
Pulmonary Delivery of Favipiravir in Rats Reaches High Local Concentrations without Causing Oxidative Lung Injury or Systemic Side Effects
 , ,
, ,  ,
,  , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals and Chemicals
2.2. Experimental Design
2.3. Measurement of Myeloperoxidase Activity in Lung Tissue Samples
2.4. Measurement of Lipid Peroxidation and Glutathione Levels in Lung Tissue Samples
2.5. Measurement of Favipiravir Level in the Plasma and Lung Tissue Samples
2.6. Histological Analysis
2.7. Statistical Analysis
3. Results
3.1. Effect of Inhaled Favipiravir on Blood Cell Counts and Hepatic and Renal Function Tests
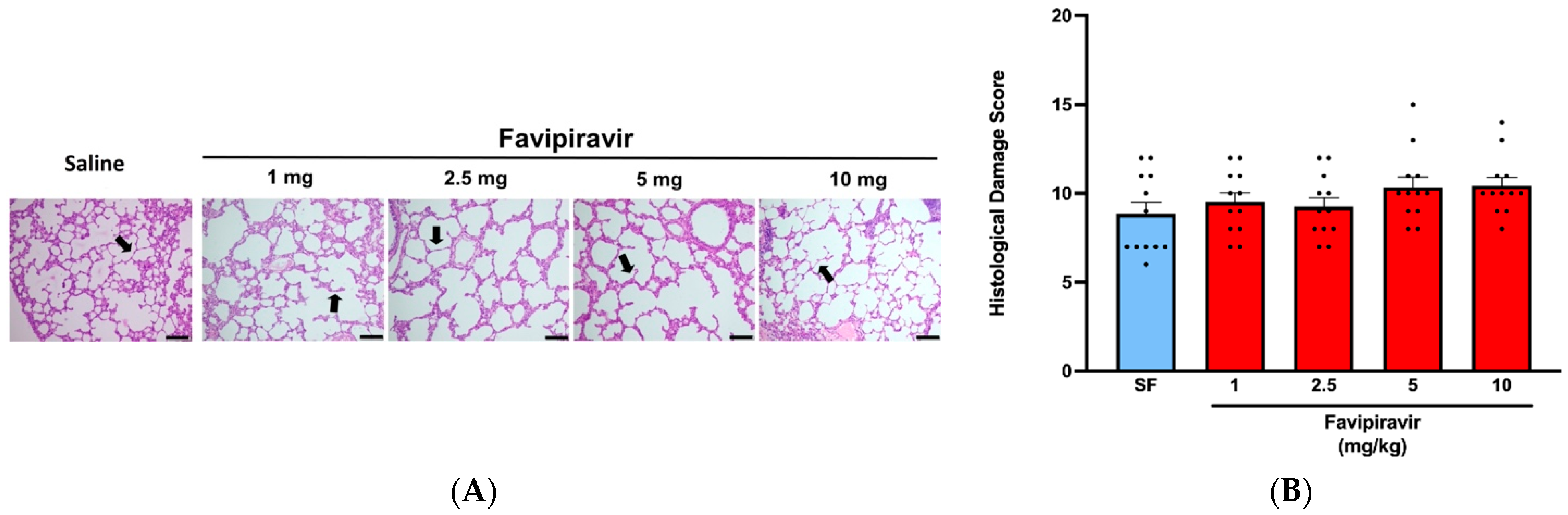
3.2. Effect of Inhaled Favipiravir on Levels of Malondialdehyde, Glutathione, Myeloperoxidase Activity and Histological Appearance of Lung Tissues
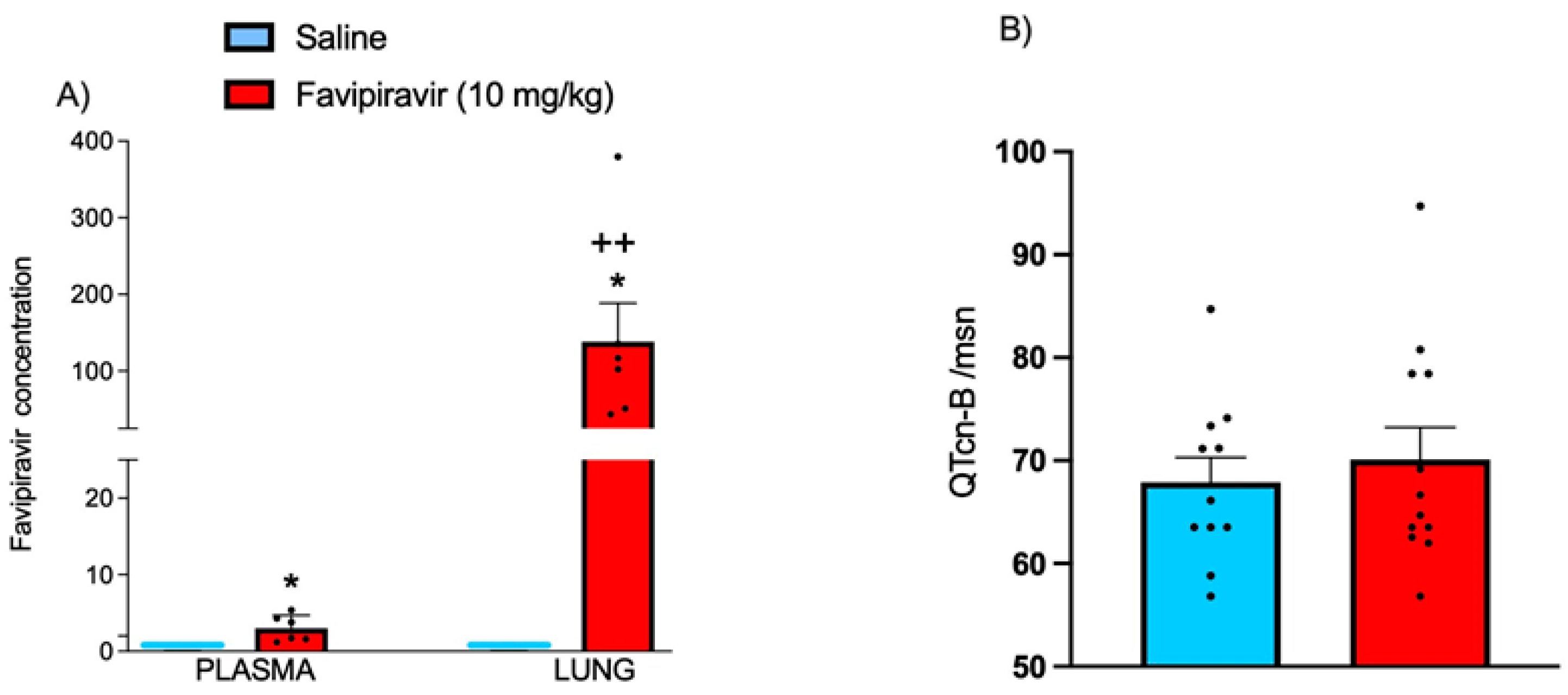
3.3. Plasma and Lung Tissue Levels of Favipiravir and QT Intervals on ECG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EC50 | half-maximal effective concentration |
| CC50 | half-cytotoxic concentration |
| SI | selectivity index |
| b.i.d | twice a day |
| q.d. | once a day |
References
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Walker, K.D.O. SARS-CoV-2 Vaccine. Glob. Reprod. Health Winter 2020, 5, e42. [Google Scholar] [CrossRef] [PubMed]
- Lythgoe, M.P.; Middleton, P. Ongoing clinical trials for the management of the COVID-19 pandemic. Trends Pharmacol. Sci. 2020, 41, 363–382. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.J.; Bergeron, E.; Benjannet, S.; Erickson, B.R.; Rollin, P.E.; Ksiazek, T.G.; Seidah, N.G.; Nichol, S.T. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol. J. 2005, 2, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahoo, B.M.; Ravi Kumar, B.; Sruti, J.; Mahapatra, M.K.; Banik, B.K.; Borah, P. Drug repurposing strategy (DRS): Emerging approach to identify potential therapeutics for treatment of novel coronavirus infection. Front. Mol. Biosci. 2021, 8, 628144. [Google Scholar] [CrossRef]
- Chang, R.Y.K.; Chow, M.Y.; Khanal, D.; Chen, D.; Chan, H.-K. Dry powder pharmaceutical biologics for inhalation therapy. Adv. Drug Deliv. Rev. 2021, 172, 64–79. [Google Scholar] [CrossRef]
- Joshi, S.; Parkar, J.; Ansari, A.; Vora, A.; Talwar, D.; Tiwaskar, M.; Patil, S.; Barkate, H. Role of favipiravir in the treatment of COVID-19. Int. J. Infect. Dis. 2021, 102, 501–508. [Google Scholar] [CrossRef]
- Kumagai, Y.; Murakawa, Y.; Hasunuma, T.; Aso, M.; Yuji, W.; Sakurai, T.; Noto, M.; Oe, T.; Kaneko, A. Lack of effect of favipiravir, a novel antiviral agent, on QT interval in healthy Japanese adults. Int. J. Clin. Pharmacol. Ther. 2015, 53, 866–874. [Google Scholar] [CrossRef]
- Agrawal, U.; Raju, R.; Udwadia, Z.F. Favipiravir: A new and emerging antiviral option in COVID-19. Med. J. Armed Forces India 2020, 76, 370–376. [Google Scholar] [CrossRef]
- Bai, C.-Q.; Mu, J.-S.; Kargbo, D.; Song, Y.-B.; Niu, W.-K.; Nie, W.-M.; Kanu, A.; Liu, W.-W.; Wang, Y.-P.; Dafae, F. Clinical and virological characteristics of Ebola virus disease patients treated with favipiravir (T-705)—Sierra Leone, 2014. Clin. Infect. Dis. 2016, 63, 1288–1294. [Google Scholar] [CrossRef]
- Sissoko, D.; Laouenan, C.; Folkesson, E.; M’lebing, A.-B.; Beavogui, A.-H.; Baize, S.; Camara, A.-M.; Maes, P.; Shepherd, S.; Danel, C. Experimental treatment with favipiravir for Ebola virus disease (the JIKI Trial): A historically controlled, single-arm proof-of-concept trial in Guinea. PLoS Med. 2016, 13, e1001967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.X.; Chen, X.P. Favipiravir: Pharmacokinetics and concerns about clinical trials for 2019-nCoV infection. Clin. Pharmacol. Ther. 2020, 108, 242–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çap, M.; Bilge, Ö.; Işık, F.; Burak, C.; Karagöz, A.; İnci, Ü.; Akyüz, A.; Aslan, B.; Altıntaş, B.; Altındağ, R. The effect of favipiravir on QTc interval in patients hospitalized with coronavirus disease 2019. J. Electrocardiol. 2020, 63, 115–119. [Google Scholar] [CrossRef] [PubMed]
- James Ives, M. Preliminary Report of Favipiravir Observational Study in Japan Released; Favipiravir Observational Study Group: Fujita, Japan, 2020. [Google Scholar]
- Chinello, P.; Petrosillo, N.; Pittalis, S.; Biava, G.; Ippolito, G.; Nicastri, E.; INMI Ebola Team. QTc interval prolongation during favipiravir therapy in an Ebolavirus-infected patient. PLoS Negl. Trop. Dis. 2017, 11, e0006034. [Google Scholar] [CrossRef] [Green Version]
- Haghjoo, M.; Golipra, R.; Kheirkhah, J.; Golabchi, A.; Shahabi, J.; Oni-Heris, S.; Sami, R.; Tajmirriahi, M.; Saravi, M.; Khatami, M. Effect of COVID-19 medications on corrected QT interval and induction of torsade de pointes: Results of a multicenter national survey. Int. J. Clin. Pract. 2021, 75, e14182. [Google Scholar] [CrossRef]
- Sodeifian, F.; Seyedalhosseini, Z.S.; Kian, N.; Eftekhari, M.; Najari, S.; Mirsaeidi, M.; Farsi, Y.; Nasiri, M.J. Drug-induced liver injury in COVID-19 patients: A systematic review. Front. Med. 2021, 8, 731436. [Google Scholar] [CrossRef]
- Yamazaki, S.; Suzuki, T.; Sayama, M.; Nakada, T.-a.; Igari, H.; Ishii, I. Suspected cholestatic liver injury induced by favipiravir in a patient with COVID-19. J. Infect. Chemother. 2021, 27, 390–392. [Google Scholar] [CrossRef]
- Corritori, S.; Savchuk, N.; Pauza, C.D. Risk/Benefit Profiles of Currently Approved Oral Antivirals for Treatment of COVID-19: Similarities and Differences. COVID 2022, 2, 1057–1076. [Google Scholar] [CrossRef]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part I: Physiological factors affecting therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 56, 588–599. [Google Scholar] [CrossRef]
- Valiulin, S.V.; Onischuk, A.A.; Dubtsov, S.N.; Baklanov, A.M.; An’kov, S.V.; Plokhotnichenko, M.E.; Tolstikova, T.G.; Dultseva, G.G.; Rusinov, V.L.; Charushin, V.N. Aerosol inhalation delivery of triazavirin in mice: Outlooks for advanced therapy against novel viral infections. J. Pharm. Sci. 2021, 110, 1316–1322. [Google Scholar] [CrossRef]
- Sahakijpijarn, S.; Moon, C.; Koleng, J.J.; Christensen, D.J.; Williams Iii, R.O. Development of remdesivir as a dry powder for inhalation by thin film freezing. Pharmaceutics 2020, 12, 1002. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, B.E.; Wyde, P.R.; Wilson, S.Z.; Meyerson, L.R. SP-303 small-particle aerosol treatment of influenza A virus infection in mice and respiratory syncytial virus infection in cotton rats. Antivir. Res. 1993, 21, 37–45. [Google Scholar] [CrossRef]
- Wachtel, H.; Kattenbeck, S.; Dunne, S.; Disse, B. The Respimat® development story: Patient-centered innovation. Pulm. Ther. 2017, 3, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Festing, M.F.; Altman, D.G. Guidelines for the design and statistical analysis of experiments using laboratory animals. ILAR J. 2002, 43, 244–258. [Google Scholar] [CrossRef]
- Charan, J.; Kantharia, N. How to calculate sample size in animal studies? J. Pharmacol. Pharmacother. 2013, 4, 303–306. [Google Scholar] [CrossRef] [Green Version]
- Arifin, W.N.; Zahiruddin, W.M. Sample size calculation in animal studies using resource equation approach. Malays. J. Med. Sci. MJMS 2017, 24, 101. [Google Scholar]
- Festing, M.F. The principles of experimental design and the determination of sample size when using animal models of traumatic brain injury. In Pre-Clinical and Clinical Methods in Brain Trauma Research; Springer: Berlin/Heidelberg, Germany, 2018; pp. 201–225. [Google Scholar]
- Hollander, M.; Wolfe, D.A. Nonparametric Statistical Methods; NY John Wiley Sons: New York, NY, USA, 1999. [Google Scholar]
- Dani, S.; Prabhu, A.; Chaitra, K.; Desai, N.; Patil, S.R.; Rajeev, R. Assessment of Streptococcus mutans in healthy versus gingivitis and chronic periodontitis: A clinico-microbiological study. Contemp. Clin. Dent. 2016, 7, 529. [Google Scholar] [CrossRef]
- Fishman, A.P. The volume of blood in the lungs. Circulation 1966, 33, 835–838. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.B.; Jacob, S. A simple practice guide for dose conversion between animals and human. J. Basic Clin. Pharm. 2016, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Yildiz Pekoz, A.; Akbal Dagistan, O.; Fael, H.; Culha, M.; Erturk, A.; Basarir, N.S.; Sahin, G.; Serhatli, M.; Cakirca, G.; Tekin, S.; et al. Pulmonary delivery of favipiravir inhalation solution for COVID-19 treatment: In vitro characterization, stability, in vitro cytotoxicity, and antiviral activity using real time cell analysis. Drug Deliv. 2022, 29, 2846–2854. [Google Scholar] [CrossRef]
- Muellinger, B.; Buchmann, N.A.; Bartholomew, J.; de Kruijf, W. Aerosol performance of the single-use Pulmospray™ soft mist inhaler for inhalation of high amounts of liquid formulations. In Proceedings of the Poster Presentation, Resyca, 23rd Int Congress Int Soc Aerosols Med (ISAM 2021), Boise, ID, USA, 22 May 2021. [Google Scholar]
- Kmecova, J.; Klimas, J. Heart rate correction of the QT duration in rats. Eur. J. Pharmacol. 2010, 641, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Zani, A.; Cordischi, L.; Cananzi, M.; De Coppi, P.; Smith, V.; Eaton, S.; Pierro, A. Assessment of a neonatal rat model of necrotizing enterocolitis. Eur. J. Pediatr. Surg. 2008, 18, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Pamukcu, O.; Kumral, Z.N.O.; Ercan, F.; Yegen, B.Ç.; Ertem, D. Anti-inflammatory effect of obestatin and ghrelin in dextran sulfate sodium–induced colitis in rats. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P.P.; Priebat, D.A.; Christensen, R.D.; Rothstein, G. Measurement of cutaneous inflammation: Estimation of neutrophil content with an enzyme marker. J. Investig. Dermatol. 1982, 78, 206–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beutler, E. Red Blood Cell Metabolism: A Manual of Biochemical Methods, 2nd ed.; Grune and Stratton: New York, NY, USA, 1975. [Google Scholar]
- Suzuki, R.; Osaka, Y. Quantitative Analysis of Favipiravir Spiked in Plasma Using by HPLC, Shimadzu Excellence in Science, Application News no L 570. Available online: https://www.shimadzu.com/an/literature/hplc/jpl220032.html (accessed on 19 July 2022).
- Furuta, Y.; Komeno, T.; Nakamura, T. Favipiravir (T-705), a broad spectrum inhibitor of viral RNA polymerase. Proc. Jpn. Acad. Ser. B 2017, 93, 449–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shannon, A.; Selisko, B.; Le, N.; Huchting, J.; Touret, F.; Piorkowski, G.; Fattorini, V.; Ferron, F.; Decroly, E.; Meier, C. Favipiravir strikes the SARS-CoV-2 at its Achilles heel, the RNA polymerase. BioRxiv 2020. [Google Scholar] [CrossRef]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Dawes, B.E.; Kalveram, B.; Ikegami, T.; Juelich, T.; Smith, J.K.; Zhang, L.; Park, A.; Lee, B.; Komeno, T.; Furuta, Y. Favipiravir (T-705) protects against Nipah virus infection in the hamster model. Sci. Rep. 2018, 8, 7604. [Google Scholar] [CrossRef] [Green Version]
- Julander, J.G.; Shafer, K.; Smee, D.F.; Morrey, J.D.; Furuta, Y. Activity of T-705 in a hamster model of yellow fever virus infection in comparison with that of a chemically related compound, T-1106. Antimicrob. Agents Chemother. 2009, 53, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Scharton, D.; Bailey, K.W.; Vest, Z.; Westover, J.B.; Kumaki, Y.; Van Wettere, A.; Furuta, Y.; Gowen, B.B. Favipiravir (T-705) protects against peracute Rift Valley fever virus infection and reduces delayed-onset neurologic disease observed with ribavirin treatment. Antivir. Res. 2014, 104, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Kaptein, S.J.; Jacobs, S.; Langendries, L.; Seldeslachts, L.; Ter Horst, S.; Liesenborghs, L.; Hens, B.; Vergote, V.; Heylen, E.; Barthelemy, K. Favipiravir at high doses has potent antiviral activity in SARS-CoV-2− infected hamsters, whereas hydroxychloroquine lacks activity. Proc. Natl. Acad. Sci. USA 2020, 117, 26955–26965. [Google Scholar] [CrossRef] [PubMed]
- Driouich, J.-S.; Cochin, M.; Lingas, G.; Moureau, G.; Touret, F.; Petit, P.-R.; Piorkowski, G.; Barthélémy, K.; Laprie, C.; Coutard, B. Favipiravir antiviral efficacy against SARS-CoV-2 in a hamster model. Nat. Commun. 2021, 12, 1735. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y. Experimental treatment with favipiravir for COVID-19: An open-label control study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, Y.; Huang, J.; Yin, P.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; et al. Favipiravir versus Arbidol for COVID-19: A Randomized Clinical Trial. Front. Pharmacol. 2020, 12, 683296. [Google Scholar] [CrossRef] [PubMed]
- Hassanipour, S.; Arab-Zozani, M.; Amani, B.; Heidarzad, F.; Fathalipour, M.; Martinez-de-Hoyo, R. The efficacy and safety of Favipiravir in treatment of COVID-19: A systematic review and meta-analysis of clinical trials. Sci. Rep. 2021, 11, 110222. [Google Scholar] [CrossRef] [PubMed]
- Therapeutics, A. Appili Therapeutics Provides Update on Phase 3 PRESECO Clinical Trial Evaluating Avigan®/ReeqonusTM. Appili Ther. 2021. Available online: https://www.businesswire.com/news/home/20211112005554/en/Appili-Therapeutics-Provides-Update-on-Phase-3-PRESECO-Clinical-Trial-Evaluating-Avigan%C2%AEReeqonus%E2%84%A2 (accessed on 17 July 2022).
- Bocan, T.M.; Basuli, F.; Stafford, R.G.; Brown, J.L.; Zhang, X.; Duplantier, A.J.; Swenson, R.E. Synthesis of [18F] Favipiravir and biodistribution in C3H/HeN Mice as assessed by positron emission tomography. Sci. Rep. 2019, 9, 1785. [Google Scholar] [CrossRef] [Green Version]
- Kumar, G.N.; Jayanti, V.K.; Johnson, M.K.; Uchic, J.; Thomas, S.; Lee, R.D.; Grabowski, B.A.; Sham, H.L.; Kempf, D.J.; Denissen, J.F. Metabolism and disposition of the HIV-1 protease inhibitor lopinavir (ABT-378) given in combination with ritonavir in rats, dogs, and humans. Pharm. Res. 2004, 21, 1622–1630. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, L. Lung tissue distribution of drugs as a key factor for COVID-19 treatment. Br. J. Pharmacol. 2020, 177, 4995. [Google Scholar] [CrossRef]
- Sun, D. Remdesivir for treatment of COVID-19: Combination of pulmonary and IV administration may offer aditional benefit. AAPS J. 2020, 22, 77. [Google Scholar] [CrossRef]
- Cazzola, M.; Rogliani, P.; Anzueto, A.; Heijdra, Y.; Hurst, J. Inhaled medication: Which device for which patient. ERS Monogr. 2015, 69, 213–223. [Google Scholar]
- O’Callaghan, C.; Barry, P.W. The science of nebulised drug delivery. Thorax 1997, 52, S31. [Google Scholar] [CrossRef] [PubMed]
- Amirav, I.; Newhouse, M.T. Transmission of coronavirus by nebulizer: A serious, underappreciated risk. Cmaj 2020, 192, E346. [Google Scholar] [CrossRef]
- Tang, J.; Li, Y.; Eames, I.; Chan, P.; Ridgway, G. Factors involved in the aerosol transmission of infection and control of ventilation in healthcare premises. J. Hosp. Infect. 2006, 64, 100–114. [Google Scholar] [CrossRef]
- Dalby, R.N.; Eicher, J.; Zierenberg, B. Development of Respimat® Soft Mist™ Inhaler and its clinical utility in respiratory disorders. Med. Devices 2011, 4, 145. [Google Scholar]
- Anderson, P. Use of Respimat® soft Mist™ inhaler in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2006, 1, 251. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.P.; Brown, J.; Steed, K.P.; Reader, S.J.; Kladders, H. Lung deposition of fenoterol and flunisolide delivered using a novel device for inhaled medicines: Comparison of RESPIMAT with conventional metered-dose inhalers with and without spacer devices. Chest 1998, 113, 957–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitcairn, G.; Reader, S.; Pavia, D.; Newman, S. Deposition of corticosteroid aerosol in the human lung by Respimat® Soft Mist™ Inhaler compared to deposition by metered dose inhaler or by Turbuhaler® dry powder inhaler. J. Aerosol Med. 2005, 18, 264–272. [Google Scholar] [CrossRef]
- El Azab, N.F. A validated UHPLC-MS/MS method for simultaneous quantification of some repurposed COVID-19 drugs in rat plasma: Application to a pharmacokinetic study. Microchem. J. 2022, 178, 107321. [Google Scholar] [CrossRef]
- Yarijani, Z.M.; Najafi, H. Kidney injury in COVID-19 patients, drug development and their renal complications: Review study. Biomed. Pharmacother. 2021, 142, 111966. [Google Scholar] [CrossRef]
- Naksuk, N.; Lazar, S.; Peeraphatdit, T. Cardiac safety of off-label COVID-19 drug therapy: A review and proposed monitoring protocol. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.B.; Elshafei, M.; Rahhal, A.; Mohamed, M.F. Severe sinus bradycardia associated with favipiravir in a COVID-19 patient. Clin. Case Rep. 2021, 9, e04566. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Report on the Deliberation Results. Evaluation and Licensing Division, Pharmaceutical and Food Safety Bureau; 2014. Available online: https://www.pmda.go.jp/files/000210319.pdf (accessed on 8 June 2022).
- Mishima, E.; Anzai, N.; Miyazaki, M.; Abe, T. Uric acid elevation by favipiravir, an antiviral drug. Tohoku J. Exp. Med. 2020, 251, 87–90. [Google Scholar] [CrossRef]
- Doi, Y.; Hibino, M.; Hase, R.; Yamamoto, M.; Kasamatsu, Y.; Hirose, M.; Mutoh, Y.; Homma, Y.; Terada, M.; Ogawa, T. A prospective, randomized, open-label trial of early versus late favipiravir therapy in hospitalized patients with COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01897-20. [Google Scholar] [CrossRef] [PubMed]
- Udwadia, Z.F.; Singh, P.; Barkate, H.; Patil, S.; Rangwala, S.; Pendse, A.; Kadam, J.; Wu, W.; Caracta, C.F.; Tandon, M. Efficacy and safety of favipiravir, an oral RNA-dependent RNA polymerase inhibitor, in mild-to-moderate COVID-19: A randomized, comparative, open-label, multicenter, phase 3 clinical trial. Int. J. Infect. Dis. 2021, 103, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Kara, A.; Yakut, S.; Caglayan, C.; Atçalı, T.; Ulucan, A.; Kandemir, F.M. Evaluation of the toxicological effects of favipiravir (T-705) on liver and kidney in rats: Biochemical and histopathological approach. Drug Chem. Toxicol. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Atçalı, T.; Yakut, S.; Çağlayan, C.; Ulucan, A.; Adem, K. Effects of favipiravir on hematologic parameters and bone marrow in the rats. J. Exp. Clin. Med. 2022, 39, 156–159. [Google Scholar] [CrossRef]
- Kaneko, S.; Kurosaki, M.; Nagata, K.; Taki, R.; Ueda, K.; Hanada, S.; Takayama, K.; Suzaki, S.; Harada, N.; Sugiyama, T. Liver injury with COVID-19 based on gastrointestinal symptoms and pneumonia severity. PLoS ONE 2020, 15, e0241663. [Google Scholar] [CrossRef]
- Hung, D.T.; Ghula, S.; Aziz, J.M.A.; Makram, A.M.; Tawfik, G.M.; Abozaid, A.A.-F.; Pancharatnam, R.A.; Ibrahim, A.M.; Shabouk, M.B.; Turnage, M. The efficacy and adverse effects of favipiravir on COVID-19 patients: A systematic review and meta-analysis of published clinical trials and observational studies. Int. J. Infect. Dis. 2022, 120, 217–227. [Google Scholar] [CrossRef]
- Özlüşen, B.; Kozan, Ş.; Akcan, R.E.; Kalender, M.; Yaprak, D.; Peltek, İ.B.; Keske, Ş.; Gönen, M.; Ergönül, Ö. Effectiveness of favipiravir in COVID-19: A live systematic review. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2575–2583. [Google Scholar] [CrossRef]
- Smyk, J.M.; Majewska, A. Favipiravir in the Battle with Respiratory Viruses. Mini Rev. Med. Chem. 2022, 22, 2224–2236. [Google Scholar] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbal-Dagistan, O.; Sevim, M.; Sen, L.S.; Basarir, N.S.; Culha, M.; Erturk, A.; Fael, H.; Kaptan, E.; Sancar, S.; Mulazimoglu Durmusoglu, L.; et al. Pulmonary Delivery of Favipiravir in Rats Reaches High Local Concentrations without Causing Oxidative Lung Injury or Systemic Side Effects. Pharmaceutics 2022, 14, 2375. https://doi.org/10.3390/pharmaceutics14112375
Akbal-Dagistan O, Sevim M, Sen LS, Basarir NS, Culha M, Erturk A, Fael H, Kaptan E, Sancar S, Mulazimoglu Durmusoglu L, et al. Pulmonary Delivery of Favipiravir in Rats Reaches High Local Concentrations without Causing Oxidative Lung Injury or Systemic Side Effects. Pharmaceutics. 2022; 14(11):2375. https://doi.org/10.3390/pharmaceutics14112375
Chicago/Turabian StyleAkbal-Dagistan, Ozlem, Mustafa Sevim, Leyla Semiha Sen, Nur Sena Basarir, Meltem Culha, Aybige Erturk, Hanan Fael, Engin Kaptan, Serap Sancar, Lutfiye Mulazimoglu Durmusoglu, and et al. 2022. "Pulmonary Delivery of Favipiravir in Rats Reaches High Local Concentrations without Causing Oxidative Lung Injury or Systemic Side Effects" Pharmaceutics 14, no. 11: 2375. https://doi.org/10.3390/pharmaceutics14112375