
Goals and Challenges of Stem Cell-Based Therapy for Corneal Blindness Due to Limbal Deficiency

 , , , ,
, , , ,
Abstract
:1. Introduction
2. The Past: The Beginnings of Stem Cell-Based Therapy for Corneal Failure
3. The Present: Available Stem Cell-Based Therapies
3.1. Cultivated Limbal Epithelial Transplantation
3.2. Autologous Non-Limbal Epithelial Cell Transplantation
3.3. Allogeneic Non-Limbal Stem Cell-Based Transplantation
3.4. Regulatory Status of Stem Cell-Based Therapy for Treatment of LSCD in Different Countries
4. The Future: Challenges to Overcome in Stem Cell-Based Therapies
4.1. Clinical Challenges
4.2. Preclinical Challenges
4.2.1. Analysis of the Corneal Epithelium after Stem Cell-Based Transplantation
4.2.2. The Need to Reconstruct the Limbal Stem Cell Niche
4.2.3. Alternative Routes of Delivering Stem Cell-Therapy
4.2.4. Other Potential Sources of Non-Limbal Cells
Embryonic Stem Cells
Induced Pluripotent Stem Cells
Dental Pulp Stem Cells
Hair Follicle Bulge-Derived Epithelial Stem Cells
Amniotic Membrane Epithelial Cells
Umbilical Cord Lining Epithelial Cells
4.3. Regulatory Challenges
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dhamodaran, K.; Subramani, M.; Ponnalagu, M.; Shetty, R.; Das, D. Ocular stem cells: A status update! Stem Cell Res. Ther. 2014, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Ramos, T.; Scott, D.; Ahmad, S. An Update on Ocular Surface Epithelial Stem Cells: Cornea and Conjunctiva. Stem Cells Int. 2015, 2015, 601731. [Google Scholar] [CrossRef] [Green Version]
- Schwab, I.R. Cultured corneal epithelia for ocular surface disease. Trans. Am. Ophthalmol. Soc. 1999, 97, 891–986. [Google Scholar]
- Mann, I. A Study of Epithelial Regeneration in the Living Eye. Br. J. Ophthalmol. 1944, 28, 26–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedenwald, J.S.; Buschke, W. Some Factors Concerned in the Mitotic and Wound-Healing Activities of the Corneal Epithelium. Trans. Am. Ophthalmol. Soc. 1944, 42, 371–383. [Google Scholar]
- Maumenee, A. Repair in cornea. Adv. Biol. Ski. 1964, 5, 208–215. [Google Scholar]
- Davanger, M.; Evensen, A. Role of the pericorneal papillary structure in renewal of corneal epithelium. Nature 1971, 229, 560–561. [Google Scholar] [CrossRef]
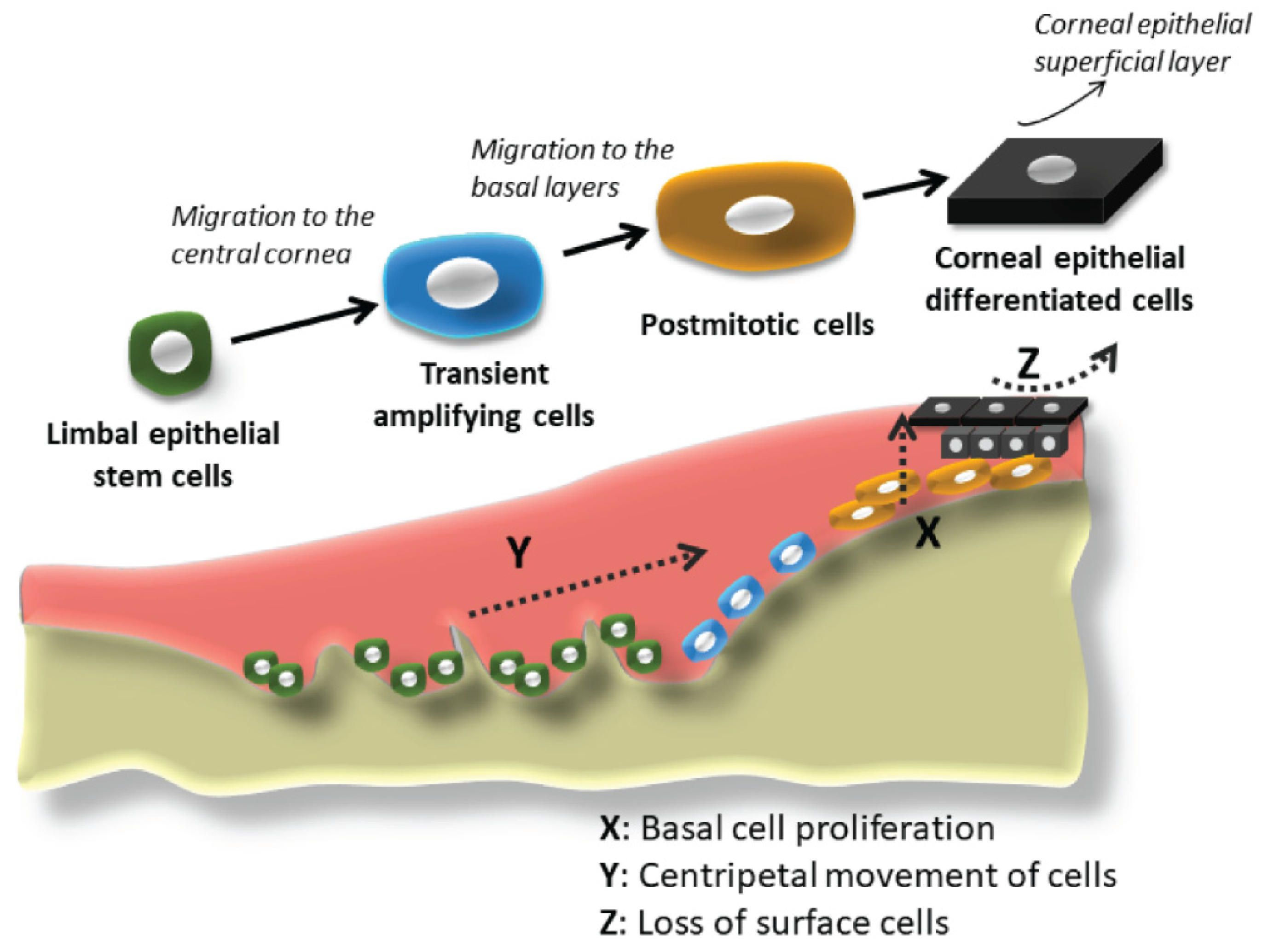
- Thoft, R.A.; Friend, J. The X, Y, Z hypothesis of corneal epithelial maintenance. Investig. Ophthalmol. Vis. Sci. 1983, 24, 1442–1443. [Google Scholar]
- Kinoshita, S.; Friend, J.; Thoft, R.A. Sex chromatin of donor corneal epithelium in rabbits. Investig. Ophthalmol. Vis. Sci. 1981, 21, 434–441. [Google Scholar]
- Schermer, A.; Galvin, S.; Sun, T.T. Differentiation-related expression of a major 64K corneal keratin in vivo and in culture suggests limbal location of corneal epithelial stem cells. J. Cell Biol. 1986, 103, 49–62. [Google Scholar] [CrossRef]
- Guo, P.; Sun, H.; Zhang, Y.; Tighe, S.; Chen, S.; Su, C.W.; Liu, Y.; Zhao, H.; Hu, M.; Zhu, Y. Limbal niche cells are a potent resource of adult mesenchymal progenitors. J. Cell. Mol. Med. 2018, 22, 3315–3322. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.X.; Borderie, V.; Chan, C.C.; Dana, R.; Figueiredo, F.C.; Gomes, J.A.; Pellegrini, G.; Shimmura, S.; Kruse, F.E. Global consensus on definition, classification, diagnosis, and staging of limbal stem cell deficiency. Cornea 2019, 38, 364–375. [Google Scholar] [CrossRef]
- Nakamura, T.; Inatomi, T.; Sotozono, C.; Koizumi, N.; Kinoshita, S. Ocular surface reconstruction using stem cell and tissue engineering. Prog. Retin. Eye Res. 2016, 51, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, K.R.; Tseng, S.C. Limbal Autograft Transplantation for Ocular Surface Disorders. Ophthalmology 1989, 96, 709–722. [Google Scholar] [CrossRef]
- Ballios, B.G.; Weisbrod, M.; Chan, C.C.; Borovik, A.; Schiff, J.R.; Tinckam, K.J.; Humar, A.; Kim, S.J.; Cole, E.H.; Slomovic, A.R. Systemic immunosuppression in limbal stem cell transplantation: Best practices and future challenges. Can. J. Ophthalmol. 2018, 53, 314–323. [Google Scholar] [CrossRef]
- Ozer, M.D.; Altinkurt, E.; Yilmaz, Y.C.; Gedik, A.C.; Alparslan, N. The surgical outcomes of limbal allograft transplantation in eyes having limbal stem cell deficiency. J. Curr. Ophthalmol. 2020, 32, 132–141. [Google Scholar] [CrossRef]
- Cheung, A.Y.; Eslani, M.; Kurji, K.H.; Wright, E.; Sarnicola, E.; Govil, A.; Holland, E.J. Long-term outcomes of living-related conjunctival limbal allograft compared with keratolimbal allograft in patients with limbal stem cell deficiency. Cornea 2020, 39, 980–985. [Google Scholar] [CrossRef]
- Sangwan, V.S.; Basu, S.; MacNeil, S.; Balasubramanian, D. Simple limbal epithelial transplantation (SLET): A novel surgical technique for the treatment of unilateral limbal stem cell deficiency. Br. J. Ophthalmol. 2012, 96, 931–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, C.J.; Myklebust Ernø, I.T.; Ringstad, H.; Tønseth, K.A.; Dartt, D.A.; Utheim, T.P. Simple limbal epithelial transplantation: Current status and future perspectives. Stem Cells Transl. Med. 2020, 9, 316–327. [Google Scholar] [CrossRef] [Green Version]
- Amescua, G.; Atallah, M.; Nikpoor, N.; Galor, A.; Perez, V.L. Modified simple limbal epithelial transplantation using cryopreserved amniotic membrane for unilateral limbal stem cell deficiency. Am. J. Ophthalmol. 2014, 158, 469–475.e2. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Patel, C.; Goyal, R.; Donthineni, P.; Singh, V.; Basu, S. Simple limbal epithelial transplantation (SLET): Review of indications, surgical technique, mechanism, outcomes, limitations, and impact. Indian J. Ophthalmol. 2019, 67, 1265–1277. [Google Scholar] [CrossRef]
- Pellegrini, G.; Traverso, C.E.; Franzi, A.T.; Zingirian, M.; Cancedda, R.; De Luca, M. Long-term restoration of damaged corneal surfaces with autologous cultivated corneal epithelium. Lancet 1997, 349, 990–993. [Google Scholar] [CrossRef]
- Notara, M.; Alatza, A.; Gilfillan, J.; Harris, A.R.; Levis, H.J.; Schrader, S.; Vernon, A.; Daniels, J.T. In sickness and in health: Corneal epithelial stem cell biology, pathology and therapy. Exp. Eye Res. 2010, 90, 188–195. [Google Scholar] [CrossRef]
- Ramírez, B.E.; Sánchez, A.; Herreras, J.M.; Fernández, I.; García-Sancho, J.; Nieto-Miguel, T.; Calonge, M. Stem Cell Therapy for Corneal Epithelium Regeneration following Good Manufacturing and Clinical Procedures. Biomed Res. Int. 2015, 2015, 408495. [Google Scholar] [CrossRef] [Green Version]
- Angunawela, R.I.; Mehta, J.S.; Daniels, J.T. Ex-vivo ocular surface stem cell therapies: Current techniques, applications, hurdles and future directions. Expert Rev. Mol. Med. 2013, 15, e4. [Google Scholar] [CrossRef]
- CCG Tseng, S.; Chen, S.Y.; Shen, Y.C.; Chen, W.L.; Hu, F.R. Critical Appraisal of Ex Vivo Expansion of Human Limbal Epithelial Stem Cells. Curr. Mol. Med. 2010, 10, 841–850. [Google Scholar] [CrossRef]
- Dua, H.S.; Miri, A.; Said, D.G. Contemporary limbal stem cell transplantation—A review. Clin. Exp. Ophthalmol. 2010, 38, 104–117. [Google Scholar] [CrossRef] [PubMed]
- Baylis, O.; Figueiredo, F.; Henein, C.; Lako, M.; Ahmad, S. 13 Years of cultured limbal epithelial cell therapy: A review of the outcomes. J. Cell. Biochem. 2011, 112, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Oie, Y.; Nishida, K. Regenerative medicine for the cornea. Biomed Res. Int. 2013, 2013, 428247. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, G.; Rama, P.; Di Rocco, A.; Panaras, A.; De Luca, M. Concise review: Hurdles in a successful example of limbal stem cell-based regenerative medicine. Stem Cells 2014, 32, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Sangwan, V.S.; Jain, R.; Basu, S.; Bagadi, A.B.; Sureka, S.; Mariappan, I.; Macneil, S. Transforming ocular surface stem cell research into successful clinical practice. Indian J. Ophthalmol. 2014, 62, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Genicio, N.; Gallo Paramo, J.; Shortt, A.J. Quantum dot labeling and tracking of cultured limbal epithelial cell transplants in vitro. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3051–3059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedrotti, E.; Passilongo, M.; Fasolo, A.; Nubile, M.; Parisi, G.; Mastropasqua, R.; Ficial, S.; Bertolin, M.; Di Iorio, E.; Ponzin, D.; et al. In Vivo Confocal Microscopy 1 Year after Autologous Cultured Limbal Stem Cell Grafts. Ophthalmology 2015, 122, 1660–1668. [Google Scholar] [CrossRef] [PubMed]
- Ghareeb, A.E.; Lako, M.; Figueiredo, F.C. Recent Advances in Stem Cell Therapy for Limbal Stem Cell Deficiency: A Narrative Review. Ophthalmol. Ther. 2020, 9, 809–831. [Google Scholar] [CrossRef]
- European Medicines Agency. EU/3/08/579. Available online: https://www.ema.europa.eu/en/medicines/human/orphan-designations/eu308579 (accessed on 6 November 2020).
- Rama, P.; Matuska, S.; Paganoni, G.; Spinelli, A.; De Luca, M.; Pellegrini, G. Limbal Stem-Cell Therapy and Long-Term Corneal Regeneration. N. Engl. J. Med. 2010, 363, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, G.; Ardigò, D.; Milazzo, G.; Iotti, G.; Guatelli, P.; Pelosi, D.; De Luca, M. Navigating Market Authorization: The Path Holoclar Took to Become the First Stem Cell Product Approved in the European Union. Stem Cells Transl. Med. 2018, 7, 146–154. [Google Scholar] [CrossRef] [Green Version]
- López-Paniagua, M.; de la Mata, A.; Galindo, S.; Blázquez, F.; Calonge, M.; Nieto-Miguel, T. Advanced therapy medicinal products for the eye: Definitions and regulatory framework. Pharmaceutics 2021, 13, 347. [Google Scholar] [CrossRef]
- Gay, M.H.; Baldomero, H.; Farge-Bancel, D.; Robey, P.G.; Rodeo, S.; Passweg, J.; Müller-Gerbl, M.; Martin, I. The survey on cellular and tissue-engineered therapies in Europe in 2016 and 2017. Tissue Eng. Part A 2021, 27, 336–350. [Google Scholar] [CrossRef] [PubMed]
- Le, Q.; Chauhan, T.; Yung, M.; Tseng, C.H.; Deng, S.X. Outcomes of Limbal Stem Cell Transplant: A Meta-analysis. JAMA Ophthalmol. 2020, 138, 660–670. [Google Scholar] [CrossRef]
- Mishan, M.A.; Yaseri, M.; Baradaran-Rafii, A.; Kanavi, M.R. Systematic review and meta-analysis investigating autograft versus allograft cultivated limbal epithelial transplantation in limbal stem cell deficiency. Int. Ophthalmol. 2019, 39, 2685–2696. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, N.; Inatomi, T.; Suzuki, T.; Sotozono, C.; Kinoshita, S. Cultivated corneal epithelial stem cell transplantation in ocular surface disorders. Ophthalmology 2001, 108, 1569–1574. [Google Scholar] [CrossRef]
- Regulation (EC) No 1394/2007 of the European Parliament and of the Council of 13 November 2007 on Advance Therapy Medicinal Products and Amending Directive 2001/83/EC and Regulation /EC) N0 726/2004. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2007:324:0121:0137:en:PDF (accessed on 29 July 2021).
- Commission Directive 2003/94/EC of 8 October 2003 Laying down the Principles and Guidelines of Good Manufacturing Practice in Respect of Medicinal Products for Human Use and Investigational Medicinal Products for Human Use. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2003:262:0022:0026:en:PDF (accessed on 29 July 2021).
- Zhao, Y.; Ma, L. Systematic review and meta-analysis on transplantation of ex vivo cultivated limbal epithelial stem cell on amniotic membrane in limbal stem cell deficiency. Cornea 2015, 34, 592–600. [Google Scholar] [CrossRef]
- Shortt, A.J.; Secker, G.A.; Notara, M.D.; Limb, G.A.; Khaw, P.T.; Tuft, S.J.; Daniels, J.T. Transplantation of Ex Vivo Cultured Limbal Epithelial Stem Cells: A Review of Techniques and Clinical Results. Surv. Ophthalmol. 2007, 52, 483–502. [Google Scholar] [CrossRef] [PubMed]
- Borderie, V.M.; Ghoubay, D.; Georgeon, C.; Borderie, M.; de Sousa, C.; Legendre, A.; Rouard, H. Long-Term Results of Cultured Limbal Stem Cell Versus Limbal Tissue Transplantation in Stage III Limbal Deficiency. Stem Cells Transl. Med. 2019, 8, 1230–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobba, S.; Chow, S.; Watson, S.; Di Girolamo, N. Clinical outcomes of xeno-free expansion and transplantation of autologous ocular surface epithelial stem cells via contact lens delivery: A prospective case series. Stem Cell Res. Ther. 2015, 6, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Hayashida, Y.; Chen, Y.T.; Tseng, S.C. Niche regulation of corneal epithelial stem cells at the limbus. Cell Res. 2007, 17, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Shimazaki, J.; Higa, K.; Kato, N.; Satake, Y. Barrier function of cultivated limbal and oral mucosal epithelial cell sheets. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5672–5680. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, H.; Yamato, M.; Nishida, K.; Okano, T. Evidence of the survival of ectopically transplanted oral mucosal epithelial stem cells after repeated wounding of cornea. Mol. Ther. 2014, 22, 1544–1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashida, Y.; Nishida, K.; Yamato, M.; Watanabe, K.; Maeda, N.; Watanabe, H.; Kikuchi, A.; Okano, T.; Tano, Y. Ocular surface reconstruction using autologous rabbit oral mucosal epithelial sheets fabricated ex vivo on a temperature-responsive culture surface. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Endo, K.I.; Cooper, L.J.; Fullwood, N.J.; Tanifuji, N.; Tsuzuki, M.; Koizumi, N.; Inatomi, T.; Sano, Y.; Kinoshita, S. The successful culture and autologous transplantation of rabbit oral mucosal epithelial cells on amniotic membrane. Investig. Ophthalmol. Vis. Sci. 2003, 44, 106–116. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Inatomi, T.; Sotozono, C.; Amemiya, T.; Kanamura, N.; Kinoshita, S. Transplantation of cultivated autologous oral mucosal epithelial cells in patients with severe ocular surface disorders. Br. J. Ophthalmol. 2004, 88, 1280–1284. [Google Scholar] [CrossRef] [PubMed]
- Cabral, J.V.; Jackson, C.J.; Utheim, T.P.; Jirsova, K. Ex vivo cultivated oral mucosal epithelial cell transplantation for limbal stem cell deficiency: A review. Stem Cell Res. Ther. 2020, 11, 301. [Google Scholar] [CrossRef] [PubMed]
- Duan, C.Y.; Xie, H.T.; Zhao, X.Y.; Xu, W.H.; Zhang, M.C. Limbal niche cells can reduce the angiogenic potential of cultivated oral mucosal epithelial cells. Cell. Mol. Biol. Lett. 2019, 24, 3. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.C.; Chen, H.L.; Lai, J.Y.; Chen, C.C.; Tsai, Y.J.; Kuo, M.T.; Chu, P.H.; Sun, C.C.; Chen, J.K.; Ma, D.H. Persistence of transplanted oral mucosal epithelial cells in human cornea. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4660–4668. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Qi, X.; Dong, Y.; Cheng, J.; Zhai, H.; Zhou, Q.; Xie, L. Comparison of the efficacy of different cell sources for transplantation in total limbal stem cell deficiency. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1253–1263. [Google Scholar] [CrossRef]
- Samoila, O.; Gocan, D. Clinical Outcomes From Cultivated Allogenic Stem Cells vs. Oral Mucosa Epithelial Transplants in Total Bilateral Stem Cells Deficiency. Front. Med. 2020, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieto-Miguel, T.; Galindo, S.; López-Paniagua, M.; Pérez, I.; Herreras, J.M.; Calonge, M. Cell Therapy Using Extraocular Mesenchymal Stem Cells. In Corneal Regeneration Therapy and Surgery; Alió, J., Alió del Barrio, J.L., Arnalich-Montiel, F., Eds.; Springer Nature: Basingstoke, UK, 2019; pp. 231–262. [Google Scholar] [CrossRef]
- Oh, J.Y.; Kim, M.K.; Shin, M.S.; Wee, W.R.; Lee, J.H. Cytokine secretion by human mesenchymal stem cells cocultured with damaged corneal epithelial cells. Cytokine 2009, 46, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Hu, N.; Zhang, Y.Y.; Gu, H.W.; Guan, H.J. Effects of bone marrow mesenchymal stem cells on cell proliferation and growth factor expression of limbal epithelial cells in vitro. Ophthalmic Res. 2012, 48, 82–88. [Google Scholar] [CrossRef]
- Tang, Q.; Luo, C.; Lu, B.; Fu, Q.; Yin, H.; Qin, Z.; Lyu, D.; Zhang, L.; Fang, Z.; Zhu, Y.; et al. Thermosensitive chitosan-based hydrogels releasing stromal cell derived factor-1 alpha recruit MSC for corneal epithelium regeneration. Acta Biomater. 2017, 61, 101–113. [Google Scholar] [CrossRef]
- Mittal, S.K.; Omoto, M.; Amouzegar, A.; Sahu, A.; Rezazadeh, A.; Katikireddy, K.R.; Shah, D.I.; Sahu, S.K.; Chauhan, S.K. Restoration of Corneal Transparency by Mesenchymal Stem Cells. Stem Cell Rep. 2016, 7, 582–590. [Google Scholar] [CrossRef] [Green Version]
- Roddy, G.W.; Oh, J.Y.; Lee, R.H.; Bartosh, T.J.; Ylostalo, J.; Coble, K.; Rosa, R.H.; Prockop, D.J. Action at a distance: Systemically administered adult stem/progenitor cells (MSCs) reduce inflammatory damage to the cornea without engraftment and primarily by secretion of TNF-α stimulated gene/protein 6. Stem Cells 2011, 29, 1572–1579. [Google Scholar] [CrossRef]
- Cejka, C.; Holan, V.; Trosan, P.; Zajicova, A.; Javorkova, E.; Cejkova, J. The Favorable Effect of Mesenchymal Stem Cell Treatment on the Antioxidant Protective Mechanism in the Corneal Epithelium and Renewal of Corneal Optical Properties Changed after Alkali Burns. Oxid. Med. Cell. Longev. 2016, 2016, 5843809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, S.K.; Foulsham, W.; Shukla, S.; Elbasiony, E.; Omoto, M.; Chauhan, S.K. Mesenchymal Stromal Cells Modulate Corneal Alloimmunity via Secretion of Hepatocyte Growth Factor. Stem Cells Transl. Med. 2019, 8, 1030–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djouad, F.; Charbonnier, L.-M.; Bouffi, C.; Louis-Plence, P.; Bony, C.; Apparailly, F.; Cantos, C.; Jorgensen, C.; Noël, D. Mesenchymal Stem Cells Inhibit the Differentiation of Dendritic Cells through an Interleukin-6-Dependent Mechanism. Stem Cells 2007, 25, 2025–2032. [Google Scholar] [CrossRef] [PubMed]
- Ren, G.; Zhang, L.; Zhao, X.; Xu, G.; Zhang, Y.; Roberts, A.I.; Zhao, R.C.; Shi, Y. Mesenchymal Stem Cell-Mediated Immunosuppression Occurs via Concerted Action of Chemokines and Nitric Oxide. Cell Stem Cell 2008, 2, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, S.; Pittenger, M.F. Human mesenchymal stem cells modulate allogeneic immune cell responses. Blood 2005, 105, 1815–1822. [Google Scholar] [CrossRef] [Green Version]
- Rohaina, C.M.; Then, K.Y.; Ng, A.M.; Wan Abdul Halim, W.H.; Zahidin, A.Z.; Saim, A.; Idrus, R.B. Reconstruction of limbal stem cell deficient corneal surface with induced human bone marrow mesenchymal stem cells on amniotic membrane. Transl. Res. 2014, 163, 200–210. [Google Scholar] [CrossRef]
- Venugopal, B.; Shenoy, S.J.; Mohan, S.; Anil Kumar, P.R.; Kumary, T.V. Bioengineered corneal epithelial cell sheet from mesenchymal stem cells—A functional alternative to limbal stem cells for ocular surface reconstruction. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 1033–1045. [Google Scholar] [CrossRef]
- Ma, Y.; Xu, Y.; Xiao, Z.; Yang, W.; Zhang, C.; Song, E.; Du, Y.; Li, L. Reconstruction of Chemically Burned Rat Corneal Surface by Bone Marrow-Derived Human Mesenchymal Stem Cells. Stem Cells 2006, 24, 315–321. [Google Scholar] [CrossRef]
- Ye, J.; Yao, K.; Kim, J.C. Mesenchymal stem cell transplantation in a rabbit corneal alkali burn model: Engraftment and involvement in wound healing. Eye 2006, 20, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.K.; Soliman, A.A.; Omar, S.M.; Mohammed, W.R. Bone marrow mesenchymal stem cell transplantation in a rabbit corneal alkali burn model (a histological and immune histo-chemical study). Int. J. Stem Cells 2015, 8, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Reinshagen, H.; Auw-Haedrich, C.; Sorg, R.V.; Boehringer, D.; Eberwein, P.; Schwartzkopff, J.; Sundmacher, R.; Reinhard, T. Corneal surface reconstruction using adult mesenchymal stem cells in experimental limbal stem cell deficiency in rabbits. Acta Ophthalmol. 2011, 89, 741–748. [Google Scholar] [CrossRef]
- Espandar, L.; Caldwell, D.; Watson, R.; Blanco-Mezquita, T.; Zhang, S.; Bunnell, B. Application of adipose-derived stem cells on scleral contact lens carrier in an animal model of severe acute alkaline burn. Eye Contact Lens 2014, 40, 243–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galindo, S.; Herreras, J.M.; López-Paniagua, M.; Rey, E.; de la Mata, A.; Plata-Cordero, M.; Calonge, M.; Nieto-Miguel, T. Therapeutic Effect of Human Adipose Tissue-Derived Mesenchymal Stem Cells in Experimental Corneal Failure Due to Limbal Stem Cell Niche Damage. Stem Cells 2017, 35, 2160–2174. [Google Scholar] [CrossRef] [Green Version]
- Zeppieri, M.; Salvetat, M.L.; Beltrami, A.P.; Cesselli, D.; Bergamin, N.; Russo, R.; Cavaliere, F.; Varano, G.P.; Alcalde, I.; Merayo, J.; et al. Human adipose-derived stem cells for the treatment of chemically burned rat cornea: Preliminary Results. Curr. Eye Res. 2013, 38, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Ghazaryan, E.; Zhang, Y.; He, Y.; Liu, X.; Li, Y.; Xie, J.; Su, G. Mesenchymal stem cells in corneal neovascularization: Comparison of different application routes. Mol. Med. Rep. 2016, 14, 3104–3112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zajicova, A.; Pokorna, K.; Lencova, A.; Krulova, M.; Svobodova, E.; Kubinova, S.; Sykova, E.; Pradny, M.; Michalek, J.; Svobodova, J.; et al. Treatment of ocular surface injuries by limbal and mesenchymal stem cells growing on nanofiber scaffolds. Cell Transplant. 2010, 19, 1281–1290. [Google Scholar] [CrossRef] [PubMed]
- Rengasamy, M.; Gupta, P.K.; Kolkundkar, U.; Singh, G.; Balasubramanian, S.; SundarRaj, S.; Chullikana, A.; Majumdar, A. Sen Preclinical safety & toxicity evaluation of pooled, allogeneic human bone marrow-derived mesenchymal stromal cells. Indian J. Med. Res. 2016, 144, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Guess, A.J.; Daneault, B.; Wang, R.; Bradbury, H.; La Perle, K.M.; Fitch, J.; Hedrick, S.L.; Hamelberg, E.; Astbury, C.; White, P.; et al. Safety Profile of Good Manufacturing Practice Manufactured Interferon γ-Primed Mesenchymal Stem/Stromal Cells for Clinical Trials. Stem Cells Transl. Med. 2017, 6, 1868–1879. [Google Scholar] [CrossRef] [PubMed]
- Gramlich, O.W.; Burand, A.J.; Brown, A.J.; Deutsch, R.J.; Kuehn, M.H.; Ankrum, J.A. Cryopreserved mesenchymal stromal cells maintain potency in a retinal ischemia/reperfusion injury model: Toward an off-the-shelf therapy. Sci. Rep. 2016, 6, 26463. [Google Scholar] [CrossRef]
- Tappenbeck, N.; Schröder, H.M.; Niebergall-Roth, E.; Hassinger, F.; Dehio, U.; Dieter, K.; Kraft, K.; Kerstan, A.; Esterlechner, J.; Frank, N.Y.; et al. In vivo safety profile and biodistribution of GMP-manufactured human skin-derived ABCB5-positive mesenchymal stromal cells for use in clinical trials. Cytotherapy 2019, 21, 546–560. [Google Scholar] [CrossRef] [PubMed]
- Labrador Velandia, S.; Di Lauro, S.; Alonso-Alonso, M.L.; Tabera Bartolomé, S.; Srivastava, G.K.; Pastor, J.C.; Fernandez-Bueno, I. Biocompatibility of intravitreal injection of human mesenchymal stem cells in immunocompetent rabbits. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 125–134. [Google Scholar] [CrossRef]
- Cotsarelis, G.; Cheng, S.Z.; Dong, G.; Sun, T.T.; Lavker, R.M. Existence of slow-cycling limbal epithelial basal cells that can be preferentially stimulated to proliferate: Implications on epithelial stem cells. Cell 1989, 57, 201–209. [Google Scholar] [CrossRef]
- Luetzkendorf, J.; Nerger, K.; Hering, J.; Moegel, A.; Hoffmann, K.; Hoefers, C.; Mueller-Tidow, C.; Mueller, L.P. Cryopreservation does not alter main characteristics of Good Manufacturing Process-grade human multipotent mesenchymal stromal cells including immunomodulating potential and lack of malignant transformation. Cytotherapy 2015, 17, 186–198. [Google Scholar] [CrossRef]
- Calonge, M.; Pérez, I.; Galindo, S.; Nieto-Miguel, T.; López-Paniagua, M.; Fernández, I.; Alberca, M.; García-Sancho, J.; Sánchez, A.; Herreras, J.M. A proof-of-concept clinical trial using mesenchymal stem cells for the treatment of corneal epithelial stem cell deficiency. Transl. Res. 2019, 206, 18–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimazaki, J.; Higa, K.; Morito, F.; Dogru, M.; Kawakita, T.; Satake, Y.; Shimmura, S.; Tsubota, K. Factors Influencing Outcomes in Cultivated Limbal Epithelial Transplantation for Chronic Cicatricial Ocular Surface Disorders. Am. J. Ophthalmol. 2007, 143, 945–953. [Google Scholar] [CrossRef] [Green Version]
- Shortt, A.J.; Secker, G.A.; Rajan, M.S.; Meligonis, G.; Dart, J.K.; Tuft, S.J.; Daniels, J.T. Ex Vivo Expansion and Transplantation of Limbal Epithelial Stem Cells. Ophthalmology 2008, 115, 1989–1997. [Google Scholar] [CrossRef] [PubMed]
- Pauklin, M.; Fuchsluger, T.A.; Westekemper, H.; Steuhl, K.P.; Meller, D. Midterm results of cultivated autologous and allogeneic limbal epithelial transplantation in limbal stem cell deficiency. Dev. Ophthalmol. 2010, 45, 57–70. [Google Scholar] [CrossRef]
- Prabhasawat, P.; Ekpo, P.; Uiprasertkul, M.; Chotikavanich, S.; Tesavibul, N. Efficacy of cultivated corneal epithelial stem cells for ocular surface reconstruction. Clin. Ophthalmol. 2012, 6, 1483–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakaria, N.; Possemiers, T.; Dhubhghaill, S.N.; Leysen, I.; Rozema, J.; Koppen, C.; Timmermans, J.P.; Berneman, Z.; Tassignon, M.J. Results of a phase I/II clinical trial: Standardized, non-xenogenic, cultivated limbal stem cell transplantation. J. Transl. Med. 2014, 12, 58. [Google Scholar] [CrossRef] [Green Version]
- Ganger, A.; Vanathi, M.; Mohanty, S.; Tandon, R. Long-term outcomes of cultivated limbal epithelial transplantation: Evaluation and comparison of results in children and adults. Biomed Res. Int. 2015, 2015, 480983. [Google Scholar] [CrossRef] [Green Version]
- Parihar, J.K.; Parihar, A.S.; Jain, V.K.; Kaushik, J.; Nath, P. Allogenic cultivated limbal stem cell transplantation versus cadaveric keratolimbal allograft in ocular surface disorder: 1-Year outcome. Int. Ophthalmol. 2017, 37, 1323–1331. [Google Scholar] [CrossRef]
- Sharma, N.; Mohanty, S.; Jhanji, V.; Vajpayee, R.B. Amniotic membrane transplantation with or without autologous cultivated limbal stem cell transplantation for the management of partial limbal stem cell deficiency. Clin. Ophthalmol. 2018, 12, 2103–2106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, J.D.; Ahmad, S.; Agrawal, A.; Bienek, C.; Atkinson, A.; Mcgowan, N.W.; Kaye, S.; Mantry, S.; Ramaesh, K.; Glover, A.; et al. Allogeneic Ex Vivo Expanded Corneal Epithelial Stem Cell Transplantation: A Randomized Controlled Clinical Trial. Stem Cells Transl. Med. 2019, 8, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Behaegel, J.; Zakaria, N.; Tassignon, M.J.; Leysen, I.; Bock, F.; Koppen, C.; Ní Dhubhghaill, S. Short- and Long-Term Results of Xenogeneic-Free Cultivated Autologous and Allogeneic Limbal Epithelial Stem Cell Transplantations. Cornea 2019, 38, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J.; Satake, Y.; Higa, K.; Yamaguchi, T.; Noma, H.; Tsubota, K. Long-term outcomes of cultivated cell sheet transplantation for treating total limbal stem cell deficiency: Long-term outcomes of cultivated cell sheet transplantation. Ocul. Surf. 2020, 18, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Directive 2001/83/EC of The European Parliament and of the Council of 6 November 2001 on the Community Code Relating to Medicinal Products for Human Use. Available online: https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-1/dir_2001_83_consol_2012/dir_2001_83_cons_2012_en.pdf (accessed on 29 July 2021).
- Arda, B.; Aciduman, A. An evaluation regarding the current situation of stem cell studies in Turkey. Stem Cell Rev. Rep. 2009, 5, 130–134. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Cellular & Gene Therapy Products. Available online: https://www.fda.gov/vaccinesblood-biologics/cellular-gene-therapy-products (accessed on 29 July 2021).
- Jokura, Y.; Yano, K.; Yamato, M. Comparison of the new Japanese legislation for expedited approval of regenerative medicine products with the existing systems in the USA and European Union. J. Tissue Eng. Regen. Med. 2018, 12, e1056–e1062. [Google Scholar] [CrossRef] [Green Version]
- Okada, K.; Koike, K.; Sawa, Y. Consideration of and expectations for the Pharmaceuticals, Medical Devices and Other Therapeutic Products Act in Japan. Regen. Ther. 2015, 1, 80–83. [Google Scholar] [CrossRef] [Green Version]
- Lahiry, S.; Choudhury, S.; Sinha, R.; Chatterjee, S. The national guidelines for stem cell research (2017): What academicians need to know? Perspect. Clin. Res. 2019, 10, 148–154. [Google Scholar] [CrossRef]
- Indian Council of Medical Research & Departmenf of Biotechnology. National Guidelines for Stem Cell Research. 2017. Available online: https://dbtindia.gov.in/sites/default/files/National_Guidelines_StemCellResearch-2017.pdf (accessed on 29 July 2021).
- Therapeutic Goods Order No. 88—Standards for Donor Selection, Testing, and Minimising Infectious Disease Transmission Via Therapeutic Goods That Are Human Blood and Blood Components, Human Tissues and Human Cellular Therapy Products. Australian Government. Available online: https://www.legislation.gov.au/Details/F2013L00854 (accessed on 29 July 2021).
- Australian Code of Good Manufacturing Practice for Human Blood and Blood Components, Human Tissues and Human Cellular Therapy Products. Australian Department of Health & Aging Therapeutic Goods Administration; Version 1.0. Available online: https://www.tga.gov.au/si (accessed on 29 July 2013).
- Jawaheer, L.; Anijeet, D.; Ramaesh, K. Diagnostic criteria for limbal stem cell deficiency—A systematic literature review. Surv. Ophthalmol. 2017, 62, 522–532. [Google Scholar] [CrossRef]
- Banayan, N.; Georgeon, C.; Grieve, K.; Borderie, V.M. Spectral-domain Optical Coherence Tomography in Limbal Stem Cell Deficiency. A Case-Control Study. Am. J. Ophthalmol. 2018, 190, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, N.; Dhubhghaill, S.N.; Taal, M.; Berneman, Z.; Koppen, C.; Tassignon, M.J. Optical coherence tomography in cultivated Limbal epithelial stem cell transplantation surgery. Asia-Pac. J. Ophthalmol. 2015, 4, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Liang, Q.; Le, Q.; Cordova, D.W.; Tseng, C.H.; Deng, S.X. Corneal Epithelial Thickness Measured Using Anterior Segment Optical Coherence Tomography as a Diagnostic Parameter for Limbal Stem Cell Deficiency. Am. J. Ophthalmol. 2020, 216, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.P.; Mysore, N. Corneal neovascularization. Exp. Eye Res. 2021, 202, 108363. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Jacobs, D.S. Long-term outcome of using Prosthetic Replacement of Ocular Surface Ecosystem (PROSE) as a drug delivery system for bevacizumab in the treatment of corneal neovascularization. Ocul. Surf. 2019, 17, 134–141. [Google Scholar] [CrossRef]
- Stern, J.H.; Tian, Y.; Funderburgh, J.; Pellegrini, G.; Zhang, K.; Goldberg, J.L.; Ali, R.R.; Young, M.; Xie, Y.; Temple, S. Regenerating Eye Tissues to Preserve and Restore Vision. Cell Stem Cell. 2018, 22, 834–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangwan, V.S.; Vemuganti, G.K.; Singh, S.; Balasubramanian, D. Successful Reconstruction of Damaged Ocular Outer Surface in Humans using Limbal and Conjuctival Stem Cell Culture Methods. Biosci. Rep. 2003, 23, 169–174. [Google Scholar] [CrossRef]
- Tsubota, K.; Satake, Y.; Kaido, M.; Shinozaki, N.; Shimmura, S.; Bissen-Miyajima, H.; Shimazaki, J. Treatment of Severe Ocular-Surface Disorders with Corneal Epithelial Stem-Cell Transplantation. N. Engl. J. Med. 1999, 340, 1697–1703. [Google Scholar] [CrossRef] [PubMed]
- Kolli, S.A.; Ahmad, S.; Lako, M.; Figueiredo, F. Successful clinical implementation of corneal epithelial stem cell therapy for treatment of unilateral limbal stem cell deficiency. Stem Cells 2010, 28, 597–610. [Google Scholar] [CrossRef]
- Le, Q.H.; Wang, W.T.; Hong, J.X.; Sun, X.H.; Zheng, T.Y.; Zhu, W.Q.; Xu, J.J. An in vivo confocal microscopy and impression cytology analysis of goblet cells in patients with chemical burns. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1397–1400. [Google Scholar] [CrossRef]
- Lagali, N.; Edén, U.; Utheim, T.P.; Chen, X.; Riise, R.; Dellby, A.; Fagerholm, P. In vivo morphology of the limbal palisades of vogt correlates with progressive stem cell deficiency in aniridia-related keratopathy. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5333–5342. [Google Scholar] [CrossRef] [Green Version]
- Ramírez, B.E.; Victoria, D.A.; Murillo, G.M.; Herreras, J.M.; Calonge, M. In vivo confocal microscopy assessment of the corneoscleral limbal stem cell niche before and after biopsy for cultivated limbal epithelial transplantation to restore corneal epithelium. Histol. Histopathol. 2015, 30, 183–192. [Google Scholar] [CrossRef]
- Mastropasqua, L.; Calienno, R.; Lanzini, M.; Nubile, M.; Colabelli-Gisoldi, R.A.; De Carlo, L.; Pocobelli, A. In vivo confocal microscopy of the sclerocorneal limbus after limbal stem cell transplantation: Looking for limbal architecture modifications and cytological phenotype correlations. Mol. Vis. 2016, 22, 748–760. [Google Scholar] [PubMed]
- Pellegrini, G.; Rama, P.; Matuska, S.; Lambiase, A.; Bonini, S.; Pocobelli, A.; Colabelli, R.G.; Spadea, L.; Fasciani, R.; Balestrazzi, E.; et al. Biological parameters determining the clinical outcome of autologous cultures of limbal stem cells. Regen. Med. 2013, 8, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Fasolo, A.; Pedrotti, E.; Passilongo, M.; Marchini, G.; Monterosso, C.; Zampini, R.; Bohm, E.; Birattari, F.; Franch, A.; Barbaro, V.; et al. Safety outcomes and long-Term effectiveness of ex vivo autologous cultured limbal epithelial transplantation for limbal stem cell deficiency. Br. J. Ophthalmol. 2017, 101, 640–649. [Google Scholar] [CrossRef]
- Parthasarathy, M.; Sasikala, R.; Gunasekaran, P.; Raja, J. Antimicrobial Activity of Human Amniotic and Chorionic Membranes. J. Acad. Ind. Res. 2014, 2, 545–547. [Google Scholar]
- Niknejad, H.; Peirovi, H.; Jorjani, M.; Ahmadiani, A.; Ghanavi, J.; Seifalian, A.M. Properties of the amniotic membrane for potential use in tissue engineering. Eur. Cells Mater. 2008, 15, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Sudha, B.; Sitalakshmi, G.; Iyer, G.K.; Krishnakumar, S. Putative stem cell markers in limal epithelial cells cultured on intact & denuded human amniotic membrane. Indian J. Med. Res. 2008, 128, 149–156. [Google Scholar] [PubMed]
- Schwab, I.R.; Reyes, M.; Isseroff, R.R. Successful transplantation of bioengineered tissue replacements in patients with ocular surface disease. Cornea 2000, 19, 421–426. [Google Scholar] [CrossRef]
- Koizumi, N.; Inatomi, T.; Quantock, A.J.; Fullwood, N.J.; Dota, A.; Kinoshita, S. Amniotic membrane as a substrate for cultivating limbal corneal epithelial cells for autologous transplantation in rabbits. Cornea 2000, 19, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Meller, D.; Pires, R.T.; Tseng, S.C. Ex vivo preservation and expansion of human limbal epithelial stem cells on amniotic membrane cultures. Br. J. Ophthalmol. 2002, 86, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Grueterich, M.; Espana, E.M.; Touhami, A.; Ti, S.E.; Tseng, S.C. Phenotypic study of a case with successful transplantation of ex vivo expanded human limbal epithelium for unilateral total limbal stem cell deficiency. Ophthalmology 2002, 109, 1547–1552. [Google Scholar] [CrossRef]
- Gomes, J.A.; Dos Santos, M.S.; Cunha, M.C.; Mascaro, V.L.; De Nadai Barros, J.N.; De Sousa, L.B. Amniotic membrane transplantation for partial and total limbal stem cell deficiency secondary to chemical burn. Ophthalmology 2003, 10, 466–473. [Google Scholar] [CrossRef]
- Kim, J.C.; Tseng, S.C. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas. Cornea 1995, 14, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J.; Yang, H.Y.; Tsubota, K. Amniotic membrane transplantation for ocular surface reconstruction in patients with chemical and thermal burns. Ophthalmology 1997, 104, 2068–2076. [Google Scholar] [CrossRef]
- Atrah, H.I. Fibrin glue. BMJ 1994, 308, 933–934. [Google Scholar] [CrossRef]
- Lagoutte, F.M.; Gauthier, L.; Comte, P.R. A fibrin sealant for perforated and preperforated corneal ulcers. Br. J. Ophthalmol. 1989, 73, 757–761. [Google Scholar] [CrossRef]
- Kopp, J.; Jeschke, M.G.; Bach, A.D.; Kneser, U.; Horch, R.E. Applied tissue engineering in the closure of severe burns and chronic wounds using cultured human autologous keratinocytes in a natural fibrin matrix. Cell Tissue Bank. 2004, 5, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Talbot, M.; Carrier, P.; Giasson, C.J.; Deschambeault, A.; Guérin, S.L.; Auger, F.A.; Bazin, R.; Germain, L. Autologous transplantation of rabbit limbal epithelia cultured on fibrin gels for ocular surface reconstruction. Mol. Vis. 2006, 12, 65–75. [Google Scholar]
- Rama, P.; Bonini, S.; Lambiase, A.; Golisano, O.; Paterna, P.; De Luca, M.; Pellegrini, G. Autologous fibrin-cultured limbal stem cells permanently restore the corneal surface of patients with total limbal stem cell deficiency. Transplantation 2001, 72, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, E.; Ferrari, S.; Fasolo, A.; Böhm, E.; Ponzin, D.; Barbaro, V. Techniques for culture and assessment of limbal stem cell grafts. Ocul. Surf. 2010, 8, 146–153. [Google Scholar] [CrossRef]
- Di Girolamo, N.; Chui, J.; Wakefield, D.; Coroneo, M.T. Cultured human ocular surface epithelium on therapeutic contact lenses. Br. J. Ophthalmol. 2007, 91, 459–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Mata, A.; Mateos-Timoneda, M.A.; Nieto-Miguel, T.; Galindo, S.; López-Paniagua, M.; Planell, J.A.; Engel, E.; Calonge, M. Poly-L/DL-lactic acid films functionalized with collagen IV as carrier substrata for corneal epithelial stem cells. Colloids Surf. B Biointerfaces 2019, 177, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Geggel, H.S.; Friend, J.; Thoft, R.A. Collagen gel for ocular surface. Investig. Ophthalmol. Vis. Sci. 1985, 26, 901–905. [Google Scholar]
- Haagdorens, M.; Cėpla, V.; Melsbach, E.; Koivusalo, L.; Skottman, H.; Griffith, M.; Valiokas, R.; Zakaria, N.; Pintelon, I.; Tassignon, M.J. In vitro cultivation of limbal epithelial stem cells on surface-modified crosslinked collagen scaffolds. Stem Cells Int. 2019, 2019, 7867613. [Google Scholar] [CrossRef] [Green Version]
- Chae, J.J.; McIntosh Ambrose, W.; Espinoza, F.A.; Mulreany, D.G.; Ng, S.; Takezawa, T.; Trexler, M.M.; Schein, O.D.; Chuck, R.S.; Elisseeff, J.H. Regeneration of corneal epithelium utilizing a collagen vitrigel membrane in rabbit models for corneal stromal wound and limbal stem cell deficiency. Acta Ophthalmol. 2015, 93, 57–66. [Google Scholar] [CrossRef]
- Levis, H.; Daniels, J.T. New technologies in limbal epithelial stem cell transplantation. Curr. Opin. Biotechnol. 2009, 20, 593–597. [Google Scholar] [CrossRef]
- Mi, S.; Chen, B.; Wright, B.; Connon, C.J. Plastic compression of a collagen gel forms a much improved scaffold for ocular surface tissue engineering over conventional collagen gels. J. Biomed. Mater. Res. Part A 2010, 95, 447–453. [Google Scholar] [CrossRef]
- Levis, H.J.; Brown, R.A.; Daniels, J.T. Plastic compressed collagen as a biomimetic substrate for human limbal epithelial cell culture. Biomaterials 2010, 31, 7726–7737. [Google Scholar] [CrossRef]
- Mi, S.; Chen, B.; Wright, B.; Connon, C.J. Ex vivo construction of an artificial ocular surface by combination of corneal limbal epithelial cells and a compressed collagen scaffold containing keratocytes. Tissue Eng. Part A 2010, 95, 447–453. [Google Scholar] [CrossRef]
- De La Mata, A.; Nieto-Miguel, T.; López-Paniagua, M.; Galindo, S.; Aguilar, M.R.; García-Fernández, L.; Gonzalo, S.; Vázquez, B.; Román, J.S.; Corrales, R.M.; et al. Chitosan-gelatin biopolymers as carrier substrata for limbal epithelial stem cells. J. Mater. Sci. Mater. Med. 2013, 24, 2819–2829. [Google Scholar] [CrossRef]
- Grolik, M.; Szczubiałka, K.; Wowra, B.; Dobrowolski, D.; Orzechowska-Wylęgała, B.; Wylęgała, E.; Nowakowska, M. Hydrogel membranes based on genipin-cross-linked chitosan blends for corneal epithelium tissue engineering. J. Mater. Sci. Mater. Med. 2012, 23, 1991–2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, X.; Beuerman, R.W.; Chan-Park, M.B.; Cheng, Z.; Ang, L.P.; Tan, D.T. Enhancement of the mechanical and biological properties of a biomembrane for tissue engineering the ocular surface. Ann. Acad. Med. Singap. 2006, 35, 210–214. [Google Scholar]
- Bray, L.J.; George, K.A.; Ainscough, S.L.; Hutmacher, D.W.; Chirila, T.V.; Harkin, D.G. Human corneal epithelial equivalents constructed on Bombyx mori silk fibroin membranes. Biomaterials 2011, 32, 5086–5091. [Google Scholar] [CrossRef]
- Li, Y.; Yang, Y.; Yang, L.; Zeng, Y.; Gao, X.; Xu, H. Poly(ethylene glycol)-modified silk fibroin membrane as a carrier for limbal epithelial stem cell transplantation in a rabbit LSCD model. Stem Cell Res. Ther. 2017, 8, 256. [Google Scholar] [CrossRef] [PubMed]
- Nishida, K.; Yamato, M.; Hayashida, Y.; Watanabe, K.; Maeda, N.; Watanabe, H.; Yamamoto, K.; Nagai, S.; Kikuchi, A.; Tano, Y.; et al. Functional bioengineered corneal epithellial sheet grafts from corneal stem cells expanded ex vivo on a temperature-responsive cell culture surface. Transplantation 2004, 77, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, G.; Haq, Z.; Kang, K.; Jabbehdari, S.; Rosenblatt, M.L.; Djalilian, A.R. Strategies for reconstructing the limbal stem cell niche. Ocul. Surf. 2019, 17, 230–240. [Google Scholar] [CrossRef]
- Oh, J.Y.; Kim, M.K.; Shin, M.S.; Lee, H.J.; Ko, J.H.; Wee, W.R.; Lee, J.H. The Anti-Inflammatory and Anti-Angiogenic Role of Mesenchymal Stem Cells in Corneal Wound Healing Following Chemical Injury. Stem Cells 2008, 26, 1047–1055. [Google Scholar] [CrossRef]
- Galindo, S.; de la Mata, A.; López-Paniagua, M.; Herreras, J.M.; Pérez, I.; Calonge, M.; Nieto-Miguel, T. Subconjunctival injection of mesenchymal stem cells for corneal failure due to limbal stem cell deficiency: State of the art. Stem Cell Res. Ther. 2021, 12, 60. [Google Scholar] [CrossRef]
- Di, G.; Du, X.; Qi, X.; Zhao, X.; Duan, H.; Li, S.; Xie, L.; Zhou, Q. Mesenchymal stem cells promote diabetic corneal epithelial wound healing through TSG-6-dependent stem cell activation and macrophage switch. Investig. Ophthalmol. Vis. Sci. 2017, 58, 4344–4354. [Google Scholar] [CrossRef]
- Zhang, N.; Luo, X.; Zhang, S.; Liu, R.; Liang, L.; Su, W.; Liang, D. Subconjunctival injection of tumor necrosis factor-α pre-stimulated bone marrow-derived mesenchymal stem cells enhances anti-inflammation and anti-fibrosis in ocular alkali burns. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 929–940. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhang, Y.; Cai, S.; Sun, M.; Wang, J.; Li, S.; Li, X.; Tighe, S.; Chen, S.; Xie, H.; et al. Human limbal niche cells are a powerful regenerative source for the prevention of limbal stem cell deficiency in a rabbit model. Sci. Rep. 2018, 8, 6566. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Wang, X.; Li, D.; Li, J.; Jiang, Z. MSCs inhibits the angiogenesis of HUVECs through the miR-211/Prox1 pathway. J. Biochem. 2019, 166, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Mittal, S.K.; Foulsham, W.; Elbasiony, E.; Singhania, D.; Sahu, S.K.; Chauhan, S.K. Therapeutic efficacy of different routes of mesenchymal stem cell administration in corneal injury. Ocul. Surf. 2019, 17, 729–736. [Google Scholar] [CrossRef]
- Xiao, Y.T.; Xie, H.T.; Liu, X.; Duan, C.Y.; Qu, J.Y.; Zhang, M.C.; Zhao, X.Y. Subconjunctival Injection of Transdifferentiated Oral Mucosal Epithelial Cells for Limbal Stem Cell Deficiency in Rats. J. Histochem. Cytochem. 2021, 69, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Sohni, A.; Verfaillie, C.M. Mesenchymal stem cells migration homing and tracking. Stem Cells Int. 2013, 2013, 130763. [Google Scholar] [CrossRef]
- Mäkelä, T.; Takalo, R.; Arvola, O.; Haapanen, H.; Yannopoulos, F.; Blanco, R.; Ahvenjärvi, L.; Kiviluoma, K.; Kerkelä, E.; Nystedt, J.; et al. Safety and biodistribution study of bone marrow-derived mesenchymal stromal cells and mononuclear cells and the impact of the administration route in an intact porcine model. Cytotherapy 2015, 17, 392–402. [Google Scholar] [CrossRef]
- Lee, R.H.; Yu, J.M.; Foskett, A.M.; Peltier, G.; Reneau, J.C.; Bazhanov, N.; Oh, J.Y.; Prockop, D.J. TSG-6 as a biomarker to predict efficacy of human mesenchymal stem/progenitor cells (hMSCs) in modulating sterile inflammation in vivo. Proc. Natl. Acad. Sci. USA 2014, 111, 16766–16771. [Google Scholar] [CrossRef] [Green Version]
- Yun, Y.I.; Park, S.Y.; Lee, H.J.; Ko, J.H.; Kim, M.K.; Wee, W.R.; Reger, R.L.; Gregory, C.A.; Choi, H.; Fulcher, S.F.; et al. Comparison of the anti-inflammatory effects of induced pluripotent stem cell–derived and bone marrow–derived mesenchymal stromal cells in a murine model of corneal injury. Cytotherapy 2017, 19, 28–35. [Google Scholar] [CrossRef]
- Haagdorens, M.; Van Acker, S.I.; Van Gerwen, V.; Ní Dhubhghaill, S.; Koppen, C.; Tassignon, M.J.; Zakaria, N. Limbal stem cell deficiency: Current treatment options and emerging therapies. Stem Cells Int. 2016, 2016, 9798374. [Google Scholar] [CrossRef] [Green Version]
- Lachaud, C.C.; Hmadcha, A.; Soria, B. Corneal Regeneration: Use of Extracorneal Stem Cells. In Corneal Regeneration Therapy and Surgery; Alió, J., Alió del Barrio, J.L., Arnalich-Montiel, F., Eds.; Springer Nature: Basingstoke, UK, 2019; pp. 123–144. [Google Scholar] [CrossRef]
- Nosrati, H.; Alizadeh, Z.; Nosrati, A.; Ashrafi-Dehkordi, K.; Banitalebi-Dehkordi, M.; Sanami, S.; Khodaei, M. Stem cell-based therapeutic strategies for corneal epithelium regeneration. Tissue Cell 2021, 68, 101470. [Google Scholar] [CrossRef] [PubMed]
- Thomson, J.A. Embryonic stem cell lines derived from human blastocysts. Science 1998, 282, 1145–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanson, C.; Hardarson, T.; Ellerström, C.; Nordberg, M.; Caisander, G.; Rao, M.; Hyllner, J.; Stenevi, U. Transplantation of human embryonic stem cells onto a partially wounded human cornea in vitro. Acta Ophthalmol. 2013, 91, 127–130. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Zhang, K.; Sun, Y.; Gao, X.; Li, Y.; Chen, Z.; Wu, X. Reconstruction of functional ocular surface by acellular porcine cornea matrix scaffold and limbal stem cells derived from human embryonic stem cells. Tissue Eng. Part A 2013, 19, 2412–2425. [Google Scholar] [CrossRef]
- Da Mata Martins, T.M.; da Silva Cunha, P.; Rodrigues, M.A.; de Carvalho, J.L.; de Souza, J.E.; de Carvalho Oliveira, J.A.; Gomes, D.A.; de Goes, A.M. Epithelial basement membrane of human decellularized cornea as a suitable substrate for differentiation of embryonic stem cells into corneal epithelial-like cells. Mater. Sci. Eng. C 2020, 116, 111215. [Google Scholar] [CrossRef]
- Ahmad, S.; Stewart, R.; Yung, S.; Kolli, S.; Armstrong, L.; Stojkovic, M.; Figueiredo, F.; Lako, M. Differentiation of Human Embryonic Stem Cells into Corneal Epithelial-Like Cells by In Vitro Replication of the Corneal Epithelial Stem Cell Niche. Stem Cells 2007, 25, 1145–1155. [Google Scholar] [CrossRef]
- Zhang, C.; Du, L.; Pang, K.; Wu, X. Differentiation of human embryonic stem cells into corneal epithelial progenitor cells under defined conditions. PLoS ONE 2017, 12, e0183303. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Du, L.; Sun, P.; Shen, L.; Zhu, J.; Pang, K.; Wu, X. Construction of tissue-engineered full-thickness cornea substitute using limbal epithelial cell-like and corneal endothelial cell-like cells derived from human embryonic stem cells. Biomaterials 2017, 124, 180–194. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Ou, S.; Ren, J.; Sun, H.; He, X.; Zhao, Z.; Wu, H.; Qu, Y.; Liu, T.; Jeyalatha, V.; et al. Tissue engineered corneal epithelium derived from clinical-grade human embryonic stem cells. Ocul. Surf. 2020, 18, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Kiskinis, E.; Eggan, K. Progress toward the clinical application of patient-specific pluripotent stem cells. J. Clin. Investig. 2010, 120, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Adult Human Fibroblasts by Defined Factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef] [Green Version]
- Casaroli-Marano, R.P. Cell-based Therapy Using Induced Plutipotent Stem Cell. In Corneal Regeneration Therapy and Surgery; Alió, J., Alió del Barrio, J.L., Arnalich-Montiel, F., Eds.; Springer Nature: Basingstoke, UK, 2019; pp. 263–273. [Google Scholar] [CrossRef]
- Chakrabarty, K.; Shetty, R.; Ghosh, A. Corneal cell therapy: With iPSCs, it is no more a far-sight. Stem Cell Res. Ther. 2018, 9, 287. [Google Scholar] [CrossRef] [Green Version]
- Theerakittayakorn, K.; Nguyen, H.T.; Musika, J.; Kunkanjanawan, H.; Imsoonthornruksa, S.; Somredngan, S.; Ketudat-Cairns, M.; Parnpai, R. Differentiation induction of human stem cells for corneal epithelial regeneration. Int. J. Mol. Sci. 2020, 21, 7834. [Google Scholar] [CrossRef]
- Hayashi, R.; Ishikawa, Y.; Ito, M.; Kageyama, T.; Takashiba, K.; Fujioka, T.; Tsujikawa, M.; Miyoshi, H.; Yamato, M.; Nakamura, Y.; et al. Generation of Corneal Epithelial Cells from Induced Pluripotent Stem Cells Derived from Human Dermal Fibroblast and Corneal Limbal Epithelium. PLoS ONE 2012, 7, 45435. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, R.; Ishikawa, Y.; Sasamoto, Y.; Katori, R.; Nomura, N.; Ichikawa, T.; Araki, S.; Soma, T.; Kawasaki, S.; Sekiguchi, K.; et al. Co-ordinated ocular development from human iPS cells and recovery of corneal function. Nature 2016, 531, 376–380. [Google Scholar] [CrossRef]
- Hayashi, R.; Ishikawa, Y.; Katori, R.; Sasamoto, Y.; Taniwaki, Y.; Takayanagi, H.; Tsujikawa, M.; Sekiguchi, K.; Quantock, A.J.; Nishida, K. Coordinated generation of multiple ocular-like cell lineages and fabrication of functional corneal epithelial cell sheets from human iPS cells. Nat. Protoc. 2017, 12, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Mikhailova, A.; Ilmarinen, T.; Uusitalo, H.; Skottman, H. Small-molecule induction promotes corneal epithelial cell differentiation from human induced pluripotent stem cells. Stem Cell Rep. 2014, 2, 219–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hongisto, H.; Vattulainen, M.; Ilmarinen, T.; Mikhailova, A.; Skottman, H. Efficient and scalable directed differentiation of clinically compatible corneal limbal epithelial stem cells from human pluripotent stem cells. J. Vis. Exp. 2018, 24, 58279. [Google Scholar] [CrossRef] [Green Version]
- Taylor, C.J.; Peacock, S.; Chaudhry, A.N.; Bradley, J.A.; Bolton, E.M. Generating an iPSC bank for HLA-matched tissue transplantation based on known donor and recipient hla types. Cell Stem Cell 2012, 11, 147–152. [Google Scholar] [CrossRef] [Green Version]
- De Rham, C.; Villard, J. Potential and limitation of HLA-based banking of human pluripotent stem cells for cell therapy. J. Immunol. Res. 2014, 2014, 518135. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, S.; Stacey, G.N.; Akazawa, C.; Aoyama, N.; Baptista, R.; Bedford, P.; Bennaceur Griscelli, A.; Chandra, A.; Elwood, N.; Girard, M.; et al. Quality control guidelines for clinical-grade human induced pluripotent stem cell lines. Regen Med. 2018, 13, 859–866. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Slevin, M.; Guo, B.Q.; Zhu, S.R. Induced pluripotent stem cells as a potential therapeutic source for corneal epithelial stem cells. Int. J. Ophthalmol. 2018, 11, 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Kelaini, S.; Cochrane, A.; Margariti, A. Direct reprogramming of adult cells: Avoiding the pluripotent state. Stem Cells Cloning Adv. Appl. 2014, 7, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Cieślar-Pobuda, A.; Rafat, M.; Knoflach, V.; Skonieczna, M.; Hudecki, A.; Małecki, A.; Urasińska, E.; Ghavami, S.; Łos, M.J. Human induced pluripotent stem cell differentiation and direct transdifferentiation into corneal epithelial-like cells. Oncotarget 2016, 7, 42314–42329. [Google Scholar] [CrossRef]
- Monteiro, B.G.; Serafim, R.C.; Melo, G.B.; Silva, M.C.; Lizier, N.F.; Maranduba, C.M.; Smith, R.L.; Kerkis, A.; Cerruti, H.; Gomes, J.A.; et al. Human immature dental pulp stem cells share key characteristic features with limbal stem cells. Cell Prolif. 2009, 42, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.Á.; Monteiro, B.G.; Melo, G.B.; Smith, R.L.; da Silva, M.C.; Lizier, N.F.; Kerkis, A.; Cerruti, H.; Kerkis, I. Corneal reconstruction with tissue-engineered cell sheets composed of human immature dental pulp stem cells. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1408–1414. [Google Scholar] [CrossRef]
- Tsai, C.L.; Chuang, P.C.; Kuo, H.K.; Chen, Y.H.; Su, W.H.; Wu, P.C. Differentiation of stem cells from human exfoliated deciduous teeth toward a phenotype of corneal epithelium in vitro. Cornea 2015, 34, 1471–1477. [Google Scholar] [CrossRef]
- Patil, S.; D’Souza, C.; Patil, P.; Patil, V.; Prabhu, M.; Bargale, A.; Kaveeshwar, V.; Kumar, S.; Shetty, P. Culture and characterization of human dental pulp-derived stem cells as limbal stem cells for corneal damage repair. Mol. Med. Rep. 2019, 20, 4688–4694. [Google Scholar] [CrossRef]
- Kushnerev, E.; Shawcross, S.G.; Sothirachagan, S.; Carley, F.; Brahma, A.; Yates, J.M.; Hillarby, M.C. Regeneration of corneal epithelium with dental pulp stem cells using a contact lens delivery system. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5192–5199. [Google Scholar] [CrossRef]
- Monteiro, B.G.; Loureiro, R.R.; Cristovam, P.C.; Covre, J.L.; Gomes, J.Á.; Kerkis, I. Amniotic membrane as a biological scaffold for dental pulp stem cell transplantation in ocular surface reconstruction. Arq. Bras. Oftalmol. 2019, 82, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Taylor, G.; Lehrer, M.S.; Jensen, P.J.; Sun, T.T.; Lavker, R.M. Involvement of follicular stem cells in forming not only the follicle but also the epidermis. Cell 2000, 102, 451–461. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Liu, Y.; Yang, Z.; Nguyen, J.; Liang, F.; Morris, R.J.; Cotsarelis, G. Stem cells in the hair follicle bulge contribute to wound repair but not to homeostasis of the epidermis. Nat. Med. 2005, 11, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Blazejewska, E.A.; Schlötzer-Schrehardt, U.; Zenkel, M.; Bachmann, B.; Chankiewitz, E.; Jacobi, C.; Kruse, F.E. Corneal Limbal Microenvironment Can Induce Transdifferentiation of Hair Follicle Stem Cells into Corneal Epithelial-like Cells. Stem Cells 2009, 27, 642–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer-Blazejewska, E.A.; Call, M.K.; Yamanaka, O.; Liu, H.; Schlötzer-Schrehardt, U.; Kruse, F.E.; Kao, W.W. From hair to cornea: Toward the therapeutic use of hair follicle-derived stem cells in the treatment of limbal stem cell deficiency. Stem Cells 2011, 29, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miki, T.; Lehmann, T.; Cai, H.; Stolz, D.B.; Strom, S.C. Stem Cell Characteristics of Amniotic Epithelial Cells. Stem Cells 2005, 23, 1549–1559. [Google Scholar] [CrossRef] [Green Version]
- Miki, T. Stem cell characteristics and the therapeutic potential of amniotic epithelial cells. Am. J. Reprod. Immunol. 2018, 80, 13003. [Google Scholar] [CrossRef] [PubMed]
- He, Y.G.; Alizadeh, H.; Kinoshita, K.; McCulley, J.P. Experimental transplantation of cultured human limbal and amniotic epithelial cells onto the corneal surface. Cornea 1999, 18, 570–579. [Google Scholar] [CrossRef]
- Fatimah, S.S.; Ng, S.L.; Chua, K.H.; Hayati, A.R.; Tan, A.E.; Tan, G.C. Value of human amniotic epithelial cells in tissue engineering for cornea. Hum. Cell 2010, 23, 141–151. [Google Scholar] [CrossRef]
- Yao, M.; Chen, J.; Yang, X.X.; Zhang, X.L.; Ji, Q.S.; Zhou, Q.; Xu, J.T. Differentiation of human amniotic epithelial cells into corneal epithelial-like cells in vitro. Int. J. Ophthalmol. 2013, 6, 564–572. [Google Scholar] [CrossRef]
- Zhou, Q.; Liu, X.Y.; Ruan, Y.X.; Wang, L.; Jiang, M.M.; Wu, J.; Chen, J. Construction of corneal epithelium with human amniotic epithelial cells and repair of limbal deficiency in rabbit models. Hum. Cell 2015, 28, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Ruetze, M.; Gallinat, S.; Lim, I.J.; Chow, E.; Phan, T.T.; Staeb, F.; Wenck, H.; Deppert, W.; Knott, A. Common features of umbilical cord epithelial cells and epidermal keratinocytes. J. Dermatol. Sci. 2008, 50, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Wong, Y.P.; Gu, H.; Cai, Y.J.; Ho, Y.; Wang, C.C.; Leung, T.Y.; Burd, A. Stem cell-like properties of human umbilical cord lining epithelial cells and the potential for epidermal reconstitution. Cytotherapy 2011, 13, 145–155. [Google Scholar] [CrossRef]
- Saleh, R.; Reza, H.M. Short review on human umbilical cord lining epithelial cells and their potential clinical applications. Stem Cell Res. Ther. 2017, 8, 222. [Google Scholar] [CrossRef] [Green Version]
- Reza, H.M.; Ng, B.Y.; Gimeno, F.L.; Phan, T.T.; Ang, L.P. Umbilical Cord Lining Stem Cells as a Novel and Promising Source for Ocular Surface Regeneration. Stem Cell Rev. Rep. 2011, 7, 935–947. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Publication’s First Author, Year (Reference No.) Country | Type of Clinical Study/No. Surgeries or Eyes/Mean Time to Final Evaluation (months) | Type of Transplant (n), GMP 1 Followed for Product Preparation | Systemic Immunosuppressants in Allogeneic Transplants | Anatomical Success (Method of Evaluation)/Statistically Significant (s), Non-Significant (ns) or Not Mentioned (nm) |
|---|---|---|---|---|
| Shimazaki et al., 2007 [90] Japan | Retrospective, observational case series/27/31.6 | Auto 2-CLET 3 (7) Allo 5-CLET (20) No | CsA 4 for 6 months | Global: 59.3% (clinical) Auto-CLET 85.7% Allo-CLET: 50.0%/ns |
| Shortt et al., 2008 [91] UK | Prospective, noncomparative, interventional case series/10/6 or 13 | Auto-CLET (3) Allo-CLET (7) Yes | CsA for 6 months | Global: 60% (clinical, ccp-IVCM 6, impression cytology) Auto-CLET: 33% Allo-CLET: 71%/nm 7 |
| Pauklin et al., 2010 [92] Germany | Prospective noncomparative interventional case series/44/28.5 | Auto-CLET (30) Allo-CLET (14) No | CsA for 12–15 months (one case had none) | Global: 68% (clinical) Auto-CLET: 76.7% Allo-CLET: 50%/s |
| Prabhasawat et al., 2012 [93] Thailand | Prospective, noncomparative case series/19/26.1 | Auto-CLET (12) Allo-CLET (7) No | CsA for 6–12 months | Global: 73.7% (clinical) Auto-CLET: 66.7% Allo-CLET: 85.7%/ns |
| Zakaria et al., 2014 [94] Belgium | Phase I-II non-randomized clinical trial/18/22 | Auto-CLET (15) Allo-CLET (3) No | CsA for 12 months | Global: 66.7% (clinical) Auto-CLET: 66.7% Allo-CLET: 66.7%/ns |
| Ramírez et al., 2015 [24] Spain | Prospective noncomparative interventional case series/20/12, 24, 36 | Auto-CLET (11) Allo-CLET (9) Yes | Mycophenolate CsA or azathioprine for 12 months | Global (clinical, ccp-IVCM): 80% at 1–2 years; 75% at 3 years Auto-CLET: 90.9% Allo-CLET: 66.7%/ns |
| Ganger et al., 2015 [95] (India) | Retrospective case series/62 (38 children, 24 adults)/12 | Auto-CLET (54) Allo-CLET (8) No | No | Global: nm Auto-CLET: 87.8% children, 99.9% adults/ns Allo-CLET: 62.5%/ns |
| Parihar et al., 2017 [96] India | Prospective interventional/50/12 | Allo-CLET (25) Allo-LTT 8 (25) No | CsA for 12 months | Global (clinical): nm Both groups had significant improvement/ns |
| Sharma et al., 2018 [97] India, USA, Australia | Prospective comparative/40/12 | Auto-CLET (20) AMT 9 (20) No | Na 10 | Global (clinical): nm Similar results in both groups |
| Calonge et al., 2019 [89] Spain | Phase I-II, randomized, controlled, double-masked clinical trial/28/12 | Allo-MSCT 11 (17) Allo-CLET (11) Yes | Yes | Global (clinical ccp-IVCM): Allo-MSCT: 85.7% Allo-CLET: 77.8%/ns MSCT was as safe as CLET |
| Campbell et al., 2019 [98] UK | Randomized, controlled, single-masked, multicenter clinical trial/16 | Allo-CLE (11) AMT (5) Yes | Prednisolone plus CsA or mycophenolate for 12 months | Global (clinical): nm sustained significant improvement in allo-CLET but not in AMT |
| Borderie et al., 2019 [47] France | Phase II, noncomparative clinical trial: CLET vs. retrospective control: LTT/30 /72 vs. 132 | Auto-CLET (7) Allo-CLET (7) Auto-LTT (8) Allo-LTT (8) No | Allo-CLET: NO Allo-LTT: CsA, steroids or chloraminophen for 12 months | Global survival (clinical) at 5 years/nm Auto-CLET: 71% Allo-CLET: 0% Auto-LTT: 75% Allo-LTT: 33% |
| Wang et al., 2019 [58] China | Retrospective cohort study/76/23.3 vs. 16.1 | Allo-CLET (42) Auto-COMET 12 (34) No | No (only oral corticosteroids for 2–3 months) | Global (clinical): nm Allo-CLET: 71.4% (Immune rejections: 9.5%) COMET: 52.9%) |
| Behaegel et al., 2019 [99] Belgium | Prospective, noncomparative case series (first 2 years); Later follow-up or retrospective review/13/2.1 (short-term) vs. 6.7 (long-term) | Auto-CLET (9) Allo-CLET (4) Yes | Not specified | Global short-term: 46.1% Auto-CLET: 77.8% Allo-CLET: 75% Global long-term: 23.1%/ns Auto-CLET: 55% Allo-CLET: 0% Success decreased over time |
| Shimazaki et al. [100] 2020 Japan | Retrospective analysis/246/89.3 | Auto-CLET + auto-COMET (171) Allo-CLET (75) No | CsA for unknown period | Global (clinical): 65.1% Auto-CLET + COMET: 65.6% Allo-CLET: 63.0%/ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calonge, M.; Nieto-Miguel, T.; de la Mata, A.; Galindo, S.; Herreras, J.M.; López-Paniagua, M. Goals and Challenges of Stem Cell-Based Therapy for Corneal Blindness Due to Limbal Deficiency. Pharmaceutics 2021, 13, 1483. https://doi.org/10.3390/pharmaceutics13091483
Calonge M, Nieto-Miguel T, de la Mata A, Galindo S, Herreras JM, López-Paniagua M. Goals and Challenges of Stem Cell-Based Therapy for Corneal Blindness Due to Limbal Deficiency. Pharmaceutics. 2021; 13(9):1483. https://doi.org/10.3390/pharmaceutics13091483
Chicago/Turabian StyleCalonge, Margarita, Teresa Nieto-Miguel, Ana de la Mata, Sara Galindo, José M. Herreras, and Marina López-Paniagua. 2021. "Goals and Challenges of Stem Cell-Based Therapy for Corneal Blindness Due to Limbal Deficiency" Pharmaceutics 13, no. 9: 1483. https://doi.org/10.3390/pharmaceutics13091483