
Sustained Intra-Articular Release and Biocompatibility of Tacrolimus (FK506) Loaded Monospheres Composed of [PDLA-PEG1000]-b-[PLLA] Multi-Block Copolymers in Healthy Horse Joints

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Tacrolimus-Loaded Monospheres
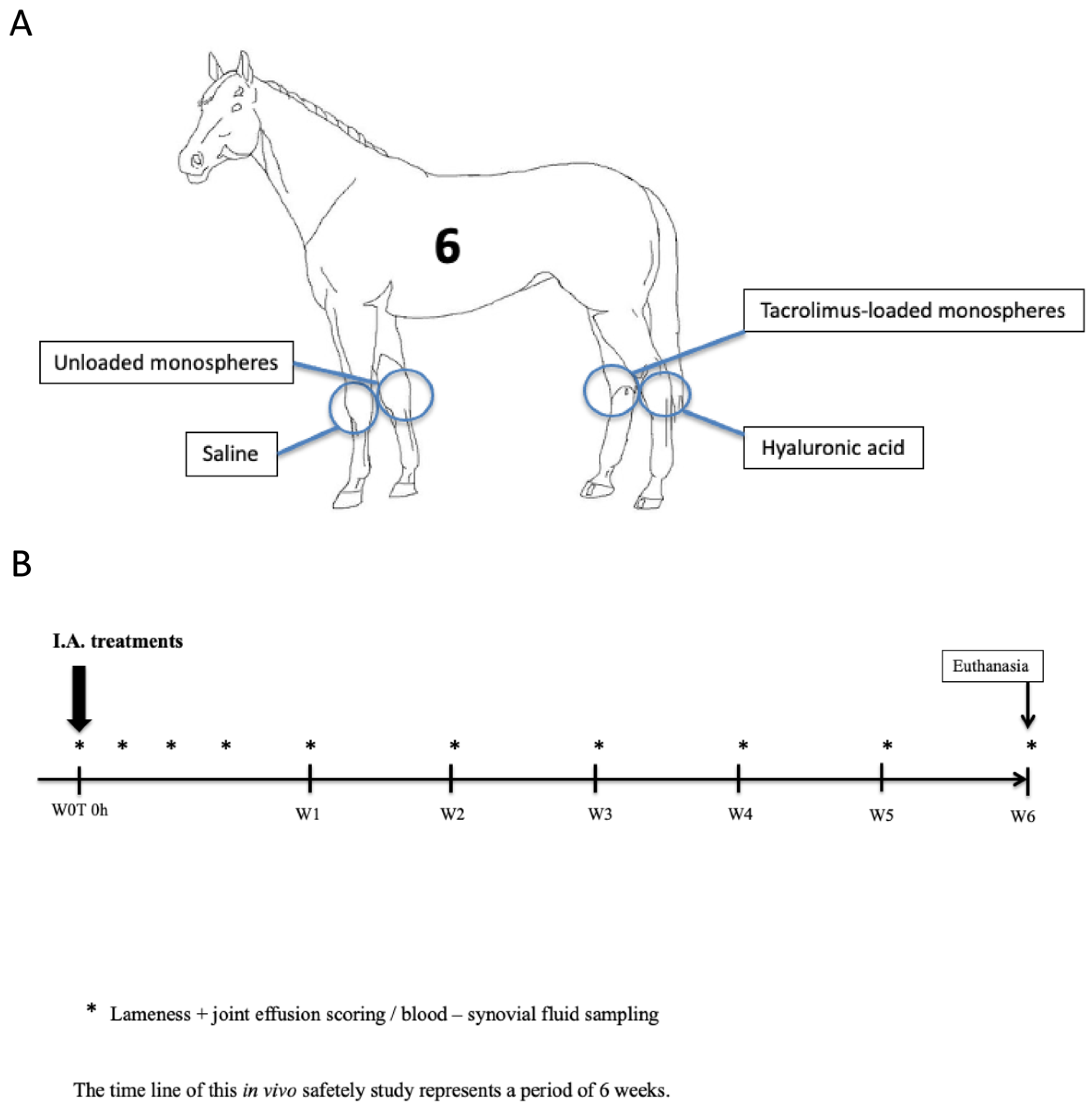
2.2. In Vivo Experimental Set Up
2.3. Evaluation of Clinical Response to the Treatment
2.4. Collection of Synovial Fluid and Plasma
2.5. Tacrolimus Concentrations in the Synovial Fluid and Serum
2.6. Synovial Fluid Analysis
2.7. Histological Analysis and Grading of Articular Cartilage and Synovial Lining
2.8. Statistical Analysis
3. Results
3.1. Clinical Response to the Intra-Articular Injections
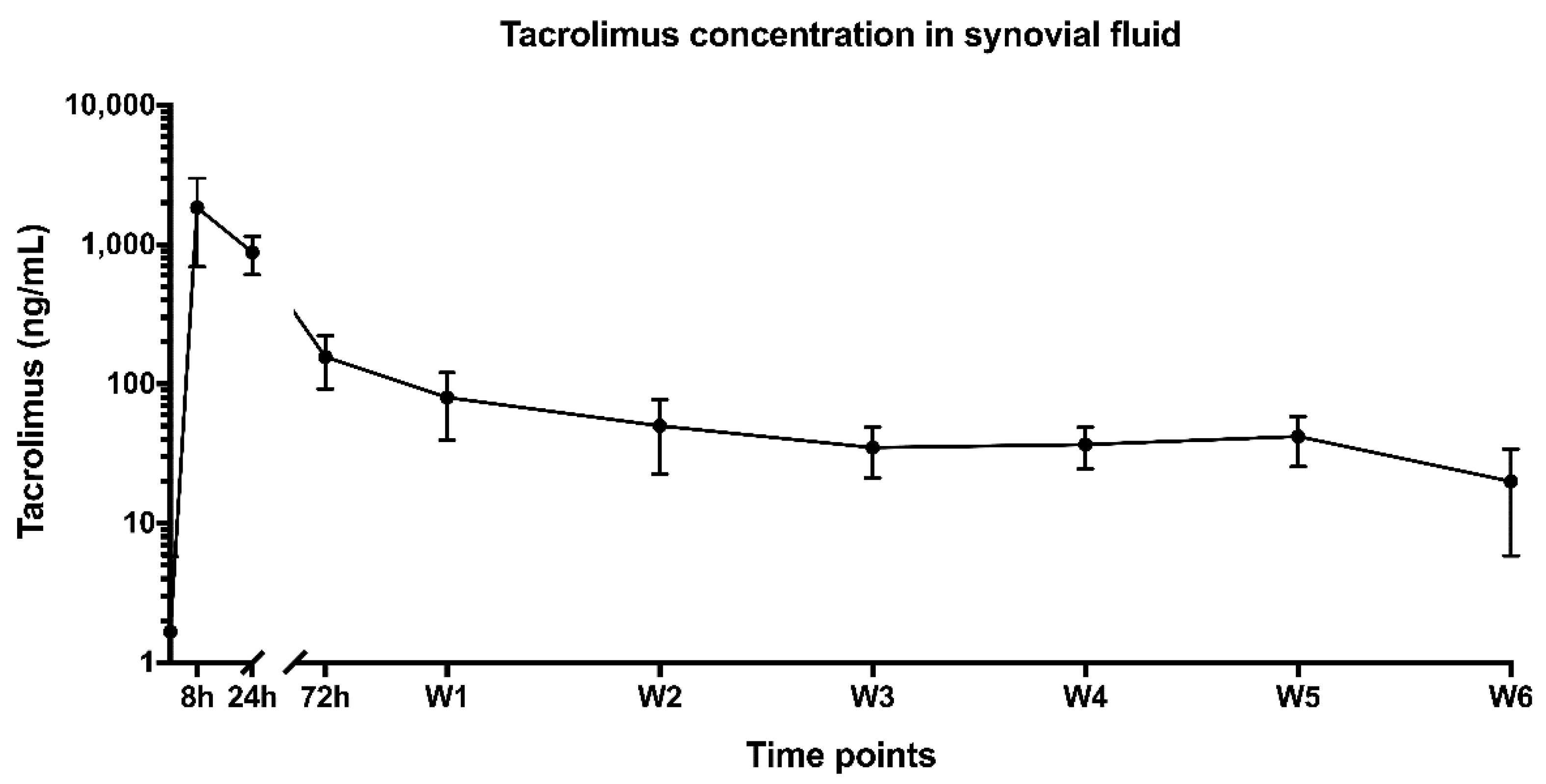
3.2. Release Kinetics of Tacrolimus-Loaded Monospheres in Healthy Horse Joints
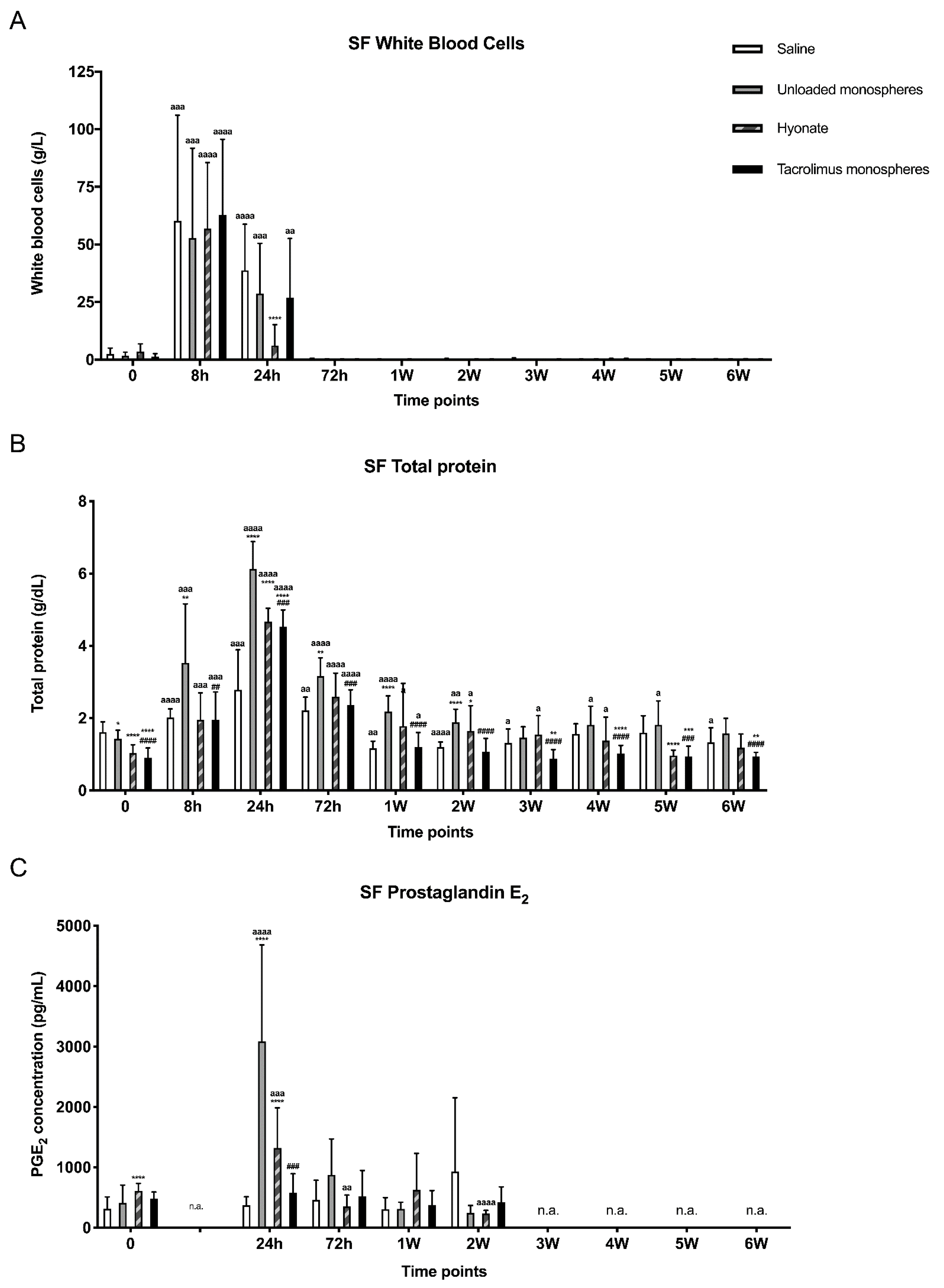
3.3. Local Inflammatory Response
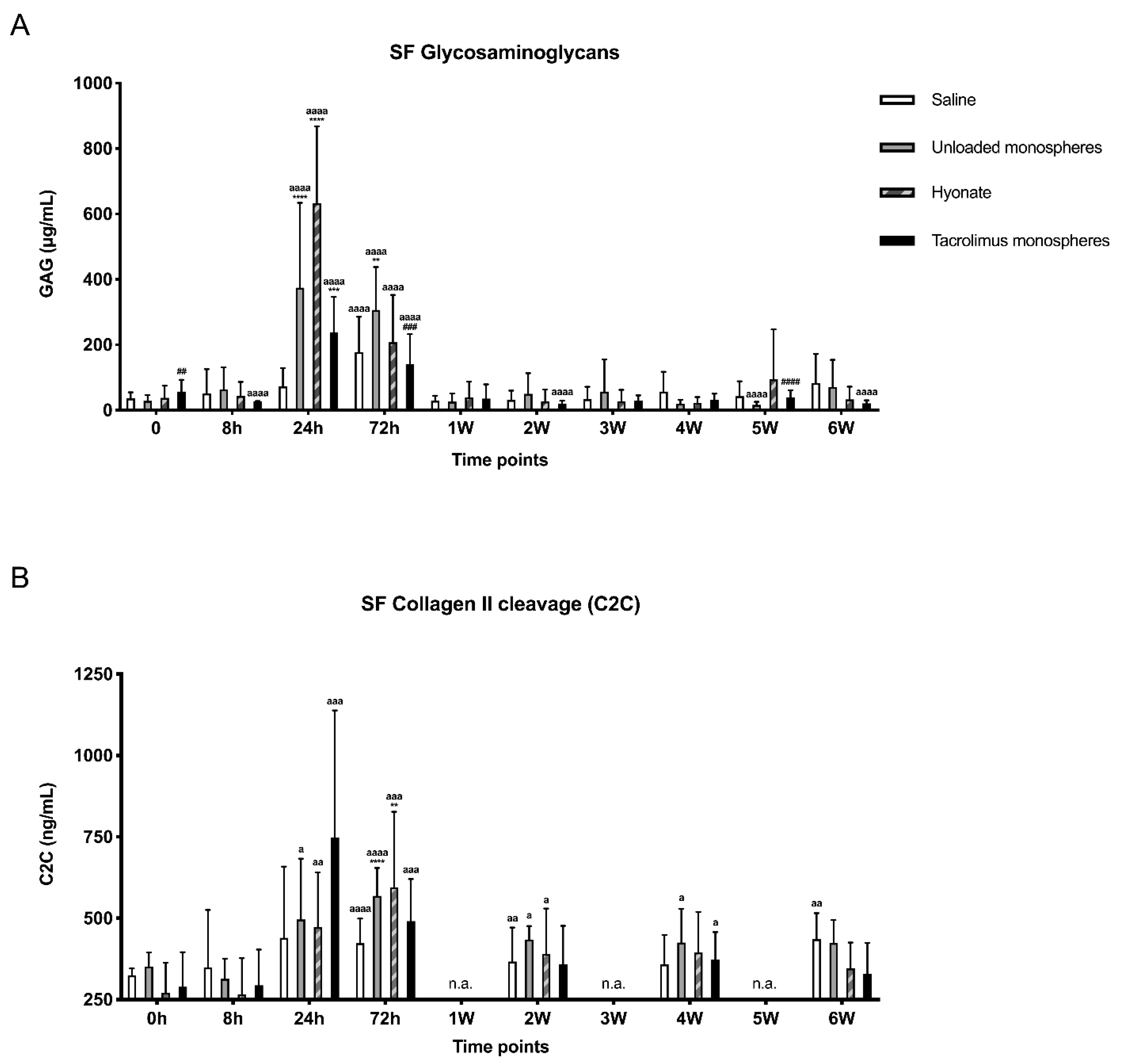
3.4. Response of Synovial Fluid Markers of Cartilage Metabolism
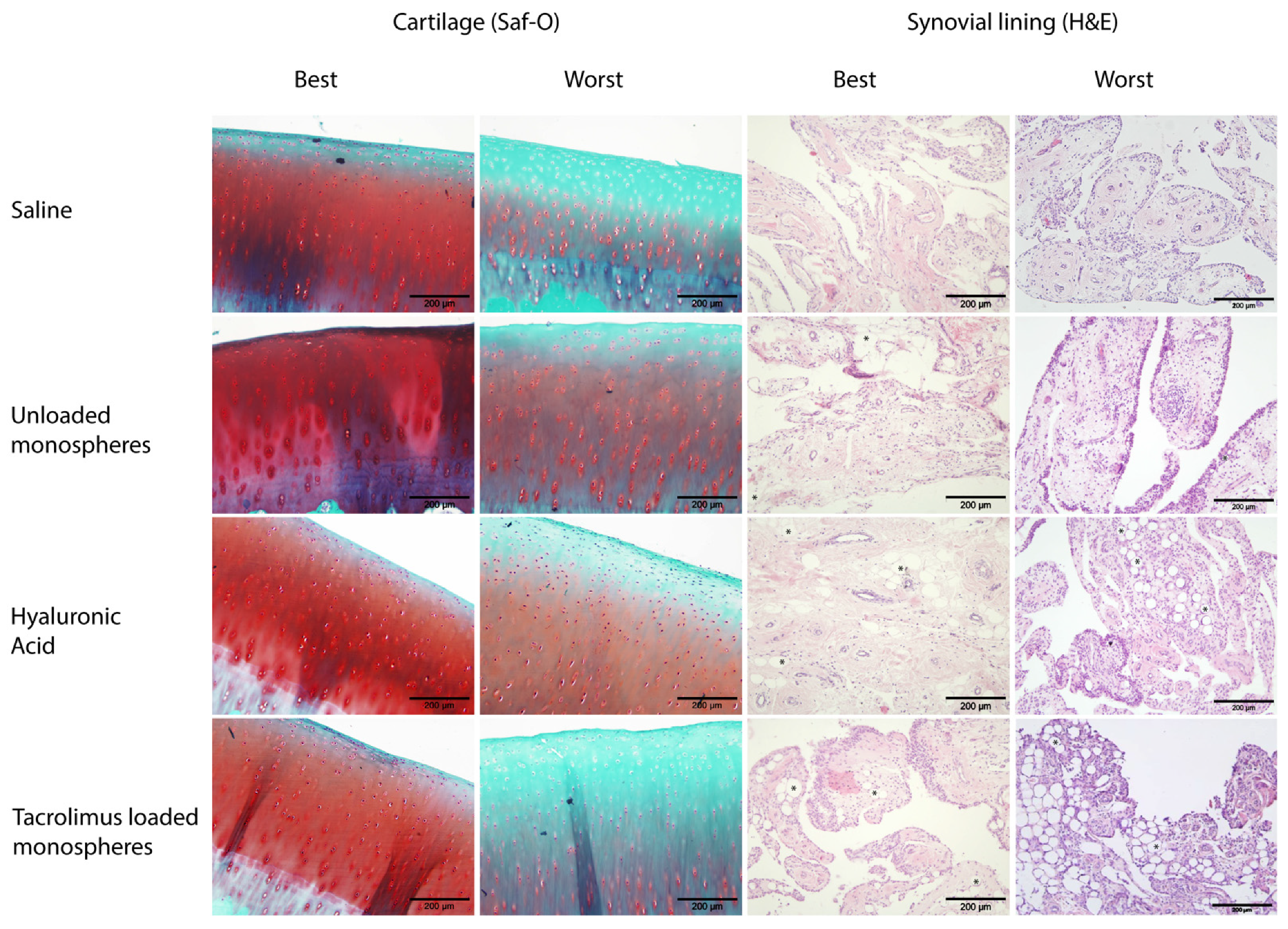
3.5. Histological Analysis
4. Discussion
4.1. Release Kinetics from Tacrolimus-Loaded Monospheres in Healthy Horse Joints
4.2. Response to the Intra-Articular Injections
4.2.1. Inflammatory Response
4.2.2. Local Effect on Cartilage
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Urwin, M.; Symmons, D.; Allison, T.; Brammah, T.; Busby, H.; Roxby, M.; Simmons, A.; Williams, G. Estimating the burden of musculoskeletal disorders in the community: The comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann. Rheum. Dis. 1998, 57, 649–655. [Google Scholar] [CrossRef]
- Van Weeren, P.R. General anatomy and physiology of joints. In Joint Disease in the Horse; McIlwraith, C.W., Frisbie, D.D., Kawcak, C.E., van Weeren, P.R., Eds.; Elsevier: St. Louis, MO, USA, 2016; p. 1. [Google Scholar]
- Fazal, S.A.; Khan, M.; Nishi, S.E.; Alam, F.; Zarin, N.; Bari, M.T.; Ashraf, G.M. A Clinical Update and Global Economic Burden of Rheumatoid Arthritis. Endocr. Metab. Immune Disord Drug. Targets 2018, 18, 98–109. [Google Scholar] [CrossRef]
- Prieto-Alhambra, D.; Judge, A.; Javaid, M.K.; Cooper, C.; Diez-Perez, A.; Arden, N.K. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann. Rheum. Dis. 2014, 73, 1659–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, B.; Gabriel, S.; Lassere, M.; Johns, N.; et al. The global burden of rheumatoid arthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1316–1322. [Google Scholar] [CrossRef] [PubMed]
- Goldring, M.B.; Goldring, S.R. Osteoarthritis. J. Cell Physiol. 2007, 213, 626–634. [Google Scholar] [CrossRef]
- Pap, T.; Korb-Pap, A. Cartilage damage in osteoarthritis and rheumatoid arthritis—two unequal siblings. Nat. Rev. Rheumatol. 2015, 11, 606–615. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, T.W.; McCabe, P.S.; McBeth, J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 312–326. [Google Scholar] [CrossRef]
- Losina, E.; Katz, J.N. Improvement at Any Cost? The Art and Science of Choosing Treatment Strategies for Rheumatoid Arthritis. Ann. Intern. Med. 2017, 167, 55–56. [Google Scholar] [CrossRef]
- Evans, C.H.; Kraus, V.B.; Setton, L.A. Progress in intra-articular therapy. Nat. Rev. Rheumatol. 2014, 10, 11–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Boom, R.; van de Lest, C.H.A.; Bull, S.; Brama, R.A.J.; van Weeren, P.R.; Barneveld, A. Influence of repeated arthrocentesis and exercise on synovial fluid concentrations of nitric oxide, prostaglandin E2 and glycosaminoglycans in healthy equine joints. Equine Vet. J. 2005, 37, 250–256. [Google Scholar] [CrossRef]
- Larsen, C.; Ostergaard, J.; Larsen, S.W.; Jensen, H.; Jacobsen, S.; Lindegaard, C.; Andersen, P.H. Intra-articular depot formulation principles: Role in the management of postoperative pain and arthritic disorders. J. Pharm. Sci. 2008, 97, 4622–4654. [Google Scholar] [CrossRef] [PubMed]
- Butoescu, N.; Jordan, O.; Doelker, E. Intra-articular drug delivery systems for the treatment of rheumatic diseases: A review of the factors influencing their performance. Eur. J. Pharm. Biopharm. 2009, 73, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Badri, W.; Miladi, K.; Nazari, Q.A.; Greige-Gerges, H.; Fessi, H.; Elaissari, A. Encapsulation of NSAIDs for inflammation management: Overview, progress, challenges and prospects. Int. J. Pharm. 2016, 515, 757–773. [Google Scholar] [CrossRef]
- Scott, L.J.; McKeage, K.; Keam, S.J.; Plosker, G.L. Tacrolimus: A further update of its use in the management of organ transplantation. Drugs 2003, 63, 1247–1297. [Google Scholar] [CrossRef]
- Van Dieren, J.M.; van Bodegraven, A.A.; Kuipers, E.J.; Bakker, E.N.; Poen, A.C.; van Dekken, H.; Nieuwenhuis, E.E.S.; van der Woude, C.J. Local application of tacrolimus in distal colitis: Feasible and safe. Inflamm. Bowel Dis. 2009, 15, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Albaghdadi, A.J.H.; Kan, F.W.K. Therapeutic Potentials of Low-Dose Tacrolimus for Aberrant Endometrial Features in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2021, 22, 2872. [Google Scholar] [CrossRef]
- Takeuchi, T.; Ishida, K.; Shiraki, K.; Yoshiyasu, T. Safety and effectiveness of tacrolimus add-on therapy for rheumatoid arthritis patients without an adequate response to biological disease-modifying anti-rheumatic drugs (DMARDs): Post-marketing surveillance in Japan. Mod. Rheumatol. 2018, 28, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.H.; Woo, J.-H.; Choi, S.J.; Ji, J.D.; Bae, S.-C.; Song, G.G. Tacrolimus for the treatment of active rheumatoid arthritis: A systematic review and meta-analysis of randomized controlled trials. Scand. J. Rheumatol. 2010, 39, 271–278. [Google Scholar] [CrossRef]
- Siebelt, M.; van der Windt, A.E.; Groen, H.C.; Sandker, M.; Waarsing, J.H.; Müller, C.; de Jong, M.; Jahr, H.; Weinans, H. FK506 protects against articular cartilage collagenous extra-cellular matrix degradation. Osteoarthr. Cartil. 2014, 22, 591–600. [Google Scholar] [CrossRef] [Green Version]
- Magari, K.; Nishigaki, F.; Sasakawa, T.; Ogawa, T.; Miyata, S.; Ohkubo, Y.; Mutoh, S.; Goto, T. Anti-arthritic properties of FK506 on collagen-induced arthritis in rats. Inflamm. Res. 2003, 52, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Kino, T.; Hatanaka, H.; Miyata, S.; Inamura, N.; Nishiyama, M.; Yajima, T.; Goto, T.; Okuhara, M.; Kohsaka, M.; Aoki, H. FK-506, a novel immunosuppressant isolated from a Streptomyces. II. Immunosuppressive effect of FK-506 in vitro. J. Antibiot. 1987, 40, 1256–1265. [Google Scholar] [CrossRef]
- Miyata, S.; Ohkubo, Y.; Mutoh, S. A review of the action of tacrolimus (FK506) on experimental models of rheumatoid arthritis. Inflamm. Res. 2005, 54, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, S.; Kato, Y.; Nishigaki, F.; Sasakawa, T.; Magari, K.; Miyata, S.; Ohkubo, Y.; Goto, T. FK506 potently inhibits T cell activation induced TNF-alpha and IL-1beta production in vitro by human peripheral blood mononuclear cells. Br. J. Pharmacol. 2000, 130, 1655–1663. [Google Scholar] [CrossRef]
- Kitahara, K.; Kusunoki, N.; Takahashi, H.; Tsuchiya, K.; Kawai, S. Tacrolimus down-regulates chemokine expressions on rheumatoid synovial fibroblasts: Screening by a DNA microarray. Inflamm. Res. 2012, 61, 1385–1394. [Google Scholar] [CrossRef]
- Kang, K.Y.; Ju, J.H.; Song, Y.W.; Yoo, D.-H.; Kim, H.-Y.; Park, S.-H. Tacrolimus treatment increases bone formation in patients with rheumatoid arthritis. Rheumatol. Int. 2013, 33, 2159–2163. [Google Scholar] [CrossRef] [PubMed]
- Bechstein, W.O. Neurotoxicity of calcineurin inhibitors: Impact and clinical management. Transpl. Int. 2000, 13, 313–326. [Google Scholar] [CrossRef]
- Andoh, T.F.; Burdmann, E.A.; Bennett, W.M. Nephrotoxicity of immunosuppressive drugs: Experimental and clinical observations. Semin. Nephrol. 1997, 17, 34–45. [Google Scholar] [PubMed]
- Curran, M.P.; Perry, C.M. Tacrolimus: In patients with rheumatoid arthritis. Drugs 2005, 65, 993–1001. [Google Scholar] [CrossRef]
- Sandker, M.J.; Duque, L.F.; Redout, E.M.; Chan, A. Degradation, intra-articular retention and biocompatibility of monospheres composed of [PDLLA-PEG-PDLLA]-b-PLLA multi-block copolymers. Acta Biomater. 2017, 48, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.; Pack, D.W.; Klibanov, A.M.; Langer, R. Visual evidence of acidic environment within degrading poly(lactic-co-glycolic acid) (PLGA) microspheres. Pharm. Res. 2000, 17, 100–106. [Google Scholar] [CrossRef]
- Sandker, M.J.; Duque, L.F.; Redout, E.M.; Klijnstra, E.C.; Steendam, R.; Kops, N.; Waarsing, J.H.; van Weeren, R.; Hennink, W.E.; Weinans, H. Degradation, Intra-Articular Biocompatibility, Drug Release, and Bioactivity of Tacrolimus-Loaded Poly( d- l-lactide-PEG)- b-poly( l-lactide) Multiblock Copolymer-Based Monospheres. ACS Biomater. Sci. Eng. 2018, 4, 2390–2403. [Google Scholar] [CrossRef] [PubMed]
- Petit, A.; Sandker, M.; Müller, B.; Meyboom, R.; van Midwoud, P.; Bruin, P.; Redout, E.M.; Versluijs-Helder, M.; van der Lest, C.H.A.; Buwalda, S.J.; et al. Release behavior and intra-articular biocompatibility of celecoxib-loaded acetyl-capped PCLA-PEG-PCLA thermogels. Biomaterials 2014, 35, 7919–7928. [Google Scholar] [CrossRef]
- McIlwraith, C.W.; Fortier, L.A.; Frisbie, D.D.; Nixon, A.J. Equine Models of Articular Cartilage Repair. Cartilage 2011, 2, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.E. The horse as a model of naturally occurring osteoarthritis. Bone Jt. Res. 2012, 1, 297–309. [Google Scholar] [CrossRef] [PubMed]
- AAEP Horse Show Committee. Guide to Veterinary Services for Horse Shows, 7th ed.; American Association of Equine Practitioners, Ed.; American Association of Equine Practitioners: Lexington, KY, USA, 1999. [Google Scholar]
- Bertone, A.L.; Palmer, J.L.; Jones, J. Synovial Fluid Cytokines and Eicosanoids as Markers of Joint Disease in Horses. Vet. Surg. 2001, 30, 528–538. [Google Scholar] [CrossRef] [PubMed]
- De Grauw, J.C.; van ve Lest, C.H.A.; Brama, P.A.J.; Rambags, B.P.B.; van Weeren, P.R. In vivo effects of meloxicam on inflammatory mediators, MMP activity and cartilage biomarkers in equine joints with acute synovitis. Equine Vet. J. 2010, 41, 693–699. [Google Scholar] [CrossRef] [PubMed]
- De Grauw, J.C.; van de Lest, C.H.A.; van Weeren, R.; Brommer, H.; Brama, P.A.J. Arthrogenic lameness of the fetlock: Synovial fluid markers of inflammation and cartilage turnover in relation to clinical joint pain. Equine Vet. J. 2006, 38, 305–311. [Google Scholar] [CrossRef]
- De Grauw, J.C.; van de Lest, C.H.A.; van Weeren, P.R. A targeted lipidomics approach to the study of eicosanoid release in synovial joints. Arthritis Res. Ther. 2011, 13, R123. [Google Scholar] [CrossRef] [Green Version]
- McIlwraith, C.W.; Frisbie, D.D.; Kawcak, C.E.; Fuller, C.J.; Hurtig, M.; Cruz, A. The OARSI histopathology initiative—Recommendations for histological assessments of osteoarthritis in the horse. Osteoarthr. Cartil. 2010, 18 (Suppl. S3), S93–S105. [Google Scholar] [CrossRef] [Green Version]
- Gawlitta, D.; van Rijen, M.H.P.; Schrijver, E.J.M.; Alblas, J.; Dhert, W.J.A. Hypoxia impedes hypertrophic chondrogenesis of human multipotent stromal cells. Tissue Eng. Part A 2012, 18, 1957–1966. [Google Scholar] [CrossRef] [PubMed]
- Egeland, E.J.; Robertsen, I.; Hermann, M.; Midtvedt, K.; Størset, E.; Gustavsen, M.T.; Reisæter, A.V.; Klaasen, R.; Bergan, S.; Holdaas, H.; et al. High Tacrolimus Clearance Is a Risk Factor for Acute Rejection in the Early Phase After Renal Transplantation. Transplantation 2017, 101, e273–e279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallis, W.J.; Simkin, P.A.; Nelp, W.B.; Foster, D.M. Intraarticular volume and clearance in human synovial effusions. Arthritis Rheum. 1985, 28, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Pitsillides, A.A.; Will, R.K.; Bayliss, M.T.; Edwards, J.C. Circulating and synovial fluid hyaluronan levels. Effects of intraarticular corticosteroid on the concentration and the rate of turnover. Arthritis Rheum. 1994, 37, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Hilton, H.; Affolter, V.K.; White, S.D. Evaluation of four topical preparations for the treatment of cannon hyperkeratosis in a horse. Vet. Dermatol. 2008, 19, 385–390. [Google Scholar] [CrossRef]
- González-Medina, S. Equine eosinophilic keratitis: An emergent ocular condition? Equine Vet. Educ. 2019, 31, 609–616. [Google Scholar] [CrossRef]
- Kershner, R.P.; Fitzsimmons, W.E. Relationship of FK506 whole blood concentrations and efficacy and toxicity after liver and kidney transplantation. Transplantation 1996, 62, 920–926. [Google Scholar] [CrossRef]
- Ogata, H.; Matsui, T.; Nakamura, M.; Iida, M.; Takazoe, M.; Suzuki, Y.; Hibi, T. A randomised dose finding study of oral tacrolimus (FK506) therapy in refractory ulcerative colitis. Gut 2006, 55, 1255–1262. [Google Scholar] [CrossRef] [Green Version]
- Owens, J.G.; Kamerling, S.G.; Stanton, S.R.; Keowen, M.L.; Prescott-Mathews, J.S. Effects of pretreatment with ketoprofen and phenylbutazone on experimentally induced synovitis in horses. Am. J. Vet. Res. 1996, 57, 866–874. [Google Scholar]
- Kalinski, P. Regulation of Immune Responses by Prostaglandin E2. J. Immunol. 2012, 188, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Cokelaere, S.M.; Plomp, S.G.M.; de Boef, E.; de Leeuw, M.; Bool, S.; van de Lest, C.H.A.; van Weeren, P.R.; Korthagen, N.M. Sustained intra-articular release of celecoxib in an equine repeated LPS synovitis model. Eur J. Pharm. Biopharm. 2018, 128, 327–336. [Google Scholar] [CrossRef]
- Johnston, G.C.A.; Wood, K.A.; Jackson, K.V.; Perkins, N.R.; Zedler, S.T. Evaluation of the inflammatory response to two intra-articular hyaluronic acid formulations in normal equine joints. J. Vet. Pharmacol. Ther. 2020, 43, 38–49. [Google Scholar] [CrossRef] [PubMed]
- De Grauw, J.C.; van de Lest, C.H.; van Weeren, P.R. Inflammatory mediators and cartilage biomarkers in synovial fluid after a single inflammatory insult: A longitudinal experimental study. Arthritis Res. Ther. 2009, 11, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, P.; Deshpande, S.; Koppikar, S.; Patil, S.; Ingale, D.; Harsulkar, A. Glycosaminoglycan measured from synovial fluid serves as a useful indicator for progression of Osteoarthritis and complements Kellgren-Lawrence Score. BBA Clin. 2016, 6, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frisbie, D.D.; Al-Sobayil, F.; Billinghurst, R.C.; Kawcak, C.E.; McIlwraith, C.W. Changes in synovial fluid and serum biomarkers with exercise and early osteoarthritis in horses. Osteoarthr. Cartil. 2008, 16, 1196–1204. [Google Scholar] [CrossRef] [Green Version]
- Van der Windt, A.E.; Jahr, H.; Farrell, E.; Verhaar, J.A.N.; Weinans, H.; van Osch, G.J.V.M. Calcineurin inhibitors promote chondrogenic marker expression of dedifferentiated human adult chondrocytes via stimulation of endogenous TGFbeta1 production. Tissue Eng. Part A 2010, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Van der Windt, A.E.; Haak, E.; Kops, N.; Verhaar, J.A.N.; Weinans, H.; Jahr, H. Inhibiting calcineurin activity under physiologic tonicity elevates anabolic but suppresses catabolic chondrocyte markers. Arthritis Rheum. 2012, 64, 1929–1939. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unloaded | Tacrolimus-Loaded | |
|---|---|---|
| Polymer | 16[PDLA-PEG1000]-84[PLLA] | 16[PDLA-PEG1000]-84[PLLA] |
| Average particle size | 37 µm | 39 µm |
| Morphology | Smooth and non-porous 1 | Smooth and non-porous 1 |
| FK506 loading | N.A. | 9.2% |
| Encapsulation efficiency | N.A. | 92% |
| Injection volume per joint | 3 mL | 3 mL |
| Monospheres injected per joint | 200 mg | 200 mg |
| Dose FK506 injected per joint | 0 mg | 18.4 mg |
| Saline | Unloaded Monospheres | Hyaluronic Acid | Tacrolimus Monospheres | |
|---|---|---|---|---|
| Synovial membrane score | 5 (4–7) | 6.5 (5–8) | 8.5 (4–11) | 6 (4–8) |
| Cartilage microscopic grade | 4.5 (4–7) | 6.5 (4–8) | 8 (4–10) | 6 (4–8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cokelaere, S.M.; Groen, W.M.G.A.C.; Plomp, S.G.M.; de Grauw, J.C.; van Midwoud, P.M.; Weinans, H.H.; van de Lest, C.H.A.; Tryfonidou, M.A.; van Weeren, P.R.; Korthagen, N.M. Sustained Intra-Articular Release and Biocompatibility of Tacrolimus (FK506) Loaded Monospheres Composed of [PDLA-PEG1000]-b-[PLLA] Multi-Block Copolymers in Healthy Horse Joints. Pharmaceutics 2021, 13, 1438. https://doi.org/10.3390/pharmaceutics13091438
Cokelaere SM, Groen WMGAC, Plomp SGM, de Grauw JC, van Midwoud PM, Weinans HH, van de Lest CHA, Tryfonidou MA, van Weeren PR, Korthagen NM. Sustained Intra-Articular Release and Biocompatibility of Tacrolimus (FK506) Loaded Monospheres Composed of [PDLA-PEG1000]-b-[PLLA] Multi-Block Copolymers in Healthy Horse Joints. Pharmaceutics. 2021; 13(9):1438. https://doi.org/10.3390/pharmaceutics13091438
Chicago/Turabian StyleCokelaere, Stefan M., Wilhelmina M.G.A.C. Groen, Saskia G.M. Plomp, Janny C. de Grauw, Paul M. van Midwoud, Harrie H. Weinans, Chris H.A. van de Lest, Marianna A. Tryfonidou, P. René van Weeren, and Nicoline M. Korthagen. 2021. "Sustained Intra-Articular Release and Biocompatibility of Tacrolimus (FK506) Loaded Monospheres Composed of [PDLA-PEG1000]-b-[PLLA] Multi-Block Copolymers in Healthy Horse Joints" Pharmaceutics 13, no. 9: 1438. https://doi.org/10.3390/pharmaceutics13091438