1. Introduction
Allogeneic hematopoietic cell transplantation (HCT) is used to treat many malignant and non-malignant disorders in children. Preparative drug regimens prior to HCT commonly utilize the nucleoside analogue fludarabine, which possesses both antileukemic activity and strong immunosuppressive activity that potentially enhances stem cell engraftment. After fludarabine phosphate is infused, it is rapidly dephosphorylated to form the principle circulating metabolite f-ara-a, which then enters the cells via nucleoside membrane transporters and is eventually phosphorylated into the cytotoxic, active form f-ara-ATP. While drug toxicity is less concerning with f-ara-a when compared with busulfan, cyclophosphamide and other myeloablative alkylating agents, f-ara-a exposure variability is still potentially linked with poor transplant outcomes including nonrelapse mortality and impaired immune reconstitution. Additionally, fludarabine neurotoxicity is a rare but serious complication of fludarabine which is thought to be dose-dependent [
1].
Our understanding of f-ara-a pharmacokinetics (PK) in pediatrics has been based on limited data generated from two clinical trials including a limited sample size, excluding children <1 year of age, and treating patients concomitantly with cytarabine in the context of relapsed leukemias [
2,
3]. Within the adult population, studies of f-ara-a PK in HCT populations found that patient specific covariates, including body weight and renal function (two covariates of great variability within the pediatric population), impact estimations of f-ara-a clearance (CL) [
4,
5,
6]. Recent studies have corroborated that body weight and renal function impact f-ara-a exposure within the pediatric population [
7,
8]. Both studies developed population PK models from which individualized f-ara-a doses can be generated for pediatric patients [
7,
8]. Additionally, in the Ivaturi model characterized both f-ara-a as well as it intracellular, active f-ara-ATP concentrations in peripheral blood mononuclear cells. They found that with each additional consecutive daily dose of fludarabine, intracellular concentrations of f-ara-ATP decrease while circulating f-ara-a concentrations remain consistent, suggesting a degree of saturation in the transport of f-ara-a intracellularly [
8].
Beyond population PK model development, evaluation of optimal f-ara-a exposure has also found early agreement within the literature. In a previous study published by our group, pediatric subjects with f-ara-a cumulative area-under-the-curve (cAUC) above 15 mg*h/L and below 19 mg*h/L had the highest probability of a positive outcome for patients transplanted for malignancy, while no such trend was readily apparent within the limited set of subjects transplanted for nonmalignant conditions [
8]. Though PK parameters were well estimated and goodness of fit (GOF) plots were acceptable, high residual unexplained variability remained within this model [
8]. In a study including pediatric and adult subjects, optimal f-ara-a exposure was found to be 20 mg*h/L with those who experienced supratherapeutic exposures having increased risk of impaired immune reconstitution and those who experienced subtherapeutic exposures having increased risk of nonrelapse mortality and graft failure [
9]. Improved event-free survival was found at the optimal f-ara-a exposure for both malignant and non-malignant disorders [
9].
The aim of the current study was to validate and refine the pediatric population PK model, previously developed by our group utilizing sparse PK sampling in a prospective multicenter pediatric clinical trial [
8]. The second aim was to compare f-ara-a exposure variability between patients dosed based on model informed dosing and those receiving fludarabine dosing based on weight or body surface area (BSA).
2. Materials and Methods
Patients recruited to participate in the study met protocol-specific eligibility criteria for transplantation, planned to undergo an allogeneic or autologous HCT that included intravenous fludarabine phosphate as part of the conditioning regimen, and included pediatric (0–17 years old) or young adult (18–22 years old). Participating HCT centers included the University of California, San Francisco (UCSF), UCSF Benioff Children’s Hospital of Oakland, University of Minnesota, and Rady Children’s Hospital San Diego were recruited between October 2019 and February 2022. F-ara-a dosing strategies employed were institution-specific; patient enrollment in this study did not change the clinical course of HCT. UCSF was the only center to utilize the Ivaturi model for Model Based Dosing (MBD) of f-ara-a via a Bayesian dosing estimation platform (InsightRX Nova) [
8]. Patient renal function was assessed by estimation of creatinine clearance (CrCL) via the Bedside Schwartz equation for patients under 17 years old and the Cockcroft-Gault equation for those over 18 years old, and CrCL estimates were capped at 150 mL/min/1.73 m
2 prior to use within the popPK model. Pediatric fat-free mass was estimated for patients over 3 years old and under 18 years old using the method published by Al-Sallami et al. [
10].
For MBD, the clinical team used patient-specific information and cAUC targets ranging from 16–20 mg*h/L to generate the f-ara-a dosing regimen for each patient. Dosing strategies employed by contributing sites, and for a minority of patients from UCSF, included BSA-based dosing (mg/m2) for patients greater than 10 kg or 2 years of age and weight-based dosing (mg/kg) for individuals less than 10 kg or 2 years of age. F-ara-a doses were given every 24 h from three to five days, depending on the patient’s conditioning regimen.
Given the rich sampling strategy utilized to build the original popPK model, plasma f-ara-a concentrations were collected using a sparse sampling strategy, with two measurements drawn per patient, to minimize extraneous blood draws for patients during HCT. The first f-ara-a concentration was drawn 0–2 h after the end of infusion, and the second f-ara-a concentration was drawn any time 2–24 h after the end of infusion. Draws were timed to optimize clinical care of the patients during HCT, and specific times of collection were recorded for each patient draw. Patient characteristics were collected at the time of transplant that included age, gender, ethnicity, total body weight, height, and markers of renal function. Transplant-specific characteristics included diagnosis, conditioning regimen, stem cell source, and degree of HLA mismatch. Patient information was uploaded by HCT center research coordinators and stored in a secure REDCap database. Plasma samples were analyzed for f-ara-a using a previously validated liquid chromatography-tandem mass spectrometry method [
11]. The F-ara-A assay was linear in the range of 2 ng/mL to 800 ng/mL. During the sample analysis, the mean accuracies (mean ± coefficient of variation) of the f-ara-a assay were 100.7% ± 8.3, 103.7% ± 8.6, and 101.2% ± 11.8 at low-, medium-, and high-quality control levels, respectively.
Software utilized to validate and refine the previously published model included NONMEM v7.5 (ICON), Perl Speaks NONMEM v4.8.1, and PiranaJS (beta version). For model refinement, the prospective data set was added to the original data set to make a combined data set. Determination of the model with the best fitness was based on –2 × log likelihood which is presented by NONMEM as the objective function value (OFV). When comparing models, a difference in the OFV of (dOFV) of 3.84, 7.88, and 10.83 are considered significant at the 0.05, 0.005, and 0.001 levels, respectively. Beyond dOFV comparisons, goodness-of-fit (GOF) plots and prediction corrected visual predictive checks (VPC) were utilized to assess model fitness. The precision of the final refined model parameters was evaluated by performing a 1000 non-parametric bootstrap analysis and reporting the 95% confidence intervals (CI) for each parameter.
Simulations were run to compare the original and refined models’ accuracy in attaining a cAUC target of 20 mg·h/L in individuals aged less than 2 years old and individuals with a body mass index (BMI) greater than 30 kg/m
2. The simulated data sets included 1000 individuals, assigning height and weight according to age and sex as described in growth curve distributions listed by the Centers for Disease Control [
12]. For both the refined and original model, 4 doses were assigned according to the typical model estimate of clearance, and f-ara-a cAUC was then predicted by NONMEM utilizing the refined model.
Variance in model-generated predicted cAUCs were statistically compared between patients who received a traditional dosing strategy and those who received MBD utilizing Levene’s test. Additionally, a descriptive evaluation of model accuracy was made. The current prospective data set was combined with the original model building data set prior to model refinement.
3. Results
Of those eligible, a total of 53 patients consented to participate in this study for model validation, with subject demographics summarized in
Table 1. This sample of subjects had median age of 8.0 years with seven individuals
2 years old (13%), and a median weight of 23.6 kg. Of the 53 subjects, 24 received MBD while 29 received traditional weight or BSA based dosing of f-ara-a.
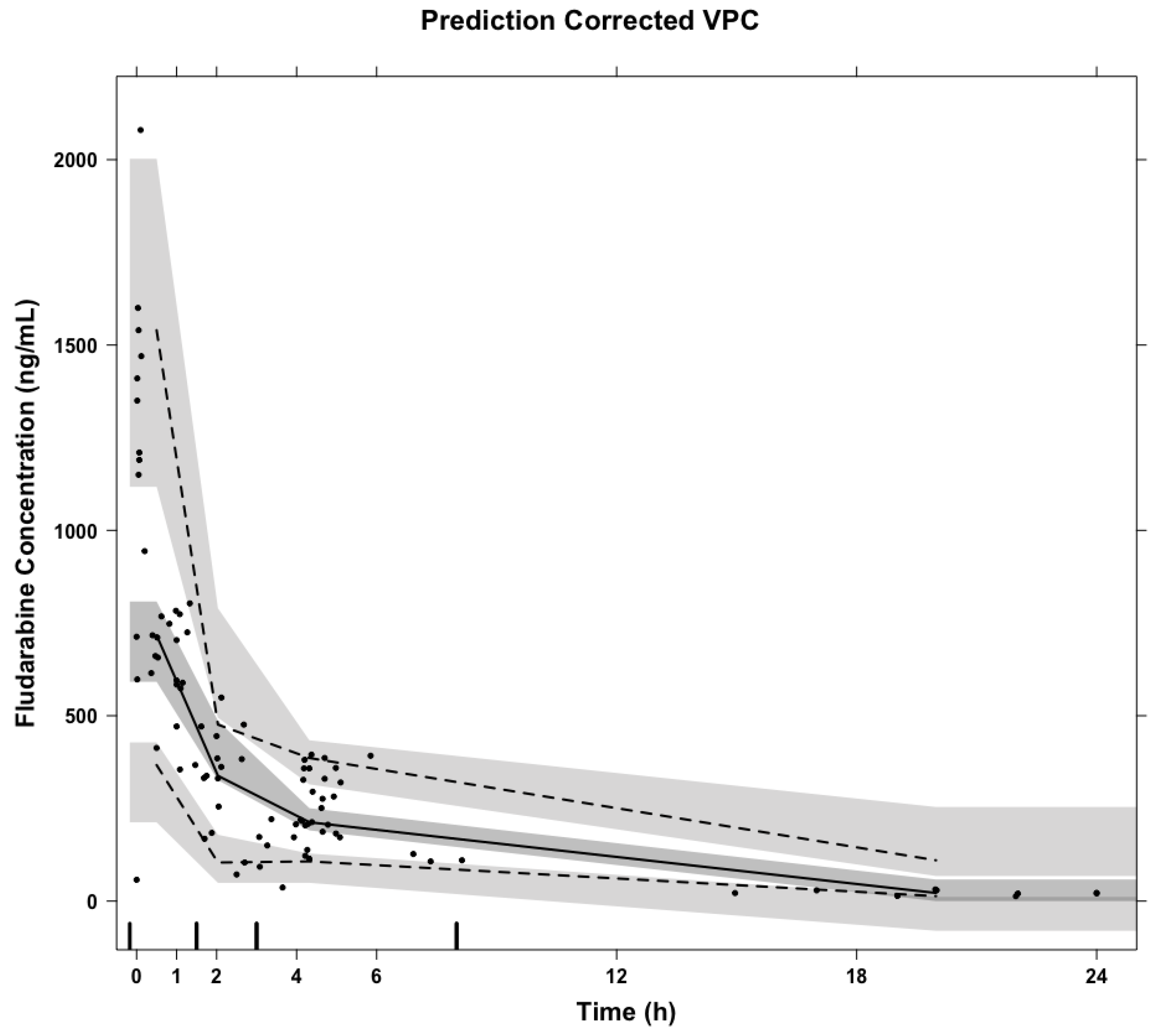
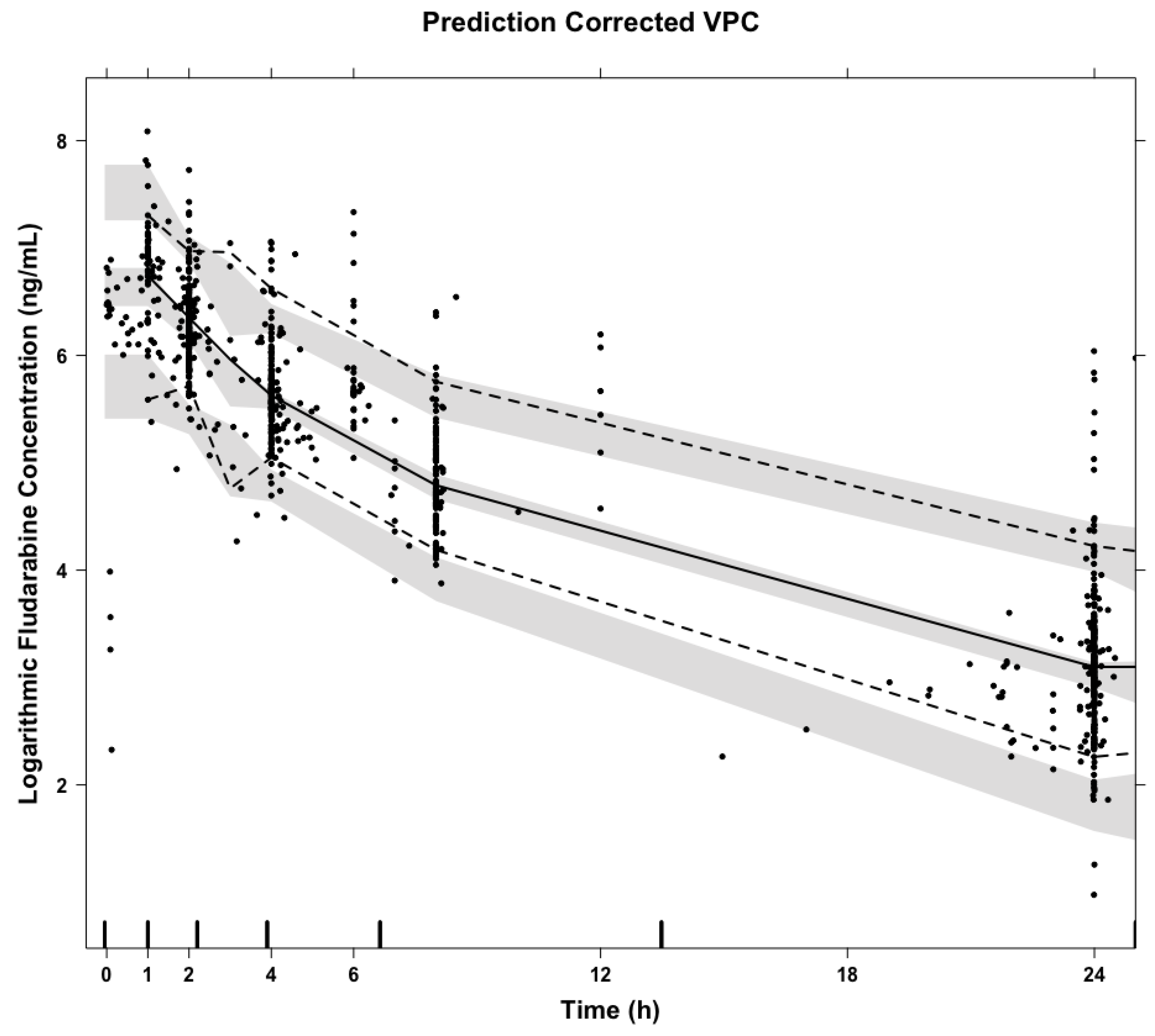
A total of 101 f-ara-a concentrations were quantifiable and utilized in model validation and refinement. A prediction corrected VPC of concentrations over time after dose suggests the popPK model well-predicted the concentrations observed in this prospective data set (
Figure 1). The total percent error of model-predicted concentrations was 6.72% as calculated by Equation (1).
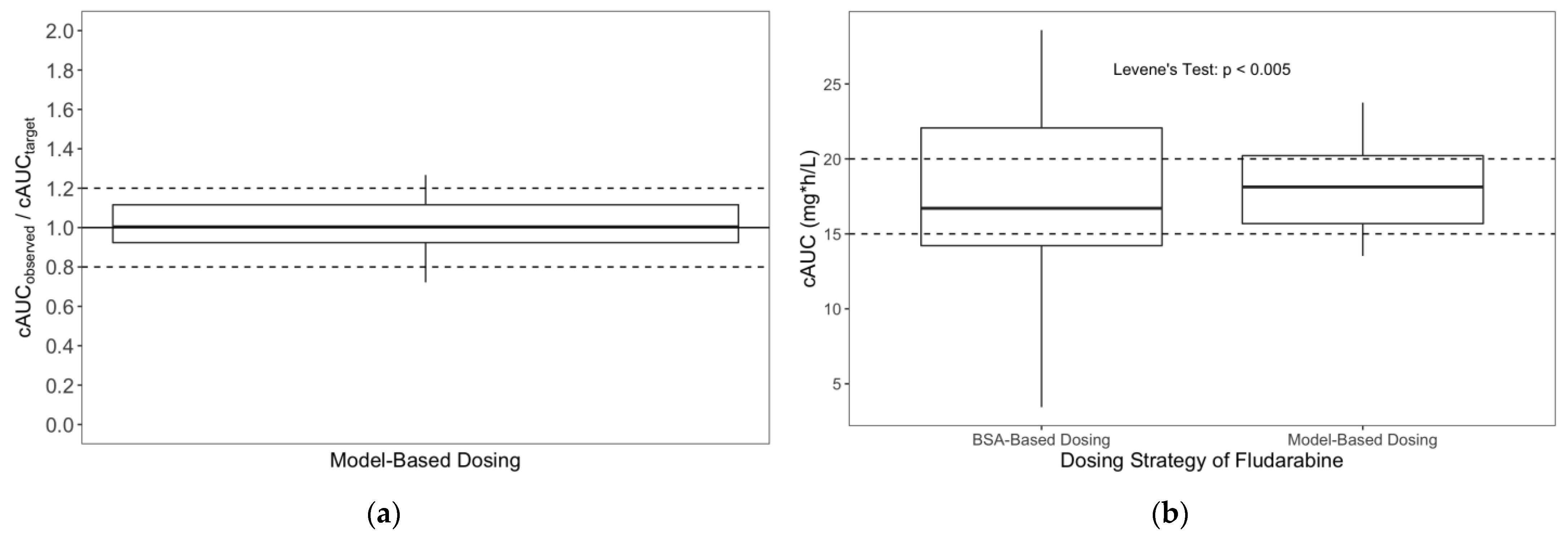
For the 24 subjects who received MBD targeting a specific cAUC goal, model accuracy was evaluated as the percentage difference of predicted cAUC to goal cAUC. The model’s median accuracy was 94% (range: 67–118%).
A comparison of variance between f-ara-a cAUCs between those who received MBD versus those who received traditional f-ara-a dosing via Levene’s test found the two groups had statistically different variance (
p < 0.005). MBD resulted in more precise attainment of f-ara-a cAUC when compared with traditional dosing strategies (
Figure 2).
Since the current data set only contains sparse f-ara-a concentrations and no f-ara-ATP concentrations, the parameters of intracellular compartment described in the original model were fixed and not further estimated. Addition of a maturation function, as defined by Equation (2),
where
is an estimated parameter that impact the shape of the exponential curve, on CL was found to significantly improve the model (dOFV-12.3). Additionally, replacing weight with fat-free mass significantly improved model fit (dOFV-11). Accounting for participant ancestry within the model did not improve the model fit. The refined model for f-ara-a CL is presented in Equation (3):
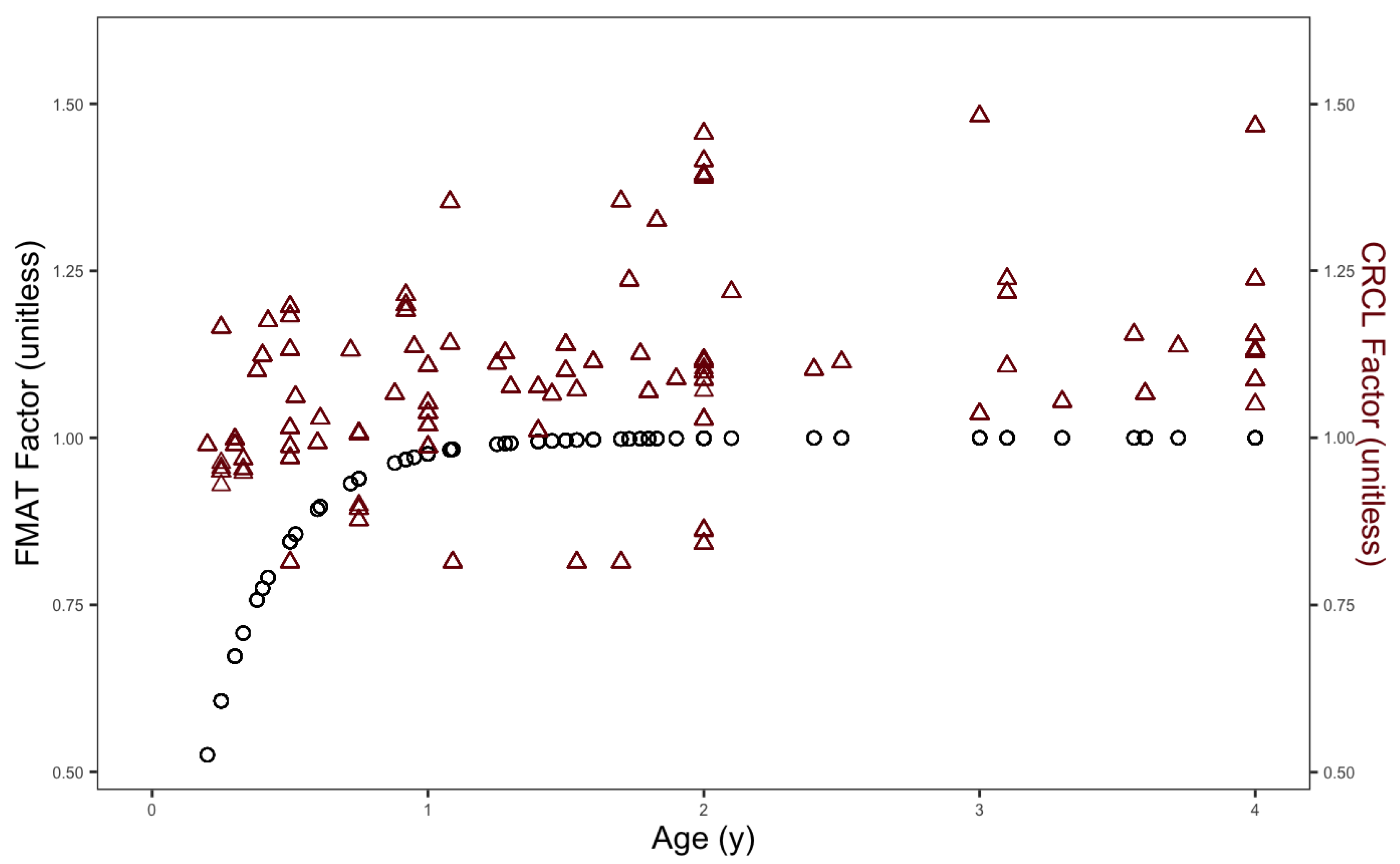
Given the primary renal clearance of f-ara-a, both the factors accounting for CrCL and maturation function in the overall f-ara-a CL are reflective of renal function; however, the maturation function is thought to account for development related factors impacting f-ara-a clearance not detectable by the approximation of CrCL as seen in
Figure 3. Final refined model parameter estimates are included in
Table 2 and a prediction corrected visual predictive check of the refined model is included in
Appendix A.
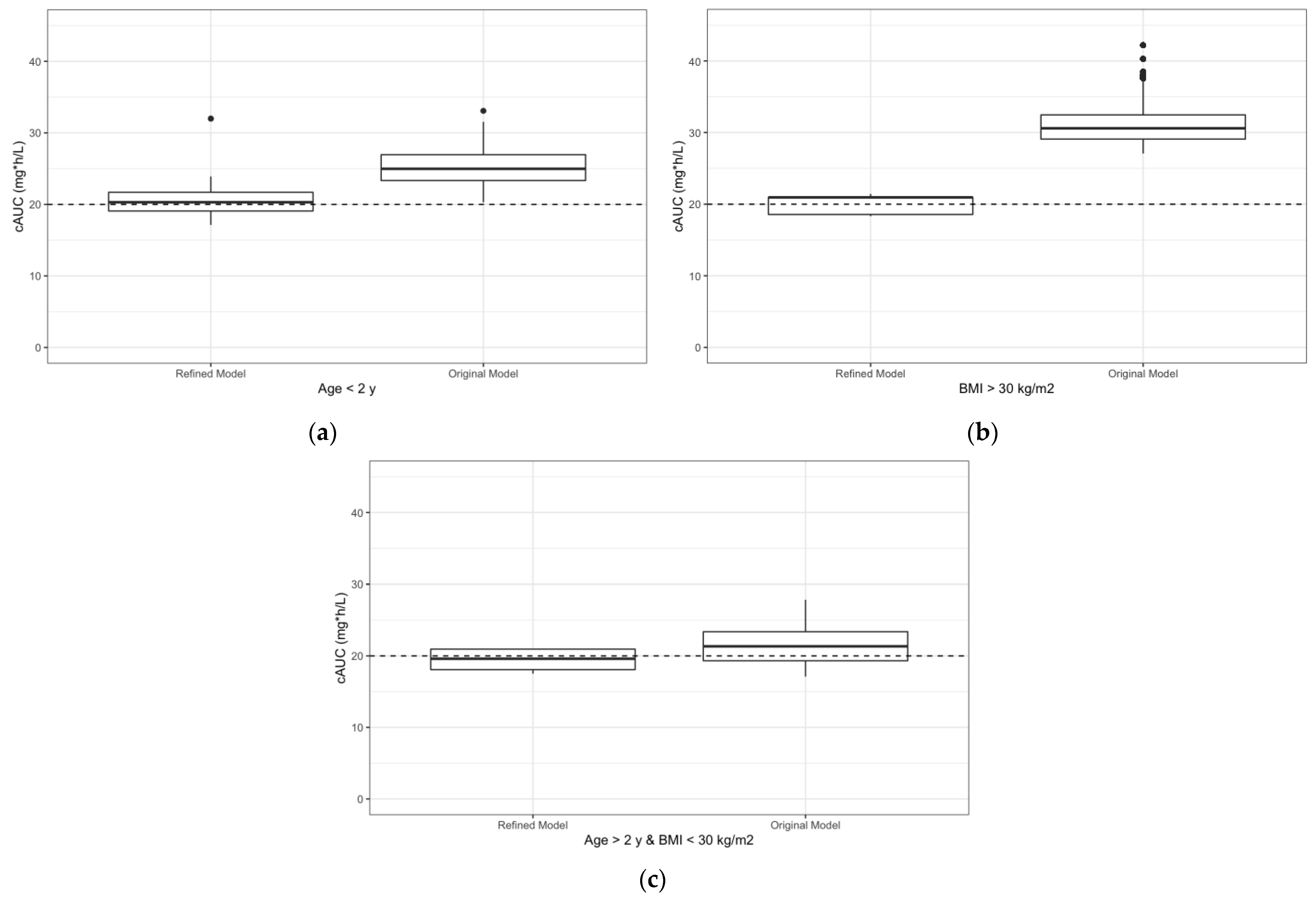
The simulated data suggest that the refined model doses improved the likelihood for achieving a specific exposure for both individuals less than 2 years old and for those with BMI greater than 30 kg/m
2 (
Figure 4). For individuals less than 2 years old, doses assigned by the refined model resulted in a predicted cAUC median (range) of 20.3 (17.1–32.0), whereas doses assigned by the original model resulted in a predicted cAUC median (range) of 25.0 (20.3–33.0). For individuals with a BMI greater than 30 kg/m
2, doses assigned by the refined model resulted in a predicted cAUC median (range) of 20.9 (18.3–21.4), whereas doses assigned by the original model resulted in a predicted cAUC median (range) of 30.6 (27.1–42.2).
4. Discussion
As popPK models are developed and translated into clinical practice, it is imperative that they are both prospectively validated with new data not utilized to develop the model and refined with the increased sample size that comes with the validation process. This is especially important when implementing popPK-based, precision dosing within vulnerable populations which generally have sample size limitations and large pharmacologic variability.
In terms of validation, the previously published f-ara-a popPK model captures the prospectively observed f-ara-a concentrations well, which is particularly notable given the lack of therapeutic drug monitoring available to adjust between doses. Unlike other medications often used in conjunction with fludarabine such as busulfan, the patient-specific PK parameter estimates appear to stay quite consistent over the course of f-ara-a administration. While busulfan is metabolized by the liver and its clearance is susceptible to drug–drug interactions and its own hepatotoxic effects, fludarabine is renally eliminated and its clearance appears consistent across its course of administration. Based on the evidence present in this study, there is likely minimal benefit to recommending therapeutic drug monitoring for f-ara-a at this time, as target exposures were easily attained with the initial dose estimate suggested by the model. Compared with traditional dosing strategies, utilizing MBD via the described model improves the precision of f-ara-a cAUC attainment. In particular, MBD avoids the extreme cAUC lows and highs previously associated with worse clinical outcomes [
9].
While the original popPK model performed well with patients greater tha 2 years of age and with normal BMIs, the additional f-ara-a PK data measured in this study particularly enabled us to study differences within f-ara-a PK within children under 2 years of age and patients with higher BMIs. The expansion of participants less than 2 years of age enabled us to approximate a maturation function on f-ara-a CL that describes how CL increases particularly over the first year of life. Caution should be used in applying the developed maturation function in individuals younger than 5 months of age given this is the model has not been validated for such individuals and, therefore, the model could suggest an erroneously low dose of fludarabine. While not a mechanistic description, the maturation function is in alignment with f-ara-a being primarily cleared renally and that kidney maturation of infants typically reaches adult equivalence by ~1–2 years of age [
13]. Further work to characterize the specific mechanisms of renal CL including the contributions of glomerular filtration and active tubular secretion is warranted. Beyond characterizing a maturation function on CL, replacing weight with fat-free mass on estimates of CL, Vc, Intercompartmental CL, and Vp additionally improved the model. This suggests f-ara-a does not likely partition into adipose tissue and, therefore, excess mass contributed by fat minimally impacts f-ara-a exposure and distribution in the body. Adopting fat-free mass into the model will enable us to improve dose recommendations for high BMI individuals, preventing doses which are erroneously and disproportionally too high.
Given improvement in model fit after including maturation function and fat-free mass as well as re-estimating the PK parameters with the expanded data set, the model accuracy is expected to improve in use within future patients. While patient-reported ancestry information was initially explored, it was not incorporated in the final refined model at this time. Furthermore, inclusion of ancestry factors needs to be completed in an equitable manner, supported by a more robust pharmacogenetic analysis.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}