
Drug Delivery by Ultrasound-Responsive Nanocarriers for Cancer Treatment


Abstract
:1. Introduction
2. Physics of Ultrasound and Its Biological Effects
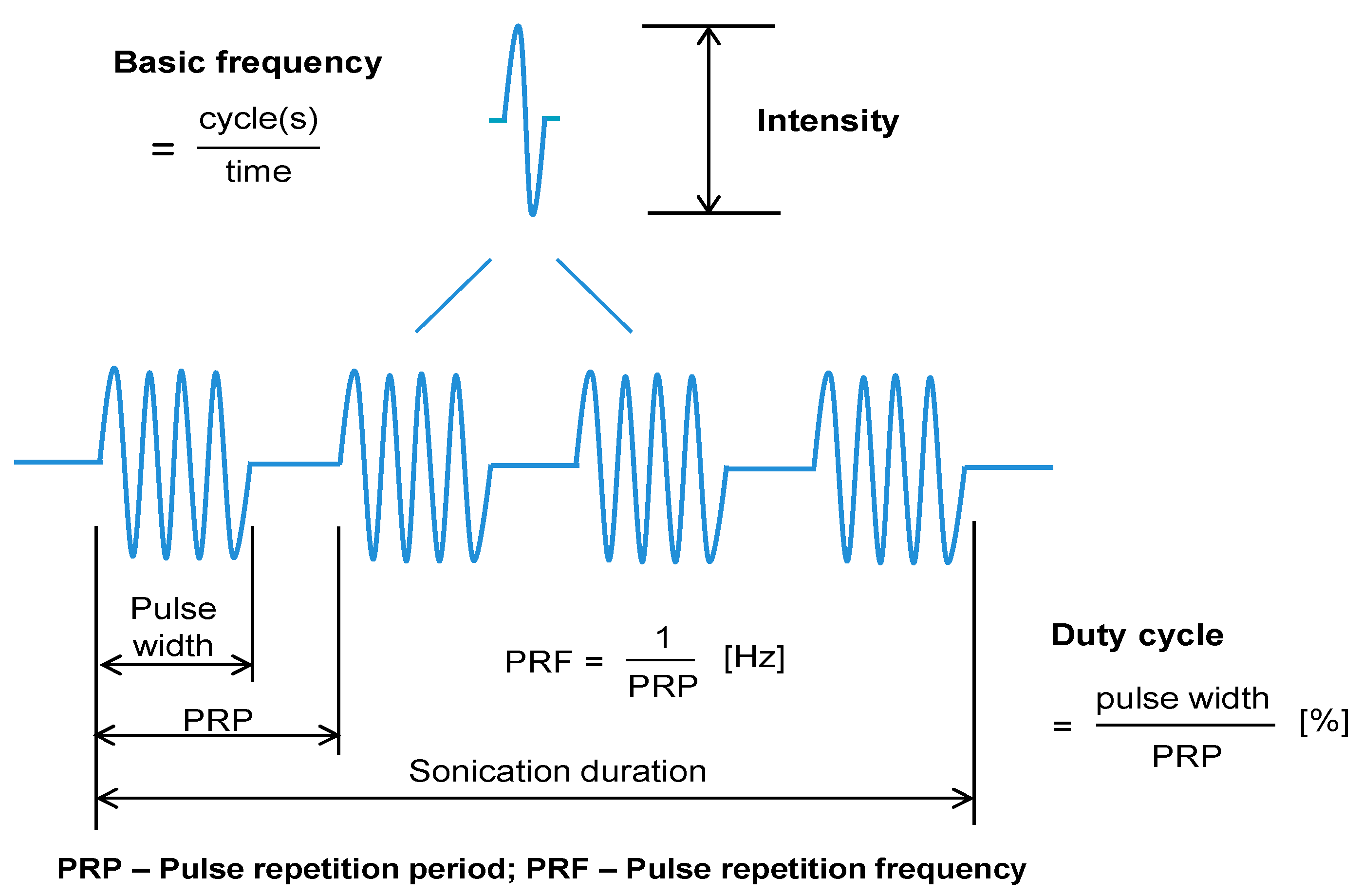
2.1. Frequency
2.2. Intensity and US-Focus
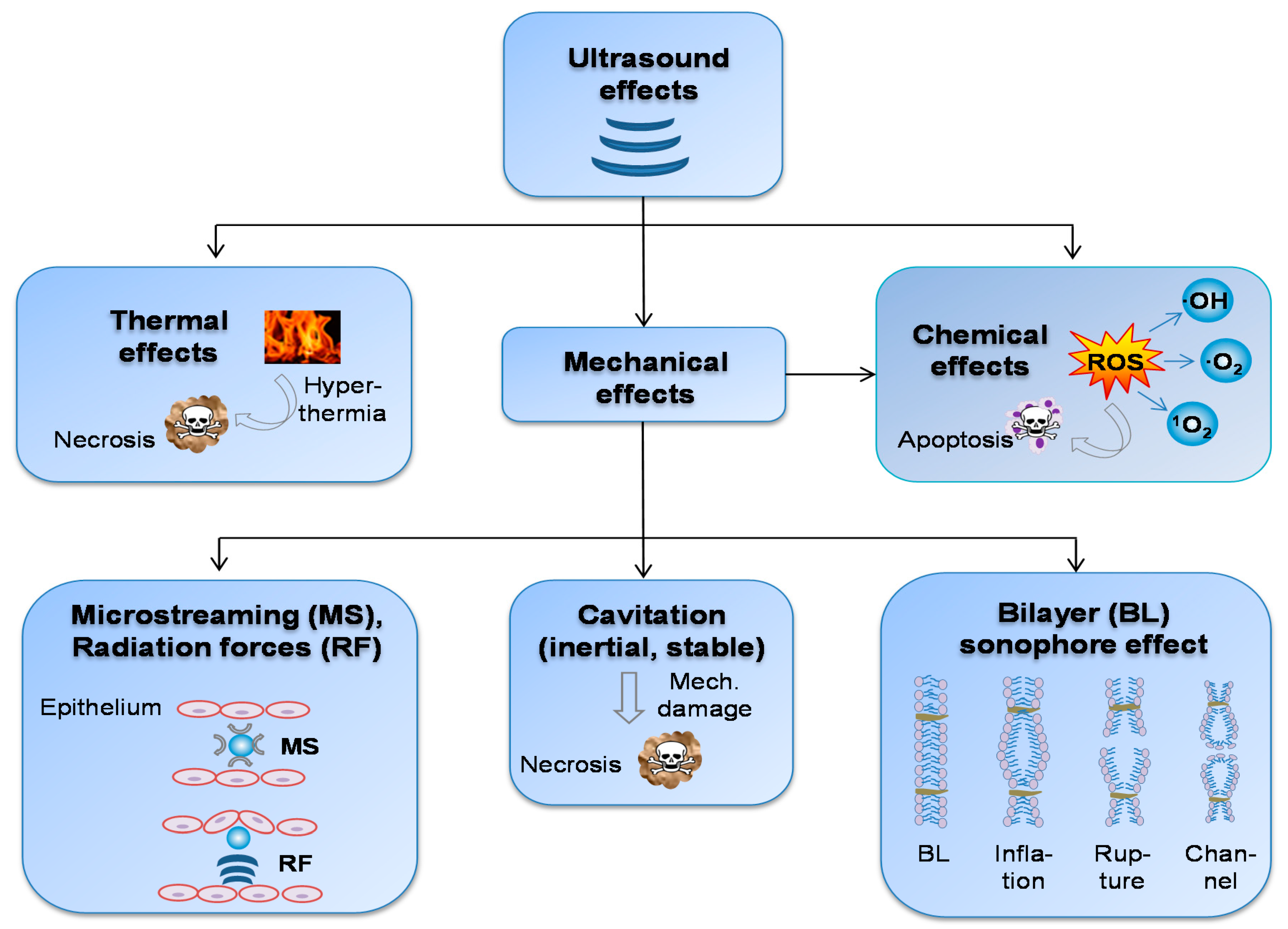
2.3. Biological US-Effects
2.3.1. Temperature Impact on Biological Effects
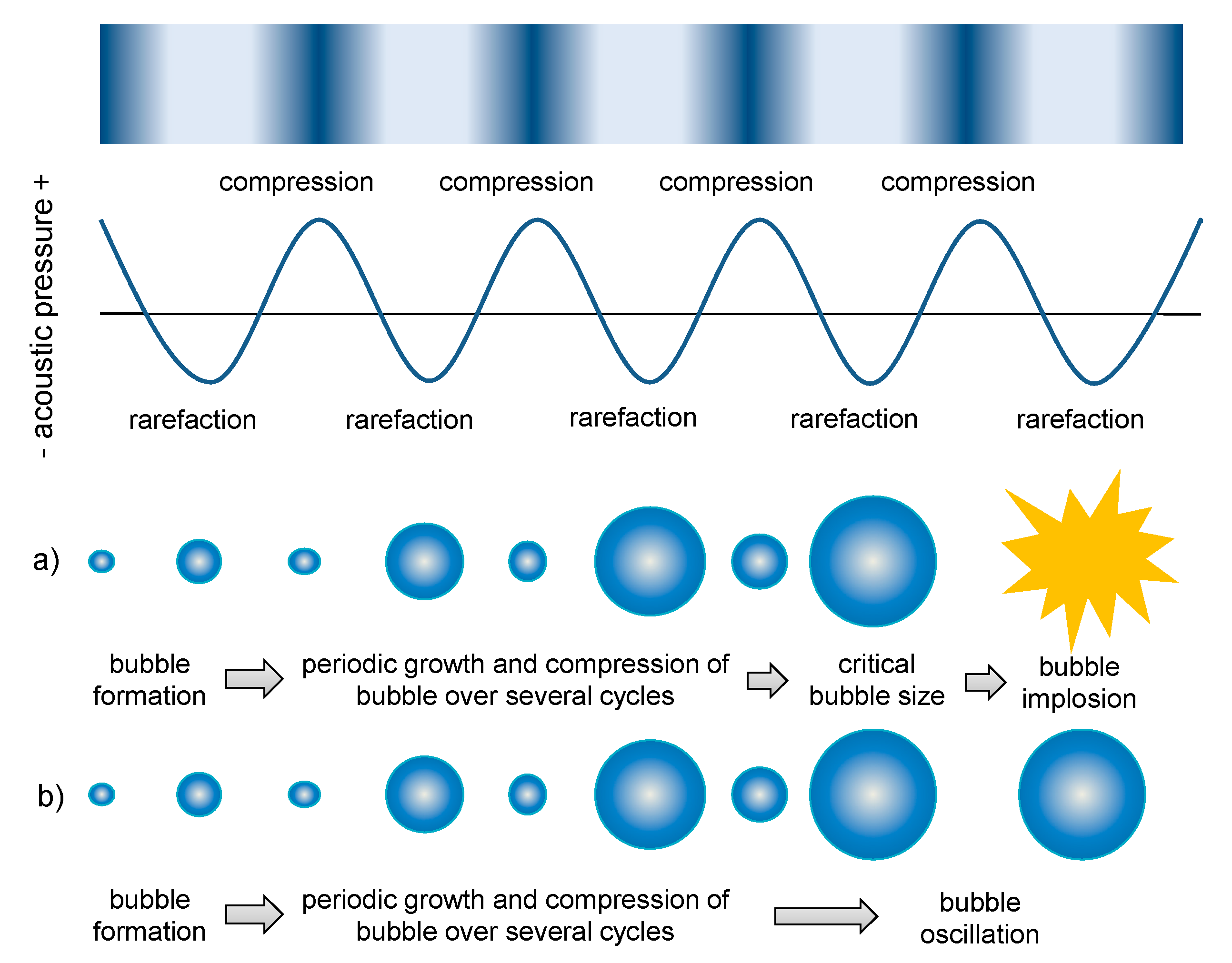
2.3.2. Mechanical Impact on Biological Effects
2.3.3. Bilayer Sonophore Effect
2.3.4. Alteration of Biodistribution
3. Concepts in Ultrasound-Triggered Drug Delivery
4. Role of Nanocarrier Properties for Ultrasound-Triggered Drug Delivery
5. Materials Used for Nano-/Microparticle Development
6. Drug Release Mechanisms and Nano-/Microparticle Types
6.1. Thermal Drug Release and Liposomes
6.2. Mechanical- and Multiple-Triggered Drug Release
6.2.1. Microbubbles
6.2.2. Nanobubbles
6.2.3. Micelles
6.2.4. Mesoporous Silica Nanoparticles (MSNs)
6.3. Natural Nanocarriers: Exosomes
7. Applications In Vivo

{kind=link}
{kind=link}
{kind=link}
| Particles: Composition | Drug/Dose [mg/kg] | US Method/Principle of Action | US Parameters/HT Protocol | Animal/ Tumor | TV [mm³] at TrS (d = 0) | Results after TIm/TrS at Day | TVR [%]/ VIR [%] | Remarks/ Special Features | Ref. | |
|---|---|---|---|---|---|---|---|---|---|---|
| (+) US | (-) US | |||||||||
| MBs: 1. oxygen and PTX loaded PFC-MB (OPLMBs) | PTX/ 20 | Non-FUS/ UTMD | Freq.: 300 kHz, Intens.: 1 W/cm2, DC: 50 %, Duration: 10 s | Mice (f)/s.c. human ovarian cancer (SKOV3) | 70–100 | 22 (TIm); 8 (TrS) | 95 VIR | 67 VIR | Simultaneous enrichment of oxygenation and selective delivery of drugs at the tumor site; efficacy: OPLMB > PLMB | [151] |
| 2. PTX loaded PFC-MB (PLMBs) | 81 VIR | 62 VIR | ||||||||
| MBs: DSPC|DPPC|DPPA (PFP) | DTX/ N/A | Non-FUS/ UTMD | Freq.: 300 KHz, Intens.: 2 W/cm2 | Rabbit (f, m)/ rabbit liver tumor (VX2) | ~450 | 22 (TIm); 8 (TrS) | 31 VIR | 9 VIR | Slight TV suppression (< 50% VIR) | [152] |
| MBs: DPPC|DPPA|DPPE-PEG2k (PFP) | HCPT/ 4 | LIFU/ UTMD | Freq.: 1 MHz, Intens.: 2 W/cm2 | Mice/s.c. murine hepatoma (H22) | ~50 | 15 (TIm); 8 (TrS) | 71 VIR | 48 VIR | MB formulation with high loading capacity for HCPT | [153] |
| MBs: DPPC|DPPG|DPPE-PEG2k (C3F8) | DOX/ N/A | LIFU/ UTMD | Freq.: 1.3 MHz; MI: 1.6 | Rat (m)/s.c. murine pancreas cancer (DSL6A) | N/A | 14 (TrS) | 70 VIR | 27 VIR | MB formulation with high loading capacity for DOX | [154] |
| LPs (MFL) + MBs: DMPC|DOTAP|DSPE-MPEG2k + SonoVue® | DTX/ 2 | FUS/ UTMD | Freq.: 1.1 MHz, Power: 20 W, PRF: 40 Hz; DC: 5% | Mice (f) /s.c. human breast cancer (MDA-MB-231) | ~150 | 28 (TrS) | (+) MBs 55 VIR | (-) MBs 33 VIR | MFLs did fuse well onto cell membrane for intracellular drug delivery; MB + FUS led to sonoporation of vascular cells and to enhanced EPR effect | [150] |
| LPs (TSLs): DPPC|DSPE-PEG2k|MPPC-CuDOX | DOX/ 6 | FUS/HT | US pulses consisted of 100-cycle bursts at 1.54 MHz, PRF: 100 Hz–5kHz, HT: 42 °C, 5 min prior to NP injection and 20 min after | Mice/murine NDL breast cancer | ≥ 30 | 28 (TrS) | 100 TVR | pH-sensitive complex between DOX and copper (CuDOX); remains associated at neutral pH, but dissociates and releases free DOX in lower-pH environments | [145] | |
| LPs (HTSCs): CFL|DPPC|MSPC|DSPE-PEG2k | HDOX/ 5 | HIFU | DC: 30%, Voltage: 190 mV for 5 min twice: immediately and 24 h after injection, 42 °C | Mice (f)/s.c. human breast cancer (MDA-MB-231) | ~106 | 16 (TrS) | 96 TVR | 70 TVR | HTSCs with high physiological stability and tunable release characteristics, by introducing LTSLs lipid components into cerasomes | [146] |
| LP-MB complex: 1. LPs.: DPPC|DSPE-PEG2k-biotin|CHOL; 2. MBs: DSPC|DSPE-PEG2000| DSPE-PEG2000-Biotins (C3F8); 3. Avidin-bridge | PTX/ N/A | FUS | Burst length: 10 ms, DC: 1%, PRF: 1 Hz, Duration: 10 min | Mice (f)/s.c. murine breast cancer (4T1) | 65–270 | 21 (TIm); 11 (TrS) | 71 VIR | 29 VIR | Increased apoptosis and reduced angiogenesis achieved | [155] |
| LPs + MBs: 1. LPs: Doxil®; 2. MBs: DPPA|DPPC|DPPE-PEG2k|Glyc. (C3F8) | DOX/ 10 | LIFU/ UTMD | Freq.: 1.1 MHz, Intens.: 2.06 W/cm2, MI: 0.48 | Mice (f)/s.c. murine hepatoma (H22) | N/A | 20 (TIm); 16 (TrS) | 80 VIR | 62 VIR | Effective and safe treatment combination of Doxil® and UTMD | [156] |
| 1. LPs (Doxil-like) + MBs: HSPC|CHOL|MPEG2000-DSPE + SonoVueTM | DOX/ 6 | LIFU/ UTMD | Freq.: 1 MHz, MI: 0.8, pulses with 10 000 cycles | Mice (f)/s.c. human prostatic cancer (PC3) | 100–200 | 28 (TrS) | (+) MBs 58 VIR | (-) MBs 17 VIR | PEG cleavage of coated LPs by MMP enzymes led to increased intracellular uptake compared to NES- LPs, but VIR: Doxil-like > ES > NES | [157] |
| 2. LPs (enzyme sensitive, ES) + MBs: POPC|CHOL|PCL + SonoVueTM | (+) MBs 39 VIR | (-) MBs 6 VIR | ||||||||
| 3. LPs (non enzyme sensitive, NES) + MBs: POPC|CHOL|MPEG2000-CHOL + SonoVueTM | (+) MBs 21 VIR | (-) MBs 12 VIR | ||||||||
| LP-MB complex 1. LPs (OX): CHOL|DPPC|DSPE-PEG2k-biotin; 2. MBs (IR): DBPC| DSPE-PEG2k, DSPE-PEG2k-biotin (PFB); 3. Avidin bridge | OX/ ~1; IR/ ~ 5 | LIUS/ UTMD | Freq.: 1 MHz, Intens.: 3.5 W/cm2, DC: 30%, PRF: 100 Hz, PNP: 0.48 Mpa, MI: 0.48 | Mice (f)/s.c. human pancreatic cancer (BxPC-3) | ~100 | 14 (TrS) | 90 VIR | 44 VIR | Dual drug loading (OX loaded LPs, IR loaded MBs) | [110] |
| LPs: Caelyx® | DOX/ 1 | LFUS | Freq.: 20 kHz, continuous wave, Intens.: > 3.16 W/m² | Mice/s.c. human colon cancer (WiDr) | N/A | 21 (TrS) | 56 VIR | 47 VIR | Non-hyperthermic US treatment shows significant effect on tumor growth; occurrence of synergistic effects between US and drugs at lower concentrations | [158] |
| DOX/ 6 | 72 VIR | 72 VIR | ||||||||
| Micelles: Plurogel (Pluronic P105 stabilized with NNDEA) | 5-FU/ 100 | LFUS | Freq.: 20 kHz, continuous wave, Intens.: >3.16 W/m² | Mice/s.c. human colon cancer (WiDr) | N/A | 21 (TrS) | 33 VIR | 16 VIR | ||
| 5-FU/ 200 | 49 VIR | 49 VIR | ||||||||
| Micelles: Plurogel (Pluronic P105 stabilized with NNDEA) | DOX/ 2.7 | LFUS | Freq.: 70 kHz, Intens.: 2 W/cm2 Power train: 1:10 pulse (0.2 s on, 1.8 s off) | Rat/s.c. rat colon cancer (DHD/K12/TRb) | N/A | ~49 (TrS) | 96 VIR, partly TVR | 76 VIR | Probably 3 synergistic US effects occurred: 1. micelle extravasation ↑, 2. DOX release, 3. intracellular drug uptake ↑ | [130] |
| Micelles: Pluronic® P-105 with PEG2k-DSPE | DOX/ 3 | Non-FUS | Freq.: 1 MHz, Intens.: 3.4 W/cm2, DC: 50 %, Duration: 30 s | Mice (f)/s.c. human ovarian cancer (A2780) | 75–125 | 21 (TrS) | 90 VIR | 80 VIR | Stabilization of Pluronic® P-105 micelles with PEG2000-DSPE; high drug-loading capacity; no enhancement of micelle extravasation by US, but intracellular drug uptake ↑ | [159] |
| Synthetic polymer NP-MB complex: 1. NP: PLGA; 2. MB: DPPC|DSPE-PEG-NH2|PLL|Glyc (C3F8) | DOX/ N/A | LIFU/ UTMD | Freq.: 1 MHz, Intens.: 1.2 w/cm2, DC: 50%, Duration: 60 s | Rabbit/ rabbit liver tumor (VX2) | N/A | 26 (TIm); 11 (TrS) | 57 VIR | N/A | Targeted destruction of MBs by LIFU was superior in comparison to non-FUS | [160] |
| Non- FUS: 43 VIR | ||||||||||
| MBs stabilized by polymeric NP: PEG-PEBCA (C3F8) | CTX/ 10 | FUS | Burst length: 10 ms, DC: 2.5%, PRF: 0.5 Hz, Duration: 2 min. MI: 0.5 | Mice (f)/s.c. human breast cancer (MDA-MB-231) | 20–30 | 43 (TIm); 22 (TrS) | 100 TVR | 83 VIR | Lower acoustic pressures (MI of 0.1 or 0.25) did not enhance tumor uptake of NPs, tissue damage observed at MI of 1 | [147] |
| Synthetic polymer NPs + MBs: MPEG-PLGA-PLL–anti CA19-9 + SonoVue® | PTX/ 2 | LIFU/ UTMD | Freq.: 1 MHz, Intens.: 2 W/cm2, DC: 20 %, Duration: 2 min | Mice (m)/s.c. human pancreatic adeno-carcinoma (Capan-1) | 50–100 | 31 (TIm); 21 (TrS) | (+) MBs 91 VIR | (-) MBs 83 VIR | Ab-mediated active targeting | [161] |
| Phase-transformation lipid NPs: DPPG|DPPC|CHOL|DSPE-PEG3.4k-tLyP-1 (PFP) | HCPT/ N/A | LIFU/ ADV, UTMD | Freq.: 1 MHz, Intens.: 3.2 W/cm2, Duration: 1 s with a 1 s pause for a total of 3 min | Mice (f)/s.c. human breast cancer (MDA-MB-231) | 100 | 14 (TrS) | 67 VIR | 40 VIR | tLyP-1 peptide with targeting and penetrating efficiency; synergistic effects of ADV and UTMD, enhanced imaging through MB formation | [148] |
| Phase-transformation lipid NPs: PFP|DPPC| DC-CHOL| DSPE-CPPs|HA | HCPT/ 4 | LIFU/ ADV, UTMD | Intens.: 3.2 W/cm2, DC: 50 %, Duration: 2 min | Mice/s.c. human hepatoma (SMMC-7721) | ~512 | 31 (TIm); 11 (TrS) | 95 VIR | 79 VIR | CPPs/HA with targeting and penetrating efficiency; synergistic effects of ADV and UTMD, enhanced imaging through MB formation | [162] |
| Phase-changeable NDs: 1. FA-modified lipid shell (PL, CHOL) 2. Fe3O4 3. PFP core | HCPT/ 4 | LIFU/ ADV, UTMD | Intens.: 3.2 W/cm², pulsed-wave mode | Mice (f)/s.c. human ovarian cancer (SKOV3) | 400–500 (d = 2) | 14 (TrS) | 74 VIR | 52 VIR | Ligand (FA)-mediated active targeting, synergistic effects of ADV and UTMD, multimodal tumor imaging (MRI, PAI) | [163] |
| MD-MB cluster: 1. MDs: PFMCP| DSPC 2. MBs: Sonazoid® | PTX/ 15 | FUS/ ACT | Activation: Freq.: 1.5 MHz, PRF: 26.1 Hz DC: 0.18 %, MI: 0.44, Duration: 45 s; Treatment: Freq.: 0.3 MHz, PRF: 100 Hz DC: 7.28 %, MI: 0.1, Duration: 300 s | Mice (m)/s.c. human pancreatic ductal adenocarcinoma (PDAC) (MIA PaCa-2luc) | 50–80 (AV: ~53) | 45 (TIm); 31 (TrS) | ACT-PTX: 86 VIR, partly TVR | PTX: 72 VIR | Two frequencies required: treatment efficiency also dependent on activation efficiency | [164] |
| MSN encapsuled in MBs: 1. NPs: MSN-folate 2. MBs: DPPC|DPPE|Glyc. (C3F8) | TAN/ 8 | LIUS/ UTMD | Freq.: 1 MHz, Intens.: 2 W/cm2 | Mice (m)/s.c. murine hepatoma (H22) | ~150 (d = 3) | 8 (TrS) | 64 VIR | 43 VIR | High drug loading capacity, multitargeting capability | [165] |
| MSN: MSN-Ce6 | DOX/ 3 | FUS/SDT+NP | 4 W/cm2 | Mice (f)/s.c. human breast cancer (MDA-MB-231) | N/A | 9 (TrS) | MSN-DOX-Ce6: 88 VIR | N/A | Synergistic effects of SDT and DDS (may be enhanced by introducing targeting molecules); high drug-loading properties | [149] |
| DOX+ Ce6: 62 VIR | ||||||||||
8. Toxicological and Biosafety Considerations
9. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 5-FU | 5-fluorouracil |
| Ab | Antibody |
| ACT | Acoustic cluster therapy |
| ADME | Absorption, distribution, metabolism and excretion/elimination |
| ADV | Acoustic droplet vaporization |
| AV | Average; C3F8, Perfluoropropane; Ce6, chlorin e6 (sonosensitizer) |
| BL | Bilayer |
| CFL | Cerasome-forming lipid |
| CHOL | Cholesterol |
| CPP | Cell penetrating peptide |
| CPT | Camptothecin |
| CTX | Cabacitaxel |
| DC | Duty cycle (effective ultrasound emission rate) |
| DC-CHOL | 3-(N-(N’,N’-Dimethylaminoethane) carbamoyl) cholesterol |
| DMPC | 1,2-dimyristoyl-sn-glycero-3-phosphocholine |
| DOTAP | 1,2-dioleoyl-3-trimethylammonium-propane |
| DPPA | 1,2-dipalmitoyl-sn-glycero-3-phosphatidic acid |
| DPPC | 1,2-dipalmitoyl-sn-glycero-3-phosphocholine |
| DPPE | 1,2-dipalmitoyl-sn-glycero-3-phosphoethanolamine |
| DTX | Docetaxel |
| ECM | Extracellular matrix |
| EPR | Enhanced permeation and retention |
| ES | Enzyme sensitive |
| FA | Folic acid |
| FUS | Focused ultrasound |
| Glyc | Glycerol |
| HA | Hyaluronic acid |
| HCPT | 10-hydroxycampthothecin |
| HDOX | Hydrophilic doxorubicin hydrochloride |
| HIFU | High-intensity focused US |
| HT | Hyperthermia |
| HTSC | HIFU and temperature-sensitive cerasome |
| IR | Irinotecan |
| ISO | International Organization for Standardization |
| LFUS | Low frequency ultrasound |
| LIFU | Low-intensity focused US |
| LIUS | Low-intensity ultrasound |
| LP | Liposome |
| LTSL | Low temperature sensitive liposomes |
| MB | Microbubble |
| MD | Microdroplet |
| MFL | Membrane fusogenic liposome |
| MI | Mechanical index |
| MMP | Matrix metalloprotease |
| MPEG2k | Methoxy polyethylene glycol 2000 |
| MPPC | 1-palmitoyl-2-hydroxy-sn-glycero-3-phosphocholine |
| MPS | Mononuclear phagocyte system |
| MRI | Magnetic resonance imaging |
| MS | Microstreaming |
| MSN | Mesoporous silica nanoparticle |
| MSPC | Monostearoylphosphatidylcholine |
| NDL | Neu deletion |
| NES | Non enzyme sensitive |
| NNDEA | N,N-diethylacrylamide |
| NP | Nanoparticle |
| OPLMB | Oxygen and paclitaxel loaded microbubbles |
| OX | Oxaliplatin |
| PAI | Photoacoustic imaging |
| PCL | PEGylated cleavable lipopeptide |
| PDAC | Pancreatic ductal adenocarcinoma |
| PEBCA | Poly-2-ethyl-butyl cyanoacrylate |
| PEG | Polyethylene glycol |
| PEG2k | Polyethylene glycol 2000 |
| PEO | Polyethylene oxide |
| PFB | Perfluorbutane |
| PFC | Perfluorocarbon |
| PFMCP | Perfluoromethylcyclopentane |
| PFP | Perfluoropentane |
| PL | Phospholipid |
| PLA | Polylactic acid |
| PLGA | Poly-d,-l-lactic glycolic acid |
| PLL | Poly-l-lysine |
| PLMB | Paclitaxel loaded microbubbles |
| PNP | Peak-negative pressure |
| POPC | 1-palmitoyl-2-oleoyl-sn-glycero-3-phosphocholine |
| PPO | Polypropylene oxide |
| PRF | Pulse repetition frequency |
| PRP | Pulse repetition period |
| PTX | Paclitaxel |
| RES | Reticuloendothelial system |
| RF | Radiation forces |
| ROS | Reactive oxygen species |
| s. c. | Subcutaneous |
| SDDS | Smart drug delivery systems |
| SDT | Sonodynamic therapy |
| TAN | Tanshinone IIA |
| TI | Thermal index |
| TIm | Tumor implantation |
| tLyP-1 | Tumor homing-penetrating peptide |
| TR | Technical report |
| TS | Technical specification |
| TrS | Treatment start |
| TSL | Thermosensitive liposome |
| TV | Tumor volume |
| TVR | Tumor volume reduction |
| UCA | Ultrasound contrast agent |
| US | Ultrasound |
| UTMD | Ultrasound targeted microbubble destruction |
| VIR | Volume inhibition rate |
| VSSA | Volume specific surface area |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.-Y.; Cheng, R.; Yang, Z.; Tian, Z.-M. Nanotechnology for Cancer Therapy Based on Chemotherapy. Molecules 2018, 23, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisso, S.; Leroux, J.-C. Nanopharmaceuticals: A focus on their clinical translatability. Int. J. Pharm. 2020, 578, 119098. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Maeda, H. A new concept for macromolecular therapeutics in cancer chemotherapy: Mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986, 46, 6387–6392. [Google Scholar] [PubMed]
- Danhier, F. To exploit the tumor microenvironment: Since the EPR effect fails in the clinic, what is the future of nanomedicine? J. Control. Release 2016, 244, 108–121. [Google Scholar] [CrossRef]
- Peer, D.; Karp, J.M.; Hong, S.; Farokhzad, O.C.; Margalit, R.; Langer, R. Nanocarriers as an emerging platform for cancer therapy. Nat. Nanotechnol. 2007, 2, 751–760. [Google Scholar] [CrossRef]
- Sharker, S.M.; Lee, J.E.; Kim, S.H.; Jeong, J.H.; In, I.; Lee, H.; Park, S.Y. pH triggered in vivo photothermal therapy and fluorescence nanoplatform of cancer based on responsive polymer-indocyanine green integrated reduced graphene oxide. Biomaterials 2015, 61, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, S.; Tavares, A.J.; Dai, Q.; Ohta, S.; Audet, J.; Dvorak, H.F.; Chan, W.C.W. Analysis of nanoparticle delivery to tumours. Nat. Rev. Mater. 2016, 1. [Google Scholar] [CrossRef]
- Rajabi, M.; Srinivasan, M.; Mousa, S.A. Nanobiomaterials in drug delivery. In Nanobiomaterials in Drug Delivery; Grumezescu, A.M., Ed.; WA William Andrew an Imprint of Elsevier: Amsterdam, The Netherlands; Boston, MA, USA; Heidelberg, Germany, 2016; pp. 1–37. ISBN 9780323428668. [Google Scholar]
- Jain, K.K. Role of Nanobiotechnology in Drug Delivery. Methods Mol. Biol. 2020, 2059, 55–73. [Google Scholar] [CrossRef] [PubMed]
- Wolfram, J.; Ferrari, M. Clinical Cancer Nanomedicine. Nano Today 2019, 25, 85–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osei, E.; Al-Asady, A. A review of ultrasound-mediated microbubbles technology for cancer therapy: A vehicle for chemotherapeutic drug delivery. J. Radiother. Pract. 2019, 19, 291–298. [Google Scholar] [CrossRef]
- Hossen, S.; Hossain, M.K.; Basher, M.K.; Mia, M.N.H.; Rahman, M.T.; Uddin, M.J. Smart nanocarrier-based drug delivery systems for cancer therapy and toxicity studies: A review. J. Adv. Res. 2019, 15, 1–18. [Google Scholar] [CrossRef]
- Boissenot, T.; Bordat, A.; Fattal, E.; Tsapis, N. Ultrasound-triggered drug delivery for cancer treatment using drug delivery systems: From theoretical considerations to practical applications. J. Control. Release 2016, 241, 144–163. [Google Scholar] [CrossRef] [PubMed]
- Draper, D.O.; Castel, J.C.; Castel, D. Rate of temperature increase in human muscle during 1 MHz and 3 MHz continuous ultrasound. J. Orthop. Sports Phys. Ther. 1995, 22, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Rassweiler, J.J.; Knoll, T.; Köhrmann, K.-U.; McAteer, J.A.; Lingeman, J.E.; Cleveland, R.O.; Bailey, M.R.; Chaussy, C. Shock wave technology and application: An update. Eur. Urol. 2011, 59, 784–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Ratnayaka, S.; Alford, A.; Kozlovskaya, V.; Liu, F.; Xue, B.; Hoyt, K.; Kharlampieva, E. Theranostic Multilayer Capsules for Ultrasound Imaging and Guided Drug Delivery. ACS Nano 2017, 11, 3135–3146. [Google Scholar] [CrossRef] [Green Version]
- Pitt, W.G.; Husseini, G.A.; Staples, B.J. Ultrasonic drug delivery—A general review. Expert Opin. Drug Deliv. 2004, 1, 37–56. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, A.; Kost, J.; Barenholz, Y. Ultrasound, liposomes, and drug delivery: Principles for using ultrasound to control the release of drugs from liposomes. Chem. Phys. Lipids 2009, 162, 1–16. [Google Scholar] [CrossRef]
- Coltrera, M.D. Ultrasound physics in a nutshell. Otolaryngol. Clin. N. Am. 2010, 43, 1149–1159. [Google Scholar] [CrossRef]
- Shriki, J. Ultrasound physics. Crit. Care Clin. 2014, 30, 1–24. [Google Scholar] [CrossRef]
- Leisure, R.G. Acoustic Waves in Solids. In Ultrasonic Spectroscopy: Applications in Condensed Matter Physics and Materials Science; Leisure, R.G., Ed.; Cambridge University Press: Cambridge, UK, 2017; pp. 56–93. ISBN 9781316658901. [Google Scholar]
- Karshafian, R.; Bevan, P.D.; Williams, R.; Samac, S.; Burns, P.N. Sonoporation by ultrasound-activated microbubble contrast agents: Effect of acoustic exposure parameters on cell membrane permeability and cell viability. Ultrasound Med. Biol. 2009, 35, 847–860. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Meng, W.; Ren, Z.; Li, B.; Zhu, T.; Chen, H.; Wang, Z.; He, B.; Zhao, D.; Jiang, H. Ultrasonic Neuromodulation and Sonogenetics: A New Era for Neural Modulation. Front. Physiol. 2020, 11, 787. [Google Scholar] [CrossRef]
- Timko, B.P.; Dvir, T.; Kohane, D.S. Remotely triggerable drug delivery systems. Adv. Mater. 2010, 22, 4925–4943. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, F.; McLoughlin, I.V.; Chauhan, S.; ter-Haar, G. Bio-effects and safety of low-intensity, low-frequency ultrasonic exposure. Prog. Biophys. Mol. Biol. 2012, 108, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Mitragotri, S. Healing sound: The use of ultrasound in drug delivery and other therapeutic applications. Nat. Rev. Drug Discov. 2005, 4, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, J.E. Basic physics of ultrasound imaging. Crit. Care Med. 2007, 35, S131–S137. [Google Scholar] [CrossRef] [PubMed]
- Kossoff, G. Basic physics and imaging characteristics of ultrasound. World J. Surg. 2000, 24, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Tharkar, P.; Varanasi, R.; Wong, W.S.F.; Jin, C.T.; Chrzanowski, W. Nano-Enhanced Drug Delivery and Therapeutic Ultrasound for Cancer Treatment and Beyond. Front. Bioeng. Biotechnol. 2019, 7, 324. [Google Scholar] [CrossRef] [Green Version]
- Van den Bijgaart, R.J.E.; Eikelenboom, D.C.; Hoogenboom, M.; Fütterer, J.J.; den Brok, M.H.; Adema, G.J. Thermal and mechanical high-intensity focused ultrasound: Perspectives on tumor ablation, immune effects and combination strategies. Cancer Immunol. Immunother. 2017, 66, 247–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, J.E.; ter Haar, G.R.; Cranston, D. High intensity focused ultrasound: Surgery of the future? Br. J. Radiol. 2003, 76, 590–599. [Google Scholar] [CrossRef]
- Escoffre, J.-M.; Novell, A.; de Smet, M.; Bouakaz, A. Focused ultrasound mediated drug delivery from temperature-sensitive liposomes: In-vitro characterization and validation. Phys. Med. Biol. 2013, 58, 8135–8151. [Google Scholar] [CrossRef]
- Beik, J.; Mehdizadeh, A.R.; Shakeri-Zadeh, A. Ultrasound in Cancer Treatment through Nanotechnology. J. Biomed. Phys. Eng. 2016, 6, 123–126. [Google Scholar]
- Zheng, T.; Chen, Y.; Peng, J.; Shi, Y.; Zhang, J.; Xiao, H.; Chen, X.; Huang, Y.; Pei, T.; Zhang, Z.; et al. A Perspective of Ultrasound-Related Micro/Nano Cancer Therapy. In Nanoparticle Drug Delivery Systems for Cancer Treatment; Jenny Stanford Publishing: Singapore, 2020; pp. 143–184. [Google Scholar]
- Dewey, W.C. Arrhenius relationships from the molecule and cell to the clinic. Int. J. Hyperth. 2009, 25, 3–20. [Google Scholar] [CrossRef]
- Gelet, A.; Chapelon, J.Y.; Poissonnier, L.; Bouvier, R.; Rouvière, O.; Curiel, L.; Janier, M.; Vallancien, G. Local recurrence of prostate cancer after external beam radiotherapy: Early experience of salvage therapy using high-intensity focused ultrasonography. Urology 2004, 63, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Song, C.W.; Kang, M.S.; Rhee, J.G.; Levitt, S.H. Effect of hyperthermia on vascular function in normal and neoplastic tissues. Ann. N. Y. Acad. Sci. 1980, 335, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Roti Roti, J.L. Cellular responses to hyperthermia (40–46 °C): Cell killing and molecular events. Int. J. Hypothermia 2008, 24, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Landon, C.D.; Park, J.-Y.; Needham, D.; Dewhirst, M.W. Nanoscale Drug Delivery and Hyperthermia: The Materials Design and Preclinical and Clinical Testing of Low Temperature-Sensitive Liposomes Used in Combination with Mild Hyperthermia in the Treatment of Local Cancer. Open Nanomed. J. 2011, 3, 38–64. [Google Scholar] [CrossRef]
- Rosenthal, I.; Sostaric, J.Z.; Riesz, P. Sonodynamic therapy--a review of the synergistic effects of drugs and ultrasound. Ultrason. Sonochem. 2004, 11, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Larina, I.V.; Evers, B.M.; Ashitkov, T.V.; Bartels, C.; Larin, K.V.; Esenaliev, R.O. Enhancement of drug delivery in tumors by using interaction of nanoparticles with ultrasound radiation. Technol. Cancer Res. Treat. 2005, 4, 217–226. [Google Scholar] [CrossRef] [Green Version]
- Husseini, G.A.; La Diaz de Rosa, M.A.; Richardson, E.S.; Christensen, D.A.; Pitt, W.G. The role of cavitation in acoustically activated drug delivery. J. Control. Release 2005, 107, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Husseini, G.A.; Pitt, W.G.; Martins, A.M. Ultrasonically triggered drug delivery: Breaking the barrier. Colloids Surf. B Biointerfaces 2014, 123, 364–386. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, V.; Kimmel, E.; Iger, Y. Ultrasound-induced intercellular space widening in fish epidermis. Ultrasound Med. Biol. 2000, 26, 473–480. [Google Scholar] [CrossRef]
- Hancock, H.A.; Smith, L.H.; Cuesta, J.; Durrani, A.K.; Angstadt, M.; Palmeri, M.L.; Kimmel, E.; Frenkel, V. Investigations into pulsed high-intensity focused ultrasound-enhanced delivery: Preliminary evidence for a novel mechanism. Ultrasound Med. Biol. 2009, 35, 1722–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, P.E.; Jenne, J.W.; Rastert, R.; Simiantonakis, I.; Sinn, H.P.; Strittmatter, H.J.; von Fournier, D.; Wannenmacher, M.F.; Debus, J. A new noninvasive approach in breast cancer therapy using magnetic resonance imaging-guided focused ultrasound surgery. Cancer Res. 2001, 61, 8441–8447. [Google Scholar]
- Arvanitis, C.D.; Bazan-Peregrino, M.; Rifai, B.; Seymour, L.W.; Coussios, C.C. Cavitation-enhanced extravasation for drug delivery. Ultrasound Med. Biol. 2011, 37, 1838–1852. [Google Scholar] [CrossRef]
- Mullick Chowdhury, S.; Lee, T.; Willmann, J.K. Ultrasound-guided drug delivery in cancer. Ultrasonography 2017, 36, 171–184. [Google Scholar] [CrossRef] [Green Version]
- Brennen, C.E. Cavitation and Bubble Dynamics; Oxford University Press: New York, NY, USA, 1995; ISBN 0195094093. [Google Scholar]
- Izadifar, Z.; Babyn, P.; Chapman, D. Ultrasound Cavitation/Microbubble Detection and Medical Applications. J. Med. Biol. Eng. 2019, 39, 259–276. [Google Scholar] [CrossRef]
- Mayer, C.R.; Geis, N.A.; Katus, H.A.; Bekeredjian, R. Ultrasound targeted microbubble destruction for drug and gene delivery. Expert Opin. Drug Deliv. 2008, 5, 1121–1138. [Google Scholar] [CrossRef] [PubMed]
- Cintas, P.; Tagliapietra, S.; Caporaso, M.; Tabasso, S.; Cravotto, G. Enabling technologies built on a sonochemical platform: Challenges and opportunities. Ultrason. Sonochem. 2015, 25, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hervouet, E.; Simonnet, H.; Godinot, C. Mitochondria and reactive oxygen species in renal cancer. Biochimie 2007, 89, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhang, Y.; Cai, C.; Tu, J.; Guo, X.; Zhang, D. Sonoporation-induced cell membrane permeabilization and cytoskeleton disassembly at varied acoustic and microbubble-cell parameters. Sci. Rep. 2018, 8, 3885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibaguchi, H.; Tsuru, H.; Kuroki, M.; Kuroki, M. Sonodynamic cancer therapy: A non-invasive and repeatable approach using low-intensity ultrasound with a sonosensitizer. Anticancer Res. 2011, 31, 2425–2429. [Google Scholar]
- Lee, J.Y.; Carugo, D.; Crake, C.; Owen, J.; de Saint Victor, M.; Seth, A.; Coussios, C.; Stride, E. Nanoparticle-Loaded Protein-Polymer Nanodroplets for Improved Stability and Conversion Efficiency in Ultrasound Imaging and Drug Delivery. Adv. Mater. 2015, 27, 5484–5492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, J.J.; Graham, S.; Myers, R.; Carlisle, R.; Stride, E.; Coussios, C.C. Ultrasound-induced inertial cavitation from gas-stabilizing nanoparticles. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 2015, 92, 23019. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J.J.; Myers, R.; Coviello, C.M.; Graham, S.M.; Shah, A.R.; Stride, E.; Carlisle, R.C.; Coussios, C.C. Ultrasound-Propelled Nanocups for Drug Delivery. Small 2015, 11, 5305–5314. [Google Scholar] [CrossRef] [Green Version]
- Juffermans, L.J.M.; Dijkmans, P.A.; Musters, R.J.P.; Visser, C.A.; Kamp, O. Transient permeabilization of cell membranes by ultrasound-exposed microbubbles is related to formation of hydrogen peroxide. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H1595–H1601. [Google Scholar] [CrossRef]
- Hassan, M.A.; Campbell, P.; Kondo, T. The role of Ca(2+) in ultrasound-elicited bioeffects: Progress, perspectives and prospects. Drug Discov. Today 2010, 15, 892–906. [Google Scholar] [CrossRef]
- Yang, C.; Li, Y.; Du, M.; Chen, Z. Recent advances in ultrasound-triggered therapy. J. Drug Target. 2019, 27, 33–50. [Google Scholar] [CrossRef]
- Schweizer, F.E.; Ryan, T.A. The synaptic vesicle: Cycle of exocytosis and endocytosis. Curr. Opin. Neurobiol. 2006, 16, 298–304. [Google Scholar] [CrossRef]
- Wang, S.; Shin, I.S.; Hancock, H.; Jang, B.; Kim, H.; Lee, S.M.; Zderic, V.; Frenkel, V.; Pastan, I.; Paik, C.H.; et al. Pulsed high intensity focused ultrasound increases penetration and therapeutic efficacy of monoclonal antibodies in murine xenograft tumors. J. Control. Release 2012, 162, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Krasovitski, B.; Frenkel, V.; Shoham, S.; Kimmel, E. Intramembrane cavitation as a unifying mechanism for ultrasound-induced bioeffects. Proc. Natl. Acad. Sci. USA 2011, 108, 3258–3263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Giacinto, F.; de Spirito, M.; Maulucci, G. Low-Intensity Ultrasound Induces Thermodynamic Phase Separation of Cell Membranes through a Nucleation-Condensation Process. Ultrasound Med. Biol. 2019, 45, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, P.; Phillips, R. Analytic models for mechanotransduction: Gating a mechanosensitive channel. Proc. Natl. Acad. Sci. USA 2004, 101, 4071–4076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solans, R.; Motta, C.; Solá, R.; La Ville, A.E.; Lima, J.; Simeón, P.; Montellà, N.; Armadans-Gil, L.; Fonollosa, V.; Vilardell, M. Abnormalities of erythrocyte membrane fluidity, lipid composition, and lipid peroxidation in systemic sclerosis: Evidence of free radical-mediated injury. Arthritis Rheum. 2000, 43, 894–900. [Google Scholar] [CrossRef]
- Paris, J.L.; Vallet-Regí, M. Ultrasound-Activated Nanomaterials for Therapeutics. Bull. Chem. Soc. Jpn. 2020, 93, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Kong, G.; Braun, R.D.; Dewhirst, M.W. Hyperthermia enables tumor-specific nanoparticle delivery: Effect of particle size. Cancer Res. 2000, 60, 4440–4445. [Google Scholar] [PubMed]
- Kong, G.; Braun, R.D.; Dewhirst, M.W. Characterization of the effect of hyperthermia on nanoparticle extravasation from tumor vasculature. Cancer Res. 2001, 61, 3027–3032. [Google Scholar] [PubMed]
- Wischhusen, J.; Padilla, F. Ultrasound-Targeted Microbubble Destruction (UTMD) for Localized Drug Delivery into Tumor Tissue. IRBM 2019, 40, 10–15. [Google Scholar] [CrossRef]
- de Cock, I.; Lajoinie, G.; Versluis, M.; de Smedt, S.C.; Lentacker, I. Sonoprinting and the importance of microbubble loading for the ultrasound mediated cellular delivery of nanoparticles. Biomaterials 2016, 83, 294–307. [Google Scholar] [CrossRef]
- Sontum, P.; Kvåle, S.; Healey, A.J.; Skurtveit, R.; Watanabe, R.; Matsumura, M.; Østensen, J. Acoustic Cluster Therapy (ACT)—A novel concept for ultrasound mediated, targeted drug delivery. Int. J. Pharm. 2015, 495, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.-K.; Shen, E.; Hu, B. The induction of the apoptosis of cancer cell by sonodynamic therapy: A review. Chin. J. Cancer Res. 2012, 24, 368–373. [Google Scholar] [CrossRef]
- Fabiilli, M.L.; Haworth, K.J.; Fakhri, N.H.; Kripfgans, O.D.; Carson, P.L.; Fowlkes, J.B. The role of inertial cavitation in acoustic droplet vaporization. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2009, 56, 1006–1017. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, N.Y.; Kennedy, A.M.; Shea, J.E.; Scaife, C.L.; Nam, K.-H. Controlled and targeted tumor chemotherapy by ultrasound-activated nanoemulsions/microbubbles. J. Control. Release 2009, 138, 268–276. [Google Scholar] [CrossRef] [Green Version]
- Ho, Y.-J.; Yeh, C.-K. Concurrent anti-vascular therapy and chemotherapy in solid tumors using drug-loaded acoustic nanodroplet vaporization. Acta Biomater. 2017, 49, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Kripfgans, O.D.; Fowlkes, J.B.; Miller, D.L.; Eldevik, O.P.; Carson, P.L. Acoustic droplet vaporization for therapeutic and diagnostic applications. Ultrasound Med. Biol. 2000, 26, 1177–1189. [Google Scholar] [CrossRef]
- Petersen, A.L.; Hansen, A.E.; Gabizon, A.; Andresen, T.L. Liposome imaging agents in personalized medicine. Adv. Drug Deliv. Rev. 2012, 64, 1417–1435. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.I.; Kwon, Y.-S.; Cho, H.-S.; Heo, S.-H.; Park, K.S.; Park, S.G.; Lee, S.-H.; Hwang, S.I.; Kim, Y.I.; Jae, H.J.; et al. Ultrasound-mediated gene and drug delivery using a microbubble-liposome particle system. Theranostics 2014, 4, 1133–1144. [Google Scholar] [CrossRef] [Green Version]
- Zununi Vahed, S.; Salehi, R.; Davaran, S.; Sharifi, S. Liposome-based drug co-delivery systems in cancer cells. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 71, 1327–1341. [Google Scholar] [CrossRef]
- Wang, S.; Huang, P.; Chen, X. Hierarchical Targeting Strategy for Enhanced Tumor Tissue Accumulation/Retention and Cellular Internalization. Adv. Mater. 2016, 28, 7340–7364. [Google Scholar] [CrossRef] [Green Version]
- Thanou, M. (Ed.) Theranostics and Image Guided Drug Delivery; Royal Society of Chemistry: Cambridge, UK, 2018; ISBN 9781788010597. [Google Scholar]
- FILAB. ISO/TR 10993-22. Biological Evaluation of Medical Devices—Part 22: Guidance on Nanomaterials; FILAB: Dijon, France, 2017. [Google Scholar]
- Bregoli, L.; Movia, D.; Gavigan-Imedio, J.D.; Lysaght, J.; Reynolds, J.; Prina-Mello, A. Nanomedicine applied to translational oncology: A future perspective on cancer treatment. Nanomedicine 2016, 12, 81–103. [Google Scholar] [CrossRef] [Green Version]
- Sztandera, K.; Gorzkiewicz, M.; Klajnert-Maculewicz, B. Gold Nanoparticles in Cancer Treatment. Mol. Pharm. 2019, 16, 1–23. [Google Scholar] [CrossRef]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat. Biotechnol. 2015, 33, 941–951. [Google Scholar] [CrossRef]
- Stylianopoulos, T.; Poh, M.-Z.; Insin, N.; Bawendi, M.G.; Fukumura, D.; Munn, L.L.; Jain, R.K. Diffusion of particles in the extracellular matrix: The effect of repulsive electrostatic interactions. Biophys. J. 2010, 99, 1342–1349. [Google Scholar] [CrossRef] [Green Version]
- Locatelli, E.; Comes Franchini, M. Biodegradable PLGA-b-PEG polymeric nanoparticles: Synthesis, properties, and nanomedical applications as drug delivery system. J. Nanopart. Res. 2012, 14, 1–17. [Google Scholar] [CrossRef]
- Fang, Y.; Xue, J.; Gao, S.; Lu, A.; Yang, D.; Jiang, H.; He, Y.; Shi, K. Cleavable PEGylation: A strategy for overcoming the “PEG dilemma” in efficient drug delivery. Drug Deliv. 2017, 24, 22–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, S.; DeGiovanni, P.-J.; Piel, B.; Rai, P. Cancer nanomedicine: A review of recent success in drug delivery. Clin. Transl. Med. 2017, 6, 44. [Google Scholar] [CrossRef] [Green Version]
- Nikam, A.P.; Ratnaparkhiand, M.P.; Chaudhari, S.P. Nanoparticles—An overview. Int. J. Res. Dev. Pharm. Life Sci. 2014, 3, 1121–1127. [Google Scholar]
- Li, L.; Yang, W.-W.; Xu, D.-G. Stimuli-responsive nanoscale drug delivery systems for cancer therapy. J. Drug Target. 2019, 27, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Pedziwiatr-Werbicka, E.; Horodecka, K.; Shcharbin, D.; Bryszewska, M. Nanoparticles in combating cancer: Opportunities and limitations. A brief review. Curr. Med. Chem. 2020, 28, 346–359. [Google Scholar] [CrossRef]
- Bamrungsap, S.; Zhao, Z.; Chen, T.; Wang, L.; Li, C.; Fu, T.; Tan, W. Nanotechnology in therapeutics: A focus on nanoparticles as a drug delivery system. Nanomedicine 2012, 7, 1253–1271. [Google Scholar] [CrossRef]
- Ahlawat, J.; Zubia, E.; Narayan, M. Nanoparticles in Cancer Treatment: Types and Preparation Methods. In Nanoparticle Drug Delivery Systems for Cancer Treatment; Gali-Muhtasib, H., Chouaib, R., Eds.; Pan Stanford Publishing: Singapore; Jenny Stanford Publishing: Singapore, 2019; pp. 23–43. ISBN 9780429341250. [Google Scholar]
- Song, G.; Petschauer, J.S.; Madden, A.J.; Zamboni, W.C. Nanoparticles and the mononuclear phagocyte system: Pharmacokinetics and applications for inflammatory diseases. Curr. Rheumatol. Rev. 2014, 10, 22–34. [Google Scholar] [CrossRef]
- Panyam, J.; Labhasetwar, V. Biodegradable nanoparticles for drug and gene delivery to cells and tissue. Adv. Drug Deliv. Rev. 2003, 55, 329–347. [Google Scholar] [CrossRef]
- Ahlawat, J.; Henriquez, G.; Narayan, M. Enhancing the Delivery of Chemotherapeutics: Role of Biodegradable Polymeric Nanoparticles. Molecules 2018, 23, 2157. [Google Scholar] [CrossRef] [Green Version]
- Pauwels, E.; Kairemo, K.; Erba, P.; Bergstrom, K. Nanoparticles in Cancer. Curr. Radiopharm. 2008, 1, 30–36. [Google Scholar] [CrossRef]
- Jia, Y.; Yuan, M.; Yuan, H.; Huang, X.; Sui, X.; Cui, X.; Tang, F.; Peng, J.; Chen, J.; Lu, S.; et al. Co-encapsulation of magnetic Fe3O4 nanoparticles and doxorubicin into biodegradable PLGA nanocarriers for intratumoral drug delivery. Int. J. Nanomed. 2012, 7, 1697–1708. [Google Scholar] [CrossRef] [Green Version]
- Sirsi, S.R.; Borden, M.A. State-of-the-art materials for ultrasound-triggered drug delivery. Adv. Drug Deliv. Rev. 2014, 72, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couture, O.; Foley, J.; Kassell, N.F.; Larrat, B.; Aubry, J.-F. Review of ultrasound mediated drug delivery for cancer treatment: Updates from pre-clinical studies. Transl. Cancer Res. 2014, 3, 494–511. [Google Scholar] [CrossRef]
- Kneidl, B.; Peller, M.; Winter, G.; Lindner, L.H.; Hossann, M. Thermosensitive liposomal drug delivery systems: State of the art review. Int. J. Nanomed. 2014, 9, 4387–4398. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.E.; Awad, N.; Paul, V.; Moussa, H.G.; Husseini, G.A. Improving the Efficacy of Anticancer Drugs via Encapsulation and Acoustic Release. Curr. Top. Med. Chem. 2018, 18, 857–880. [Google Scholar] [CrossRef]
- Nardecchia, S.; Sánchez-Moreno, P.; de Vicente, J.; Marchal, J.A.; Boulaiz, H. Clinical Trials of Thermosensitive Nanomaterials: An Overview. Nanomaterials 2019, 9, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daraee, H.; Etemadi, A.; Kouhi, M.; Alimirzalu, S.; Akbarzadeh, A. Application of liposomes in medicine and drug delivery. Artif. Cells Nanomed. Biotechnol. 2016, 44, 381–391. [Google Scholar] [CrossRef]
- Sun, T.; Zhang, Y.S.; Pang, B.; Hyun, D.C.; Yang, M.; Xia, Y. Engineered nanoparticles for drug delivery in cancer therapy. Angew. Chem. Int. Ed. Engl. 2014, 53, 12320–12364. [Google Scholar] [CrossRef]
- Gao, J.; Nesbitt, H.; Logan, K.; Burnett, K.; White, B.; Jack, I.G.; Taylor, M.A.; Love, M.; Callan, B.; McHale, A.P.; et al. An ultrasound responsive microbubble-liposome conjugate for targeted irinotecan-oxaliplatin treatment of pancreatic cancer. Eur. J. Pharm. Biopharm. 2020, 157, 233–240. [Google Scholar] [CrossRef]
- von Bibra, H.; Voigt, J.-U.; Fröman, M.; Bone, D.; Wranne, B.; Juhlin-Dannfeldt, A. Interaction of Microbubbles with Ultrasound. Echocardiography 1999, 16, 733–741. [Google Scholar] [CrossRef]
- de Jong, N.; Bouakaz, A.; Frinking, P. Basic acoustic properties of microbubbles. Echocardiography 2002, 19, 229–240. [Google Scholar] [CrossRef]
- Ibsen, S.; Schutt, C.E.; Esener, S. Microbubble-mediated ultrasound therapy: A review of its potential in cancer treatment. Drug Des. Devel. Ther. 2013, 7, 375–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernot, S.; Klibanov, A.L. Microbubbles in ultrasound-triggered drug and gene delivery. Adv. Drug Deliv. Rev. 2008, 60, 1153–1166. [Google Scholar] [CrossRef] [Green Version]
- Udroiu, I. Ultrasonic drug delivery in Oncology. J. BUON 2015, 20, 381–390. [Google Scholar]
- Tartis, M.S.; McCallan, J.; Lum, A.F.H.; LaBell, R.; Stieger, S.M.; Matsunaga, T.O.; Ferrara, K.W. Therapeutic effects of paclitaxel-containing ultrasound contrast agents. Ultrasound Med. Biol. 2006, 32, 1771–1780. [Google Scholar] [CrossRef]
- Fokong, S.; Theek, B.; Wu, Z.; Koczera, P.; Appold, L.; Jorge, S.; Resch-Genger, U.; van Zandvoort, M.; Storm, G.; Kiessling, F.; et al. Image-guided, targeted and triggered drug delivery to tumors using polymer-based microbubbles. J. Control. Release 2012, 163, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Mørch, Ý.; Hansen, R.; Berg, S.; Åslund, A.K.O.; Glomm, W.R.; Eggen, S.; Schmid, R.; Johnsen, H.; Kubowicz, S.; Snipstad, S.; et al. Nanoparticle-stabilized microbubbles for multimodal imaging and drug delivery. Contrast Media Mol. Imaging 2015, 10, 356–366. [Google Scholar] [CrossRef] [Green Version]
- Lv, Y.; Hao, L.; Hu, W.; Ran, Y.; Bai, Y.; Zhang, L. Novel multifunctional pH-sensitive nanoparticles loaded into microbubbles as drug delivery vehicles for enhanced tumor targeting. Sci. Rep. 2016, 6, 29321. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Chen, Y.; Yu, T.; Guo, Y.; Liu, F.; Yao, Y.; Li, P.; Wang, D.; Wang, Z.; Chen, Y.; et al. Drug Release from Phase-Changeable Nanodroplets Triggered by Low-Intensity Focused Ultrasound. Theranostics 2018, 8, 1327–1339. [Google Scholar] [CrossRef]
- Kawabata, K.; Sugita, N.; Yoshikawa, H.; Azuma, T.; Umemura, S.-I. Nanoparticles with Multiple Perfluorocarbons for Controllable Ultrasonically Induced Phase Shifting. Jpn. J. Appl. Phys. 2005, 44, 4548–4552. [Google Scholar] [CrossRef]
- Mi, P. Stimuli-responsive nanocarriers for drug delivery, tumor imaging, therapy and theranostics. Theranostics 2020, 10, 4557–4588. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Rognin, N.G.; Krupka, T.M.; Solorio, L.; Yoshiara, H.; Guenette, G.; Sanders, C.; Kamiyama, N.; Exner, A.A. Acoustic characterization and pharmacokinetic analyses of new nanobubble ultrasound contrast agents. Ultrasound Med. Biol. 2013, 39, 2137–2146. [Google Scholar] [CrossRef] [Green Version]
- Rapoport, N. Drug-Loaded Perfluorocarbon Nanodroplets for Ultrasound-Mediated Drug Delivery. Adv. Exp. Med. Biol. 2016, 880, 221–241. [Google Scholar] [CrossRef] [PubMed]
- Baghbani, F.; Moztarzadeh, F.; Mohandesi, J.A.; Yazdian, F.; Mokhtari-Dizaji, M. Novel alginate-stabilized doxorubicin-loaded nanodroplets for ultrasounic theranosis of breast cancer. Int. J. Biol. Macromol. 2016, 93, 512–519. [Google Scholar] [CrossRef]
- Batrakova, E.V.; Bronich, T.K.; Vetro, J.A.; Kabanov, A.V. Polymer Micelles as Drug Carriers. In Nanoparticulates as Drug Carriers; Torčilin, V.P., Ed.; Imperial College Press: London, UK, 2006; pp. 57–93. ISBN 978-1-86094-630-1. [Google Scholar]
- Rapoport, N. Physical stimuli-responsive polymeric micelles for anti-cancer drug delivery. Prog. Polym. Sci. 2007, 32, 962–990. [Google Scholar] [CrossRef]
- Nagarajan, R. Solubilization of hydrocarbons and resulting aggregate shape transitions in aqueous solutions of Pluronic® (PEO–PPO–PEO) block copolymers. Colloids Surf. B Biointerfaces 1999, 16, 55–72. [Google Scholar] [CrossRef]
- Lu, Y.; Park, K. Polymeric micelles and alternative nanonized delivery vehicles for poorly soluble drugs. Int. J. Pharm. 2013, 453, 198–214. [Google Scholar] [CrossRef] [Green Version]
- Nelson, J.L.; Roeder, B.L.; Carmen, J.C.; Roloff, F.; Pitt, W.G. Ultrasonically activated chemotherapeutic drug delivery in a rat model. Cancer Res. 2002, 62, 7280–7283. [Google Scholar]
- Paris, J.L.; Cabañas, M.V.; Manzano, M.; Vallet-Regí, M. Polymer-Grafted Mesoporous Silica Nanoparticles as Ultrasound-Responsive Drug Carriers. ACS Nano 2015, 9, 11023–11033. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Chen, L.; Nie, W.; Wang, W.; Qin, M.; Mo, X.; Wang, H.; He, C. Dual-Responsive Mesoporous Silica Nanoparticles Mediated Codelivery of Doxorubicin and Bcl-2 SiRNA for Targeted Treatment of Breast Cancer. J. Phys. Chem. C 2016, 120, 22375–22387. [Google Scholar] [CrossRef]
- Ma, K.; Sai, H.; Wiesner, U. Ultrasmall sub-10 nm near-infrared fluorescent mesoporous silica nanoparticles. J. Am. Chem. Soc. 2012, 134, 13180–13183. [Google Scholar] [CrossRef]
- Meng, H.; Xue, M.; Xia, T.; Ji, Z.; Tarn, D.Y.; Zink, J.I.; Nel, A.E. Use of size and a copolymer design feature to improve the biodistribution and the enhanced permeability and retention effect of doxorubicin-loaded mesoporous silica nanoparticles in a murine xenograft tumor model. ACS Nano 2011, 5, 4131–4144. [Google Scholar] [CrossRef] [Green Version]
- Manzano, M.; Vallet-Regí, M. Ultrasound responsive mesoporous silica nanoparticles for biomedical applications. Chem. Commun. 2019, 55, 2731–2740. [Google Scholar] [CrossRef] [Green Version]
- Peng, S.-Y.; Zou, M.-Z.; Zhang, C.-X.; Ma, J.-B.; Zeng, X.; Xiao, W. Fabrication of rapid-biodegradable nano-vectors for endosomal-triggered drug delivery. J. Drug Deliv. Sci. Technol. 2020, 55, 101450. [Google Scholar] [CrossRef]
- Wu, M.; Chen, W.; Chen, Y.; Zhang, H.; Liu, C.; Deng, Z.; Sheng, Z.; Chen, J.; Liu, X.; Yan, F.; et al. Focused Ultrasound-Augmented Delivery of Biodegradable Multifunctional Nanoplatforms for Imaging-Guided Brain Tumor Treatment. Adv. Sci. 2018, 5, 1700474. [Google Scholar] [CrossRef]
- Li, X.; Wang, Z.; Xia, H. Ultrasound Reversible Response Nanocarrier Based on Sodium Alginate Modified Mesoporous Silica Nanoparticles. Front. Chem. 2019, 7, 59. [Google Scholar] [CrossRef]
- Sun, W.; Li, Z.; Zhou, X.; Yang, G.; Yuan, L. Efficient exosome delivery in refractory tissues assisted by ultrasound-targeted microbubble destruction. Drug Deliv. 2019, 26, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.-C.; Gao, J.-Q. Exosomes as novel bio-carriers for gene and drug delivery. Int. J. Pharm. 2017, 521, 167–175. [Google Scholar] [CrossRef]
- Yousefpour, P.; Chilkoti, A. Co-opting biology to deliver drugs. Biotechnol. Bioeng. 2014, 111, 1699–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Qu, L.; Shuang, T.; Wu, S.; Su, Y.; Lu, F.; Wang, D.; Chen, B.; Hao, Q. Low-intensity ultrasound radiation increases exosome yield for efficient drug delivery. J. Drug Deliv. Sci. Technol. 2020, 57, 101713. [Google Scholar] [CrossRef]
- Yuana, Y.; Balachandran, B.; van der Wurff-Jacobs, K.M.G.; Schiffelers, R.M.; Moonen, C.T. Potential Use of Extracellular Vesicles Generated by Microbubble-Assisted Ultrasound as Drug Nanocarriers for Cancer Treatment. Int. J. Mol. Sci. 2020, 21, 24. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Liu, Y.; Guo, K.; Zhang, K.; Liu, Q.; Wang, P.; Wang, X. Ultrasound Facilitates Naturally Equipped Exosomes Derived from Macrophages and Blood Serum for Orthotopic Glioma Treatment. ACS Appl. Mater. Interfaces 2019, 11, 14576–14587. [Google Scholar] [CrossRef] [PubMed]
- Kheirolomoom, A.; Lai, C.-Y.; Tam, S.M.; Mahakian, L.M.; Ingham, E.S.; Watson, K.D.; Ferrara, K.W. Complete regression of local cancer using temperature-sensitive liposomes combined with ultrasound-mediated hyperthermia. J. Control. Release 2013, 172, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.; Gao, J.; Jiang, L.; Luo, J.; Jing, L.; Li, X.; Jin, Y.; Dai, Z. Nanohybrid liposomal cerasomes with good physiological stability and rapid temperature responsiveness for high intensity focused ultrasound triggered local chemotherapy of cancer. ACS Nano 2015, 9, 1280–1293. [Google Scholar] [CrossRef]
- Snipstad, S.; Berg, S.; Mørch, Ý.; Bjørkøy, A.; Sulheim, E.; Hansen, R.; Grimstad, I.; van Wamel, A.; Maaland, A.F.; Torp, S.H.; et al. Ultrasound Improves the Delivery and Therapeutic Effect of Nanoparticle-Stabilized Microbubbles in Breast Cancer Xenografts. Ultrasound Med. Biol. 2017, 43, 2651–2669. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Zhao, H.; Zhou, Z.; Xia, Y.; Wang, Z.; Ran, H.; Li, P.; Ren, J. Peptide-Functionalized Phase-Transformation Nanoparticles for Low Intensity Focused Ultrasound-Assisted Tumor Imaging and Therapy. Nano Lett. 2018, 18, 1831–1841. [Google Scholar] [CrossRef]
- Xu, P.; Yao, J.; Li, Z.; Wang, M.; Zhou, L.; Zhong, G.; Zheng, Y.; Li, N.; Zhai, Z.; Yang, S.; et al. Therapeutic Effect of Doxorubicin-Chlorin E6-Loaded Mesoporous Silica Nanoparticles Combined with Ultrasound on Triple-Negative Breast Cancer. Int. J. Nanomed. 2020, 15, 2659–2668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Han, J.; Park, S.Y.; Kim, H.; Park, J.-H.; Lee, H.J. Antitumor Efficacy of Focused Ultrasound-MFL Nanoparticles Combination Therapy in Mouse Breast Cancer Xenografts. Materials 2020, 13, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Chang, S.; Sun, J.; Zhu, S.; Yin, M.; Zhu, Y.; Wang, Z.; Xu, R.X. Ultrasound-mediated destruction of paclitaxel and oxygen loaded lipid microbubbles for combination therapy in ovarian cancer xenografts. Cancer Lett. 2015, 361, 147–154. [Google Scholar] [CrossRef]
- Kang, J.; Wu, X.; Wang, Z.; Ran, H.; Xu, C.; Wu, J.; Wang, Z.; Zhang, Y. Antitumor effect of docetaxel-loaded lipid microbubbles combined with ultrasound-targeted microbubble activation on VX2 rabbit liver tumors. J. Ultrasound Med. 2010, 29, 61–70. [Google Scholar] [CrossRef]
- Li, P.; Zheng, Y.; Ran, H.; Tan, J.; Lin, Y.; Zhang, Q.; Ren, J.; Wang, Z. Ultrasound triggered drug release from 10-hydroxycamptothecin-loaded phospholipid microbubbles for targeted tumor therapy in mice. J. Control. Release 2012, 349–354. [Google Scholar] [CrossRef]
- Tinkov, S.; Coester, C.; Serba, S.; Geis, N.A.; Katus, H.A.; Winter, G.; Bekeredjian, R. New doxorubicin-loaded phospholipid microbubbles for targeted tumor therapy: In-vivo characterization. J. Control. Release 2010, 148, 368–372. [Google Scholar] [CrossRef]
- Yan, F.; Li, L.; Deng, Z.; Jin, Q.; Chen, J.; Yang, W.; Yeh, C.-K.; Wu, J.; Shandas, R.; Liu, X.; et al. Paclitaxel-liposome-microbubble complexes as ultrasound-triggered therapeutic drug delivery carriers. J. Control. Release 2013, 166, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Jiang, Y.; Luo, F.; Li, P. Effectiveness of localized ultrasound-targeted microbubble destruction with doxorubicin liposomes in H22 mouse hepatocellular carcinoma model. J. Drug Target. 2015, 323–334. [Google Scholar] [CrossRef]
- Olsman, M.; Sereti, V.; Andreassen, K.; Snipstad, S.; van Wamel, A.; Eliasen, R.; Berg, S.; Urquhart, A.J.; Andresen, T.L.; Davies, C.d.L. Ultrasound-mediated delivery enhances therapeutic efficacy of MMP sensitive liposomes. J. Control. Release 2020, 325, 121–134. [Google Scholar] [CrossRef]
- Myhr, G.; Moan, J. Synergistic and tumour selective effects of chemotherapy and ultrasound treatment. Cancer Lett. 2006, 232, 206–213. [Google Scholar] [CrossRef]
- Gao, Z.-G.; Fain, H.D.; Rapoport, N. Controlled and targeted tumor chemotherapy by micellar-encapsulated drug and ultrasound. J. Control. Release 2005, 102, 203–222. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Wang, Z.; Dong, G.; Sun, Y.; Wang, X.; Rong, Y.; Li, M.; Wang, D.; Ran, H. Low-intensity focused ultrasound mediated localized drug delivery for liver tumors in rabbits. Drug Deliv. 2016, 23, 2280–2289. [Google Scholar] [CrossRef]
- Xing, L.; Shi, Q.; Zheng, K.; Shen, M.; Ma, J.; Li, F.; Liu, Y.; Lin, L.; Tu, W.; Duan, Y.; et al. Ultrasound-Mediated Microbubble Destruction (UMMD) Facilitates the Delivery of CA19-9 Targeted and Paclitaxel Loaded mPEG-PLGA-PLL Nanoparticles in Pancreatic Cancer. Theranostics 2016, 6, 1573–1587. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Wu, M.; Zhu, L.; Tian, Y.; Wu, M.; Li, Y.; Deng, L.; Jiang, W.; Shen, W.; Wang, Z.; et al. Cell-penetrating Peptide-modified Targeted Drug-loaded Phase-transformation Lipid Nanoparticles Combined with Low-intensity Focused Ultrasound for Precision Theranostics against Hepatocellular Carcinoma. Theranostics 2018, 8, 1892–1910. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xu, F.; Huang, J.; Xu, J.; Liu, Y.; Yao, Y.; Ao, M.; Li, A.; Hao, L.; Cao, Y.; et al. Low-intensity focused ultrasound (LIFU)-activated nanodroplets as a theranostic agent for noninvasive cancer molecular imaging and drug delivery. Biomater. Sci. 2018, 6, 2838–2849. [Google Scholar] [CrossRef] [PubMed]
- Kotopoulis, S.; Stigen, E.; Popa, M.; Safont, M.M.; Healey, A.; Kvåle, S.; Sontum, P.; Gjertsen, B.T.; Gilja, O.H.; McCormack, E. Sonoporation with Acoustic Cluster Therapy (ACT®) induces transient tumour volume reduction in a subcutaneous xenograft model of pancreatic ductal adenocarcinoma. J. Control. Release 2017, 245, 70–80. [Google Scholar] [CrossRef]
- Lv, Y.; Cao, Y.; Li, P.; Liu, J.; Chen, H.; Hu, W.; Zhang, L. Ultrasound-Triggered Destruction of Folate-Functionalized Mesoporous Silica Nanoparticle-Loaded Microbubble for Targeted Tumor Therapy. Adv. Healthc. Mater. 2017, 6, 1700354. [Google Scholar] [CrossRef]
- Sayes, C.M.; Reed, K.L.; Warheit, D.B. Assessing toxicity of fine and nanoparticles: Comparing in vitro measurements to in vivo pulmonary toxicity profiles. Toxicol. Sci. 2007, 97, 163–180. [Google Scholar] [CrossRef] [Green Version]
- Stone, V.; Johnston, H.; Schins, R.P.F. Development of in vitro systems for nanotoxicology: Methodological considerations. Crit. Rev. Toxicol. 2009, 39, 613–626. [Google Scholar] [CrossRef]
- Kunzmann, A.; Andersson, B.; Thurnherr, T.; Krug, H.; Scheynius, A.; Fadeel, B. Toxicology of engineered nanomaterials: Focus on biocompatibility, biodistribution and biodegradation. Biochim. Biophys. Acta 2011, 1810, 361–373. [Google Scholar] [CrossRef]
- Lehner, R.; Wang, X.; Marsch, S.; Hunziker, P. Intelligent nanomaterials for medicine: Carrier platforms and targeting strategies in the context of clinical application. Nanomedicine 2013, 9, 742–757. [Google Scholar] [CrossRef]
- Delcassian, D.; Patel, A.K. Nanotechnology and drug delivery. In Bioengineering Innovative Solutions for Cancer; Ladame, S., Chang, J.Y.H., Eds.; Academic Press: London, UK, 2020; pp. 197–219. ISBN 9780128138861. [Google Scholar]
- Anchordoquy, T.J.; Barenholz, Y.; Boraschi, D.; Chorny, M.; Decuzzi, P.; Dobrovolskaia, M.A.; Farhangrazi, Z.S.; Farrell, D.; Gabizon, A.; Ghandehari, H.; et al. Mechanisms and Barriers in Cancer Nanomedicine: Addressing Challenges, Looking for Solutions. ACS Nano 2017, 11, 12–18. [Google Scholar] [CrossRef]
- Sukhanova, A.; Bozrova, S.; Sokolov, P.; Berestovoy, M.; Karaulov, A.; Nabiev, I. Dependence of Nanoparticle Toxicity on Their Physical and Chemical Properties. Nanoscale Res. Lett. 2018, 13, 44. [Google Scholar] [CrossRef] [Green Version]
- Warheit, D.B. How meaningful are the results of nanotoxicity studies in the absence of adequate material characterization? Toxicol. Sci. 2008, 101, 183–185. [Google Scholar] [CrossRef]
- Pan, Y.; Neuss, S.; Leifert, A.; Fischler, M.; Wen, F.; Simon, U.; Schmid, G.; Brandau, W.; Jahnen-Dechent, W. Size-dependent cytotoxicity of gold nanoparticles. Small 2007, 3, 1941–1949. [Google Scholar] [CrossRef]
- Bahadar, H.; Maqbool, F.; Niaz, K.; Abdollahi, M. Toxicity of Nanoparticles and an Overview of Current Experimental Models. Iran. Biomed. J. 2016, 20, 1–11. [Google Scholar] [CrossRef]
- Dukhin, S.S.; Labib, M.E. Convective diffusion of nanoparticles from the epithelial barrier toward regional lymph nodes. Adv. Colloid Interface Sci. 2013, 199–200, 23–43. [Google Scholar] [CrossRef] [Green Version]
- Oberdörster, G.; Maynard, A.; Donaldson, K.; Castranova, V.; Fitzpatrick, J.; Ausman, K.; Carter, J.; Karn, B.; Kreyling, W.; Lai, D.; et al. Principles for characterizing the potential human health effects from exposure to nanomaterials: Elements of a screening strategy. Part. Fibre Toxicol. 2005, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Barua, S.; Mitragotri, S. Challenges associated with Penetration of Nanoparticles across Cell and Tissue Barriers: A Review of Current Status and Future Prospects. Nano Today 2014, 9, 223–243. [Google Scholar] [CrossRef] [PubMed]
- Champion, J.A.; Mitragotri, S. Role of target geometry in phagocytosis. Proc. Natl. Acad. Sci. USA 2006, 103, 4930–4934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexis, F.; Pridgen, E.; Molnar, L.K.; Farokhzad, O.C. Factors affecting the clearance and biodistribution of polymeric nanoparticles. Mol. Pharm. 2008, 5, 505–515. [Google Scholar] [CrossRef] [Green Version]
- Lynch, I.; Cedervall, T.; Lundqvist, M.; Cabaleiro-Lago, C.; Linse, S.; Dawson, K.A. The nanoparticle-protein complex as a biological entity; a complex fluids and surface science challenge for the 21st century. Adv. Colloid Interface Sci. 2007, 134-135, 167–174. [Google Scholar] [CrossRef]
- Lundqvist, M.; Stigler, J.; Elia, G.; Lynch, I.; Cedervall, T.; Dawson, K.A. Nanoparticle size and surface properties determine the protein corona with possible implications for biological impacts. Proc. Natl. Acad. Sci. USA 2008, 105, 14265–14270. [Google Scholar] [CrossRef] [Green Version]
- Walkey, C.D.; Chan, W.C.W. Understanding and controlling the interaction of nanomaterials with proteins in a physiological environment. Chem. Soc. Rev. 2012, 41, 2780–2799. [Google Scholar] [CrossRef] [PubMed]
- Silindir-Gunay, M.; Karpuz, M.; Ozer, A.Y. Targeted Alpha Therapy and Nanocarrier Approach. Cancer Biother. Radiopharm. 2020. [Google Scholar] [CrossRef] [PubMed]
- Muttil, P.; Kunda, N.K. Mucosal Delivery of Drugs and Biologics in Nanoparticles; Springer: Cham, Switzerland, 2020; ISBN 978-3-030-35909-6. [Google Scholar]
- Qian, X.; Han, X.; Chen, Y. Insights into the unique functionality of inorganic micro/nanoparticles for versatile ultrasound theranostics. Biomaterials 2017, 142, 13–30. [Google Scholar] [CrossRef] [PubMed]
- Arami, H.; Khandhar, A.; Liggitt, D.; Krishnan, K.M. In vivo delivery, pharmacokinetics, biodistribution and toxicity of iron oxide nanoparticles. Chem. Soc. Rev. 2015, 44, 8576–8607. [Google Scholar] [CrossRef]
- Shankar, H.; Pagel, P.S. Potential adverse ultrasound-related biological effects: A critical review. Anesthesiology 2011, 115, 1109–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Concept | Principle | Additional Information |
|---|---|---|
| Hyperthermia | - induces drug release from specially designed thermo-sensitive nanoparticles (e.g., Thermodox®) [40] - leads to increased blood flow and fenestration in heated tumor tissue, resulting in improved nanoparticle accumulation in tumors [70,71] | - see also Section 2.3.1 |
| Ultrasound targeted microbubble destruction (UTMD) and sonoporation | - combines low frequency moderate power US with microbubbles for triggering cavitation, thus obtaining the sonoporation effect [72] | - Sonoporation: biophysical process that is based on stable or inertial acoustic cavitation of microbubbles; used for enhancing the permeability of plasma membranes through the generation of short-lived pores - see also Section 2.3.1 |
| Sonoprinting | - based on US application to nanoparticle-loaded microbubbles, which leads to a direct deposition of nanoparticles along with parts of the bubble shell onto cell membranes, followed by cell internalization after several hours | - novel mechanism of using microbubbles for drug delivery, as recently proposed by Cock et al. [73]. |
| Acoustic cluster therapy (ACT®) | - comprises i.v. administration of free-flowing clusters of negatively charged microbubbles and positively charged microdroplets (oil droplets) - co-administration of drugs or loading of microdroplets with lipophilic therapeutic agent - initiation of vaporization process of the oil droplet by activating the clusters with US - production of large gas bubbles by inwards diffusion of blood gases (20–30 µm) and transient occlusion of blood flow (~5–10 min) - drug release from microdroplets due to cluster activation into the local blood compartment - induction of biomechanical effects by further US application, leading to increased vascular permeability and locally enhanced extravasation of components from the vascular compartment (e.g., released or co-administered drugs) [74] | - immediate drug wash out is avoided due to the transient occlusion of the vessel, and the drug is kept locally at high concentrations for a certain period of time |
| Sonodynamic therapy (SDT) | - three key elements necessary: low-intensity US, special agents known as sonosensitizers and molecular oxygen - principle relies on the accumulation of sonosensitizers in the tumor tissue and their activation by the action of ultrasonic cavitation - interaction of the induced sonosensitizer with the surrounding oxygen molecules will lead to the generation of reactive oxygen species (ROS) and eventually to the irreversible destruction of the targeted tumor tissue [75] | - approach complementary to photodynamic therapy; here, however, US instead of light is used as the external stimulus [76] |
| Acoustic droplet vaporization (ADV) | - technique employs volatile liquid acoustic phase shift nanodroplets that are typically composed of a PFC core and lipid coating - penetration of small nanodroplets into the extravascular stroma tissue of tumors followed by US exposition - PFC droplets inside the coating then undergo a phase transition from liquid into an expanding gas bubble - major effect of ADV is inertial cavitation (see 2.3.1) [77] - expansion of the droplets during the transition process to form gas bubbles leads to disruption of the lipid coating and thus a rapid release of the drug content [78] - in addition, inertial cavitation effect of ADV can also cause physical disruption at the tumor site [79] | - first introduced by Kripfgans et al. [80] |
| Concept | Principle | Additional Information |
|---|---|---|
| Surface functionalization of nanocarriers | - modification of NP surfaces to achieve desired NP properties and behavior, such as stimulus-responsiveness, targeting, stability and others [13] | - e.g., nanoparticles can be PEGylated for escaping the RES and thus for increasing the blood circulation time. Further possible surface modifications include the binding of antibodies or ligands to enhance target-specific drug delivery [10] |
| Co-delivery | - simultaneous transport of different agents such as therapeutic drugs and imaging agents [80], two chemotherapeutic drugs, oligonucleotides and chemotherapeutics [81] or chemotherapeutics and anticancer metals [82] | - offers promising strategies for increasing therapeutic efficacies |
| Multiple triggered systems | - systems sensitive to multiple stimuli - can be applied as hierarchical platforms, which are based on changeable particle sizes, switchable surface charges and activatable surface ligands - potentially enhancing both, tumor tissue accumulation/retention and cellular internalization of nanocarriers - stepwise drug release possible [69,83] | - e.g., exposure of a moiety on the NP surface that induces uptake after a certain environmental condition is present (e.g., heat, low pH, enzymes) |
| Theranostic approach | - Theranostics: combined term derived from the words ‘diagnosis’ and ‘therapy’, meaning that diagnostic imaging and therapeutic treatment can be carried out using a single multifunctional nanomaterial | - development of image-guided drug delivery systems is possible (e.g., US or MRI imaging combined with US-mediated drug delivery) [84] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Entzian, K.; Aigner, A. Drug Delivery by Ultrasound-Responsive Nanocarriers for Cancer Treatment. Pharmaceutics 2021, 13, 1135. https://doi.org/10.3390/pharmaceutics13081135
Entzian K, Aigner A. Drug Delivery by Ultrasound-Responsive Nanocarriers for Cancer Treatment. Pharmaceutics. 2021; 13(8):1135. https://doi.org/10.3390/pharmaceutics13081135
Chicago/Turabian StyleEntzian, Kristin, and Achim Aigner. 2021. "Drug Delivery by Ultrasound-Responsive Nanocarriers for Cancer Treatment" Pharmaceutics 13, no. 8: 1135. https://doi.org/10.3390/pharmaceutics13081135