A Simple, Safe, and Effective Method for Preparing Autologous Bio-Based Fibrin Glue for Ophthalmic Use

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Collection
2.2. Preparation of FGs
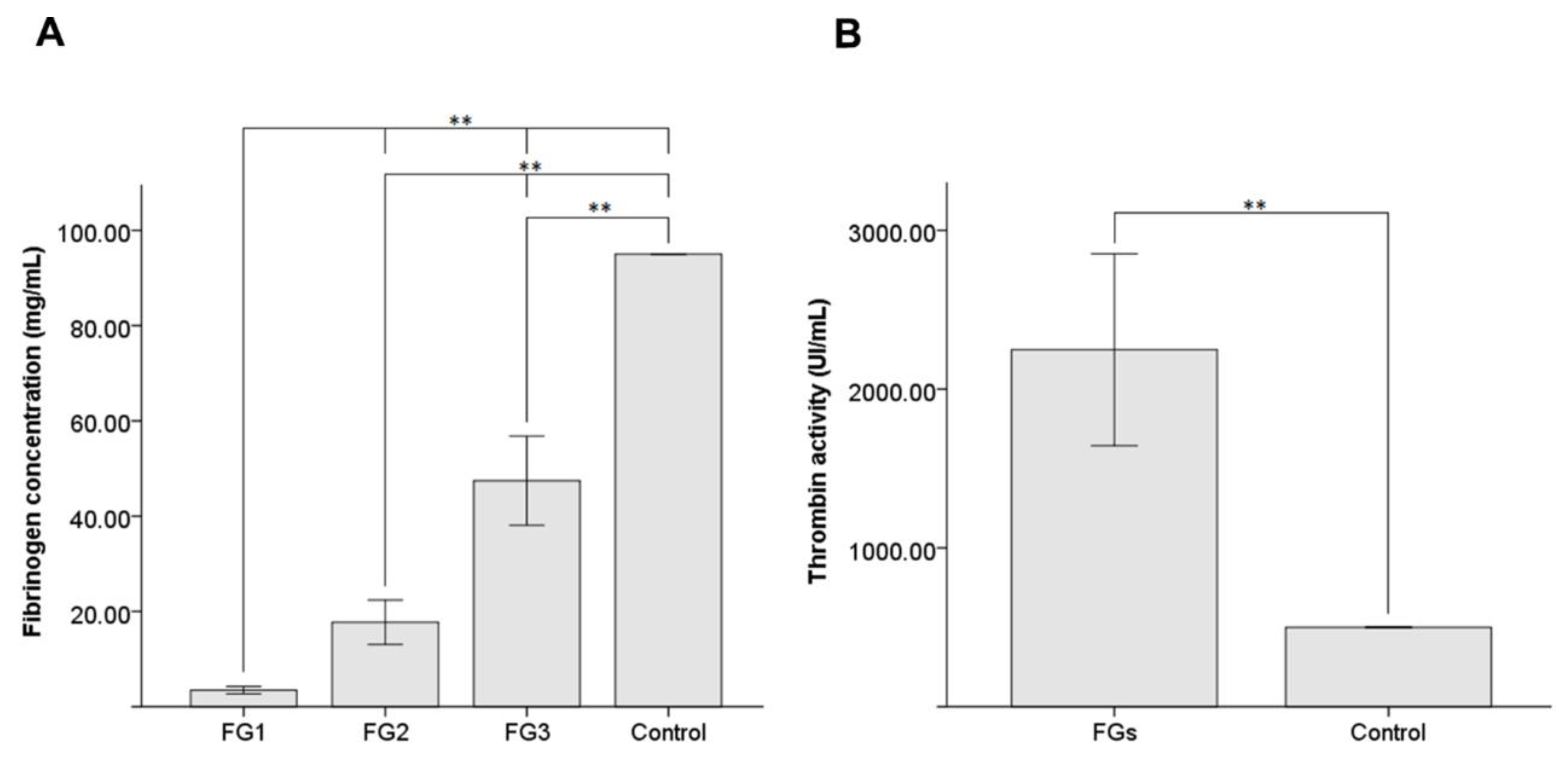
2.3. Fibrinogen Quantification
2.4. Thrombin Activity Quantification
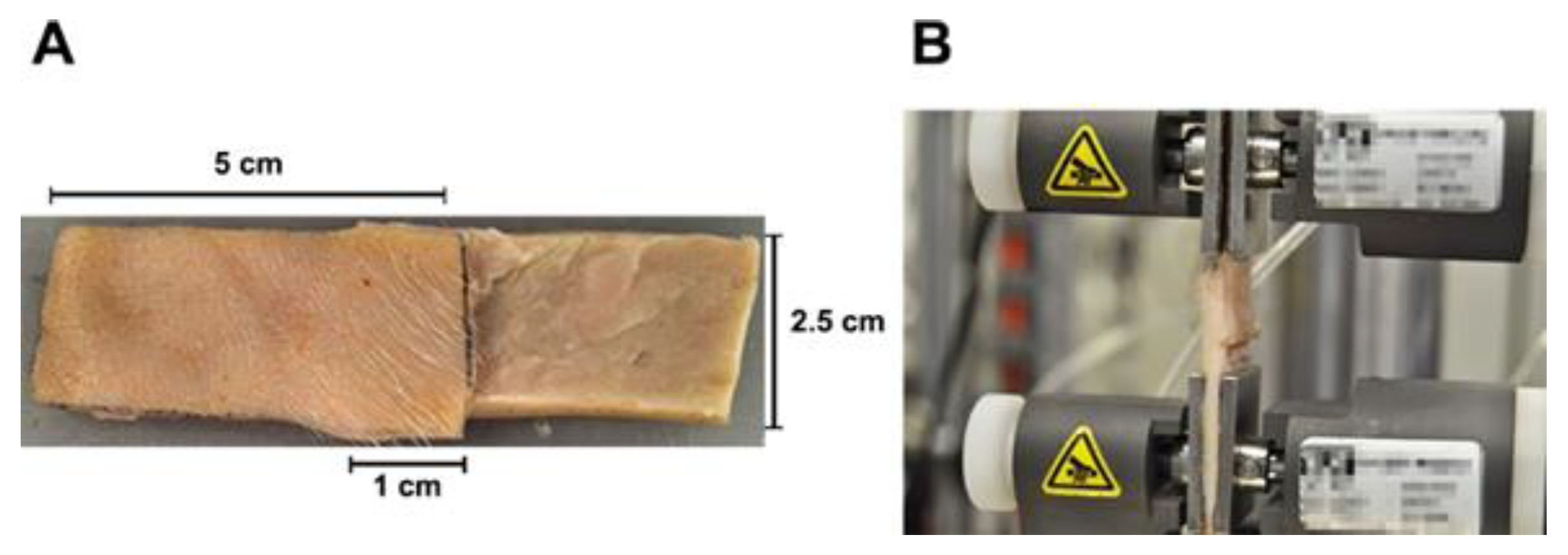
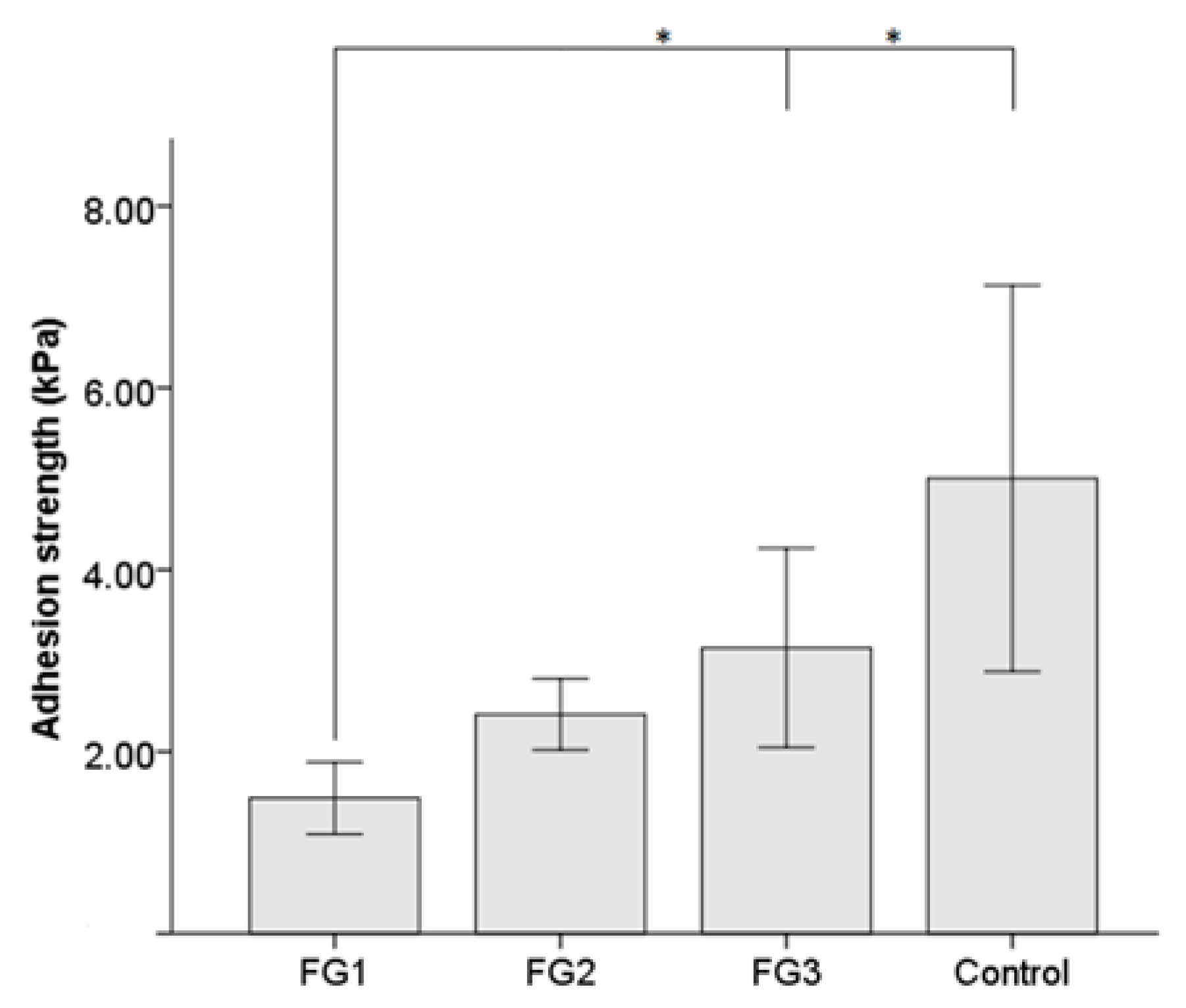
2.5. Adhesion Strength Measurement
2.6. Preclinical Study
2.6.1. Animals
2.6.2. Surgical Procedure
2.6.3. Clinical Follow-Up
2.7. Histology
2.8. Data Analysis
3. Results
3.1. Characteristics of FGs
3.2. Preclinical Study
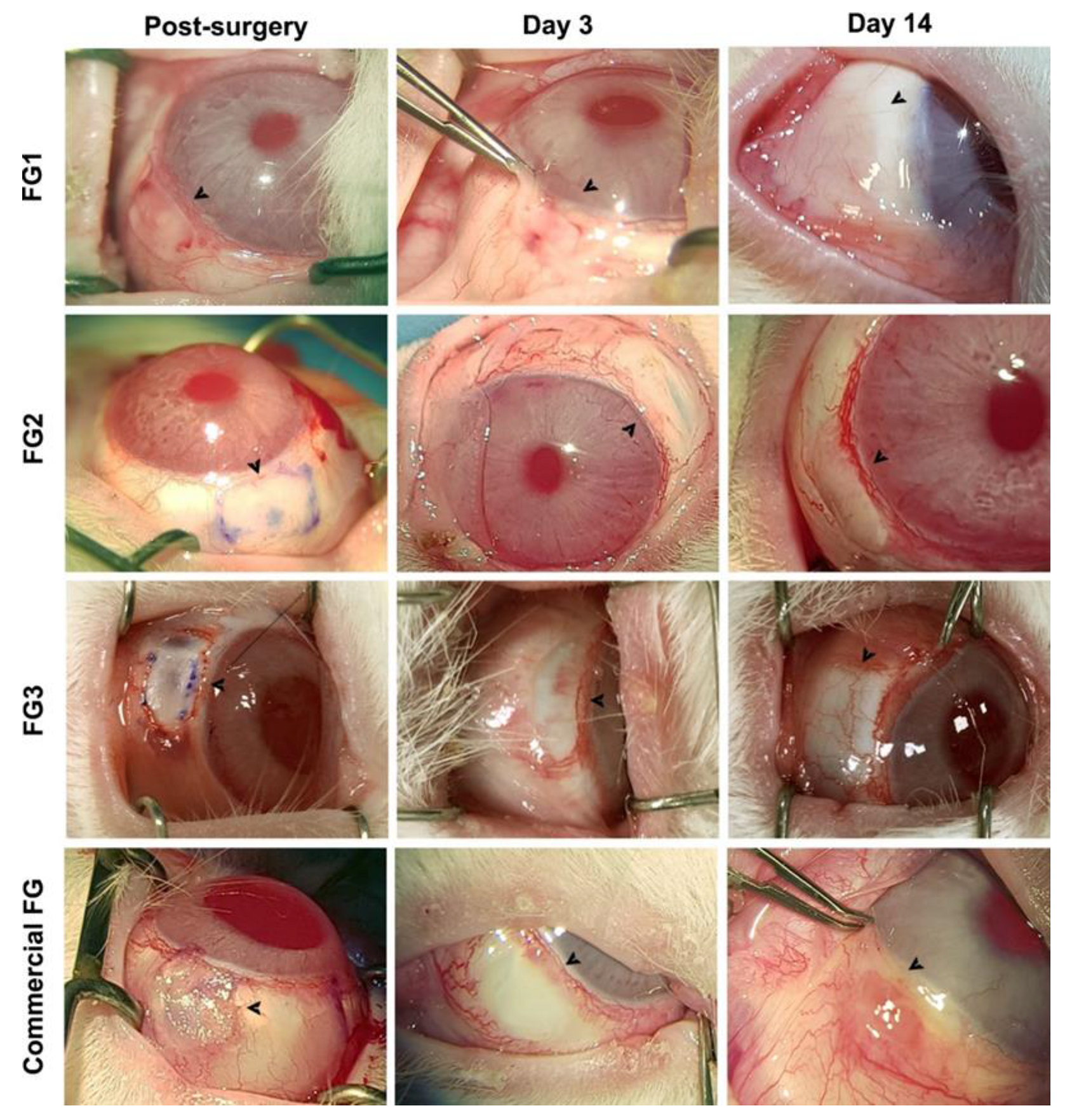
3.2.1. Intraoperative and Clinical Observations
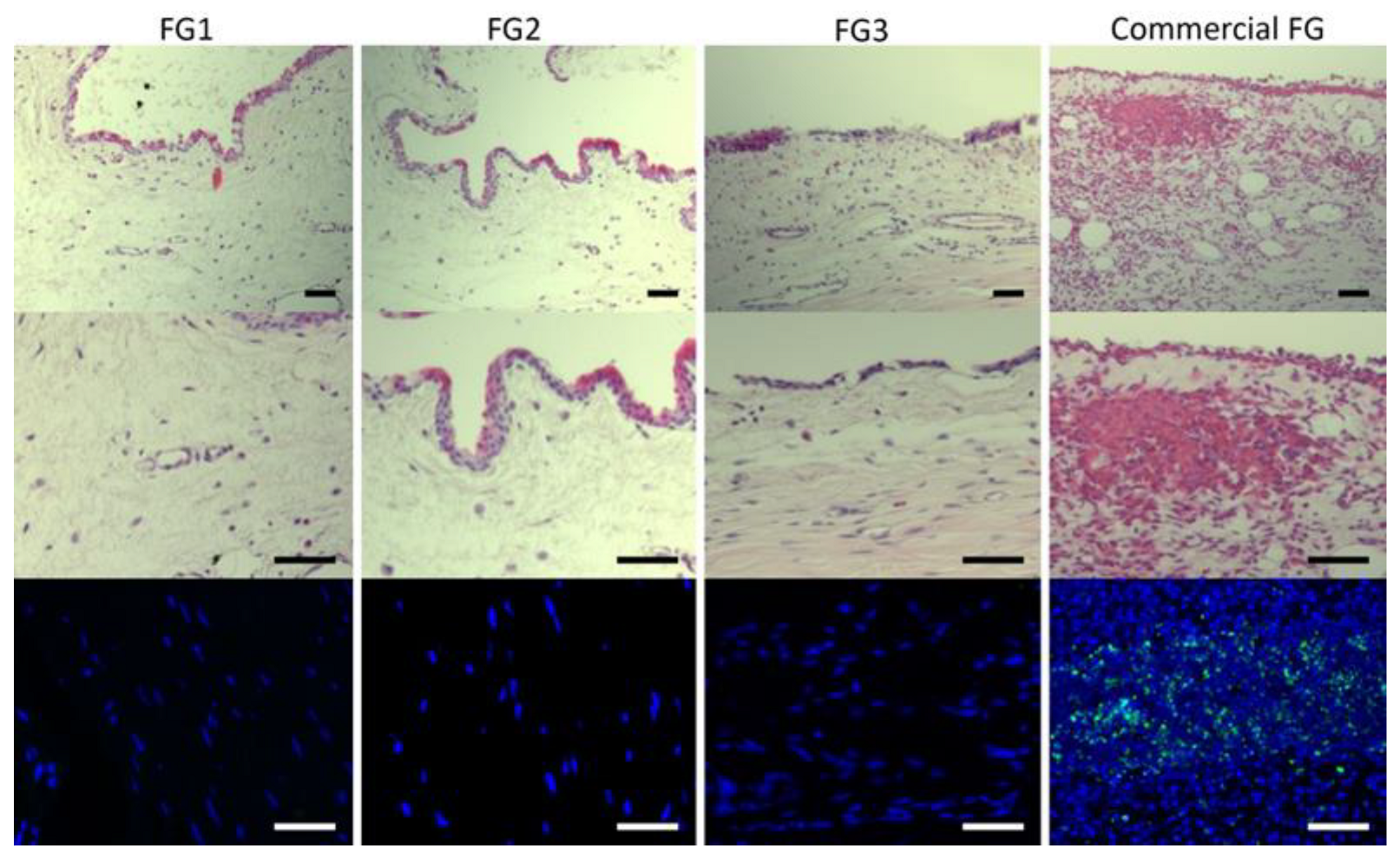
3.2.2. Histological Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Panda, A.; Kumar, S.; Kumar, A.; Bansal, R.; Bhartiya, S. Fibrin Glue in Ophthalmology. Indian J. Ophthalmol. 2009, 57, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Somani, S.N.; Moshirfar, M.; Shmunes, K.M.; Ronquillo, Y.C. Comparison and Application of Commercially Available Fibrin Sealants in Ophthalmology. Ocul. Surf. 2020, 18, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Romano, V.; Cruciani, M.; Conti, L.; Fontana, L. Fibrin Glue versus Sutures for Conjunctival Autografting in Primary Pterygium Surgery. Cochrane Database Syst. Rev. 2016, 2016, 14. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.M.; Boisjoly, H. Advances in the Use of Adhesives in Ophthalmology. Curr. Opin. Ophthalmol. 2004, 15, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Guhan, S.; Peng, S.L.; Janbatian, H.; Saadeh, S.; Greenstein, S.; Al Bahrani, F.; Fadlallah, A.; Yeh, T.C.; Melki, S.A. Surgical Adhesives in Ophthalmology: History and Current Trends. Br. J. Ophthalmol. 2018, 102, 1328–1335. [Google Scholar] [CrossRef] [PubMed]
- Alió, J.L.; Gómez, J.; Mulet, E.; Mahiques Bujanda, M.M.; Martin Martinez, J.M.; Molina, Y. A New Acrylic Tissue Adhesive for Conjunctival Surgery: Experimental Study. Ophthalmic Res. 2003, 35, 306–312. [Google Scholar] [CrossRef]
- Trujillo-de Santiago, G.; Sharifi, R.; Yue, K.; Sani, E.S.; Kashaf, S.S.; Alvarez, M.M.; Leijten, J.; Khademhosseini, A.; Dana, R.; Annabi, N. Ocular Adhesives: Design, Chemistry, Crosslinking Mechanisms, and Applications. Biomaterials 2019, 197, 345–367. [Google Scholar] [CrossRef] [Green Version]
- Radosevich, M.; Goubran, H.A.; Burnouf, T. Fibrin Sealant: Scientific Rationale, Production Methods, Properties, and Current Clinical Use. Vox Sang. 1997, 72, 133–143. [Google Scholar] [CrossRef]
- Cho, S.Y.; Kim, M.S.; Oh, S.J.; Chung, S.K. Comparison of Synthetic Glues and 10-0 Nylon in Rabbit Lamellar Keratoplasty. Cornea 2013, 32, 1265–1268. [Google Scholar] [CrossRef]
- Anitua, E.; Andia, I.; Ardanza, B.; Nurden, P.; Nurden, A.T. Autologous Platelets as a Source of Proteins for Healing and Tissue Regeneration. Thromb. Haemost. 2004, 91, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Nugent, R.B.; Lee, G.A. Ophthalmic Use of Blood-Derived Products. Surv. Ophthalmol. 2015, 60, 406–434. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Kumar, D.A.; Jacob, S.; Baid, C.; Agarwal, A.; Srinivasan, S. Fibrin Glue-Assisted Sutureless Posterior Chamber Intraocular Lens Implantation in Eyes with Deficient Posterior Capsules. J. Cataract Refract. Surg. 2008, 34, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Kheirkhah, A.; Casas, V.; Raju, V.K.; Tseng, S.C.G. Sutureless Amniotic Membrane Transplantation for Partial Limbal Stem Cell Deficiency. Am. J. Ophthalmol. 2008, 145, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spotnitz, W.D. Commercial Fibrin Sealants in Surgical Care. Am. J. Surg. 2001, 182, 8–14. [Google Scholar] [CrossRef]
- Chen, T.M.; Tzeng, Y.S.; Tsai, J.C.; Burnouf, T. Single-Donor Allogeneic Platelet Fibrin Glue and Osteoconductive Scaffold in Orbital Floor Fracture Reconstruction. Ann. Plast. Surg. 2013, 70, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Thorn, J.J.; Sørensen, H.; Weis-Fogh, U.; Andersen, M. Autologous Fibrin Glue with Growth Factors in Reconstructive Maxillofacial Surgery. Int. J. Oral Maxillofac. Surg. 2004, 33, 95–100. [Google Scholar] [CrossRef]
- Alston, S.M.; Solen, K.A.; Broderick, A.H.; Sukavaneshvar, S.; Mohammad, S.F. New Method to Prepare Autologous Fibrin Glue on Demand. Transl. Res. 2007, 149, 187–195. [Google Scholar] [CrossRef]
- Buchta, C.; Hedrich, H.C.; Macher, M.; Höcker, P.; Redl, H. Biochemical Characterization of Autologous Fibrin Sealants Produced by CryoSeal® and Vivostat® in Comparison to the Homologous Fibrin Sealant Product Tissucol/Tisseel®. Biomaterials 2005, 26, 6233–6241. [Google Scholar] [CrossRef]
- Rock, G.; Neurath, D.; Semple, E.; Harvey, M.; Freedman, M. Preparation and Characterization of Human Thrombin for Use in a Fibrin Glue. Transfus. Med. 2007, 17, 187–191. [Google Scholar] [CrossRef]
- DePalma, L.; Criss, V.R.; Luban, N.L. The Preparation of Fibrinogen Concentrate for Use as Fibrin Glue by Four Different Methods. Transfusion 1993, 33, 717–720. [Google Scholar] [CrossRef]
- Yoshida, H.; Kamiya, A. A Quicker Preparation Method for Autologous Fibrin Glue. Biol. Pharm. Bull. 1998, 21, 1367–1370. [Google Scholar] [CrossRef] [Green Version]
- Aizawa, P.; Winge, S.; Karlsson, G. Large-Scale Preparation of Thrombin from Human Plasma. Thromb. Res. 2008, 122, 560–567. [Google Scholar] [CrossRef]
- Quarmby, J.W.; Engelke, C.; Chitolie, A.; Morgan, R.A.; Belli, A.M. Autologous Thrombin for Treatment of Pseudoaneurysms. Lancet 2002, 359, 946–947. [Google Scholar] [CrossRef]
- Clauss, A. Gerinnungsphzysiologische schnellmethode zur bestimmung des fibrinogens [Rapid physiological coagulation method in determination of fibrinogen]. Acta Haematol. 1957, 17, 237–246. [Google Scholar] [CrossRef]
- ASTM-F 2255-05; Standard Test Method for Strength Properties of Tissue Adhesives in Lap-Shear by Tension Loading. ASTM Int.: West Conshohocken, PA, USA, 2005.
- Marticorena, J.; Rodríguez-Ares, M.T.; Touriño, R.; Mera, P.; Valladares, M.J.; Martinez-De-La-Casa, J.M.; Benitez-Del-Castillo, J.M. Pterygium Surgery: Conjunctival Autograft Using a Fibrin Adhesive. Cornea 2006, 25, 34–36. [Google Scholar] [CrossRef]
- Szurman, P.; Warga, M.; Grisanti, S.; Roters, S.; Rohrbach, J.M.; Aisenbrey, S.; Kaczmarek, R.T.; Bartz-Schmidt, K.U. Sutureless Amniotic Membrane Fixation Using Fibrin Glue for Ocular Surface Reconstruction in a Rabbit Model. Cornea 2006, 25, 460–466. [Google Scholar] [CrossRef]
- Sekiyama, E.; Nakamura, T.; Kurihara, E.; Cooper, L.J.; Fullwood, N.J.; Takaoka, M.; Hamuro, J.; Kinoshita, S. Novel Sutureless Transplantation of Bioadhesive-Coated, Freeze-Dried Amniotic Membrane for Ocular Surface Reconstruction. Investig. Ophthalmol. Vis. Sci. 2007, 48, 1528–1534. [Google Scholar] [CrossRef] [Green Version]
- Higa, K.; Shimmura, S.; Kato, N.; Kawakita, T.; Miyashita, H.; Itabashi, Y.; Fukuda, K.; Shimazaki, J.; Tsubota, K. Proliferation and Differentiation of Transplantable Rabbit Epithelial Sheets Engineered with or without an Amniotic Membrane Carrier. Investig. Ophthalmol. Vis. Sci. 2007, 48, 597–604. [Google Scholar] [CrossRef] [Green Version]
- Nanavaty, M.A.; Vijjan, K.S.; Yvon, C. Deep Anterior Lamellar Keratoplasty: A Surgeon’s Guide. J. Curr. Ophthalmol. 2018, 30, 297–310. [Google Scholar] [CrossRef]
- Alharbi, S.S.; Alameer, A. Use of Fibrin Glue in the Management of Descemet Membrane Perforation during Deep Anterior Lamellar Keratoplasty. Middle East Afr. J. Ophthalmol. 2019, 26, 168–171. [Google Scholar] [CrossRef]
- Lee, J.H.; Kang, N.Y. Comparison of Fibrin Glue and Sutures for Conjunctival Wound Closure in Strabismus Surgery. Korean J. Ophthalmol. 2011, 25, 178–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonelli, E.; De Almeida, H.C.; Bambirra, E.A. Tissue Adhesives for a Sutureless Fadenoperation: An Experimental Study in a Rabbit Model. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4340–4345. [Google Scholar] [CrossRef] [PubMed]
- Daponte, P.L.; Cigna, A.; Lescano, O.; Sipowicz, F.; Pena, B.; Abud, G.; Di-Virgilio, G.; Chirinos, A.; Bodino, G.F. Conjunctival Autograft With Fibrin Glue for Pterygium: A Long Term Recurrence Assessment. Med. Hypothesis Discov. Innov. Ophthalmol. J. 2019, 8, 272–277. [Google Scholar]
- Uy, H.S.; Reyes, J.M.G.; Flores, J.D.G.; Lim-Bon-Siong, R. Comparison of Fibrin Glue and Sutures for Attaching Conjunctival Autografts after Pterygium Excision. Ophthalmology 2005, 112, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Alston, S.M.; Solen, K.A.; Sukavaneshvar, S.; Fazal Mohammad, S. In Vivo Efficacy of a New Autologous Fibrin Sealant. J. Surg. Res. 2008, 146, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Chapman, J.R. Autologous Thrombin: Intraoperative Production from Whole Blood. J. Extra. Corpor. Technol. 2008, 40, 94–98. [Google Scholar]
- Hartman, A.R.; Galanakis, D.K.; Honig, M.P.; Seifert, F.C.; Anagnostopoulos, C.E. Intraoperative Procurement. Arch. Surg. 1992, 127, 357–359. [Google Scholar] [CrossRef]
- Petakov, M.; Mandić-Radić, S.; Taseski, J.; Balint, B.; Bugarski, D.; Malićević, Ž.; Černak, I. The use of single-donor fibrin glue prepared by recycled cryoprecipitation in experimental liver surgery. Haematologia 2002, 32, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, M.; Heselhaus, J.; Wozniak, J.; Weinandy, S.; Mela, P.; Tschoeke, B.; Schmitz-Rode, T.; Jockenhoevel, S. Fibrin-Based Tissue Engineering: Comparison of Different Methods of Autologous Fibrinogen Isolation. Tissue Eng. Part C Methods 2013, 19, 216–226. [Google Scholar] [CrossRef]
- Wolberg, A.S.; Campbell, R.A. Thrombin Generation, Fibrin Clot Formation and Hemostasis. Transfus. Apher. Sci. 2008, 38, 15–23. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Vega-Cueto, L.; Persinal-Medina, M.; Vázquez, N.; Chacón, M.; Alfonso-Bartolozzi, B.; Alonso-Alonso, S.; Sánchez, T.; Berisa-Prado, S.; Martínez-López, L.M.; Merayo-Lloves, J.; et al. A Simple, Safe, and Effective Method for Preparing Autologous Bio-Based Fibrin Glue for Ophthalmic Use. Pharmaceutics 2022, 14, 2325. https://doi.org/10.3390/pharmaceutics14112325
Fernández-Vega-Cueto L, Persinal-Medina M, Vázquez N, Chacón M, Alfonso-Bartolozzi B, Alonso-Alonso S, Sánchez T, Berisa-Prado S, Martínez-López LM, Merayo-Lloves J, et al. A Simple, Safe, and Effective Method for Preparing Autologous Bio-Based Fibrin Glue for Ophthalmic Use. Pharmaceutics. 2022; 14(11):2325. https://doi.org/10.3390/pharmaceutics14112325
Chicago/Turabian StyleFernández-Vega-Cueto, Luis, Mairobi Persinal-Medina, Natalia Vázquez, Manuel Chacón, Belén Alfonso-Bartolozzi, Sergio Alonso-Alonso, Teresa Sánchez, Silvia Berisa-Prado, Laura María Martínez-López, Jesús Merayo-Lloves, and et al. 2022. "A Simple, Safe, and Effective Method for Preparing Autologous Bio-Based Fibrin Glue for Ophthalmic Use" Pharmaceutics 14, no. 11: 2325. https://doi.org/10.3390/pharmaceutics14112325