


Evaluation and Validation of the Limited Sampling Strategy of Polymyxin B in Patients with Multidrug-Resistant Gram-Negative Infection
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PMB Administration and Sample Collection
2.3. Quantification of PMB Concentration in Plasma
2.4. Development of LSSs in Our Center
2.5. Validation of the Predictive Performance of LSSs Developed in Our Center
2.6. Validation of the Predictive Performance of LSSs in Other Study Centers
2.7. Prediction of the Performance of LSSs at Infusion Time and Sampling Time Error in Real-World Clinical Practice
2.7.1. PopPK Model Analysis
2.7.2. Infusion Time Error
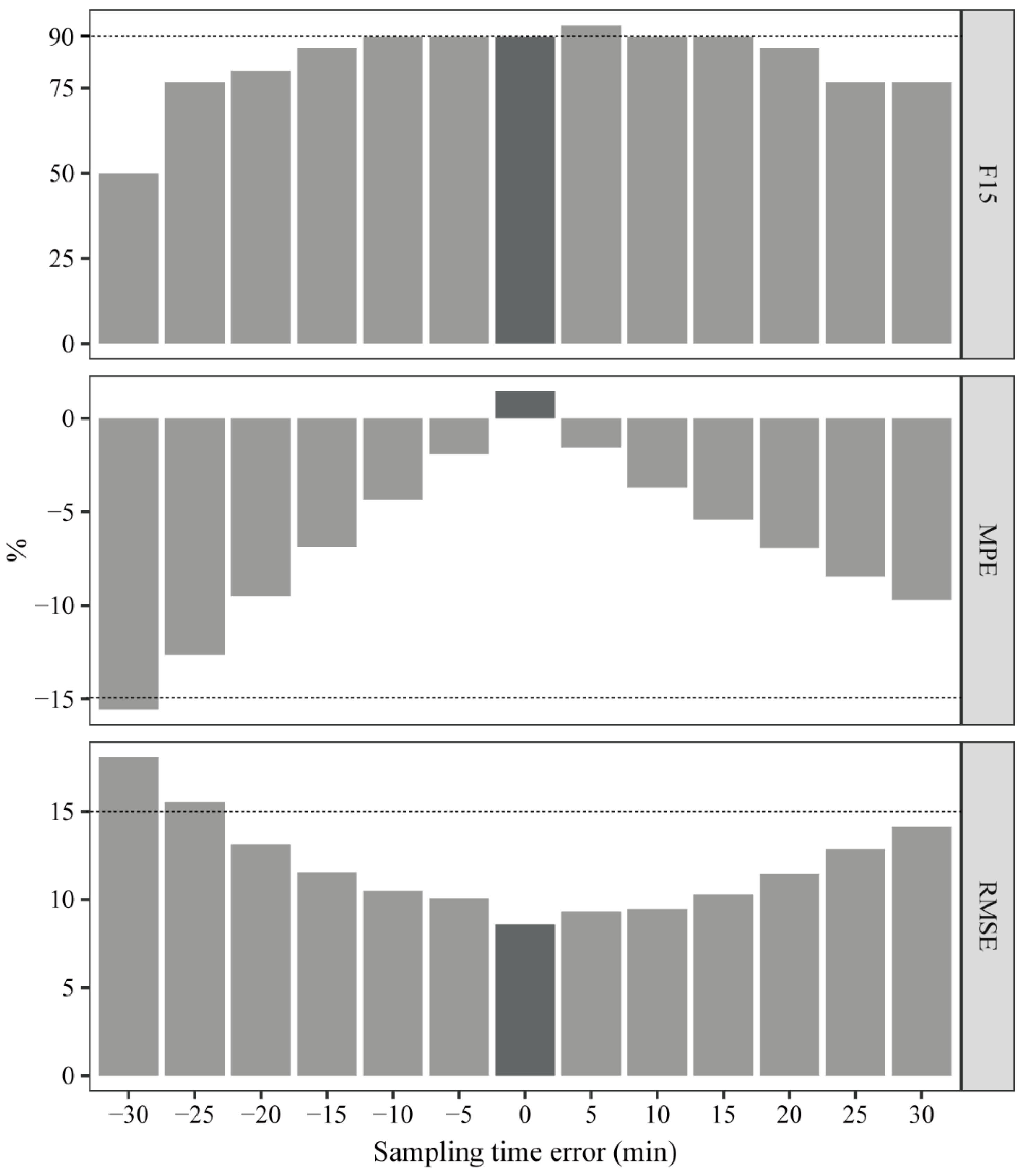
2.7.3. Sampling Time Error
3. Results
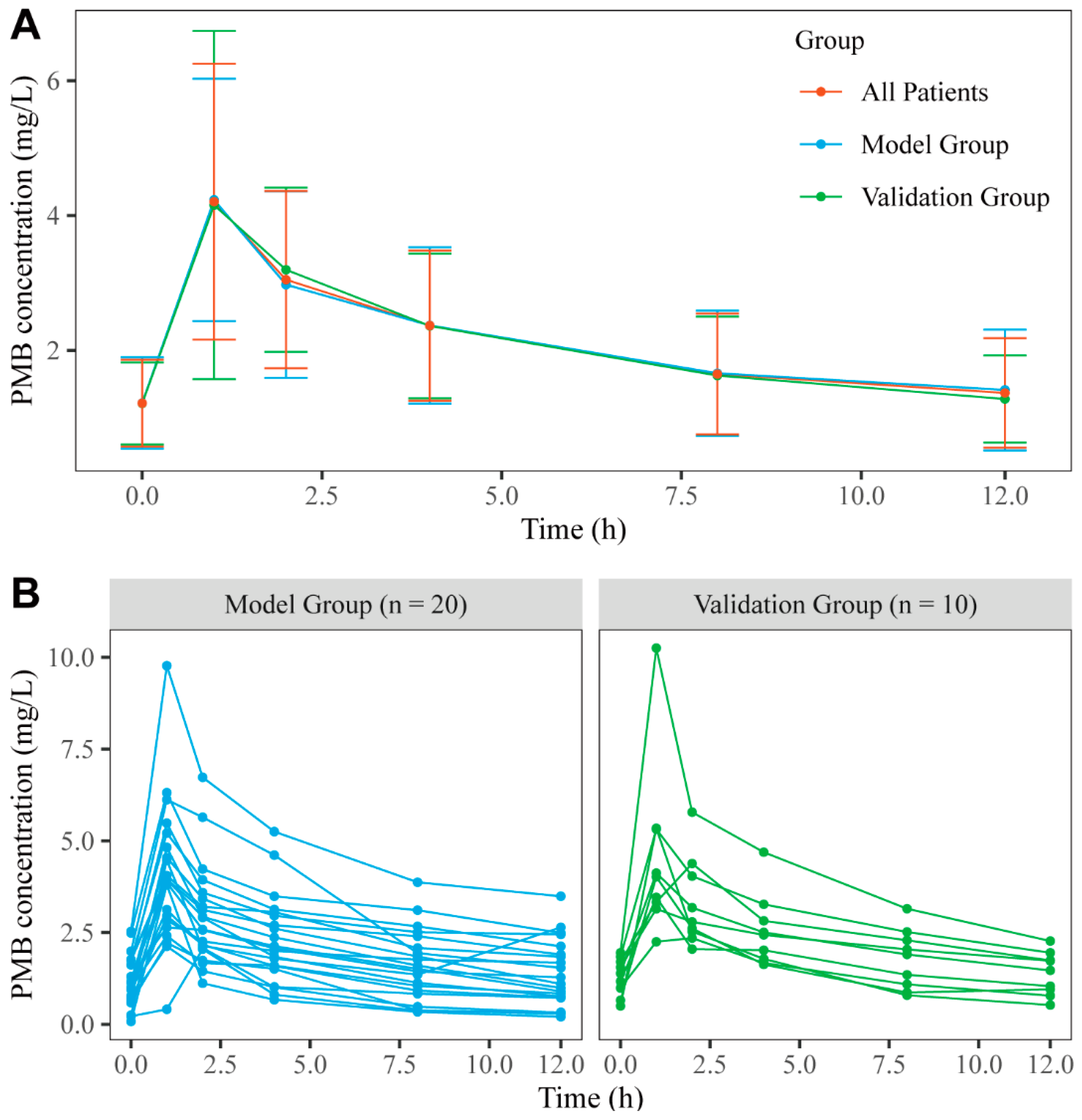
3.1. Patients and Data Collection
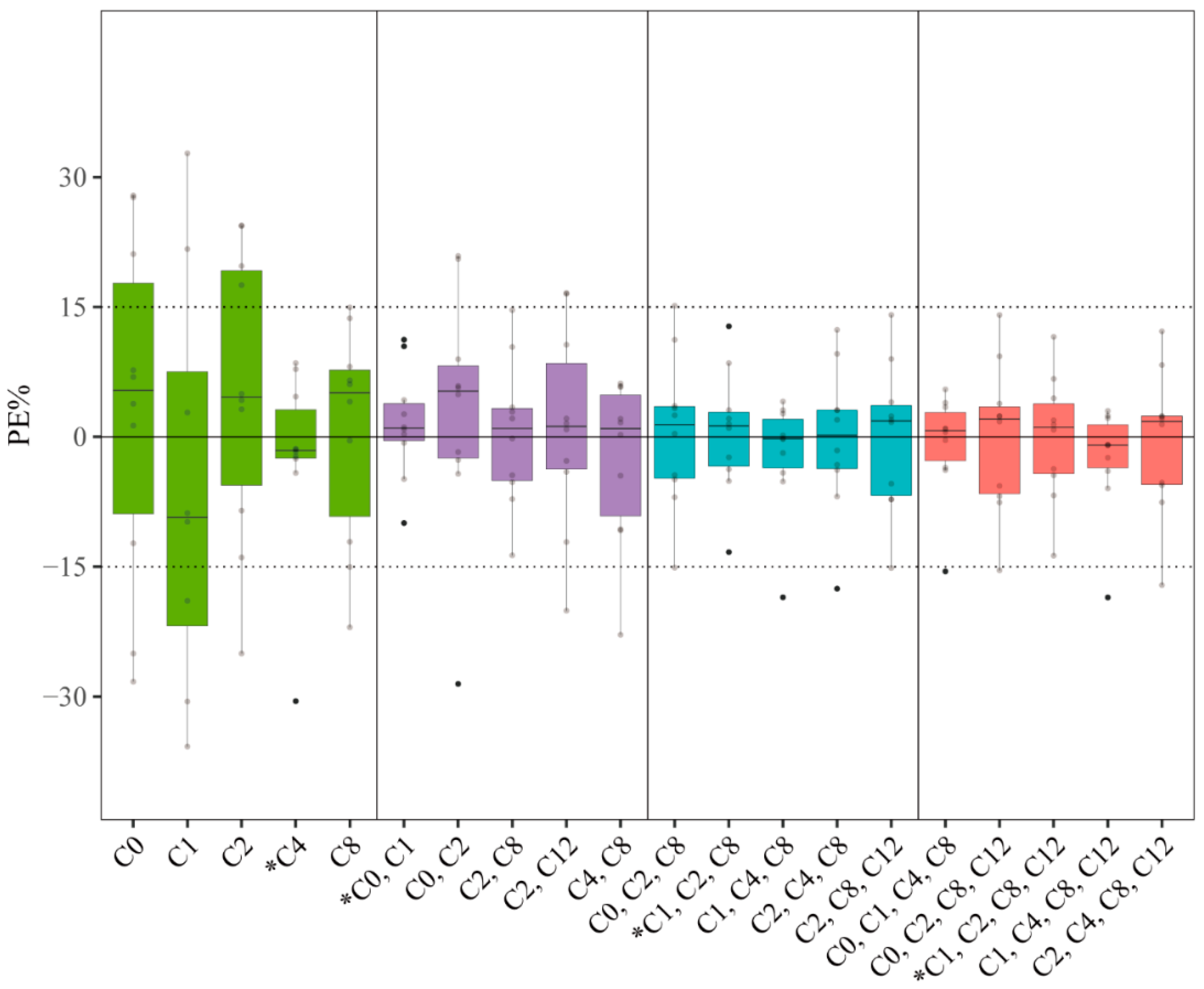
3.2. Development and Validation of LSSs in Our Center
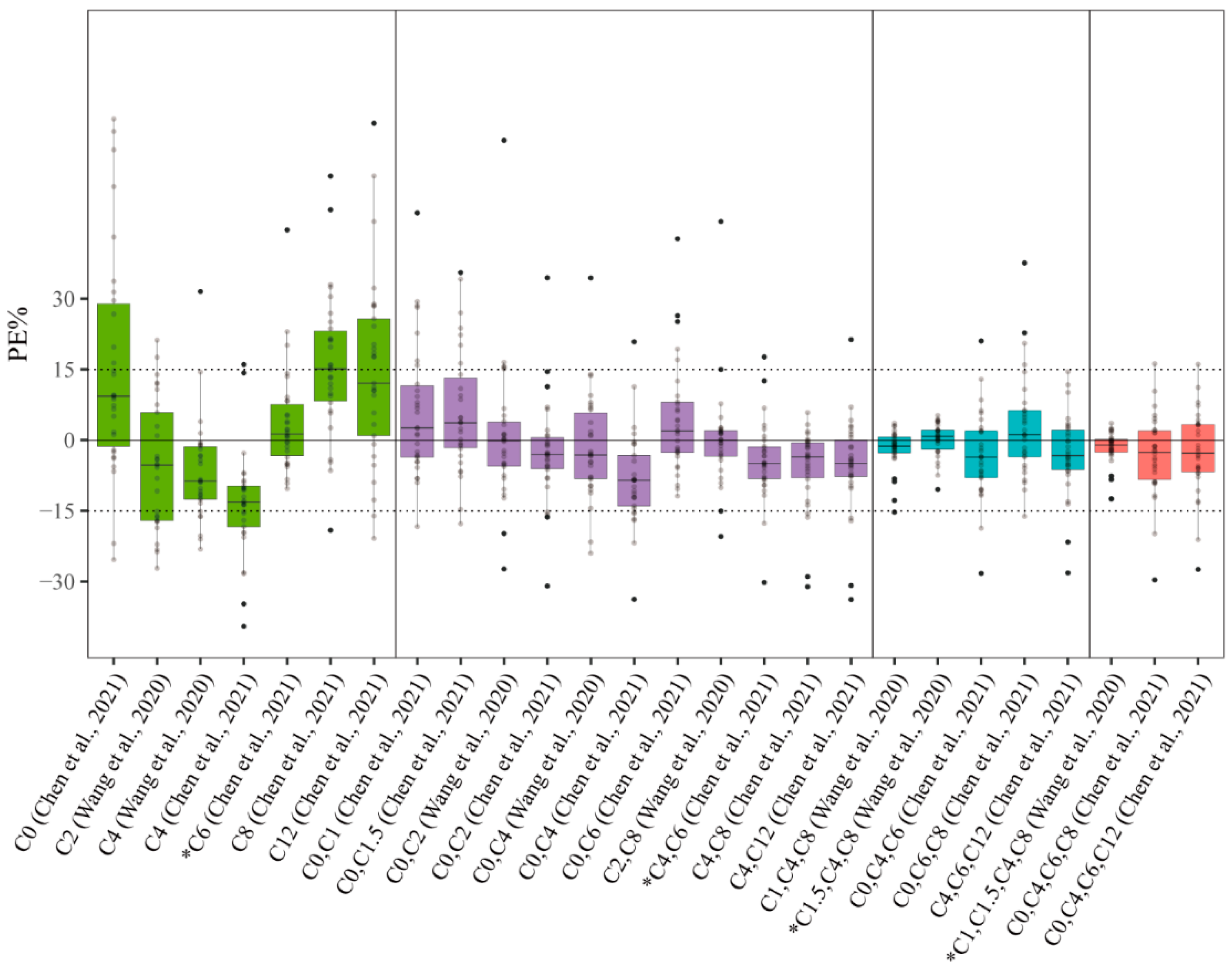
3.3. Validation of the Predictive Performance of LSSs in the Published Literature
3.4. Predictive Performance of LSSs at Infusion Time and Sampling Time Error in Real-World Clinical Practice
3.4.1. PopPK Model
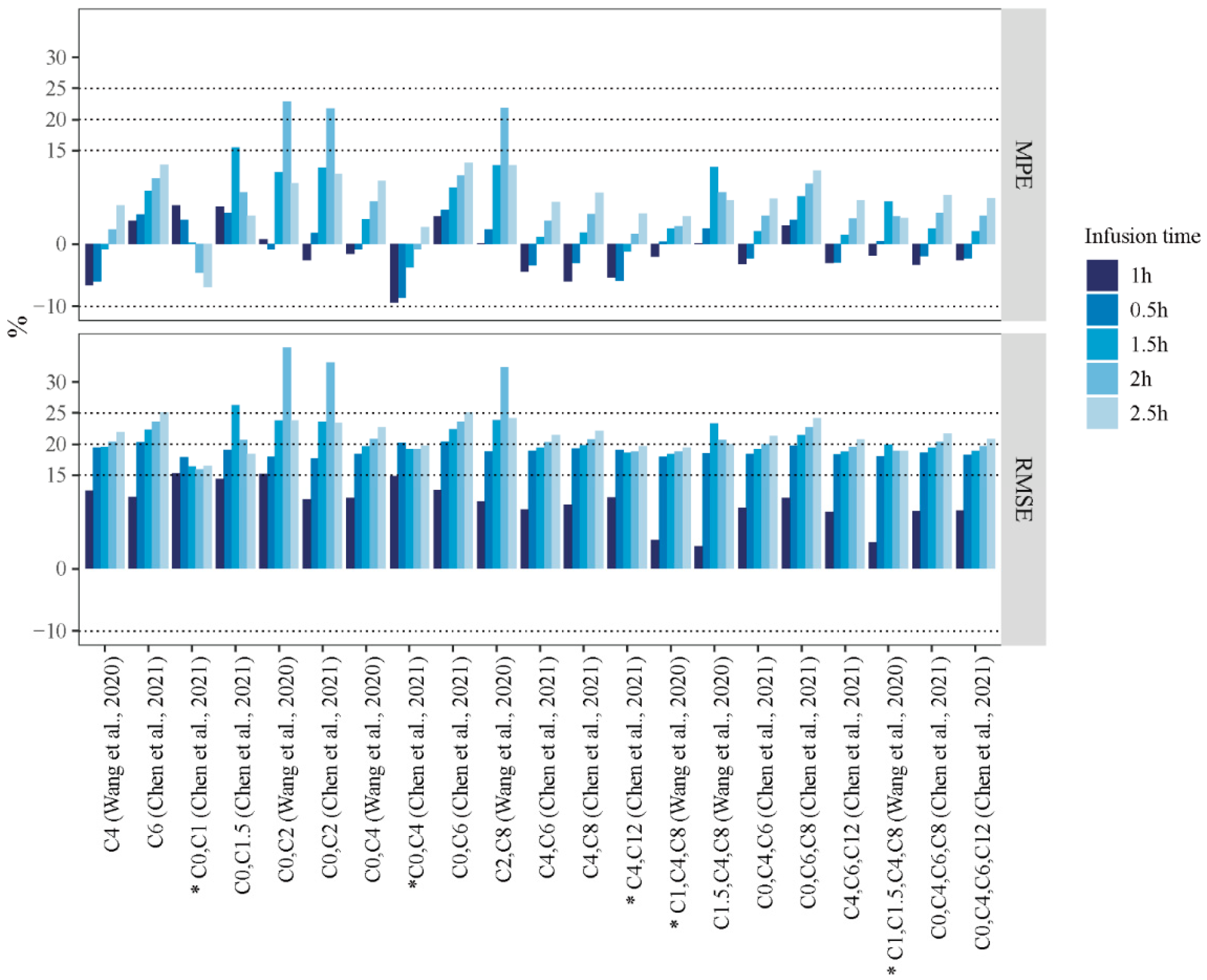
3.4.2. Infusion Time Error
3.4.3. Sampling Time Error
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morrill, H.J.; Pogue, J.M.; Kaye, K.S.; LaPlante, K.L. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infect. Dis. 2015, 2, ofv050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (U.S.). Antibiotic Resistance Threats in the United States, 2019; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019. [CrossRef] [Green Version]
- Medina, E.; Pieper, D.H. Tackling Threats and Future Problems of Multidrug-Resistant Bacteria. Curr. Top. Microbiol. Immunol. 2016, 398, 3–33. [Google Scholar] [CrossRef]
- Frieri, M.; Kumar, K.; Boutin, A. Antibiotic Resistance. J. Infect. Public Health 2017, 10, 369–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velkov, T.; Roberts, K.D.; Nation, R.L.; Thompson, P.E.; Li, J. Pharmacology of Polymyxins: New Insights into an “old” Class of Antibiotics. Future Microbiol. 2013, 8, 711–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nation, R.L.; Li, J.; Cars, O.; Couet, W.; Dudley, M.N.; Kaye, K.S.; Mouton, J.W.; Paterson, D.L.; Tam, V.H.; Theuretzbacher, U.; et al. Framework for Optimisation of the Clinical Use of Colistin and Polymyxin B: The Prato Polymyxin Consensus. Lancet Infect. Dis. 2015, 15, 225–234. [Google Scholar] [CrossRef]
- Dixon, R.A.; Chopra, I. Leakage of Periplasmic Proteins from Escherichia Coli Mediated by Polymyxin B Nonapeptide. Antimicrob. Agents Chemother. 1986, 29, 781–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Nation, R.L.; Turnidge, J.D.; Milne, R.W.; Coulthard, K.; Rayner, C.R.; Paterson, D.L. Colistin: The Re-Emerging Antibiotic for Multidrug-Resistant Gram-Negative Bacterial Infections. Lancet Infect. Dis. 2006, 6, 589–601. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kasiakou, S.K. Colistin: The Revival of Polymyxins for the Management of Multidrug-Resistant Gram-Negative Bacterial Infections. Clin. Infect. Dis. 2005, 40, 1333–1341. [Google Scholar] [CrossRef] [Green Version]
- Poirel, L.; Jayol, A.; Nordmann, P. Polymyxins: Antibacterial Activity, Susceptibility Testing, and Resistance Mechanisms Encoded by Plasmids or Chromosomes. Clin. Microbiol. Rev. 2017, 30, 557–596. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, V.N.; Stulberger, E.A.; Takacs, F.J. Colistimethate Overdosage. J. Urol. 1970, 104, 176–178. [Google Scholar] [CrossRef]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the Management of Adults with Hospital-Acquired, Ventilator-Associated, and Healthcare-Associated Pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, Y.; Leck, H.; Tan, R.W.; Teo, J.Q.; Lim, T.-P.; Lee, W.; Chlebicki, M.P.; Kwa, A.L. Clinical Experience with High-Dose Polymyxin B against Carbapenem-Resistant Gram-Negative Bacterial Infections-A Cohort Study. Antibiotics 2020, 9, 451. [Google Scholar] [CrossRef] [PubMed]
- Valachis, A.; Samonis, G.; Kofteridis, D.P. The Role of Aerosolized Colistin in the Treatment of Ventilator-Associated Pneumonia: A Systematic Review and Metaanalysis. Crit. Care Med. 2015, 43, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Haseeb, A.; Faidah, H.S.; Alghamdi, S.; Alotaibi, A.F.; Elrggal, M.E.; Mahrous, A.J.; Almarzoky Abuhussain, S.S.; Obaid, N.A.; Algethamy, M.; AlQarni, A.; et al. Dose Optimization of Colistin: A Systematic Review. Antibiotics 2021, 10, 1454. [Google Scholar] [CrossRef]
- Khawcharoenporn, T.; Apisarnthanarak, A.; Mundy, L.M. Intrathecal Colistin for Drug-Resistant Acinetobacter Baumannii Central Nervous System Infection: A Case Series and Systematic Review. Clin. Microbiol. Infect. 2010, 16, 888–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuji, B.T.; Pogue, J.M.; Zavascki, A.P.; Paul, M.; Daikos, G.L.; Forrest, A.; Giacobbe, D.R.; Viscoli, C.; Giamarellou, H.; Karaiskos, I.; et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-Infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy 2019, 39, 10–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoudi, L.; Mohammadpour, A.H.; Niknam, R.; Ahmadi, A.; Mojtahedzdeh, M. Limited Sampling Strategy for Estimation of Amikacin Optimal Sampling Time in Critically Ill Adults. Anaesth. Intensive Care 2014, 42, 228–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magis-Escurra, C.; Later-Nijland, H.M.J.; Alffenaar, J.W.C.; Broeders, J.; Burger, D.M.; van Crevel, R.; Boeree, M.J.; Donders, A.R.T.; van Altena, R.; van der Werf, T.S.; et al. Population Pharmacokinetics and Limited Sampling Strategy for First-Line Tuberculosis Drugs and Moxifloxacin. Int. J. Antimicrob. Agents 2014, 44, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Alsultan, A.; An, G.; Peloquin, C.A. Limited Sampling Strategy and Target Attainment Analysis for Levofloxacin in Patients with Tuberculosis. Antimicrob. Agents Chemother. 2015, 59, 3800–3807. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, H.; Wang, Q.; Wang, X.; Kong, X.; Wang, X.; Zhang, X.; Zhan, Q.; Li, P. Estimation of the Area under Concentration-Time Curve of Polymyxin B Based on Limited Sampling Concentrations in Chinese Patients with Severe Pneumonia. Eur. J. Clin. Pharmacol. 2021, 77, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Q.; Zhu, Z.; Feng, M.; Sun, T.; Yang, J.; Zhang, X. Population Pharmacokinetics and Limited Sampling Strategy for Therapeutic Drug Monitoring of Polymyxin B in Chinese Patients with Multidrug-Resistant Gram-Negative Bacterial Infections. Front. Pharmacol. 2020, 11, 829. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.-Y.; Jiao, Z.; Mao, J.-J.; Qiu, X.-Y. External Evaluation of Published Population Pharmacokinetic Models of Tacrolimus in Adult Renal Transplant Recipients. Br. J. Clin. Pharmacol. 2016, 81, 891–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.-Q.; Chen, K.-F.; Ding, J.-J.; Tan, H.-Y.; Yang, N.; Lin, Y.-Q.; Wu, C.-F.; Xie, Y.-L.; Yang, G.-P.; Liu, J.-J.; et al. External Evaluation of Published Population Pharmacokinetic Models of Polymyxin B. Eur. J. Clin. Pharmacol. 2021, 77, 1909–1917. [Google Scholar] [CrossRef]
- Hanafin, P.O.; Nation, R.L.; Scheetz, M.H.; Zavascki, A.P.; Sandri, A.M.; Kwa, A.L.; Cherng, B.P.Z.; Kubin, C.J.; Yin, M.T.; Wang, J.; et al. Assessing the Predictive Performance of Population Pharmacokinetic Models for Intravenous Polymyxin B in Critically Ill Patients. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 1525–1537. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Q.; Qin, Z.; Xing, H.; Xu, M.; Pei, H.; Yang, J.; Zhang, X. A Simple and Robust Liquid Chromatography with Tandem Mass Spectrometry Analytical Method for Therapeutic Drug Monitoring of Plasma and Cerebrospinal Fluid Polymyxin B1 and B2. Ther. Drug Monit. 2020, 42, 716–723. [Google Scholar] [CrossRef]
- Dalere, G.M.; Lum, B.L.; Cooney, G.F.; Wong-Chin, M. Comparison of Three Methods for Cyclosporine Area under the Curve Monitoring Calculations. Ther. Drug Monit. 1995, 17, 305–307. [Google Scholar] [CrossRef]
- Abd Rahman, A.N.; Tett, S.E.; Staatz, C.E. How Accurate and Precise Are Limited Sampling Strategies in Estimating Exposure to Mycophenolic Acid in People with Autoimmune Disease? Clin. Pharmacokinet. 2014, 53, 227–245. [Google Scholar] [CrossRef]
- David, O.J.; Johnston, A. Limited Sampling Strategies for Estimating Cyclosporin Area under the Concentration–Time Curve: Review of Current Algorithms. Ther. Drug Monit. 2001, 23, 100–114. [Google Scholar] [CrossRef]
- Sheiner, L.B.; Beal, S.L. Some Suggestions for Measuring Predictive Performance. J. Pharmacokinet. Biopharm. 1981, 9, 503–512. [Google Scholar] [CrossRef]
- Ting, L.S.L.; Villeneuve, E.; Ensom, M.H.H. Beyond Cyclosporine: A Systematic Review of Limited Sampling Strategies for Other Immunosuppressants. Ther. Drug Monit. 2006, 28, 419–430. [Google Scholar] [CrossRef]
- Sobiak, J.; Resztak, M.; Chrzanowska, M.; Zachwieja, J.; Ostalska-Nowicka, D. The Evaluation of Multiple Linear Regression-Based Limited Sampling Strategies for Mycophenolic Acid in Children with Nephrotic Syndrome. Molecules 2021, 26, 3723. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Barraclough, K.A.; Isbel, N.M.; Franklin, M.E.; Lee, K.J.; Taylor, P.J.; Campbell, S.B.; Petchey, W.G.; Staatz, C.E. Evaluation of Limited Sampling Strategies for Mycophenolic Acid after Mycophenolate Mofetil Intake in Adult Kidney Transplant Recipients. Ther. Drug Monit. 2010, 32, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Sarem, S.; Nekka, F.; Ahmed, I.S.; Litalien, C.; Li, J. Impact of Sampling Time Deviations on the Prediction of the Area under the Curve Using Regression Limited Sampling Strategies: Impact of Sampling Time Deviations on Area Under Curve Prediction. Biopharm. Drug Dispos. 2015, 36, 417–428. [Google Scholar] [CrossRef]
- Zelenitsky, S.A.; Ariano, R.E.; Zhanel, G.G. Pharmacodynamics of Empirical Antibiotic Monotherapies for an Intensive Care Unit (ICU) Population Based on Canadian Surveillance Data. J. Antimicrob. Chemother. 2011, 66, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandri, A.M.; Landersdorfer, C.B.; Jacob, J.; Boniatti, M.M.; Dalarosa, M.G.; Falci, D.R.; Behle, T.F.; Bordinhão, R.C.; Wang, J.; Forrest, A.; et al. Population Pharmacokinetics of Intravenous Polymyxin B in Critically Ill Patients: Implications for Selection of Dosage Regimens. Clin. Infect. Dis. 2013, 57, 524–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avedissian, S.N.; Miglis, C.; Kubin, C.J.; Rhodes, N.J.; Yin, M.T.; Cremers, S.; Prickett, M.; Scheetz, M.H. Polymyxin B Pharmacokinetics in Adult Cystic Fibrosis Patients. Pharmacotherapy 2018, 38, 730–738. [Google Scholar] [CrossRef]
- Miglis, C.; Rhodes, N.J.; Avedissian, S.N.; Kubin, C.J.; Yin, M.T.; Nelson, B.C.; Pai, M.P.; Scheetz, M.H. Population Pharmacokinetics of Polymyxin B in Acutely Ill Adult Patients. Antimicrob. Agents Chemother. 2018, 62, e01475-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Deng, Y.; Zhu, Z.-Y.; Liu, Y.-P.; Xu, P.; Li, X.; Xie, Y.-L.; Yao, H.-C.; Yang, L.; Zhang, B.-K.; et al. Population Pharmacokinetics of Polymyxin B and Dosage Optimization in Renal Transplant Patients. Front. Pharmacol. 2021, 12, 727170. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, Q.; Chen, Z.; Chen, W.; Zhan, Q.; Wang, C. Effectiveness, Nephrotoxicity, and Therapeutic Drug Monitoring of Polymyxin B in Nosocomial Pneumonia among Critically Ill Patients. Clin. Respir. J. 2022, 16, 402–412. [Google Scholar] [CrossRef]
- Wang, P.; Zhang, Q.; Zhu, Z.; Pei, H.; Feng, M.; Sun, T.; Yang, J.; Zhang, X. Comparing the Population Pharmacokinetics of and Acute Kidney Injury Due to Polymyxin B in Chinese Patients with or without Renal Insufficiency. Antimicrob. Agents Chemother. 2021, 65, e01900-20. [Google Scholar] [CrossRef] [PubMed]
- Ting, L.S.L.; Partovi, N.; Levy, R.D.; Ignaszewski, A.P.; Ensom, M.H.H. Performance of Limited Sampling Strategies for Predicting Mycophenolic Acid Area under the Curve in Thoracic Transplant Recipients. J. Heart Lung Transplant. 2008, 27, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Q.; Feng, M.; Sun, T.; Yang, J.; Zhang, X. Population Pharmacokinetics of Polymyxin B in Obese Patients for Resistant Gram-Negative Infections. Front. Pharmacol. 2021, 12, 754844. [Google Scholar] [CrossRef]
- Kubin, C.J.; Nelson, B.C.; Miglis, C.; Scheetz, M.H.; Rhodes, N.J.; Avedissian, S.N.; Cremers, S.; Yin, M.T. Population Pharmacokinetics of Intravenous Polymyxin B from Clinical Samples. Antimicrob. Agents Chemother. 2018, 62, e01493-17. [Google Scholar] [CrossRef] [Green Version]
- Hee, K.H.; Leaw, Y.K.J.; Ong, J.L.; Lee, L.S. Development and Validation of Liquid Chromatography Tandem Mass Spectrometry Method Quantitative Determination of Polymyxin B1, Polymyxin B2, Polymyxin B3 and Isoleucine-Polymyxin B1 in Human Plasma and Its Application in Clinical Studies. J. Pharm. Biomed. Anal. 2017, 140, 91–97. [Google Scholar] [CrossRef]
- He, J.; Gao, S.; Hu, M.; Chow, D.S.-L.; Tam, V.H. A Validated Ultra-Performance Liquid Chromatography-Tandem Mass Spectrometry Method for the Quantification of Polymyxin B in Mouse Serum and Epithelial Lining Fluid: Application to Pharmacokinetic Studies. J. Antimicrob. Chemother. 2013, 68, 1104–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Y.; Peng, B.; Li, L.; Wang, J.; Wang, X.; Qi, G.; Rong, R.; Wang, L.; Qiu, J.; Xu, M.; et al. Estimation of Mycophenolic Acid Area under the Curve with Limited-Sampling Strategy in Chinese Renal Transplant Recipients Receiving Enteric-Coated Mycophenolate Sodium. Ther. Drug Monit. 2017, 39, 29–36. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 30) | Model Group (n = 20) | Validation Group (n = 10) | p Value a |
|---|---|---|---|---|
| No. (%) of patients | ||||
| Sex | 0.431 | |||
| Male | 21 (70) | 15 (75) | 6 (60) | |
| Female | 9 (30) | 5 (25) | 4 (40) | |
| PMB doses (mg/12 h) | ||||
| 40 | 1 (3.3) | 1 (5) | 0 (0) | 0.294 |
| 50 | 18 (60) | 10 (50) | 8 (80) | |
| 75 | 11 (36.7) | 9 (45) | 2 (20) | |
| Infusion duration (h) | 1 | 1 | 1 | |
| Frequency (h) | 12 | 12 | 12 | |
| Mean ± SD or median (interquartile range) | ||||
| Age (years) | 58.86 ± 17.01 | 59.21 ± 16.81 | 58.20 ± 18.27 | 0.882 |
| Total body weight (kg) | 58.73 ± 10.93 | 60.83 ± 11.55 | 54.55 ± 8.60 | 0.141 |
| Height (cm) | 166.17 ± 6.79 | 166.80 ± 6.88 | 164.9 ± 6.77 | 0.480 |
| Total bilirubin (µmol/L) | 47.06 ± 48.30 | 40.13 ± 38.78 | 59.53 ± 62.35 | 0.317 |
| Total protein (g/L) | 56.94 ± 9.15 | 56.19 ± 9.61 | 58.52 ± 8.41 | 0.539 |
| Alanine aminotransferase (U/L) | 35.28 ± 33.47 | 29.89 ± 32.40 | 45.50 ± 34.75 | 0.239 |
| Aspartate aminotransferase (U/L) | 45.17 ± 29.00 | 39.11 ± 19.58 | 56.70 ± 40.30 | 0.122 |
| Glutamyl transpeptidase (U/L) | 74.55 ± 85.18 | 71.53 ± 95.35 | 80.30 ± 65.59 | 0.797 |
| Serum creatinine (µmol/L) | 123.21 ± 83.10 | 126.42 ± 96.03 | 117.10 ± 54.5 | 0.780 |
| Creatinine clearance (mL/min) | 66.37 ± 45.84 | 69.41 ± 45.32 | 60.60 ± 48.72 | 0.631 |
| AUCobs (mg·h/L) | 46.10 (34.02–65.52) | 46.09 (32.36–68.75) | 47.69 (36.40–65.76) | 0.971 |
| Time Point | Equation | MPE% | RMSE% | R | F15% |
|---|---|---|---|---|---|
| C4 | 20.623 × C4 + 2.889 | −2.31 | 10.6 | 0.994 | 90 |
| C0, C1 | 23.006 × C0 + 6.037 × C1 − 1.853 | 1.53 | 6.21 | 0.992 | 100 |
| C1, C2, C8 | 0.600 × C1 + 8.356 × C2 + 14.078 × C8 + 0.997 | 0.44 | 6.9 | 0.992 | 100 |
| C1, C2, C8, C12 | 0.637 × C1 + 8.749 × C2 + 9.749 × C8 + 4.380 × C12 + 0.669 | −0.18 | 6.87 | 0.991 | 100 |
| Time Point | Equation | Reference | MPE% | RMSE% | R | F15% |
|---|---|---|---|---|---|---|
| C6 | 8.147 + 21.961 × C6 | [21] a | 3.71 | 11.57 | 0.993 | 90 |
| C4, C6 | 2.030 + 8.532 × C4 + 13.465 × C6 | [21] | −4.34 | 9.48 | 0.991 | 90 |
| C1.5, C4, C8 | 0.599 + 1.964 × C1.5 + 3.169 × C4 + 6.633 × C8 | [22] b | 0.13 | 3.63 | 0.997 | 100 |
| C1, C1.5, C4, C8 | 0.260 + 0.460 × C1 + 1.137 × C1.5 + 3.644 × C4 + 6.480 × C8 | [22] | −1.84 | 4.26 | 0.998 | 100 |
| Infusion Duration | Time Point | LSSs Equation | Reference | MPE% | RMSE% | R | F15% |
|---|---|---|---|---|---|---|---|
| 0.5 h | C2, C8 | −0.274 + 4.671 × C2 + 7.181 × C8 | [22] a | 2.31 | 18.83 | 0.947 | 83.33 |
| 1 h | C6 | 8.147 + 21.961 × C6 | [21] b | 3.71 | 11.57 | 0.993 | 90.00 |
| C4, C6 | 2.030 + 8.532 × C4 + 13.465 × C6 | [21] | −4.34 | 9.48 | 0.991 | 90.00 | |
| 1.5 h | C4, C8 | 0.196 + 13.903 × C4 + 9.725 × C8 | [21] | 1.90 | 19.85 | 0.942 | 83.33 |
| 2 h | C4, C12 | 0.546 + 14.120 × C4 + 11.235 × C12 | [21] | 1.63 | 18.86 | 0.947 | 83.33 |
| 2.5 h | 4.93 | 19.67 | 0.948 | 83.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Zhang, B.; Cheng, Y.; Chen, M.; Lin, H.; Huang, B.; Que, W.; Liu, M.; Zhou, L.; Weng, Q.; et al. Evaluation and Validation of the Limited Sampling Strategy of Polymyxin B in Patients with Multidrug-Resistant Gram-Negative Infection. Pharmaceutics 2022, 14, 2323. https://doi.org/10.3390/pharmaceutics14112323
Li X, Zhang B, Cheng Y, Chen M, Lin H, Huang B, Que W, Liu M, Zhou L, Weng Q, et al. Evaluation and Validation of the Limited Sampling Strategy of Polymyxin B in Patients with Multidrug-Resistant Gram-Negative Infection. Pharmaceutics. 2022; 14(11):2323. https://doi.org/10.3390/pharmaceutics14112323
Chicago/Turabian StyleLi, Xueyong, Bingqing Zhang, Yu Cheng, Maohua Chen, Hailing Lin, Binglin Huang, Wancai Que, Maobai Liu, Lili Zhou, Qinyong Weng, and et al. 2022. "Evaluation and Validation of the Limited Sampling Strategy of Polymyxin B in Patients with Multidrug-Resistant Gram-Negative Infection" Pharmaceutics 14, no. 11: 2323. https://doi.org/10.3390/pharmaceutics14112323