

Bioprinted Membranes for Corneal Tissue Engineering: A Review

 , ,
, ,  ,
,  ,
,  ,
,
Abstract
:
1. Introduction
2. Corneal Anatomy and Physiology
2.1. Corneal Epithelium
2.2. Corneal Stroma
2.3. Corneal Endothelium
3. Cells
3.1. Epithelium Cells
3.2. Stroma Cells
3.3. Endothelium Cells
4. Corneal Scarring
4.1. Keratoconus
4.2. Dry Eye Disease
4.3. Bacterial Keratitis
4.4. Light and Chemical Injuries
4.5. Corneal Abrasion and Foreign Body
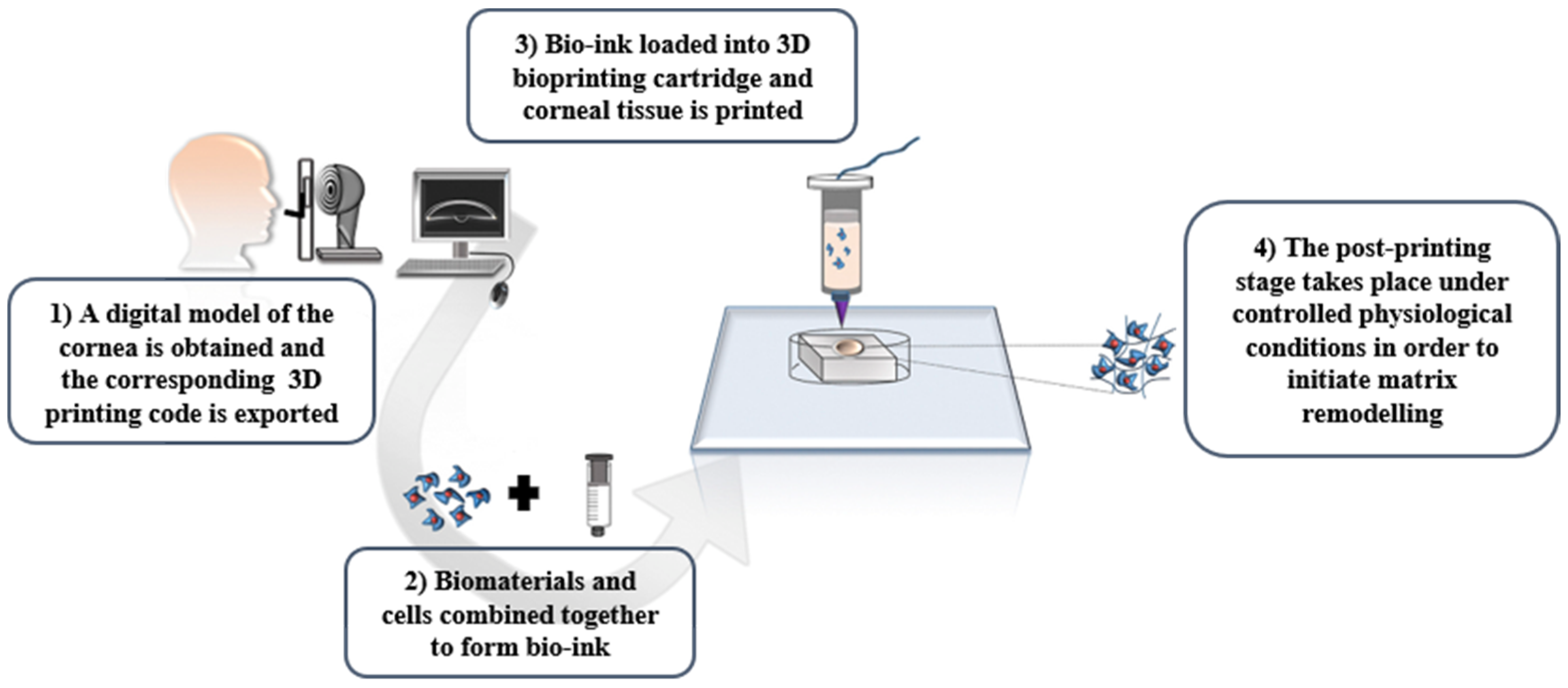
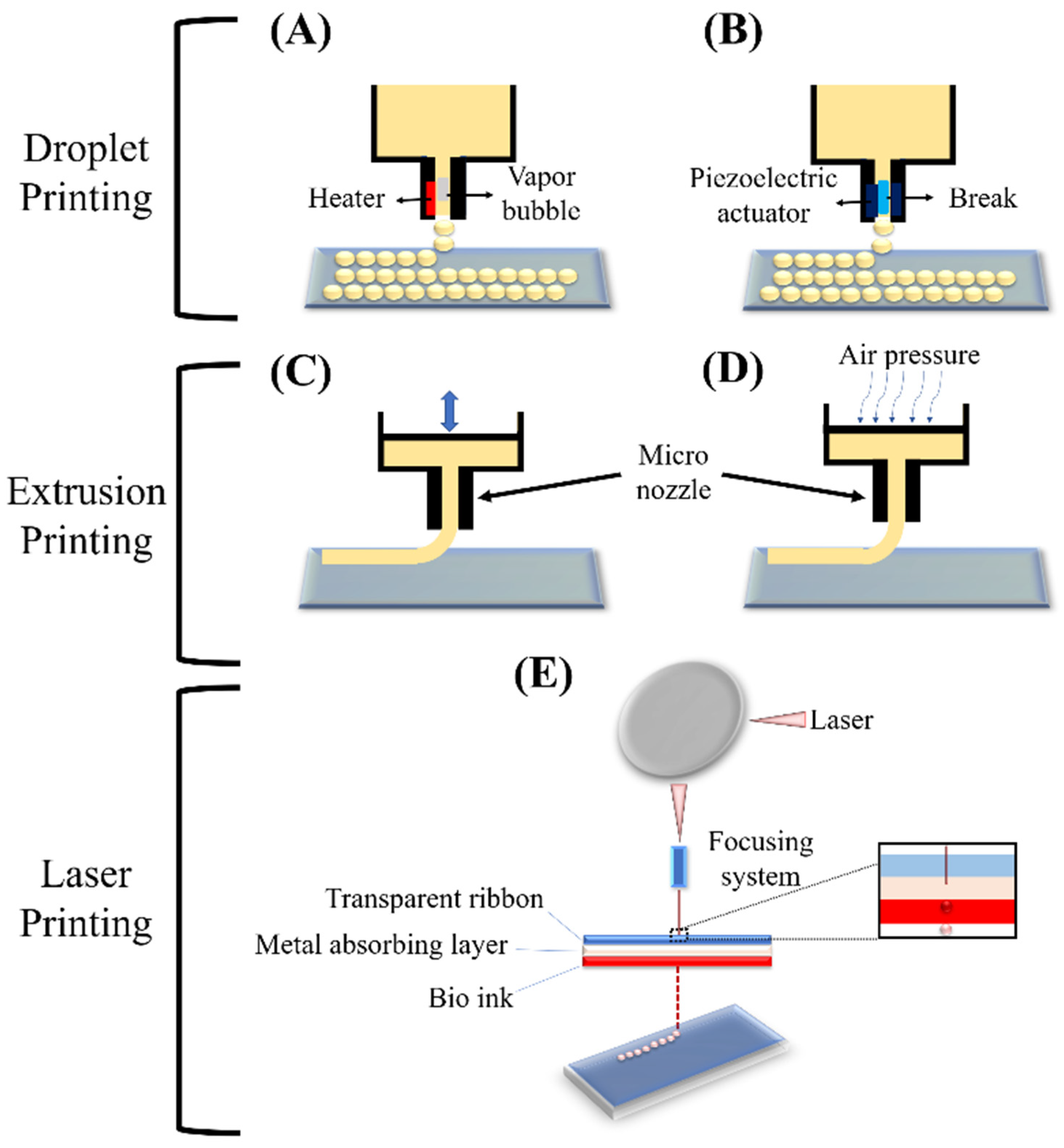
5. Three-Dimensional Bioprinting
Corneal Bioprinting
6. Nanotechnology in CTE
7. Conclusions and Future Progress
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lanza, R.; Langer, R.; Vacanti, J.P.; Atala, A. Principles of Tissue Engineering; Academic Press: Cambridge, MA, USA, 2020. [Google Scholar]
- Salehi, A.O.M.; Keshel, S.H.; Sefat, F.; Tayebi, L. Use of Polycaprolactone in Corneal Tissue Engineering: A Review. Mater. Today Commun. 2021, 27, 102402. [Google Scholar] [CrossRef]
- Goodarzi, H.; Jadidi, K.; Pourmotabed, S.; Sharifi, E.; Aghamollaei, H. Preparation and in vitro characterization of cross-linked collagen–gelatin hydrogel using EDC/NHS for corneal tissue engineering applications. Int. J. Biol. Macromol. 2019, 126, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, S.; Keshel, S.H.; Farzi, G.A.; Momeni-Moghadam, M.; Ahmadi, E.D.; Asencio, I.O.; Mozafari, M.; Sefat, F. Scaffolds for corneal tissue engineering. In Handbook of Tissue Engineering Scaffolds; Elsevier: Amsterdam, The Netherlands, 2021; Volume 2, pp. 649–672. [Google Scholar]
- Chen, Z.; You, J.; Liu, X.; Cooper, S.; Hodge, C.; Sutton, G.; Crook, J.M.; Wallace, G.G. Biomaterials for corneal bioengineering. Biomed. Mater. 2018, 13, 032002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Yan, C.; Zhu, M.; Yao, Q.; Shao, C.; Lu, W.; Wang, J.; Mo, X.; Gu, P.; Fu, Y. Electrospun nanofibrous SF/P (LLA-CL) membrane: A potential substratum for endothelial keratoplasty. Int. J. Nanomed. 2015, 10, 3337. [Google Scholar]
- Wu, Z.; Kong, B.; Liu, R.; Sun, W.; Mi, S. Engineering of corneal tissue through an aligned PVA/collagen composite nanofibrous electrospun scaffold. Nanomaterials 2018, 8, 124. [Google Scholar] [CrossRef] [Green Version]
- Akter, F. Tissue Engineering Made Easy; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Ahearne, M.; Fernández-Pérez, J.; Masterton, S.; Madden, P.W.; Bhattacharjee, P. Designing Scaffolds for Corneal Regeneration. Adv. Funct. Mater. 2020, 30, 1908996. [Google Scholar] [CrossRef] [Green Version]
- Koons, G.L.; Diba, M.; Mikos, A.G. Materials design for bone-tissue engineering. Nat. Rev. Mater. 2020, 5, 584–603. [Google Scholar] [CrossRef]
- Guérin, L.-P.; Le-Bel, G.; Desjardins, P.; Couture, C.; Gillard, E.; Boisselier, É.; Bazin, R.; Germain, L.; Guérin, S.L. The Human Tissue-Engineered Cornea (hTEC): Recent Progress. Int. J. Mol. Sci. 2021, 22, 1291. [Google Scholar] [CrossRef]
- Nosrati, H.; Abpeikar, Z.; Mahmoudian, Z.G.; Zafari, M.; Majidi, J.; Alizadeh, A.; Moradi, L.; Asadpour, S. Corneal epithelium tissue engineering: Recent advances in regeneration and replacement of the corneal surface. Regen. Med. 2020, 15, 2029–2044. [Google Scholar] [CrossRef]
- Salehi, A.O.M.; Nourbakhsh, M.S.; Rafienia, M.; Baradaran-Rafii, A.; Keshel, S.H. Corneal stromal regeneration by hybrid oriented poly (ε-caprolactone)/lyophilized silk fibroin electrospun scaffold. Int. J. Biol. Macromol. 2020, 161, 377–388. [Google Scholar] [CrossRef]
- Salehi, A.O.M.; Keshel, S.H.; Rafienia, M.; Nourbakhsh, M.S.; Baradaran-Rafii, A. Promoting keratocyte stem like cell proliferation and differentiation by aligned polycaprolactone-silk fibroin fibers containing Aloe vera. Biomater. Adv. 2022, 137, 212840. [Google Scholar] [CrossRef]
- Janmohammadi, M.; Nazemi, Z.; Salehi, A.O.M.; Seyfoori, A.; John, J.V.; Nourbakhsh, M.S.; Akbari, M. Cellulose-based composite scaffolds for bone tissue engineering and localized drug delivery. Bioact. Mater. 2023, 20, 137–163. [Google Scholar] [CrossRef] [PubMed]
- Movahedi, M.; Salehi, A.O.M.; Moezi, D.; Yarahmadian, R. In vitro and in vivo study of aspirin loaded, electrospun polycaprolactone–maltodextrin membrane for enhanced skin tissue regeneration. Int. J. Polym. Mater. Polym. Biomater. 2021, 71, 1334–1344. [Google Scholar] [CrossRef]
- Movahedi, M.; Salehi, A.O.M.; Etemad, S. Casein release and characterization of electrospun nanofibres for cartilage tissue engineering. Bull. Mater. Sci. 2022, 45, 76. [Google Scholar] [CrossRef]
- Biazar, E.; Baradaran-Rafii, A.; Heidari-Keshel, S.; Tavakolifard, S. Oriented nanofibrous silk as a natural scaffold for ocular epithelial regeneration. J. Biomater. Sci. Polym. Ed. 2015, 26, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Jeng, B.H. Indications for keratoplasty in management of corneal ectasia. Curr. Opin. Ophthalmol. 2022, 33, 318–323. [Google Scholar] [CrossRef]
- El Zarif, M.; Alió, J.L.; Alió del Barrio, J.L.; De Miguel, M.P.; Abdul Jawad, K.; Makdissy, N. Corneal stromal regeneration: A review of human clinical studies in keratoconus treatment. Front. Med. 2021, 8, 650724. [Google Scholar] [CrossRef]
- Kumar, A.; Yun, H.; Funderburgh, M.L.; Du, Y. Regenerative therapy for the Cornea. Prog. Retin. Eye Res. 2021, 87, 101011. [Google Scholar] [CrossRef]
- Ghezzi, C.E.; Rnjak-Kovacina, J.; Kaplan, D.L. Corneal tissue engineering: Recent advances and future perspectives. Tissue Eng. Part B Rev. 2015, 21, 278–287. [Google Scholar] [CrossRef] [Green Version]
- Kong, B.; Mi, S. Electrospun scaffolds for corneal tissue engineering: A review. Materials 2016, 9, 614. [Google Scholar] [CrossRef] [Green Version]
- Wicklein, V.J.; Singer, B.B.; Scheibel, T.; Salehi, S. Nanoengineered Biomaterials for Corneal Regeneration. In Nanoengineered Biomaterials for Regenerative Medicine; Elsevier: Amsterdam, The Netherlands, 2021; pp. 379–415. [Google Scholar]
- Nosrati, H.; Alizadeh, Z.; Nosrati, A.; Ashrafi-Dehkordi, K.; Banitalebi-Dehkordi, M.; Sanami, S.; Khodaei, M. Stem cell-based therapeutic strategies for corneal epithelium regeneration. Tissue Cell 2021, 68, 101470. [Google Scholar] [CrossRef] [PubMed]
- Bigham, A.; Salehi, A.O.M.; Rafienia, M.; Salamat, M.R.; Rahmati, S.; Raucci, M.G.; Ambrosio, L. Zn-substituted Mg2SiO4 nanoparticles-incorporated PCL-silk fibroin composite scaffold: A multifunctional platform towards bone tissue regeneration. Mater. Sci. Eng. C 2021, 127, 112242. [Google Scholar] [CrossRef] [PubMed]
- Ulag, S.; Uysal, E.; Bedir, T.; Sengor, M.; Ekren, N.; Ustundag, C.B.; Midha, S.; Kalaskar, D.M.; Gunduz, O. Recent developments and characterization techniques in 3D printing of corneal stroma tissue. Polym. Adv. Technol. 2021, 32, 3287–3296. [Google Scholar] [CrossRef]
- Mahdavi, S.S.; Abdekhodaie, M.J.; Mashayekhan, S.; Baradaran-Rafii, A.; Djalilian, A.R. Bioengineering approaches for corneal regenerative medicine. Tissue Eng. Regen. Med. 2020, 17, 567–593. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.; Reddy, N. Biomimetic approaches for tissue engineering. J. Biomater. Sci. Polym. Ed. 2021, 29, 1667–1685. [Google Scholar] [CrossRef] [PubMed]
- Sanie-Jahromi, F.; Eghtedari, M.; Mirzaei, E.; Jalalpour, M.H.; Asvar, Z.; Nejabat, M.; Javidi-Azad, F. Propagation of limbal stem cells on polycaprolactone and polycaprolactone/gelatin fibrous scaffolds and transplantation in animal model. BioImpacts BI 2020, 10, 45. [Google Scholar] [CrossRef] [PubMed]
- Mahdavi, S.S.; Abdekhodaie, M.J.; Kumar, H.; Mashayekhan, S.; Baradaran-Rafii, A.; Kim, K. Stereolithography 3D bioprinting method for fabrication of human corneal stroma equivalent. Ann. Biomed. Eng. 2020, 48, 1955–1970. [Google Scholar] [CrossRef] [PubMed]
- Miotto, M.; Gouveia, R.M.; Ionescu, A.M.; Figueiredo, F.; Hamley, I.W.; Connon, C.J. 4D corneal tissue engineering: Achieving time-dependent tissue self-Curvature through localized control of cell actuators. Adv. Funct. Mater. 2021, 29, 1807334. [Google Scholar] [CrossRef] [Green Version]
- Isaacson, A.; Swioklo, S.; Connon, C.J. 3D bioprinting of a corneal stroma equivalent. Exp. Eye Res. 2021, 173, 188–193. [Google Scholar] [CrossRef]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef]
- Kang, H.-W.; Lee, S.J.; Ko, I.K.; Kengla, C.; Yoo, J.J.; Atala, A. A 3D bioprinting system to produce human-scale tissue constructs with structural integrity. Nat. Biotechnol. 2016, 34, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Jeong, C.G.; Atala, A. 3D printing and biofabrication for load bearing tissue engineering. Eng. Miner. Load Bear. Tissue 2015, 881, 3–14. [Google Scholar]
- Shafiee, A.; Atala, A. Printing technologies for medical applications. Trends Mol. Med. 2016, 22, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Colaco, M.; Igel, D.A.; Atala, A. The potential of 3D printing in urological research and patient care. Nat. Rev. Urol. 2021, 15, 213. [Google Scholar] [CrossRef] [PubMed]
- Gillispie, G.J.; Han, A.; Uzun-Per, M.; Fisher, J.; Mikos, A.G.; Niazi, M.K.K.; Yoo, J.J.; Lee, S.J.; Atala, A. The Influence of Printing Parameters and Cell Density on Bioink Printing Outcomes. Tissue Eng. Part A 2020, 26, 1349–1358. [Google Scholar] [CrossRef]
- Akter, F. Principles of Tissue Engineering. In Tissue Engineering Made Easy; Elsevier: Amsterdam, The Netherlands, 2016; pp. 3–16. [Google Scholar]
- Sridhar, M.S. Anatomy of the cornea and ocular surface. Ind. J. Ophthalmol. 2021, 66, 190. [Google Scholar] [CrossRef]
- Baradaran-Rafii, A.; Biazar, E.; Heidari-Keshel, S. Cellular response of limbal stem cells on polycaprolactone nanofibrous scaffolds for ocular epithelial regeneration. Curr. Eye Res. 2016, 41, 326–333. [Google Scholar] [CrossRef]
- Palchesko, R.N.; Carrasquilla, S.D.; Feinberg, A.W. Natural biomaterials for corneal tissue engineering, repair, and regeneration. Adv. Healthc. Mater. 2021, 7, 1701434. [Google Scholar] [CrossRef]
- Islam, M.M.; Sharifi, R.; Gonzalez-Andrades, M. Corneal Tissue Engineering. In Corneal Regeneration; Springer: Berlin/Heidelberg, Germany, 2019; pp. 23–37. [Google Scholar]
- Stepp, M.A.; Tadvalkar, G.; Hakh, R.; Pal-Ghosh, S. Corneal epithelial cells function as surrogate Schwann cells for their sensory nerves. Glia 2017, 65, 851–863. [Google Scholar] [CrossRef]
- Campbell, J.D.; Ahmad, S.; Agrawal, A.; Bienek, C.; Atkinson, A.; Mcgowan, N.W.; Kaye, S.; Mantry, S.; Ramaesh, K.; Glover, A. Allogeneic Ex Vivo Expanded Corneal Epithelial Stem Cell Transplantation: A Randomized Controlled Clinical Trial. Stem Cells Transl. Med. 2021, 8, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Arabpour, Z.; Baradaran-Rafii, A.; Bakhshaiesh, N.L.; Ai, J.; Ebrahimi-Barough, S.; Esmaeili Malekabadi, H.; Nazeri, N.; Vaez, A.; Salehi, M.; Sefat, F. Design and characterization of biodegradable multi layered electrospun nanofibers for corneal tissue engineering applications. J. Biomed. Mater. Res. Part A 2021, 107, 2340–2349. [Google Scholar] [CrossRef] [PubMed]
- Hancox, Z.; Keshel, S.H.; Yousaf, S.; Saeinasab, M.; Shahbazi, M.-A.; Sefat, F. The progress in corneal translational medicine. Biomater. Sci. 2020, 8, 6469–6504. [Google Scholar] [CrossRef] [PubMed]
- Kianersi, S.; Solouk, A.; Saber-Samandari, S.; Keshel, S.H.; Pasbakhsh, P. Alginate nanoparticles as ocular drug delivery carriers. J. Drug Deliv. Sci. Technol. 2021, 66, 102889. [Google Scholar] [CrossRef]
- Fernández-Pérez, J.; Kador, K.E.; Lynch, A.P.; Ahearne, M. Characterization of extracellular matrix modified poly (ε-caprolactone) electrospun scaffolds with differing fiber orientations for corneal stroma regeneration. Mater. Sci. Eng. C 2020, 108, 110415. [Google Scholar] [CrossRef]
- Kostenko, A.; Swioklo, S.; Connon, C.J. Alginate in corneal tissue engineering. Biomed. Mater. 2022, 17, 022004. [Google Scholar] [CrossRef]
- Delaey, J.; De Vos, L.; Koppen, C.; Dubruel, P.; Van Vlierberghe, S.; Van den Bogerd, B. Tissue engineered scaffolds for corneal endothelial regeneration: A material’s perspective. Biomater. Sci. 2022, 10, 2440–2461. [Google Scholar] [CrossRef]
- Bosch, B.M.; Bosch-Rue, E.; Perpiñan-Blasco, M.; Perez, R.A. Design of functional biomaterials as substrates for corneal endothelium tissue engineering. Regen. Biomater. 2022, 9, rbac052. [Google Scholar] [CrossRef]
- Takahashi, H. Corneal endothelium and phacoemulsification. Cornea 2016, 35, S3–S7. [Google Scholar] [CrossRef]
- Eghrari, A.O.; Riazuddin, S.A.; Gottsch, J.D. Overview of the cornea: Structure, function, and development. In Progress in Molecular Biology and Translational Science; Elsevier: Amsterdam, The Netherlands, 2015; pp. 7–23. [Google Scholar]
- El Zarif, M.; del Barrio, J.L.A.; Arnalich-Montiel, F.; De Miguel, M.P.; Makdissy, N.; Alió, J.L. Corneal stroma regeneration: A new approach for the treatment of cornea disease. Asia-Pac. J. Ophthalmol. 2020, 9, 571–579. [Google Scholar] [CrossRef]
- Zhao, J.; Tian, M.; Li, Y.; Su, W.; Fan, T. Construction of tissue-engineered human corneal endothelium for corneal endothelial regeneration using a crosslinked amniotic membrane scaffold. Acta Biomater. 2022, 147, 185–197. [Google Scholar] [CrossRef]
- Kim, D.K.; Sim, B.R.; Khang, G. Nature-derived aloe vera gel blended silk fibroin film scaffolds for cornea endothelial cell regeneration and transplantation. ACS Appl. Mater. Interfaces 2016, 8, 15160–15168. [Google Scholar] [CrossRef] [PubMed]
- Sang, S.; Yan, Y.; Shen, Z.; Cao, Y.; Duan, Q.; He, M.; Zhang, Q. Photo-crosslinked hydrogels for tissue engineering of corneal epithelium. Exp. Eye Res. 2022, 218, 109027. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, S.; Jain, S. The Anatomy and Physiology of Cornea. In Keratoprostheses and Artificial Corneas; Springer: Berlin/Heidelberg, Germany, 2015; pp. 19–25. [Google Scholar]
- Binte, M.; Yusoff, N.Z.; Riau, A.K.; Yam, G.H.; Binte Halim, N.S.H.; Mehta, J.S. Isolation and propagation of human corneal stromal keratocytes for tissue engineering and cell therapy. Cells 2022, 11, 178. [Google Scholar] [CrossRef]
- Lagali, N. Corneal stromal regeneration: Current status and future therapeutic potential. Curr. Eye Res. 2020, 45, 278–290. [Google Scholar] [CrossRef] [Green Version]
- Matthyssen, S.; Van den Bogerd, B.; Dhubhghaill, S.N.; Koppen, C.; Zakaria, N. Corneal regeneration: A review of stromal replacements. Acta Biomater. 2021, 69, 31–41. [Google Scholar] [CrossRef]
- Del Barrio, J.L.A.; Arnalich-Montiel, F.; De Miguel, M.P.; El Zarif, M.; Alió, J.L. Corneal stroma regeneration: Preclinical studies. Exp. Eye Res. 2021, 202, 108314. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, L.; Zhao, J.; Liang, J.; Zhang, Z.; Li, Q.; Zhang, J.; Wan, P.; Wu, Z. Reconstructing auto tissue engineering lamellar cornea with aspartic acid modified acellular porcine corneal stroma and preconditioned limbal stem cell for corneal regeneration. Biomaterials 2022, 289, 121745. [Google Scholar] [CrossRef] [PubMed]
- Formisano, N.; van der Putten, C.; Grant, R.; Sahin, G.; Truckenmüller, R.K.; Bouten, C.V.; Kurniawan, N.A.; Giselbrecht, S. Mechanical Properties of Bioengineered Corneal Stroma. Adv. Healthc. Mater. 2021, 10, 2100972. [Google Scholar] [CrossRef] [PubMed]
- Khalili, M.; Asadi, M.; Kahroba, H.; Soleyman, M.R.; Andre, H.; Alizadeh, E. Corneal endothelium tissue engineering: An evolution of signaling molecules, cells, and scaffolds toward 3D bioprinting and cell sheets. J. Cell. Physiol. 2021, 236, 3275–3303. [Google Scholar] [CrossRef] [PubMed]
- Klyce, S.D. 12. Endothelial pump and barrier function. Exp. Eye Res. 2020, 198, 108068. [Google Scholar] [CrossRef] [PubMed]
- Atalay, E.; Özalp, O.; Yıldırım, N. Advances in the diagnosis and treatment of keratoconus. Ther. Adv. Ophthalmol. 2021, 13, 25158414211012796. [Google Scholar] [CrossRef] [PubMed]
- Tafti, M.F.; Aghamollaei, H.; Moghaddam, M.M.; Jadidi, K.; Alio, J.L.; Faghihi, S. Emerging tissue engineering strategies for the corneal regeneration. J. Tissue Eng. Regen. Med. 2022, 16, 683–706. [Google Scholar] [CrossRef] [PubMed]
- Niazi, S.; Niknejad, H.; Niazi, F.; Doroodgar, F.; Sanginabadi, A. Tissue-engineered recombinant human collagen-based corneal substitutes in end-stage keratoconus. Investig. Ophthalmol. Vis. Sci. 2021, 60, 5105. [Google Scholar]
- Sharif, R.; Priyadarsini, S.; Rowsey, T.G.; Ma, J.-X.; Karamichos, D. Corneal tissue engineering: An in vitro model of the stromal-nerve interactions of the human cornea. JoVE J. Vis. Exp. 2021, 131, e56308. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, P.; Ahearne, M. Significance of crosslinking approaches in the development of next generation hydrogels for corneal tissue engineering. Pharmaceutics 2021, 13, 319. [Google Scholar] [CrossRef]
- Qin, J.; Yin, N. Tobramycin Collagen Fast Dissolving Ocular Films for Corneal Tissue Engineering of Keratoconus. J. Biomater. Tissue Eng. 2021, 9, 804–809. [Google Scholar] [CrossRef]
- Alió del Barrio, J.L.; Alió, J.L. Cellular therapy of the corneal stroma: A new type of corneal surgery for keratoconus and corneal dystrophies. Eye Vis. 2021, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jadidi, K.; Mosavi, S.A.; Nejat, F.; Aghamolaei, H.; Pirhadi, S. Innovative intra-corneal ring-supported graft surgery for treatment of keratoconus and cornea regeneration: Surgical technique and case report. Ind. J. Ophthalmol. 2022, 70, 3412–3415. [Google Scholar]
- Teo, A.W.J.; Mansoor, H.; Sim, N.; Lin, M.T.-Y.; Liu, Y.-C. In Vivo Confocal Microscopy Evaluation in Patients with Keratoconus. J. Clin. Med. 2022, 11, 393. [Google Scholar] [CrossRef]
- Veernala, I.; Jaffet, J.; Fried, J.; Mertsch, S.; Schrader, S.; Basu, S.; Vemuganti, G.; Singh, V. Lacrimal gland regeneration: The unmet challenges and promise for dry eye therapy. Ocul. Surf. 2022, 25, 129–141. [Google Scholar] [CrossRef]
- Gong, Q.; Zhang, S.; Jiang, L.; Lin, M.; Xu, Z.; Yu, Y.; Wang, Q.; Lu, F.; Hu, L. The effect of nerve growth factor on corneal nerve regeneration and dry eye after LASIK. Exp. Eye Res. 2021, 203, 108428. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Al-Sheikh, O.; Elisseeff, J.H.; Grant, M.P. Biomaterials and tissue engineering strategies for conjunctival reconstruction and dry eye treatment. Middle East Afr. J. Ophthalmol. 2015, 22, 428. [Google Scholar] [PubMed] [Green Version]
- Hill, L.J.; Moakes, R.J.; Vareechon, C.; Butt, G.; Ng, A.; Brock, K.; Chouhan, G.; Vincent, R.C.; Abbondante, S.; Williams, R.L. Sustained release of decorin to the surface of the eye enables scarless corneal regeneration. NPJ Regen. Med. 2021, 3, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabbara, K.F.; El-Asrar, A.M.A.; Khairallah, M. Ocular Infections; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Xenoulis, P.G.; Steiner, J.M. Lipid metabolism and hyperlipidemia in dogs. Vet. J. 2010, 183, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Wang, Y.; Zhang, H.; Gao, N.; Hu, A. Limbal allografting from living-related donors to treat partial limbal deficiency secondary to ocular chemical burns. Arch. Ophthalmol. 2011, 129, 1267–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wipperman, J.; Dorsch, J.N. Evaluation and management of corneal abrasions. Am. Fam. Physician 2013, 87, 114–120. [Google Scholar] [PubMed]
- Shahid, S.M.; Harrison, N. Corneal abrasion: Assessment and management. InnovAiT 2013, 6, 551–554. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, J.; Ji, Z.; Yan, W.; Zhao, H.; Huang, W.; Liu, H. Application of Bioprinting in Ophthalmology. Int. J. Bioprinting 2022, 8, 552. [Google Scholar] [CrossRef]
- Song, Y.; Hua, S.; Sayyar, S.; Chen, Z.; Chung, J.; Liu, X.; Yue, Z.; Angus, C.; Filippi, B.; Beirne, S. Corneal bioprinting using a high concentration pure collagen I transparent bioink. Bioprinting 2022, 28, e00235. [Google Scholar] [CrossRef]
- Stafiej, P.; Küng, F.; Thieme, D.; Czugala, M.; Kruse, F.E.; Schubert, D.W.; Fuchsluger, T.A. Adhesion and metabolic activity of human corneal cells on PCL based nanofiber matrices. Mater. Sci. Eng. C 2017, 71, 764–770. [Google Scholar] [CrossRef]
- Zhang, M.; Yang, F.; Han, D.; Zhang, S.Y.; Dong, Y.; Li, X.; Ling, L.; Deng, Z.; Cao, X.; Tian, J. 3D Bioprinting of Corneal Decellularized Extracellular Matrix (CECM): GelMA Composite Hydrogel for Corneal Stroma Engineering. 2022. Available online: https://ssrn.com/abstract=4246348 (accessed on 20 October 2022).
- Kim, J.I.; Kim, J.Y.; Park, C.H. Fabrication of transparent hemispherical 3D nanofibrous scaffolds with radially aligned patterns via a novel electrospinning method. Sci. Rep. 2021, 8, 3424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chameettachal, S.; Pati, F. Preparation and Characterization of Decellularized Corneal Matrix Hydrogel for Different Clinical Indications and 3D Bioprinting Applications; RAIITH: Kirkcaldy, UK, 2022. [Google Scholar]
- Lindsay, C.D.; Roth, J.G.; LeSavage, B.L.; Heilshorn, S.C. Bioprinting of stem cell expansion lattices. Acta Biomater. 2021, 95, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Phamduy, T.B.; Sweat, R.S.; Azimi, M.S.; Burow, M.E.; Murfee, W.L.; Chrisey, D.B. Printing cancer cells into intact microvascular networks: A model for investigating cancer cell dynamics during angiogenesis. Integr. Biol. 2015, 7, 1068–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betsch, M.; Cristian, C.; Lin, Y.Y.; Blaeser, A.; Schöneberg, J.; Vogt, M.; Buhl, E.M.; Fischer, H.; Duarte Campos, D.F. Incorporating 4D into bioprinting: Real-time magnetically directed collagen fiber alignment for generating complex multilayered tissues. Adv. Healthc. Mater. 2021, 7, 1800894. [Google Scholar] [CrossRef] [PubMed]
- Leberfinger, A.N.; Dinda, S.; Wu, Y.; Koduru, S.V.; Ozbolat, V.; Ravnic, D.J.; Ozbolat, I.T. Bioprinting functional tissues. Acta Biomater. 2021, 95, 32–49. [Google Scholar] [CrossRef] [PubMed]
- Atala, A. Introduction: 3D Printing for Biomaterials; ACS Publications: Washington, DC, USA, 2020. [Google Scholar]
- Murphy, S.V.; De Coppi, P.; Atala, A. Opportunities and challenges of translational 3D bioprinting. Nat. Biomed. Eng. 2020, 4, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.T.; Bittner, S.M.; Watson, E.; Smoak, M.M.; Diaz-Gomez, L.; Molina, E.R.; Kim, Y.S.; Hudgins, C.D.; Melchiorri, A.J.; Scott, D.W. Multimaterial dual gradient three-dimensional printing for osteogenic differentiation and spatial segregation. Tissue Eng. Part A 2020, 26, 239–252. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Xue, Q.; Li, J.; Ma, L.; Yao, Y.; Ye, H.; Cui, Z.; Yang, H. 3D bioprinting for artificial cornea: Challenges and perspectives. Med. Eng. Phys. 2021, 71, 68–78. [Google Scholar] [CrossRef]
- Dubbin, K.; Tabet, A.; Heilshorn, S.C. Quantitative criteria to benchmark new and existing bio-inks for cell compatibility. Biofabrication 2017, 9, 044102. [Google Scholar] [CrossRef]
- Cidonio, G.; Glinka, M.; Dawson, J.; Oreffo, R. The cell in the ink: Improving biofabrication by printing stem cells for skeletal regenerative medicine. Biomaterials 2021, 209, 10–24. [Google Scholar] [CrossRef]
- Liu, W.; Heinrich, M.A.; Zhou, Y.; Akpek, A.; Hu, N.; Liu, X.; Guan, X.; Zhong, Z.; Jin, X.; Khademhosseini, A. Extrusion bioprinting of shear-thinning gelatin methacryloyl bioinks. Adv. Healthc. Mater. 2017, 6, 1601451. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.A.; Marquardt, L.M.; Heilshorn, S.C. The diverse roles of hydrogel mechanics in injectable stem cell transplantation. Curr. Opin. Chem. Eng. 2017, 15, 15–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernal, P.N.; Delrot, P.; Loterie, D.; Li, Y.; Malda, J.; Moser, C.; Levato, R. Volumetric bioprinting of complex living-tissue constructs within seconds. Adv. Mater. 2021, 31, 1904209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigoryan, B.; Paulsen, S.J.; Corbett, D.C.; Sazer, D.W.; Fortin, C.L.; Zaita, A.J.; Greenfield, P.T.; Calafat, N.J.; Gounley, J.P.; Ta, A.H. Multivascular networks and functional intravascular topologies within biocompatible hydrogels. Science 2021, 364, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Skylar-Scott, M.A.; Uzel, S.G.; Nam, L.L.; Ahrens, J.H.; Truby, R.L.; Damaraju, S.; Lewis, J.A. Biomanufacturing of organ-specific tissues with high cellular density and embedded vascular channels. Sci. Adv. 2021, 5, eaaw2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.; Hudson, A.; Shiwarski, D.; Tashman, J.; Hinton, T.; Yerneni, S.; Bliley, J.; Campbell, P.; Feinberg, A. 3D bioprinting of collagen to rebuild components of the human heart. Science 2021, 365, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Meek, K.M.; Knupp, C. Corneal structure and transparency. Prog. Retin. Eye Res. 2015, 49, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Mohan, R.R.; Kempuraj, D.; D’Souza, S.; Ghosh, A. Corneal stromal repair and regeneration. Prog. Retin. Eye Res. 2022, 91, 101090. [Google Scholar] [CrossRef]
- Gouveia, R.M.; Lepert, G.; Gupta, S.; Mohan, R.R.; Paterson, C.; Connon, C.J. Assessment of corneal substrate biomechanics and its effect on epithelial stem cell maintenance and differentiation. Nat. Commun. 2021, 10, 1496. [Google Scholar] [CrossRef] [Green Version]
- Sorkio, A.; Koch, L.; Koivusalo, L.; Deiwick, A.; Miettinen, S.; Chichkov, B.; Skottman, H. Human stem cell based corneal tissue mimicking structures using laser-assisted 3D bioprinting and functional bioinks. Biomaterials 2021, 171, 57–71. [Google Scholar] [CrossRef]
- Duarte Campos, D.F.; Rohde, M.; Ross, M.; Anvari, P.; Blaeser, A.; Vogt, M.; Panfil, C.; Yam, G.H.F.; Mehta, J.S.; Fischer, H. Corneal bioprinting utilizing collagen-based bioinks and primary human keratocytes. J. Biomed. Mater. Res. Part A 2021, 107, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Su, X.; Xu, Y.; Kong, B.; Sun, W.; Mi, S. Bioprinting three-dimensional cell-laden tissue constructs with controllable degradation. Sci. Rep. 2016, 6, 24474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutlehria, S.; Dinh, T.C.; Bagde, A.; Patel, N.; Gebeyehu, A.; Singh, M. High-throughput 3D bioprinting of corneal stromal equivalents. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 2981–2994. [Google Scholar] [CrossRef] [PubMed]
- Osidak, E.O.; Kozhukhov, V.I.; Osidak, M.S.; Domogatsky, S.P. Collagen as Bioink for Bioprinting: A Comprehensive Review. Int. J. Bioprinting 2020, 6, 270. [Google Scholar]
- Zhang, B.; Xue, Q.; Hu, H.-Y.; Yu, M.-F.; Gao, L.; Luo, Y.-C.; Li, Y.; Li, J.-T.; Ma, L.; Yao, Y.-F. Integrated 3D bioprinting-based geometry-control strategy for fabricating corneal substitutes. J. Zhejiang Univ. Sci. B 2021, 20, 945–959. [Google Scholar] [CrossRef]
- Bektas, C.K.; Hasirci, V. Cell loaded 3D bioprinted GelMA hydrogels for corneal stroma engineering. Biomater. Sci. 2020, 8, 438–449. [Google Scholar] [CrossRef]
- Kim, K.W.; Lee, S.J.; Park, S.H.; Kim, J.C. Ex vivo functionality of 3D bioprinted corneal endothelium engineered with ribonuclease 5-overexpressing human corneal endothelial cells. Adv. Healthc. Mater. 2021, 7, 1800398. [Google Scholar] [CrossRef]
- Kong, B.; Chen, Y.; Liu, R.; Liu, X.; Liu, C.; Shao, Z.; Xiong, L.; Liu, X.; Sun, W.; Mi, S. Fiber reinforced GelMA hydrogel to induce the regeneration of corneal stroma. Nat. Commun. 2020, 11, 1435. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Park, M.-N.; Kim, J.; Jang, J.; Kim, H.-K.; Cho, D.-W. Characterization of cornea-specific bioink: High transparency, improved in vivo safety. J. Tissue Eng. 2021, 10, 2041731418823382. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Jang, J.; Park, J.; Lee, K.-P.; Lee, S.; Lee, D.-M.; Kim, K.H.; Kim, H.K.; Cho, D.-W. Shear-induced alignment of collagen fibrils using 3D cell printing for corneal stroma tissue engineering. Biofabrication 2021, 11, 035017. [Google Scholar] [CrossRef]
- Gouveia, R.M.; Koudouna, E.; Jester, J.; Figueiredo, F.; Connon, C.J. Template curvature influences cell alignment to create improved human corneal tissue equivalents. Adv. Biosyst. 2017, 1, 1700135. [Google Scholar] [CrossRef] [PubMed]
- Trujillo-de Santiago, G.; Sharifi, R.; Yue, K.; Sani, E.S.; Kashaf, S.S.; Alvarez, M.M.; Leijten, J.; Khademhosseini, A.; Dana, R.; Annabi, N. Ocular adhesives: Design, chemistry, crosslinking mechanisms, and applications. Biomaterials 2021, 197, 345–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koppa Raghu, P.; Bansal, K.K.; Thakor, P.; Bhavana, V.; Madan, J.; Rosenholm, J.M.; Mehra, N.K. Evolution of nanotechnology in delivering drugs to eyes, skin, and wounds via topical route. Pharmaceuticals 2020, 13, 167. [Google Scholar] [CrossRef] [PubMed]
- Patra, H.K.; Azharuddin, M.; Islam, M.M.; Papapavlou, G.; Deb, S.; Osterrieth, J.; Zhu, G.H.; Romu, T.; Dhara, A.K.; Jafari, M.J.; et al. Rational Nanotoolbox with Theranostic Potential for Medicated Pro-Regenerative Corneal Implants. Adv. Funct. Mater. 2021, 29, 1903760. [Google Scholar] [CrossRef]
- Krishna, L.; Dhamodaran, K.; Jayadev, C.; Chatterjee, K.; Shetty, R.; Khora, S.S.; Das, D. Nanostructured scaffold as a determinant of stem cell fate. Stem Cell Res. Ther. 2016, 7, 188. [Google Scholar] [CrossRef]
- Motealleh, A.; Kehr, N.S. Nanocomposite hydrogels and their applications in tissue engineering. Adv. Healthc. Mater. 2017, 6, 1600938. [Google Scholar] [CrossRef] [PubMed]
- Tayebi, T.; Baradaran-Rafii, A.; Hajifathali, A.; Rahimpour, A.; Zali, H.; Shaabani, A.; Niknejad, H. Biofabrication of chitosan/chitosan nanoparticles/polycaprolactone transparent membrane for corneal endothelial tissue engineering. Sci. Rep. 2021, 11, 7060. [Google Scholar] [CrossRef]
- Chang, M.-C.; Kuo, Y.-J.; Hung, K.-H.; Peng, C.-L.; Chen, K.-Y.; Yeh, L.-K. Liposomal dexamethasone–moxifloxacin nanoparticle combinations with collagen/gelatin/alginate hydrogel for corneal infection treatment and wound healing. Biomed. Mater. 2020, 15, 055022. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F.J.; De La Fuente, M.; Merayo, J.; Durán, J.; Orive, G. Plasma rich in growth factors for the treatment of ocular surface diseases. Curr. Eye Res. 2016, 41, 875–882. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Corneal Layer | Bioprinting Method | Material | Cell Source | Results | Ref. |
|---|---|---|---|---|---|
| Stroma | Extrusion | ALG, COL bioink, FRESH support | CKCs |
| [33] |
| Laser | Matrigel, COL bioink | LECs |
| [112] | |
| Extrusion | COL, dC | CKCs |
| [121] | |
| Droplet | COL, AG | CKCs |
| [113] | |
| Extrusion | GelMa, reinforced with PEG, PCL Fibers | LSSCs |
| [120] | |
| Extrusion | GelMa | CKCs |
| [118] | |
| Extrusion | dC | CKCs |
| [122] | |
| Endothelium | Extrusion | Gelatin, RGD bioink, amniotic membrane dC support | CECs |
| [119] |
| Epithelium | Extrusion | GelMa bioink, GelMa dome-shaped mold | CEpCs |
| [117] |
| Extrusion | ALG, GelMa, COL | CEpCs |
| [114] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orash Mahmoud Salehi, A.; Heidari-Keshel, S.; Poursamar, S.A.; Zarrabi, A.; Sefat, F.; Mamidi, N.; Behrouz, M.J.; Rafienia, M. Bioprinted Membranes for Corneal Tissue Engineering: A Review. Pharmaceutics 2022, 14, 2797. https://doi.org/10.3390/pharmaceutics14122797
Orash Mahmoud Salehi A, Heidari-Keshel S, Poursamar SA, Zarrabi A, Sefat F, Mamidi N, Behrouz MJ, Rafienia M. Bioprinted Membranes for Corneal Tissue Engineering: A Review. Pharmaceutics. 2022; 14(12):2797. https://doi.org/10.3390/pharmaceutics14122797
Chicago/Turabian StyleOrash Mahmoud Salehi, Amin, Saeed Heidari-Keshel, Seyed Ali Poursamar, Ali Zarrabi, Farshid Sefat, Narsimha Mamidi, Mahmoud Jabbarvand Behrouz, and Mohammad Rafienia. 2022. "Bioprinted Membranes for Corneal Tissue Engineering: A Review" Pharmaceutics 14, no. 12: 2797. https://doi.org/10.3390/pharmaceutics14122797