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef]
- Nitzan, D.W.; Nitzan, U.; Dan, P.; Yedgar, S. The role of hyaluronic acid in protecting surface-active phospholipids from lysis by exogenous phospholipase A(2). Rheumatology 2001, 40, 336–340. [Google Scholar] [CrossRef] [Green Version]
- Nitzan, D.W. The process of lubrication impairment and its involvement in temporomandibular joint disc displacement: A theoretical concept. J. Oral Maxillofac. Surg. 2001, 59, 36–45. [Google Scholar] [CrossRef]
- Nitzan, D.W.; Marmary, Y. The “anchored disc phenomenon”: A proposed etiology for sudden-onset, severe, and persistent closed lock of the temporomandibular joint. J. Oral Maxillofac. Surg. 1997, 55, 797–802. [Google Scholar] [CrossRef]
- Zardeneta, G.; Milam, S.B.; Schmitz, J.P. Iron-dependent generation of free radicals: Plausible mechanisms in the progressive deterioration of the temporomandibular joint. J. Oral Maxillofac. Surg. 2000, 58, 302–308. [Google Scholar] [CrossRef]
- Nitzan, D.W.; Etsion, I. Adhesive force: The underlying cause of the disc anchorage to the fossa and/or eminence in the temporomandibular joint—A new concept. Int. J. Oral Maxillofac. Surg. 2002, 31, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, D.W. ‘Friction and adhesive forces’—Possible underlying causes for temporomandibular joint internal derangement. Cells Tissues Organs. 2003, 174, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Mashiah, R.; Seror, J.; Kadar, A.; Dolkart, O.; Pritsch, T.; Goldberg, R.; Klein, J. Lipid-hyaluronan synergy strongly reduces intrasynovial tissue boundary friction. Acta Biomater. 2019, 83, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.; Ziolek, R.M.; Gazzarrini, E.; Owen, D.M.; Lorenz, C.D. On the interaction of hyaluronic acid with synovial fluid lipid membranes. Phys. Chem. Chem. Phys. 2019, 21, 9845–9857. [Google Scholar] [CrossRef]
- Hilšer, P.; Suchánková, A.; Mendová, K.; Eleršič Filipič, K.; Daniel, M.; Vrbka, M. A new insight into more effective viscosupplementation based on the synergy of hyaluronic acid and phospholipids for cartilage friction reduction. Biotribology 2021, 25, 100166. [Google Scholar] [CrossRef]
- Milam, S.B.; Schmitz, J.P. Molecular biology of temporomandibular joint disorders: Proposed mechanisms of disease. J. Oral Maxillofac. Surg. 1995, 53, 1448–1454. [Google Scholar] [CrossRef]
- Milam, S.B.; Zardeneta, G.; Schmitz, J.P. Oxidative stress and degenerative temporomandibular joint disease: A proposed hypothesis. J. Oral Maxillofac. Surg. 1998, 56, 214–223. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Tojyo, I.; Yoshida, H.; Fujita, S. Role of hypoxia and interleukin-1beta in gene expressions of matrix metalloproteinases in temporomandibular joint disc cells. Arch. Oral Biol. 2005, 50, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Stegenga, B.; de Bont, L.G.; Boering, G.; van Willigen, J.D. Tissue responses to degenerative changes in the temporomandibular joint: A review. J. Oral Maxillofac. Surg. 1991, 49, 1079–1088. [Google Scholar] [CrossRef]
- Martin-Granizo, R.; Correa-Muñoz, D.C. Chondromalacia as pathological finding in arthroscopy of the temporomandibular joint: A retrospective study. J. Craniomaxillofac. Surg. 2018, 46, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Dijkgraaf, L.C.; de Bont, L.G.; Boering, G.; Liem, R.S. The structure, biochemistry, and metabolism of osteoarthritic cartilage: A review of the literature. J. Oral Maxillofac. Surg. 1995, 53, 1182–1192. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Wolford, L.M.; Ellis, E.; Neff, A. The hierarchy of different treatments for arthrogenous temporomandibular disorders: A network meta-analysis of randomized clinical trials. J. Craniomaxillofac. Surg. 2020, 48, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary Approach to the Temporomandibular Joint Osteoarthritis-Review of the Literature. Medicina 2020, 56, 225. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Mechanisms of Action and Efficacy of Hyaluronic Acid, Corticosteroids and Platelet-Rich Plasma in the Treatment of Temporomandibular Joint Osteoarthritis-A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7405. [Google Scholar] [CrossRef] [PubMed]
- Thein-Han, W.W.; Misra, R.D. Biomimetic chitosan-nanohydroxyapatite composite scaffolds for bone tissue engineering. Acta Biomater. 2009, 5, 1182–1197. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Meng, X.; Xing, R.; Liu, S.; Chen, X.; Qin, Y.; Yu, H.; Li, P. Design, synthesis and antimicrobial activity of 6-N-substituted chitosan derivatives. Bioorg. Med. Chem. Lett. 2016, 26, 4548–4551. [Google Scholar] [CrossRef]
- Sukpaita, T.; Chirachanchai, S.; Pimkhaokham, A.; Ampornaramveth, R.S. Chitosan-Based Scaffold for Mineralized Tissues Regeneration. Mar. Drugs. 2021, 19, 551. [Google Scholar] [CrossRef]
- Elieh-Ali-Komi, D.; Hamblin, M.R. Chitin and Chitosan: Production and Application of Versatile Biomedical Nanomaterials. Int. J. Adv. Res. 2016, 4, 411–427. [Google Scholar]
- Chocholata, P.; Kulda, V.; Babuska, V. Fabrication of Scaffolds for Bone-Tissue Regeneration. Materials 2019, 12, 568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Mo, X.; Ma, F.; Li, S.; Wu, G.; Tang, B.; Lin, L. Synthesis of carboxymethyl chitosan-strontium complex and its therapeutic effects on relieving osteoarthritis. Carbohydr. Polym. 2021, 261, 117869. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yang, B.; Li, M.; Li, J.; Wan, Y. Enhanced dual network hydrogels consisting of thiolated chitosan and silk fibroin for cartilage tissue engineering. Carbohydr. Polym. 2020, 227, 115335. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.Y.; Lin, Y.C.; Lu, H.T.; Ho, Y.C.; Weng, S.C.; Tsai, M.L.; Mi, F.L. A novel injectable in situ forming gel based on carboxymethyl hexanoyl chitosan/hyaluronic acid polymer blending for sustained release of berberine. Carbohydr. Polym. 2019, 206, 664–673. [Google Scholar] [CrossRef]
- Wang, Y.; Yuan, X.; Yu, K.; Meng, H.; Zheng, Y.; Peng, J.; Lu, S.; Liu, X.; Xie, Y.; Qiao, K. Fabrication of nanofibrous microcarriers mimicking extracellular matrix for functional microtissue formation and cartilage regeneration. Biomaterials 2018, 171, 118–132. [Google Scholar] [CrossRef]
- Satitsri, S.; Muanprasat, C. Chitin and Chitosan Derivatives as Biomaterial Resources for Biological and Biomedical Applications. Molecules 2020, 25, 5961. [Google Scholar] [CrossRef]
- Patrulea, V.; Ostafe, V.; Borchard, G.; Jordan, O. Chitosan as a starting material for wound healing applications. Eur. J. Pharm. Biopharm. 2015, 97, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Xu, W.; Mohan, A.; Pitts, N.L.; Udenigwe, C.; Mason, B. Bile acid-binding capacity of lobster shell-derived chitin, chitosan and chitooligosaccharides. Food Biosci. 2020, 33, 100476. [Google Scholar] [CrossRef]
- Wang, M.; Chen, L.J.; Ni, J.; Weng, J.; Yue, C.Y. Manufacture and evaluation of bioactive and biodegradable materials and scaffolds for tissue engineering. J. Mater. Sci. Mater. Med. 2001, 12, 855–860. [Google Scholar] [CrossRef]
- Hahn, T.; Tafi, E.; Paul, A.; Salvia, R.; Falabella, P.; Zibek, S. Current state of chitin purification and chitosan production from insects. J. Chem. Technol. Biotechnol. 2020, 95, 2775–2795. [Google Scholar] [CrossRef]
- Synowiecki, J.; Al-Khateeb, N.A. Production, properties, and some new applications of chitin and its derivatives. Crit. Rev. Food Sci. Nutr. 2003, 43, 145–171. [Google Scholar] [CrossRef]
- Cheung, R.C.; Ng, T.B.; Wong, J.H.; Chan, W.Y. Chitosan: An Update on Potential Biomedical and Pharmaceutical Applications. Mar. Drugs 2015, 13, 5156–5186. [Google Scholar] [CrossRef]
- Kaczmarek, M.B.; Struszczyk-Swita, K.; Li, X.; Szczęsna-Antczak, M.; Daroch, M. Enzymatic Modifications of Chitin, Chitosan, and Chitooligosaccharides. Front. Bioeng. Biotechnol. 2019, 7, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grifoll-Romero, L.; Pascual, S.; Aragunde, H.; Biarnés, X.; Planas, A. Chitin Deacetylases: Structures, Specificities, and Biotech Applications. Polymers 2018, 10, 352. [Google Scholar] [CrossRef] [Green Version]
- Pakizeh, M.; Moradi, A.; Ghassemi, T. Chemical extraction and modification of chitin and chitosan from shrimp shells. Eur. Polym. J. 2021, 159, 110709. [Google Scholar] [CrossRef]
- Morin-Crini, N.; Lichtfouse, E.; Torri, G.; Crini, G. Applications of chitosan in food, pharmaceuticals, medicine, cosmetics, agriculture, textiles, pulp and paper, biotechnology, and environmental chemistry. Environ. Chem. Lett. 2019, 17, 1667–1692. [Google Scholar] [CrossRef] [Green Version]
- Batista, A.C.L.; Souza, F.E.; Paiva, W.S. Review of fungal chitosan: Past, present and perspectives in Brazil. Polímeros 2018, 28, 3. [Google Scholar] [CrossRef] [Green Version]
- Younes, I.; Rinaudo, M. Chitin and chitosan preparation from marine sources. Structure, properties and applications. Mar. Drugs 2015, 13, 1133. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.L.; Chen, Y.B.; Lo, Y.L.; Lin, Y.H. Development of chitosan/β-glycerophosphate/glycerol hydrogel as a thermosensitive coupling agent. Carbohydr. Polym. 2016, 147, 409–414. [Google Scholar] [CrossRef]
- Islam, S.; Bhuiyan, M.A.R.; Islam, M.N. Chitin and Chitosan: Structure, Properties and Applications in Biomedical Engineering. J. Polym. Environ. 2017, 27, 854–866. [Google Scholar] [CrossRef]
- Thadathil, N.; Velappan, S.P. Recent developments in chitosanase research and its biotechnological applications: A review. Food Chem. 2014, 150, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, A.; Sittinger, M.; Risbud, M.V. Chitosan: A versatile biopolymer for orthopaedic tissue-engineering. Biomaterials 2005, 26, 5983–5990. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Wang, Y.; Yang, G. The Modulation of Chitosan-DNA Interaction by Concentration and pH in Solution. Polymers 2019, 11, 646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bravo-Anaya, L.M.; Soltero, J.F.; Rinaudo, M. DNA/chitosan electrostatic complex. Int. J. Biol. Macromol. 2016, 88, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Goldmann, K.; Ensminger, S.M.; Spriewald, B.M. Oral gene application using chitosan-DNA nanoparticles induces transferable tolerance. Clin. Vaccine Immunol. 2012, 19, 1758–1764. [Google Scholar] [CrossRef] [Green Version]
- Mao, H.Q.; Roy, K.; Troung-Le, V.L.; Janes, K.A.; Lin, K.Y.; Wang, Y.; August, J.T.; Leong, K.W. Chitosan-DNA nanoparticles as gene carriers: Synthesis, characterization and transfection efficiency. J. Control. Release 2001, 70, 399–421. [Google Scholar] [CrossRef]
- Moeini, A.; Pedram, P.; Makvandi, P.; Malinconico, M.; Gomez d’Ayala, G. Wound healing and antimicrobial effect of active secondary metabolites in chitosan-based wound dressings: A review. Carbohydr. Polym. 2020, 233, 115839. [Google Scholar] [CrossRef]
- Ma, Z.; Kotaki, M.; Inai, R.; Ramakrishna, S. Potential of nanofiber matrix as tissue-engineering scaffolds. Tissue Eng. 2005, 11, 101–109. [Google Scholar] [CrossRef]
- Aranaz, I.; Alcántara, A.R.; Civera, M.C.; Arias, C.; Elorza, B.; Heras Caballero, A.; Acosta, N. Chitosan: An Overview of Its Properties and Applications. Polymers 2021, 13, 3256. [Google Scholar] [CrossRef]
- Valachová, K.; Šoltés, L. Versatile Use of Chitosan and Hyaluronan in Medicine. Molecules 2021, 26, 1195. [Google Scholar] [CrossRef]
- Bayer, I.S. Hyaluronic Acid and Controlled Release: A Review. Molecules. 2020, 25, 2649. [Google Scholar] [CrossRef]
- Vigetti, D.; Karousou, E.; Viola, M.; Deleonibus, S.; De Luca, G.; Passi, A. Hyaluronan: Biosynthesis and signaling. Biochim. Biophys. Acta. 2014, 1840, 2452–2459. [Google Scholar] [CrossRef] [Green Version]
- Salwowska, N.M.; Bebenek, K.A.; Żądło, D.A.; Wcisło-Dziadecka, D.L. Physiochemical properties and application of hyaluronic acid: A systematic review. J. Cosmet. Dermatol. 2016, 15, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef] [PubMed]
- Turley, E.A.; Noble, P.W.; Bourguignon, L.Y. Signaling properties of hyaluronan receptors. J. Biol. Chem. 2002, 277, 4589–4592. [Google Scholar] [CrossRef] [Green Version]
- Litwiniuk, M.; Krejner, A.; Speyrer, M.S.; Gauto, A.R.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds 2016, 28, 78–88. [Google Scholar] [PubMed]
- Kim, H.; Jeong, H.; Han, S.; Beack, S.; Hwang, B.W.; Shin, M.; Oh, S.S.; Hahn, S.K. Hyaluronate and its derivatives for customized biomedical applications. Biomaterials 2017, 123, 155–171. [Google Scholar] [CrossRef]
- Juncan, A.M.; Moisa, D.; Santini, A.; Morgovan, C.; Rus, L.-L.; Vonica-Tincu, A.L.; Loghin, F. Advantages of Hyaluronic Acid and Its Combination with Other Bioactive Ingredients in Cosmeceuticals. Molecules 2021, 26, 4429. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef]
- Kim, J.; Chang, J.Y.; Kim, Y.Y.; Kim, M.J.; Kho, H.S. Effects of molecular weight of hyaluronic acid on its viscosity and enzymatic activities of lysozyme and peroxidase. Arch. Oral Biol. 2018, 89, 55–64. [Google Scholar] [CrossRef]
- Huang, G.; Chen, J. Preparation and applications of hyaluronic acid and its derivatives. Int. J. Biol. Macromol. 2019, 125, 478–484. [Google Scholar] [CrossRef]
- Oh, E.J.; Park, K.; Kim, K.S.; Kim, J.; Yang, J.A.; Kong, J.H.; Lee, M.Y.; Hoffman, A.S.; Hahn, S.K. Target specific and long-acting delivery of protein, peptide, and nucleotide therapeutics using hyaluronic acid derivatives. J. Control. Release 2010, 141, 2–12. [Google Scholar] [CrossRef]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Vet. Sci. 2019, 6, 192. [Google Scholar] [CrossRef] [Green Version]
- Allan, C.R.; Hadwiger, L.A. The fungicidal effect of chitosan on fungi of varying cell wall composition. Exp. Mycol. 1979, 3, 285–287. [Google Scholar] [CrossRef]
- Sudarshan, N.R.; Hoover, D.G.; Knorr, D. Antibacterial action of chitosan. Food Biotechnol. 1992, 6, 257–272. [Google Scholar] [CrossRef]
- Zheng, L.Y.; Zhu, J.F. Study on Antimicrobial Activity of Chitosan with Different Molecular Weights. Carbohydr. Polym. 2003, 54, 527–530. [Google Scholar] [CrossRef]
- Beanes, S.R.; Dang, C.; Soo, C.; Ting, K. Skin repair and scar formation: The central role of TGF-beta. Expert Rev. Mol. Med. 2003, 5, 1–22. [Google Scholar] [CrossRef]
- Uragami, T.; Tokura, S. Material Science of Chitin and Chitosan, 1st ed.; Springer: New York, NY, USA, 2006; pp. 51–79. [Google Scholar]
- Chen, W.Y.; Rogers, A.A.; Lydon, M.J. Characterization of biologic properties of wound fluid collected during early stages of wound healing. J. Invest. Dermatol. 1992, 99, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.M.; Kim, S.K. Chitooligosaccharides inhibit activation and expression of matrix metalloproteinase-2 in human dermal fibroblasts. FEBS Lett. 2006, 580, 2661–2666. [Google Scholar] [CrossRef] [Green Version]
- Gorzelanny, C.; Pöppelmann, B.; Strozyk, E.; Moerschbacher, B.M.; Schneider, S.W. Specific interaction between chitosan and matrix metalloprotease 2 decreases the invasive activity of human melanoma cells. Biomacromolecules 2007, 8, 3035–3040. [Google Scholar] [CrossRef]
- Shikhman, A.R.; Amiel, D.; D’Lima, D.; Hwang, S.B.; Hu, C.; Xu, A.; Hashimoto, S.; Kobayashi, K.; Sasho, T.; Lotz, M.K. Chondroprotective activity of N-acetylglucosamine in rabbits with experimental osteoarthritis. Ann. Rheum. Dis. 2005, 64, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, K. Autoimmunity and Transplantation. In Janeway’s Immunobiology, 8th ed.; Garland Science, Taylor & Francis Group: New York, NY, USA, 2012; Volume 1, pp. 637–638. [Google Scholar]
- Mirahmadi, F.; Tafazzoli-Shadpour, M.; Shokrgozar, M.A.; Bonakdar, S. Enhanced mechanical properties of thermosensitive chitosan hydrogel by silk fibers for cartilage tissue engineering. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 4786–4794. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.K.; Matthew, H.W. Application of chitosan-based polysaccharide biomaterials in cartilage tissue engineering: A review. Biomaterials 2000, 21, 2589–2598. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M. A review of chitin and chitosan applications. React. Funct. Polym. 2000, 46, 1–27. [Google Scholar] [CrossRef]
- Zhao, M.; Chen, Z.; Liu, K.; Wan, Y.Q.; Li, X.D.; Luo, X.W.; Bai, Y.G.; Yang, Z.L.; Feng, G. Repair of articular cartilage defects in rabbits through tissue-engineered cartilage constructed with chitosan hydrogel and chondrocytes. J. Zhejiang Univ. Sci. B. 2015, 16, 914–923. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Jin, X.; Cong, Y.; Liu, Y.; Fu, J. Degradable natural polymer hydrogels for articular cartilage tissue engineering. J. Chem. Technol. Biotechnol. 2013, 88, 327–339. [Google Scholar] [CrossRef]
- Hao, T.; Wen, N.; Cao, J.K.; Wang, H.B.; Lü, S.H.; Liu, T.; Lin, Q.X.; Duan, C.M.; Wang, C.Y. The support of matrix accumulation and the promotion of sheep articular cartilage defects repair in vivo by chitosan hydrogels. Osteoarthr. Cartil. 2010, 18, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Comblain, F.; Rocasalbas, G.; Gauthier, S.; Henrotin, Y. Chitosan: A promising polymer for cartilage repair and viscosupplementation. Biomed. Mater. Eng. 2017, 28, S209–S215. [Google Scholar] [CrossRef]
- Howling, G.I.; Dettmar, P.W.; Goddard, P.A.; Hampson, F.C.; Dornish, M.; Wood, E.J. The effect of chitin and chitosan on the proliferation of human skin fibroblasts and keratinocytes in vitro. Biomaterials 2001, 22, 2959–2966. [Google Scholar] [CrossRef]
- Qi, L.; Xu, Z. In vivo antitumor activity of chitosan nanoparticles. Bioorg. Med. Chem. Lett. 2006, 16, 4243–4245. [Google Scholar] [CrossRef]
- Dass, C.R.; Choong, P.F. The use of chitosan formulations in cancer therapy. J. Microencapsul. 2008, 25, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Tokoro, A.; Tatewaki, N.; Suzuki, K.; Mikami, T.; Suzuki, S.; Suzuki, M. Growth-inhibitory effect of hexa-N-acetylchitohexaose and chitohexaose against Meth-A solid tumor. Chem. Pharm. Bull. 1988, 36, 784–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, J.; Saiki, I.; Nishimura, S.; Nishi, N.; Tokura, S.; Azuma, I. Inhibitory effect of chitin heparinoids on the lung metastasis of B16-BL6 melanoma. Jpn. J. Cancer Res. 1989, 80, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Yagi, K.; Iwakawa, S.; Hirai, M. Chitosan induces apoptosis via caspase-3 activation in bladder tumor cells. Jpn. J. Cancer Res. 2001, 92, 459–466. [Google Scholar] [CrossRef]
- Khor, E.; Lim, L.Y. Implantable applications of chitin and chitosan. Biomaterials 2003, 24, 2339–2349. [Google Scholar] [CrossRef]
- Hamedi, H.; Moradi, S.; Hudson, S.M.; Tonelli, A.E. Chitosan based hydrogels and their applications for drug delivery in wound dressings: A review. Carbohydr. Polym. 2018, 199, 445–460. [Google Scholar] [CrossRef]
- Muzzarelli, R.A.A. Chitins and chitosans for the repair of wounded skin, nerve, cartilage and bone. Carbohydr. Polym. 2009, 76, 167–182. [Google Scholar] [CrossRef]
- Ong, S.Y.; Wu, J.; Moochhala, S.M.; Tan, M.H.; Lu, J. Development of a chitosan-based wound dressing with improved hemostatic and antimicrobial properties. Biomaterials 2008, 29, 4323–4332. [Google Scholar] [CrossRef]
- Ishihara, M.; Nakanishi, K.; Ono, K.; Sato, M.; Kikuchi, M.; Saito, Y.; Yura, H.; Matsui, T.; Hattori, H.; Uenoyama, M.; et al. Photocrosslinkable chitosan as a dressing for wound occlusion and accelerator in healing process. Biomaterials 2002, 23, 833–840. [Google Scholar] [CrossRef]
- Chung, Y.C.; Su, Y.P.; Chen, C.C.; Jia, G.; Wang, H.L.; Wu, J.C.; Lin, J.G. Relationship between antibacterial activity of chitosan and surface characteristics of cell wall. Acta Pharmacol. Sin. 2004, 25, 932–936. [Google Scholar]
- Visveswaraiah, P.M.; Prasad, D.; Johnson, S. Chitosan A novel way to intervene in enamel demineralization—An in vitro study. Int. J. Curr. Microbiol. Appl. Sci. 2014, 3, 617. [Google Scholar]
- Costa, E.M.; Silva, S.; Madureira, A.R.; Cardelle-Cobas, A.; Tavaria, F.K.; Pintado, M.M. A comprehensive study into the impact of a chitosan mouthwash upon oral microorganism’s biofilm formation in vitro. Carbohydr. Polym. 2014, 101, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Di Giulio, M.; Di Bartolomeo, S.; Di Campli, E.; Sancilio, S.; Marsich, E.; Travan, A.; Cataldi, A.; Cellini, L. The Effect of a Silver Nanoparticle Polysaccharide System on Streptococcal and Saliva-Derived Biofilms. Int. J. Mol. Sci. 2013, 14, 13615–13625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakhri, E.; Eslami, H.; Maroufi Ganbarov, K.; Yousefi, M.; Tanomand, A.; Yousefi, B.; Mahmoudi, S.; Kafil, H.S. Chitosan biomaterials application in dentistry. Int. J. Biol. Macromol. 2020, 162, 956–974. [Google Scholar] [CrossRef] [PubMed]
- Machut, K.; Zoltowska, A.; Pawlowska, E.; Derwich, M. Plasma Rich in Growth Factors in the Treatment of Endodontic Periapical Lesions in Adult Patients: Case Reports. Int. J. Mol. Sci. 2021, 22, 9458. [Google Scholar] [CrossRef]
- Loyola-Rodríguez, J.P.; Torres-Méndez, F.; Espinosa-Cristobal, L.F.; García-Cortes, J.O.; Loyola-Leyva, A.; González, F.J.; Soto-Barreras, U.; Nieto-Aguilar, R.; Contreras-Palma, G. Antimicrobial activity of endodontic sealers and medications containing chitosan and silver nanoparticles against Enterococcus faecalis. J. Appl. Biomater. Funct. Mater. 2019, 17, 2280800019851771. [Google Scholar] [CrossRef] [Green Version]
- Atila, D.; Chen, C.Y.; Lin, C.P.; Lee, Y.L.; Hasirci, V.; Tezcaner, A.; Lin, F.H. In vitro evaluation of injectable Tideglusib-loaded hyaluronic acid hydrogels incorporated with Rg1-loaded chitosan microspheres for vital pulp regeneration. Carbohydr. Polym. 2022, 278, 118976. [Google Scholar] [CrossRef]
- Farea, M.; Husein, A.; Halim, A.S.; Abdullah, N.A.; Mokhtar, K.I.; Lim, C.K.; Berahim, Z.; Mokhtar, K. Synergistic effects of chitosan scaffold and TGFβ1 on the proliferation and osteogenic differentiation of dental pulp stem cells derived from human exfoliated deciduous teeth. Arch. Oral Biol. 2014, 59, 1400–1411. [Google Scholar] [CrossRef]
- Tanikonda, R.; Ravi, R.K.; Kantheti, S.; Divella, S. Chitosan: Applications in Dentistry. Trends Biomater. Artif. Organs 2014, 28, 74–78. [Google Scholar]
- Ho, M.H.; Hsieh, C.C.; Hsiao, S.H.; Thien, D.V.H. Fabrication of asymmetric chitosan GTR membranes for the treatment of periodontal disease. Carbohydr. Polym. 2010, 79, 955–963. [Google Scholar] [CrossRef]
- Ji, Q.X.; Deng, J.; Xing, X.M.; Yuan, C.Q.; Yu, X.B.; Xu, Q.C.; Yue, J. Biocompatibility of a chitosan-based injectable thermosensitive hydrogel and its effects on dog periodontal tissue regeneration. Carbohydr. Polym. 2010, 82, 1153–1160. [Google Scholar] [CrossRef]
- Needleman, I.G.; Smales, F.C. In vitro assessment of bioadhesion for periodontal and buccal drug delivery. Biomaterials 1995, 16, 617–624. [Google Scholar] [CrossRef]
- Sukpaita, T.; Chirachanchai, S.; Suwattanachai, P.; Everts, V.; Pimkhaokham, A.; Ampornaramveth, R.S. In Vivo Bone Regeneration Induced by a Scaffold of Chitosan/Dicarboxylic Acid Seeded with Human Periodontal Ligament Cells. Int. J. Mol. Sci. 2019, 20, 4883. [Google Scholar] [CrossRef] [Green Version]
- Su, W.T.; Wu, P.S.; Ko, C.S.; Huang, T.Y. Osteogenic differentiation and mineralization of human exfoliated deciduous teeth stem cells on modified chitosan scaffold. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 41, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Alnufaiy, B.M.; Lambarte, R.N.A.; Al-Hamdan, K.S. The Osteogenetic Potential of Chitosan Coated Implant: An In Vitro Study. J. Stem Cells Regen. Med. 2020, 16, 44–49. [Google Scholar] [CrossRef]
- Li, F.L.; Wu, C.B.; Sun, H.J.; Zhou, Q. Comparison of Autologous Platelet-Rich Plasma and Chitosan in the Treatment of Temporomandibular Joint Osteoarthritis: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2021, 79, 324–332. [Google Scholar] [CrossRef]
- Talaat, W.M.; Haider, M.; Kawas, S.A.; Kandil, N.G.; Harding, D.R. Chitosan-Based Thermosensitive Hydrogel for Controlled Drug Delivery to the Temporomandibular Joint. J. Craniofac. Surg. 2016, 27, 735–740. [Google Scholar] [CrossRef]
- Li, H.P.; Sun, S.F.; Fan, B.T.; Shen, P.; Zheng, J.S.; Zhang, S.Y. Prevention of adhesions in the temporomandibular joint by the use of chitosan membrane in goats. Br. J. Oral Maxillofac. Surg. 2017, 55, 26–30. [Google Scholar] [CrossRef]
- Bousnaki, M.; Bakopoulou, A.; Papadogianni, D.; Barkoula, N.M.; Alpantaki, K.; Kritis, A.; Chatzinikolaidou, M.; Koidis, P. Fibro/chondrogenic differentiation of dental stem cells into chitosan/alginate scaffolds towards temporomandibular joint disc regeneration. J. Mater. Sci. Mater. Med. 2018, 29, 97. [Google Scholar] [CrossRef]
- Wu, Y.; Gong, Z.; Li, J.; Meng, Q.; Fang, W.; Long, X. The pilot study of fibrin with temporomandibular joint derived synovial stem cells in repairing TMJ disc perforation. Biomed. Res. Int. 2014, 2014, 454021. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | List of Specific Criteria |
|---|---|
| Inclusion criteria | -Randomized controlled trials -Randomized clinical trials -Case-control studies -Case reports -Animal studies -Study population: humans diagnosed with TMD, animal models -Methods of treatment: intraarticular injections of chitosan, usage of chitosan-based scaffolds placed in the TMJs -Papers written in English |
| Exclusion criteria | -Comments -Systematic reviews and metanalyses -Study population: patients without the diagnosis of TMD -Methods of treatment: conservative methods of treatment (including physiotherapy, occlusal splint therapy and pharmacotherapy) -Papers written in languages other than English |
| Comparable Characteristic [References] | Chitosan | Hyaluronic Acid |
|---|---|---|
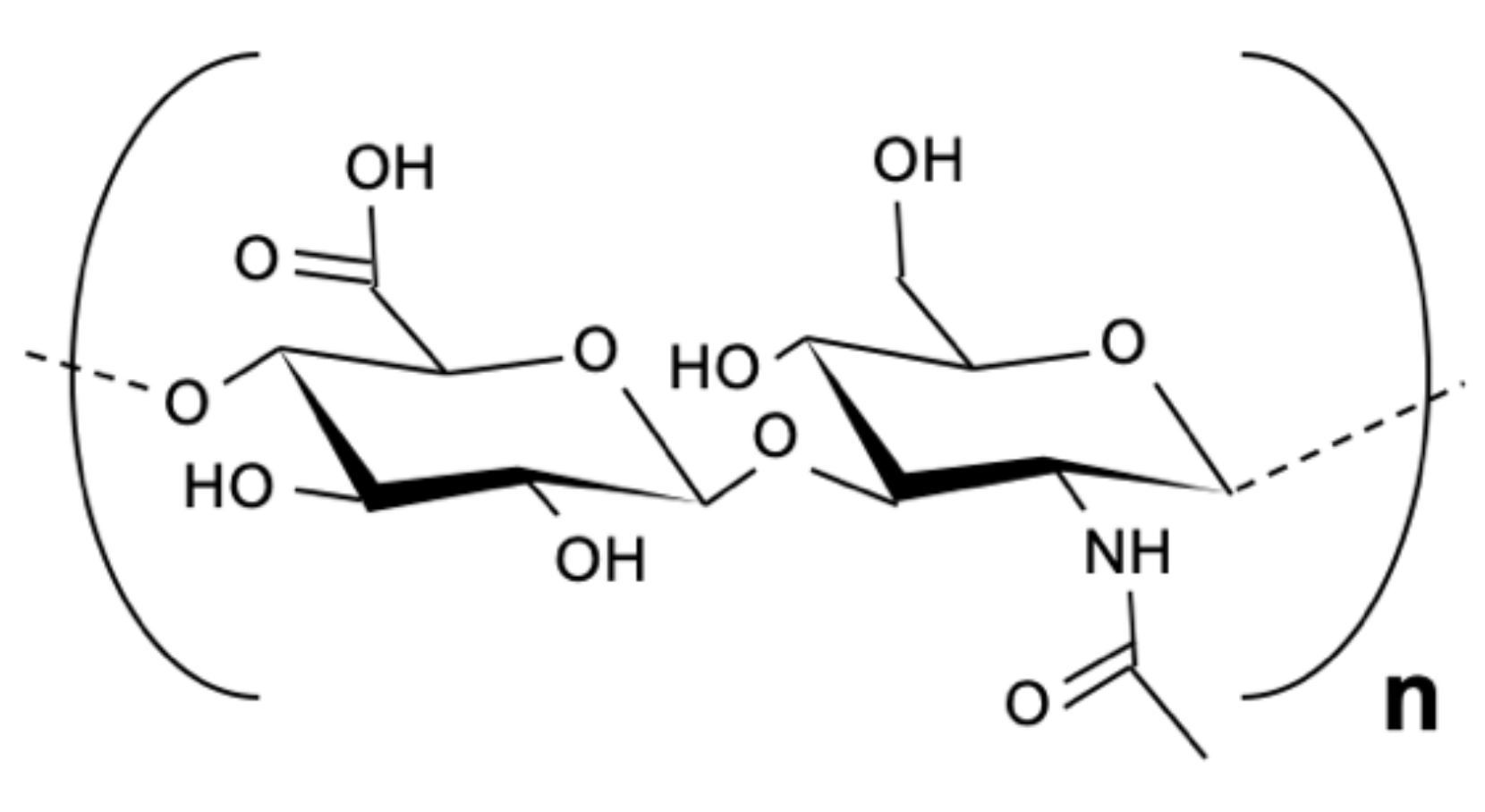
| Chemical structure [36,37,61,62] | mucopolysaccharide; deacetylated glucosamine (GlcN) and acetylated N-acetyl-glucosamine (GlcNAc) | mucopolysaccharide; D-glucuronic acid (D-GlcA) and N-acetylglucosamine (GlcNAc) |
| Electric charge [42,62] | cationic | anionic |
| Glycoside linkages [36,37,42,61,62,63,64,66] | β-(1–4) | β-(1–4) and β-(1–3) |
| Origin [29,36,37,61,62,71] | chitin ex. shells of shrimp or other crustaceans | 1. ECM of vertebrate’s tissue, 2. bacterial sources, 3. chemoenzymatic sources |
| Appearance [44,64] | white or gray, translucent flake or powder solid, tasteless, odorless, non-toxic | transparent, viscous fluid or white powder |
| Molecular weight [42,64] | 300–1000 kDa | 4–20,000 kDa |
| Degradation enzyme [51,63,66] | chitosanases (hydrolasis) | hyaluronidases (hydrolasis) |
| Solubility [29,50,64,71] | only in solutions of pH ≤ 7 | good in organic and inorganic solutions; HA depolimerizes when 4 < pH < 11 |
| Physiochemical properties [36,37,40,42,61,62,63,66,71] | depend on molecular weight and acetylation degree: 1. bioadhesive, 2. biocompatible, 3. biodegradable | 1. viscosity, 2. elasticity, 3. lubrication, 4. a high capacity for holding water, 5. biocompatible, 6. biodegradable, 7. bioadhesive |
| Biological properties [37,57,59,72,73] | 1. mucoadhesive, 2. bactericidal, 3. fungicidal activity, 4. wound healing potential 5. antioxidant activity, 6. cholesterol and triglyceride trapping, 7. hypoglycemic effects | depend on the molecular size of HA: 1. regulation of cell division, migration, differentiation; 2. HA is an extracellular transmitting molecule in signaling pathways; 3. participates in tissue regeneration and inflammation 4. provides structural framework for cells |
| Reference | Study Design | Participants and Intervention | Endpoint and Results |
|---|---|---|---|
| Li et al. [118] | Retrospective, case control study | 27 patients (24 women, 3 men, aged 25.74 ± 9.75): - chitosan group (15 patients): 3 intraarticular injections of 1.0 mL of chitosan once a month for 3 months - PRP group (12 patients): 3 intraarticular injections of 1.0 mL of PRP once a month for 3 months | Endpoint: 6 months MIO improved significantly in both groups, significantly better results presented PRP group. Pain intensity decreased in both groups, significantly lower pain intensity at 6 months after the treatment presented PRP group. Both of the groups reported relief of TMJ sounds. Complications after intraarticular injections were observed only in the PRP group. |
| Talaat et al. [119] | Animal study | 13 adult male New Zealand white rabbits (18 weeks old on average; mean weight of 2.5 kg) - study group (left TMJs) injection of 0.2 mL of Chitosan/β-glycerophosphate/Hyaluronic Acid into rabbits’ left TMJs - control group (right TMJs) injection of 0.2 mL of Hyaluronic Acid (10 mg/mL) | Endpoint: 7 days Hydrogel scaffolds were able to retain significantly more of injected HA in the rabbits TMJs after 7 days compared to the control. |
| Li et al. [120] | Animal study | 6 healthy adult goats: - control group (2 goats)—retrodiscal tissues were cut off without any other procedures - experimental group (4 goats)—retrodiscal tissues were cut off and chitosan membrane was placed between the articular disc and the condyle | Endpoint: 6 months Experimental group presented smooth condylar surfaces, with no hyperemia or adhesion, and significantly greater maximum passive mouth opening comparing to control group. Control group was diagnosed with severe intraarticular adhesions. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derwich, M.; Lassmann, L.; Machut, K.; Zoltowska, A.; Pawlowska, E. General Characteristics, Biomedical and Dental Application, and Usage of Chitosan in the Treatment of Temporomandibular Joint Disorders: A Narrative Review. Pharmaceutics 2022, 14, 305. https://doi.org/10.3390/pharmaceutics14020305
Derwich M, Lassmann L, Machut K, Zoltowska A, Pawlowska E. General Characteristics, Biomedical and Dental Application, and Usage of Chitosan in the Treatment of Temporomandibular Joint Disorders: A Narrative Review. Pharmaceutics. 2022; 14(2):305. https://doi.org/10.3390/pharmaceutics14020305
Chicago/Turabian StyleDerwich, Marcin, Lukasz Lassmann, Katarzyna Machut, Agata Zoltowska, and Elzbieta Pawlowska. 2022. "General Characteristics, Biomedical and Dental Application, and Usage of Chitosan in the Treatment of Temporomandibular Joint Disorders: A Narrative Review" Pharmaceutics 14, no. 2: 305. https://doi.org/10.3390/pharmaceutics14020305