
Cancer Treatment and Immunotherapy during Pregnancy
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Pregnancy and Oncological Medicines
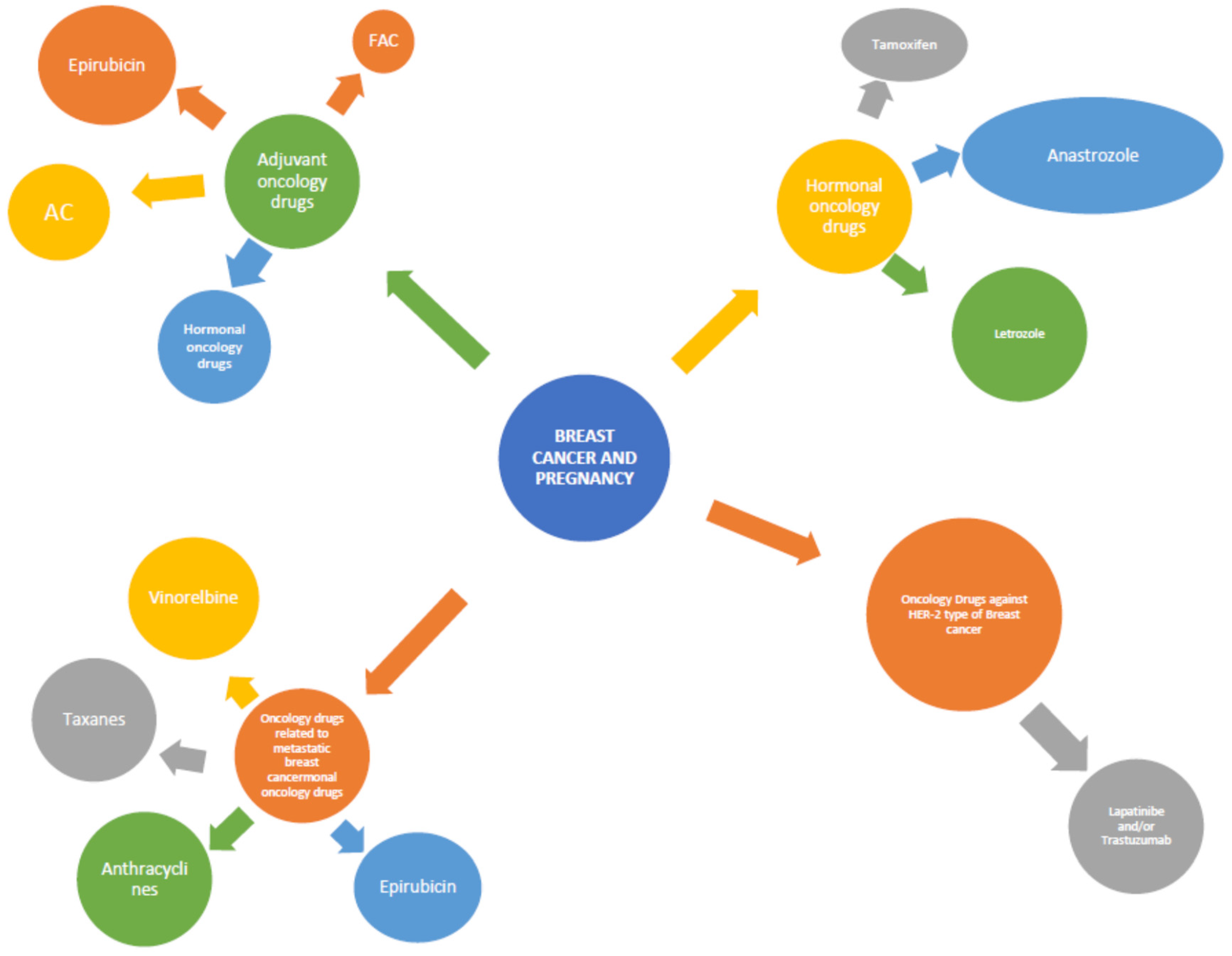
2.1. Pregnancy and Anticancer Drug Treatment for the Breast Cancer
2.1.1. The Adjuvant Oncology Drugs
2.1.2. Hormonal Oncology Drugs
2.1.3. Oncology Drugs against HER-2 Type Breast Cancer
2.1.4. Oncology Drugs Related to Metastatic Breast Cancer
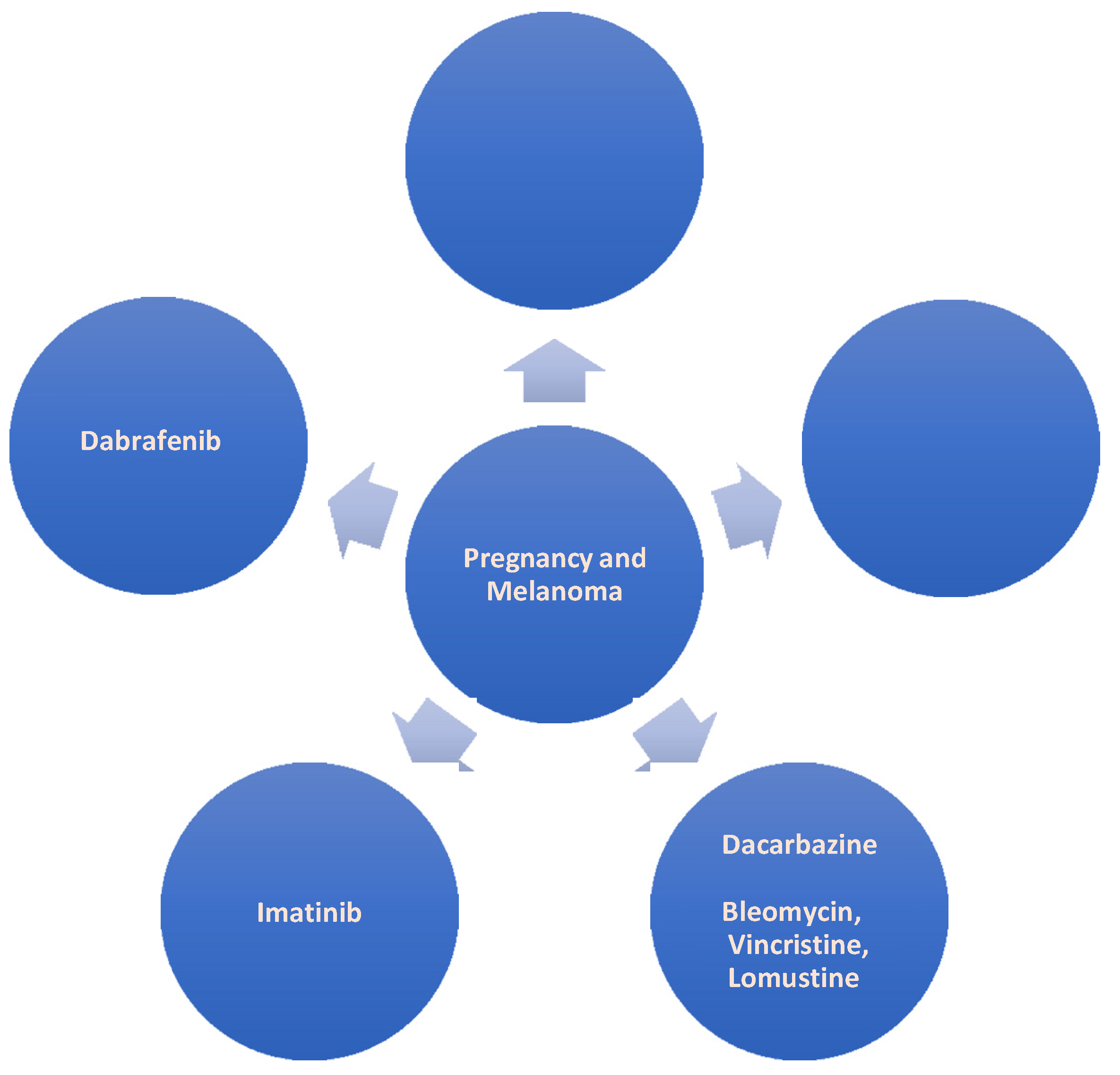
2.2. Pregnancy and Anti-Cancer Drug Treatment for Melanoma (Figure 2)

2.3. Pregnancy and Anti-Cancer Drug Treatment for the Cervix (Figure 3)

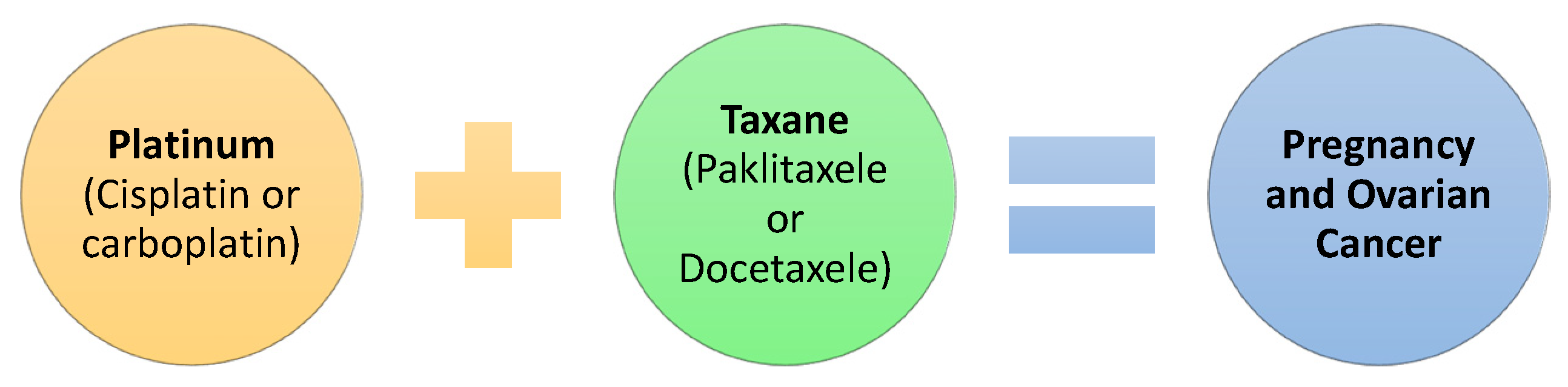
2.4. Pregnancy and Anti-Cancer Drug Treatment for Ovarian Cancer (Figure 4)

2.5. Pregnancy and Anti-Cancer Drug Treatment for Thyroid Cancer
2.6. Pregnancy and Anti-Cancer Drug Treatment of Lymphomas (Figure 5)

- Cyclophosphamide, vincristine, and prednisone (CVP): This therapeutic option does not appear to present significant defects in fetuses if administered after the first three months of gestation [52]. However, it is reported that it can adversely affect the fertility of people of a reproductive age. At the same time, the pregnant woman receiving treatment may experience the following: neutropenia, thrombocytopenia, anemia, alopecia, insomnia, fatigue, peripheral neuropathy, etc. Therefore, the treating physician should be suspicious and closely monitor the progress of the patient [53];
- Cyclophosphamide, vincristine, prednisone, and adriamycin (CHOP): This scheme has proven to be safe if administered after the first trimester but not earlier [52];
2.7. Pregnancy and Other Cancers
2.8. Pregnancy and Lung Cancer
2.9. Pregnancy and Brain Tumors (Figure 6)

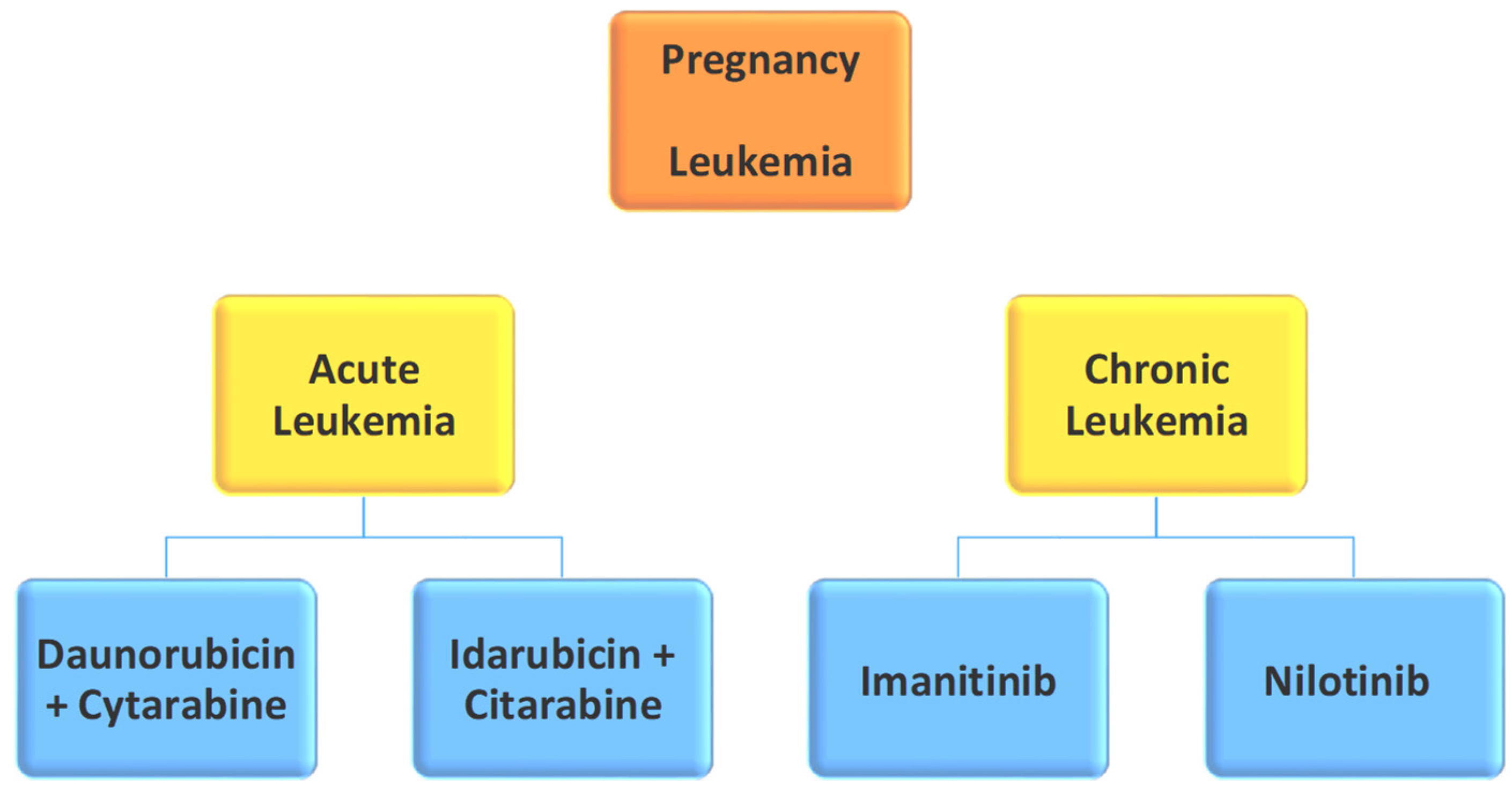
2.10. Pregnancy and Leukemia (Figure 7)

2.11. Pregnancy and Acute Promyelocytic Leukemia
3. Cancer Pregnancy Treatment and Cardiotoxicity
4. Immunotherapy during Pregnancy
5. Cancer Treatment and the Role of Νutraceuticals
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Available online: https://www.cancer.org/cancer/cancer-causes.html (accessed on 10 January 2022).
- McCormick, A.; Peterson, E. Cancer in Pregnancy. Obstet. Gynecol. Clin. N. Am. 2018, 45, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Dotters-Katz, S.; McNeil, M.; Limmer, J.; Kuller, J. Cancer and Pregnancy. Obstet. Gynecol. Surv. 2014, 69, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Albright, C.M.; Wenstrom, K.D. Malignancies in Pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 33, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Maggen, C.; Wolters, V.E.R.A.; Cardonick, E.; Fumagalli, M.; Halaska, M.J.; Lok, C.A.R.; de Haan, J.; Van Tornout, K.; Van Calsteren, K.; Amant, F. Pregnancy and Cancer: The INCIP Project. Curr. Oncol. Rep. 2020, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, J.; Post, A.L.; Chien, A.J.; Olin, R.; Tsai, K.K.; Ngo, Z.; Van Loon, K. Multidisciplinary Management of Cancer during Pregnancy. JCO Oncol. Pract. 2020, 16, 545–557. [Google Scholar] [CrossRef]
- Cubillo, A.; Morales, S.; Goñi, E.; Matute, F.; Muñoz, J.L.; Pérez-Díaz, D.; de Santiago, J.; Rodríguez-Lescure, Á. Multidisciplinary consensus on cancer management during pregnancy. Clin. Transl. Oncol. 2021, 23, 1054–1066. [Google Scholar] [CrossRef]
- Donegan, W.L. Cancer and Pregnancy. CA Cancer J. Clin. 1983, 33, 194–214. [Google Scholar] [CrossRef]
- Pavlidis, N. Coexistence of Pregnancy and Malignancy. Oncologist 2002, 7, 279–287. [Google Scholar] [CrossRef]
- Hampe, M.E.; Rhoton-Vlasak, A.S. Fertility Preservation in Breast Cancer with Case-Based Examples for Guidance. J. Assist. Reprod. Genet. 2020, 37, 717–729. [Google Scholar] [CrossRef]
- Miyamoto, S.; Yamada, M.; Kasai, Y.; Miyauchi, A.; Andoh, K. Anticancer Drugs during Pregnancy. Jpn. J. Clin. Oncol. 2016, 46, 795–804. [Google Scholar] [CrossRef] [Green Version]
- Peccatori, F.A.; Azim, H.A.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G. Cancer, Pregnancy and Fertility: ESMO Clinical Practice Guidelines for Diagnosis, Treatment, and Follow-Up. Ann. Oncol. 2013, 24, vi160–vi170. [Google Scholar] [CrossRef] [PubMed]
- Azim, H.A.; Peccatori, F.A.; Pavlidis, N. Treatment of The Pregnant Mother with Cancer: A Systematic Review on The Use of Cytotoxic, Endocrine, Targeted Agents and Immunotherapy during Pregnancy. Part I: Solid Tumors. Cancer Treat. Rev. 2010, 36, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Peccatori, F.A.; Azim, H.A.; Scarfone, G.; Gadducci, A.; Bonazzi, C.; Gentilini, O.; Galimberti, V.; Intra, M.; Locatelli, M.; Acaia, B.; et al. Weekly Epirubicin in The Treatment of Gestational Breast Cancer (GBC). Breast Cancer Res. Treat. 2008, 115, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Hahn, K.M.E.; Johnson, P.H.; Gordon, N.; Kuerer, H.; Middleton, L.; Ramirez, M.; Yang, W.; Perkins, G.; Hortobagyi, G.N.; Theriault, R.L. Treatment of Pregnant Breast Cancer Patients and Outcomes of Children Exposed to Chemotherapy in Utero. Cancer 2006, 107, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Pereg, D.; Lishner, M. Maternal and Fetal Effects of Systemic Therapy in The Pregnant Woman with Cancer. Recent Results Cancer Res. 2008, 178, 21–38. [Google Scholar] [CrossRef]
- Sharma, G.N.; Dave, R.; Sanadya, J.; Sharma, P.; Sharma, K.K. Various types and management of breast cancer: An overview. J. Adv. Pharm. Technol. Res. 2010, 1, 109–126. [Google Scholar]
- Braems, G.; Denys, H.; De Wever, O.; Cocquyt, V.; Van den Broecke, R. Use of Tamoxifen Before and during Pregnancy. Oncologist 2011, 16, 1547–1551. [Google Scholar] [CrossRef]
- Drugs.com, 2020. Retrieved 2021. Available online: https://www.drugs.com/pregnancy/anastrozole.html (accessed on 29 January 2022).
- Gill, S.K.; Moretti, M.; Koren, G. Is the use of letrozole to induce ovulation teratogenic? Can. Fam. Physician. 2008, 54, 353–354. [Google Scholar]
- Beltrame, D.; di Salle, E.; Giavini, E.; Gunnarsson, K.; Brughera, M. Reproductive Toxicity of Exemestane, An Antitumoral Aromatase Inactivator, in Rats and Rabbits. Reprod. Toxicol. 2001, 15, 195–213, Erratum in Reprod. Toxicol. 2001, 15, 601–602. [Google Scholar] [CrossRef]
- Kharb, R.; Haider, K.; Neha, K.; Yar, M.S. Aromatase Inhibitors: Role in Postmenopausal Breast Cancer. Arch. Pharm. 2020, 353, 2000081. [Google Scholar] [CrossRef]
- Lambertini, M.; Viglietti, G. Pregnancies in Young Women with Diagnosis and Treatment of HER2-Positive Breast Cancer. Oncotarget 2019, 10, 803–804. [Google Scholar] [CrossRef] [PubMed]
- Goodyer, M.J.; Ismail, J.R.; O’Reilly, S.P.; Moylan, E.J.; Ryan, C.A.M.; Hughes, P.A.; O’Connor, A. Safety of Trastuzumab (Herceptin®) during Pregnancy: Two Case Reports. Cases J. 2009, 2, 9329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azim, H.A.; Peccatori, F.A. Treatment of Metastatic Breast Cancer during Pregnancy: We Need to Talk! Breast 2008, 17, 426–428. [Google Scholar] [CrossRef] [PubMed]
- Still, R.; Brennecke, S. Melanoma in Pregnancy. Obstet. Med. 2017, 10, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Grunewald, S.; Jank, A. New systemic agents in dermatology with respect to fertility, pregnancy, and lactation. J. Dtsch. Dermatol. Ges. 2015, 13, 277–290. [Google Scholar] [CrossRef]
- Pye, S.M.; Cortes, J.; Ault, P.; Hatfield, A.; Kantarjian, H.; Pilot, R.; Rosti, G.; Apperley, J.F. The Effects of Imatinib on Pregnancy Outcome. Blood 2008, 111, 5505–5508. [Google Scholar] [CrossRef]
- Ali, R.; Ozkalemkas, F.; Ozcelik, T.; Ozkocaman, V.; Ozkan, A. Imatinib and Pregnancy. J. Clin. Oncol. 2006, 24, 3812–3813. [Google Scholar] [CrossRef]
- Dipaola, R.S.; Goodin, S.; Ratzell, M.; Florczyk, M.; Karp, G.; Ravikumar, T. Chemotherapy for Metastatic Melanoma during Pregnancy. Gynecol. Oncol. 1997, 66, 526–530. [Google Scholar] [CrossRef]
- Pagès, C.; Robert, C.; Thomas, L.; Maubec, E.; Sassolas, B.; Granel-Brocard, F.; Chevreau, C.; De Raucourt, S.; Leccia, M.; Fichet, D.; et al. Management and Outcome of Metastatic Melanoma during Pregnancy. Br. J. Dermatol. 2009, 162, 274–281. [Google Scholar] [CrossRef]
- Vuoristo, M.-S.; Hahka-Kemppinen, M.; Parvinen, L.-M.; Pyrhönen, S.; Seppä, H.; Korpela, M.; Kellokumpu-Lehtinen, P. Randomized Trial of Dacarbazine Versus Bleomycin, Vincristine, Lomustine and Dacarbazine (BOLD) Chemotherapy Combined with Natural Or Recombinant Interferon-α in Patients with Advanced Melanoma. Melanoma Res. 2005, 15, 291–296. [Google Scholar] [CrossRef]
- Jhaveri, M.B.; Driscoll, M.S.; Grant-Kels, J.M. Melanoma in Pregnancy. Clin. Obstet. Gynecol. 2011, 54, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Beharee, N.; Shi, Z.; Wu, D.; Wang, J. Diagnosis and Treatment of Cervical Cancer in Pregnant Women. Cancer Med. 2019, 8, 5425–5430. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Van Calsteren, K.; Halaska, M.J.; Beijnen, J.; Lagae, L.; Hanssens, M.; Heyns, L.; Lannoo, L.; Ottevanger, N.P.; Vanden Bogaert, W.; et al. Gynecologic Cancers in Pregnancy. Int. J. Gynecol. Cancer 2009, 19, S1–S12. [Google Scholar] [CrossRef] [PubMed]
- Fruscio, R.; de Haan, J.; Van Calsteren, K.; Verheecke, M.; Mhallem, M.; Amant, F. Ovarian Cancer in Pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 41, 108–117. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E. New Treatments in Ovarian Cancer. Ann. Oncol. 2017, 28, viii57–viii60. [Google Scholar] [CrossRef]
- Méndez, L.E.; Mueller, A.; Salom, E.; González-Quintero, V.H. Paclitaxel and Carboplatin Chemotherapy Administered during Pregnancy for Advanced Epithelial Ovarian Cancer. Obstet. Gynecol. 2003, 102, 1200–1202. [Google Scholar]
- Mir, O.; Berveiller, P.; Ropert, S.; Goffinet, F.; Goldwasser, F. Use of Platinum Derivatives during Pregnancy. Cancer 2008, 113, 3069–3074. [Google Scholar] [CrossRef]
- Serkies, K.; Węgrzynowicz, E.; Jassem, J. Paclitaxel and Cisplatin Chemotherapy for Ovarian Cancer during Pregnancy: Case Report and Review of The Literature. Arch. Gynecol. Obstet. 2011, 283, 97–100. [Google Scholar] [CrossRef]
- Ghaemmaghami, F.; Abbasi, F.; Abadi, A.G.N. A Favorable Maternal and Neonatal Outcome Following Chemotherapy with Etoposide, Bleomycin, and Cisplatin for Management of Grade 3 Immature Teratoma of The Ovary. J. Gynecol. Oncol. 2009, 20, 257–259. [Google Scholar] [CrossRef]
- Sema, Y.; Aysun, F.; Abdullah, Y.; Ethem, U. The Follow-Up of Thyroid Disease in 188 Pregnant Women According to The Guidelines of ATA (American Thyroid Association) 2017. Reprod. Med. Int. 2020, 3. [Google Scholar] [CrossRef]
- Khaled, H.; Al Lahloubi, N.; Rashad, N. A Review on Thyroid Cancer during Pregnancy: Multitasking Is Required. J. Adv. Res. 2016, 7, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L.; Newbold, K.; Papotti, M.; Berruti, A. Thyroid Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment, and Follow-Up. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef] [PubMed]
- Østensen, M.; Khamashta, M.; Lockshin, M.; Parke, A.; Brucato, A.; Carp, H.; Doria, A.; Rai, R.; Meroni, P.L.; Cetin, I.; et al. Anti-inflammatory and immunosuppressive drugs and reproduction. Arthritis. Res. Ther. 2006, 8, 209. [Google Scholar] [CrossRef] [Green Version]
- Imran, S.A.; Rajaraman, M. Management of Differentiated Thyroid Cancer in Pregnancy. J. Thyroid. Res. 2011, 2011, 549609. [Google Scholar] [CrossRef] [PubMed]
- Pereg, D.; Koren, G.; Lishner, M. The Treatment of Hodgkin’s and Non-Hodgkin’s Lymphoma in Pregnancy. Haematologica 2007, 92, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Bachanova, V.; Connors, J.M. Hodgkin Lymphoma in Pregnancy. Curr. Hematol. Malig. Rep. 2013, 8, 211–217. [Google Scholar] [CrossRef]
- Wolters, V.; Heimovaara, J.; Maggen, C.; Cardonick, E.; Boere, I.; Lenaerts, L.; Amant, F. Management of pregnancy in women with cancer. Int. J. Gynecol. Cancer 2021, 31, 314–322. [Google Scholar] [CrossRef]
- Cotteret, C.; Pham, Y.-V.; Marcais, A.; Driessen, M.; Cisternino, S.; Schlatter, J. Maternal ABVD Chemotherapy for Hodgkin Lymphoma in a Dichorionic Diamniotic Pregnancy: A Case Report. BMC Pregnancy Childbirth 2020, 20, 231. [Google Scholar] [CrossRef]
- Avilés, A.; Neri, N. Hematological Malignancies and Pregnancy: A Final Report of 84 Children Who Received Chemotherapy in Utero. Clin. Lymphoma 2001, 2, 173–177. [Google Scholar] [CrossRef]
- Moshe, Y.; Bentur, O.S.; Lishner, M.; Avivi, I. The Management of Hodgkin Lymphomas in Pregnancies. Eur. J. Haematol. 2017, 99, 385–391. [Google Scholar] [CrossRef]
- Marcus, R.; Imrie, K.; Belch, A.; Cunningham, D.; Flores, E.; Catalano, J.; Solal-Celigny, P.; Offner, F.; Walewski, J.; Raposo, J.; et al. CVP Chemotherapy Plus Rituximab Compared with CVP As First-Line Treatment for Advanced Follicular Lymphoma. Blood 2005, 105, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Dawson, A.L.; Riehle-Colarusso, T.; Reefhuis, J.; Arena, J.F.; the National Birth Defects Prevention Study. Maternal Exposure to Methotrexate and Birth Defects: A Population-Based Study. Am. J. Med. Genet. A 2014, 164, 2212–2216. [Google Scholar] [CrossRef] [PubMed]
- Mantilla-Rivas, E.; Brennan, A.; Goldrich, A.; Bryant, J.R.; Oh, A.K.; Rogers, G.F. Extremity Findings of Methotrexate Embryopathy. Hand 2019, 15, NP14–NP21. [Google Scholar] [CrossRef] [PubMed]
- Yates, R.; Zhang, J. Lung Cancer in Pregnancy: An Unusual Case of Complete Response to Chemotherapy. Cureus 2015, 7, e440. [Google Scholar] [CrossRef]
- Mitrou, S.; Petrakis, D.; Fotopoulos, G.; Zarkavelis, G.; Pavlidis, N. Lung Cancer during Pregnancy: A Narrative Review. J. Adv. Res. 2016, 7, 571–574. [Google Scholar] [CrossRef]
- Van Calsteren, K.; Heyns, L.; De Smet, F.; Van Eycken, L.; Gziri, M.M.; Van Gemert, W.; Halaska, M.; Vergote, I.; Ottevanger, N.; Amant, F. Cancer during Pregnancy: An Analysis of 215 Patients Emphasizing The Obstetrical and The Neonatal Outcomes. J. Clin. Oncol. 2010, 28, 683–689. [Google Scholar] [CrossRef]
- Blumenthal, D.T.; Parreño, M.G.H.; Batten, J.; Chamberlain, M.C. Management of Malignant Gliomas during Pregnancy. Cancer 2008, 113, 3349–3354. [Google Scholar] [CrossRef]
- Evans, A.C.; Nelson, M.B.; Dhall, G. Pregnancy in a Patient with a Malignant Brain Tumor Taking Temozolomide. J. Pediatr. Oncol. Nurs. 2015, 32, 326–328. [Google Scholar] [CrossRef]
- Nolan, S.; Czuzoj-Shulman, N.; Abenhaim, H.A. Pregnancy Outcomes among Leukemia Survivors: A Population-Based Study on 14.5 Million Births. J. Matern. Fetal. Neonatal. Med. 2019, 34, 2283–2289. [Google Scholar] [CrossRef]
- Webb, M.J.; Jafta, D. Imatinib Use in Pregnancy. Turk. J. Haematol. 2012, 29, 405–408. [Google Scholar] [CrossRef]
- Abruzzese, E.; Trawinska, M.M.; De Fabritiis, P.; Perrotti, A.P. Tyrosine kinase inhibitors and pregnancy. Mediterr. J. Hematol. Infect. Dis. 2014, 6, e2014028. [Google Scholar] [CrossRef] [PubMed]
- Fracchiolla, N.S.; Sciumè, M.; Dambrosi, F.; Guidotti, F.; Ossola, M.W.; Chidini, G.; Gianelli, U.; Merlo, D.; Cortelezzi, A. Acute Myeloid Leukemia and Pregnancy: Clinical Experience from a Single Center and a Review of The Literature. BMC Cancer 2017, 17, 442. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Patel, S. Treatment of Acute Myeloid Leukemia during Pregnancy. Ann. Pharmacother. 2014, 49, 48–68. [Google Scholar] [CrossRef] [PubMed]
- Santolaria, A.; Perales, A.; Montesinos, P.; Sanz, M.A. Acute Promyelocytic Leukemia during Pregnancy: A Systematic Review of The Literature. Cancers 2020, 12, 968. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Giri, S.; Manandhar, S.; Pathak, R.; Bhatt, V. Acute Promyelocytic Leukemia during Pregnancy: A Systematic Analysis of Outcome. Leuk. Lymphoma 2015, 57, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.A.; Wiernik, P.H.; Kleiner, G.J. Acute Promyelocytic Leukemia and Pregnancy. a Case Report. Cancer 1995, 76, 2237–2241. [Google Scholar] [CrossRef]
- Sham, R.L. All-Trans Retinoic Acid-Induced Labor in a Pregnant Patient with Acute Promyelocytic Leukemia. Am. J. Hematol. 1996, 53, 145. [Google Scholar] [CrossRef]
- Herrmann, J. Adverse Cardiac Effects of Cancer Therapies: Cardiotoxicity and Arrhythmia. Nat. Rev. Cardiol. 2020, 17, 474–502. [Google Scholar] [CrossRef]
- Sachdeva, V.; Roy, A.; Bharadvaja, N. Current Prospects of Nutraceuticals: A Review. Curr. Pharm. Biotechnol. 2020, 21, 884–896. [Google Scholar] [CrossRef]
- Barbarisi, M.; Iaffaioli, R.V.; Armenia, E.; Schiavo, L.; De Sena, G.; Tafuto, S.; Barbarisi, A.; Quagliariello, V. Novel Nanohydrogel of Hyaluronic Acid Loaded with Quercetin Alone and in Combination with Temozolomide As New Therapeutic Tool, CD44 Targeted Based, of Glioblastoma Multiforme. J. Cell. Physiol. 2018, 233, 6550–6564. [Google Scholar] [CrossRef]
- Mathews, T.J.; Hamilton, B.E. Mean age of mothers is on the rise: United states, 2000–2014. NCHS Data Brief 2016, 232, 1–8. [Google Scholar]
- Food and Drug Administration, HHS. Content and format of labeling for human prescription drug and biological products; requirements for pregnancy and lactation labeling. final rule. Fed. Regist. 2014, 79, 72063–72103. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25509060 (accessed on 1 March 2022).
- Bucheit, A.D.; Hardy, J.T.; Szender, J.B.; Glitza Oliva, I.C. Conception and viable twin pregnancy in a patient with metastatic melanoma while treated with CTLA-4 and PD-1 checkpoint inhibition. Melanoma Res. 2020, 30, 423–425. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Kim, K.B.; Minor, D.R. Case report of a pregnancy during ipilimumab therapy. J. Glob. Oncol. 2018, 4, 1–3. [Google Scholar] [CrossRef]
- Xu, W.; Moor, R.J.; Walpole, E.T.; Atkinson, V.G. Pregnancy with successful fetal and maternal outcome in a melanoma patient treated with nivolumab in the first trimester: Case report and review of the literature. Melanoma Res. 2019, 29, 333–337. [Google Scholar] [CrossRef]
- Haiduk, J.; Ziemer, M. Pregnancy in a patient with metastatic uveal melanoma treated with nivolumab. J. Dtsch. Dermatol. Ges. 2021, 19, 762–765. [Google Scholar] [CrossRef]
- Polnaszek, B.; Mullen, M.; Bligard, K.; Raghuraman, N.; Massad, L.S. Term pregnancy after complete response of placental site trophoblastic tumor to immunotherapy. Obstet. Gynecol. 2021, 138, 115–118. [Google Scholar] [CrossRef]
- Burotto, M.; Gormaz, J.G.; Samtani, S.; Valls, N.; Silva, R.; Rojas, C.; Portiño, S.; de la Jara, C. Viable pregnancy in a patient with metastatic melanoma treated with double checkpoint immunotherapy. Semin. Oncol. 2018, 45, 164–169. [Google Scholar] [CrossRef]
- Menzer, C.; Beedgen, B.; Rom, J.; Duffert, C.M.; Volckmar, A.-L.; Sedlaczek, O.; Richtig, E.; Enk, A.; Jäger, D.; Hassel, J.C. Immunotherapy with ipilimumab plus nivolumab in a stage IV melanoma patient during pregnancy. Eur. J. Cancer 2018, 104, 239–242. [Google Scholar] [CrossRef]
- National Toxicology Program. NTP Monograph: Developmental Effects and Pregnancy Outcomes Associated with Cancer Chemotherapy Use during Pregnancy. NTP Monogr. 2013, 2, 214. [Google Scholar]
- Mubarak, A.A.S.; Kakil, I.R.; Awidi, A.; Al-Homsi, U.; Fawzi, Z.; Kelta, M.; Al-Hassan, A. Normal outcome of pregnancy in chronic myeloid leukemia treated with interferon-alpha in 1st trimester: Report of 3 cases and review of the literature. Am. J. Hematol. 2002, 69, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.R.; Hale, T.W.; Mock, R.E. Transfer of interferon alfa into human breast milk. J. Hum. Lact. 2000, 16, 226–228. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Tissue | Therapeutic Choice | |||||
|---|---|---|---|---|---|---|
| Breast Cancer | (Adjuvant drugs) | FAC | Epirubicin | AC | ||
| (Hormonal treatment) | Anastrozole | Letrozole | Tamoxifen | |||
| (Anti Her 2) | Lapatinib | Trastuzumab | ||||
| (Metastatic cancer) | Epirubicin | Taxanes | Vinorelbine | Anthracyclines | ||
| Melanoma | Cisplatin | Imatinib | Dabrafenib | Ipilimumab | Decarbazine + Bleomycine, Vincristine, Lomustine | |
| Cervical Cancer | Cisplatin | Paclitaxel | Carboplatin | |||
| Ovarian Cancer | Taxanes (Paclitaxele/Docetaxele) | Platinum (Cisplatin/Carboplatin) | ||||
| Lymphomas | (Hodgkin) | MOPP | ABVD | |||
| (Non-Hodgkin) | Methotrexate | CVP | CHOP | |||
| Brain Tumors | Temozolomide | PCV | ||||
| Leukemia | Acute | Daunorubicin | Cytarabine | Idarubicin | ||
| Chronic | Imatinib | Nilotinib | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koutras, A.; Ntounis, T.; Fasoulakis, Z.; Papalios, T.; Pittokopitou, S.; Prokopakis, I.; Syllaios, A.; Valsamaki, A.; Chionis, A.; Symeonidis, P.; et al. Cancer Treatment and Immunotherapy during Pregnancy. Pharmaceutics 2022, 14, 2080. https://doi.org/10.3390/pharmaceutics14102080
Koutras A, Ntounis T, Fasoulakis Z, Papalios T, Pittokopitou S, Prokopakis I, Syllaios A, Valsamaki A, Chionis A, Symeonidis P, et al. Cancer Treatment and Immunotherapy during Pregnancy. Pharmaceutics. 2022; 14(10):2080. https://doi.org/10.3390/pharmaceutics14102080
Chicago/Turabian StyleKoutras, Antonios, Thomas Ntounis, Zacharias Fasoulakis, Theodoros Papalios, Savia Pittokopitou, Ioannis Prokopakis, Athanasios Syllaios, Asimina Valsamaki, Athanasios Chionis, Panagiotis Symeonidis, and et al. 2022. "Cancer Treatment and Immunotherapy during Pregnancy" Pharmaceutics 14, no. 10: 2080. https://doi.org/10.3390/pharmaceutics14102080