
Development of a Cyclodextrin-Based Mucoadhesive-Thermosensitive In Situ Gel for Clonazepam Intranasal Delivery

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. HPLC Assay of Clonazepam (CLZ)
2.3. Experimental Design
2.4. Thermosensitive Gels Preparation
2.5. Characterization of Thermosensitive Gels
2.5.1. Determination of pH
2.5.2. Determination of Gelation Temperature
2.5.3. Determination of Gelation Time
2.5.4. Determination of Gel Strength
2.5.5. Determination of Gel Mucoadhesive Strength
2.5.6. Determination of Mucoadhesion Time
2.5.7. Rheological Studies
2.6. In Vitro Drug Release Studies
2.7. Cytotoxicity and Transport Studies
2.8. Statistical Analysis
3. Results
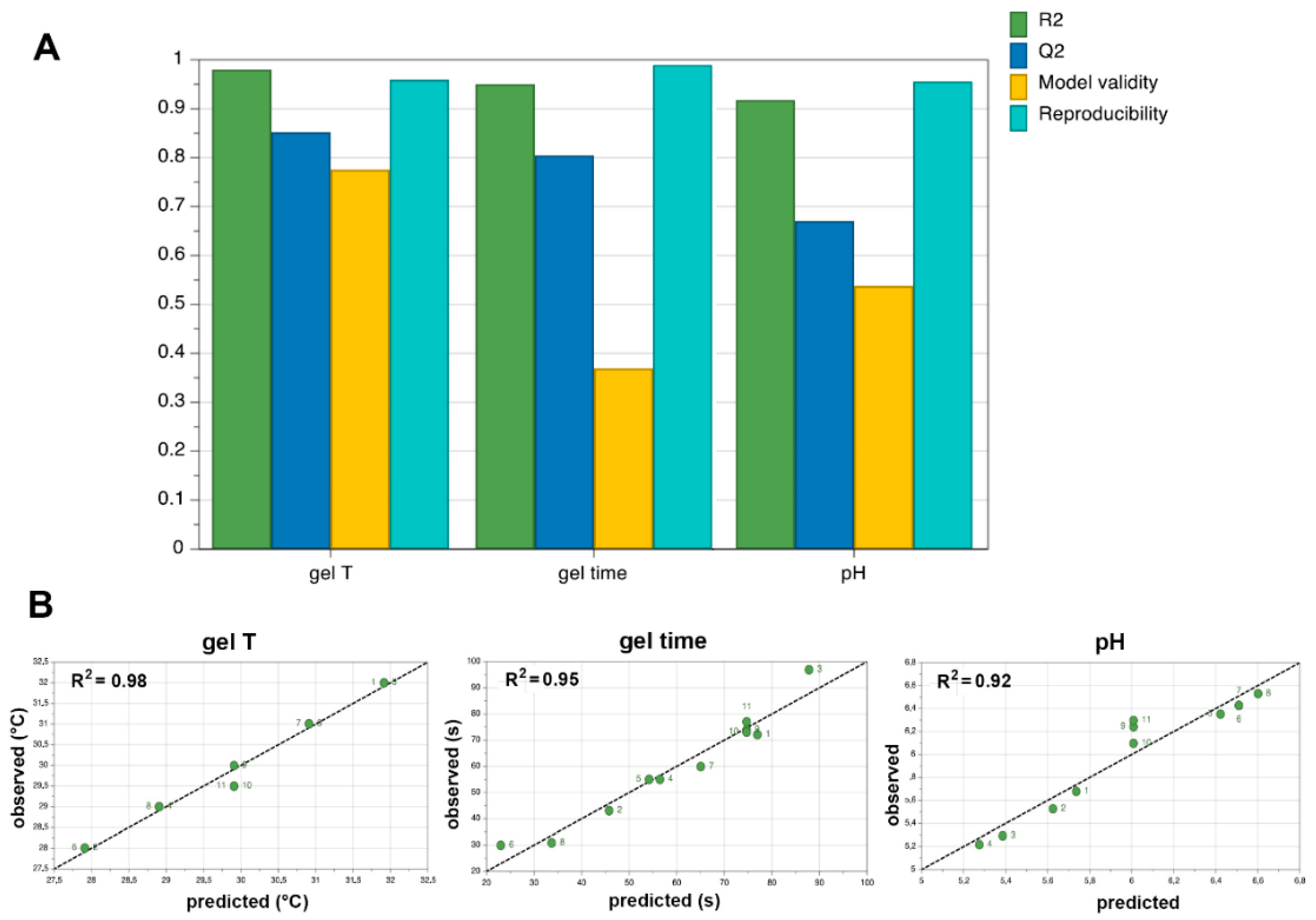
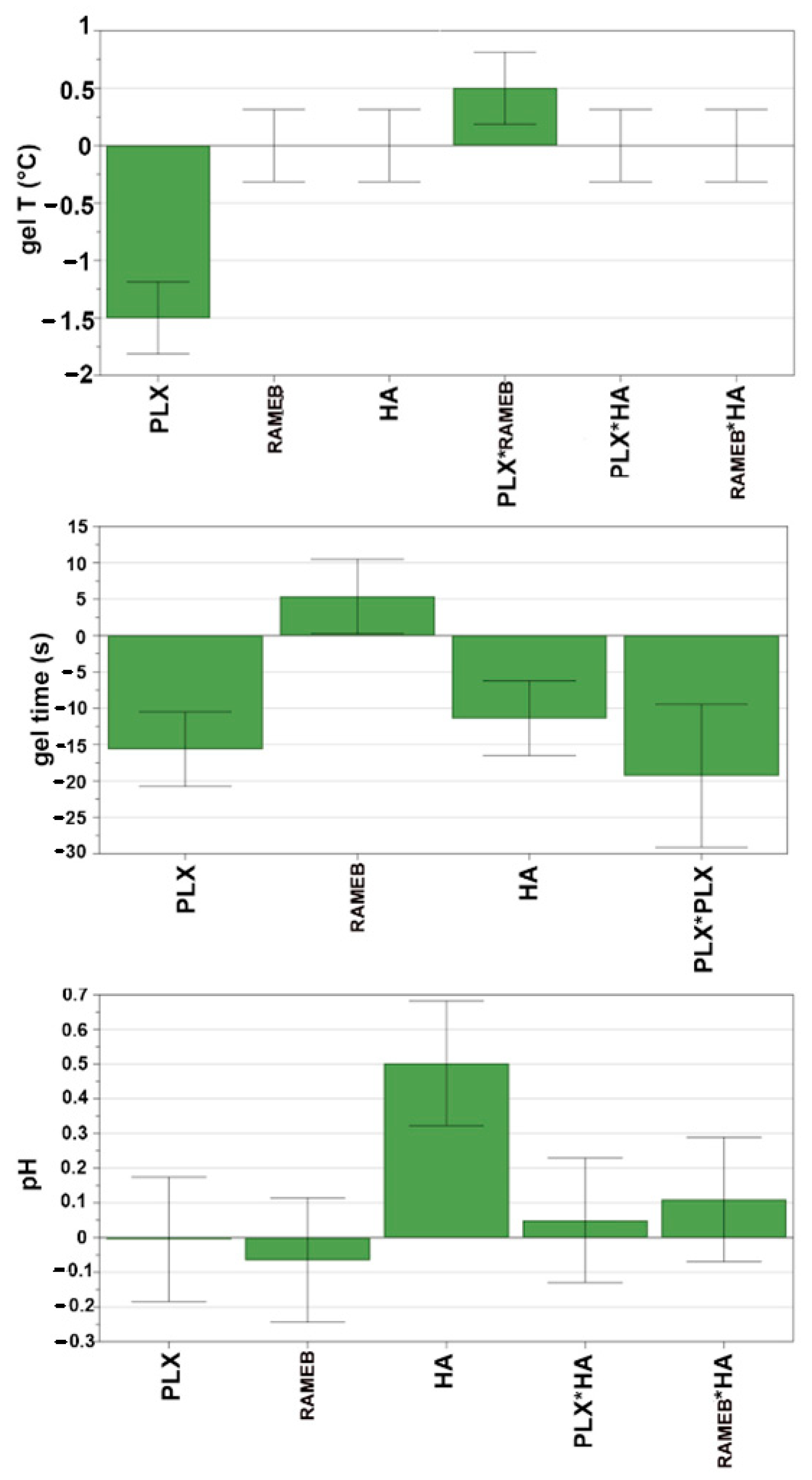
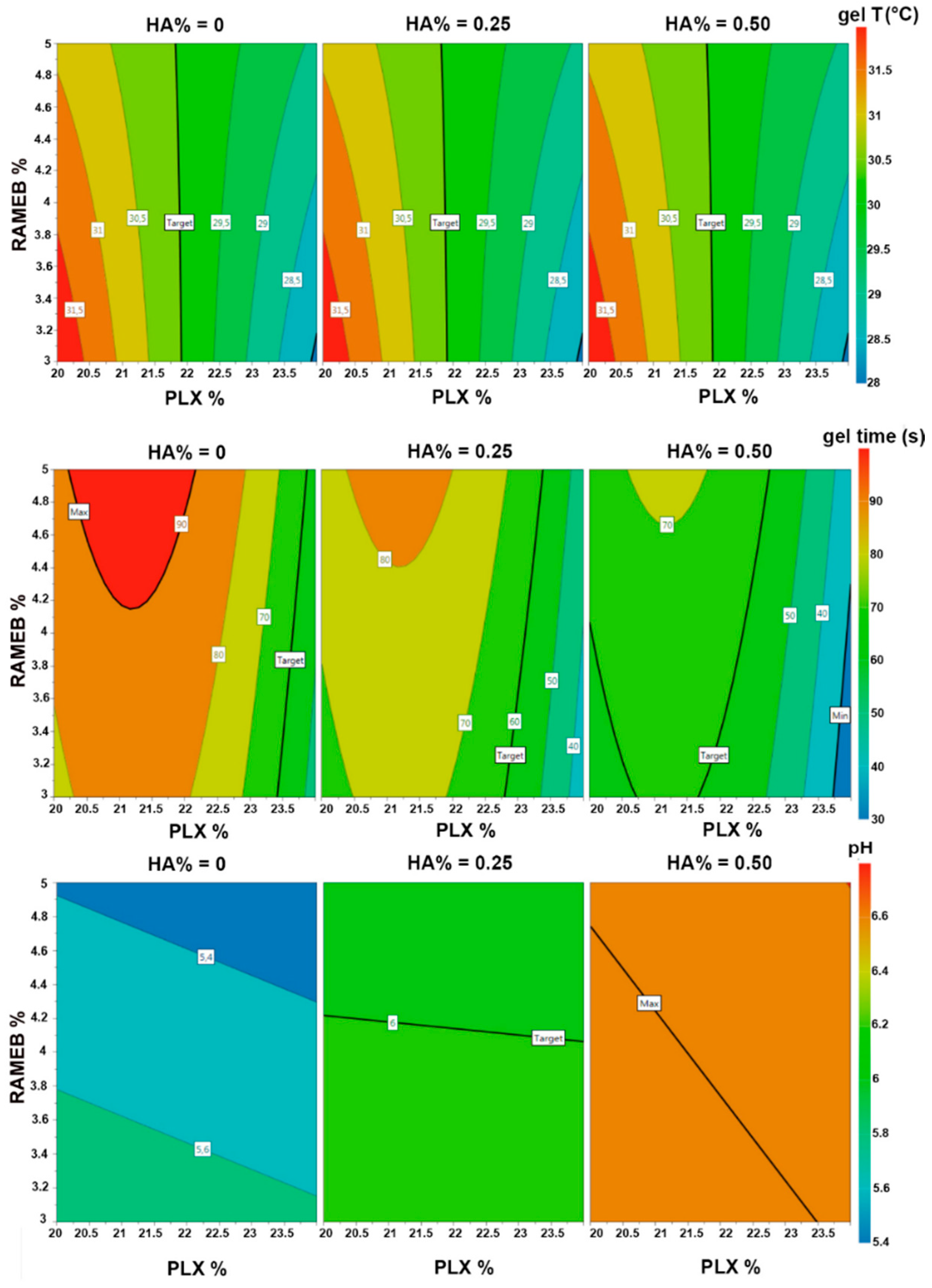
3.1. Pre-Formulation Studies with Design of Experiment (DoE)
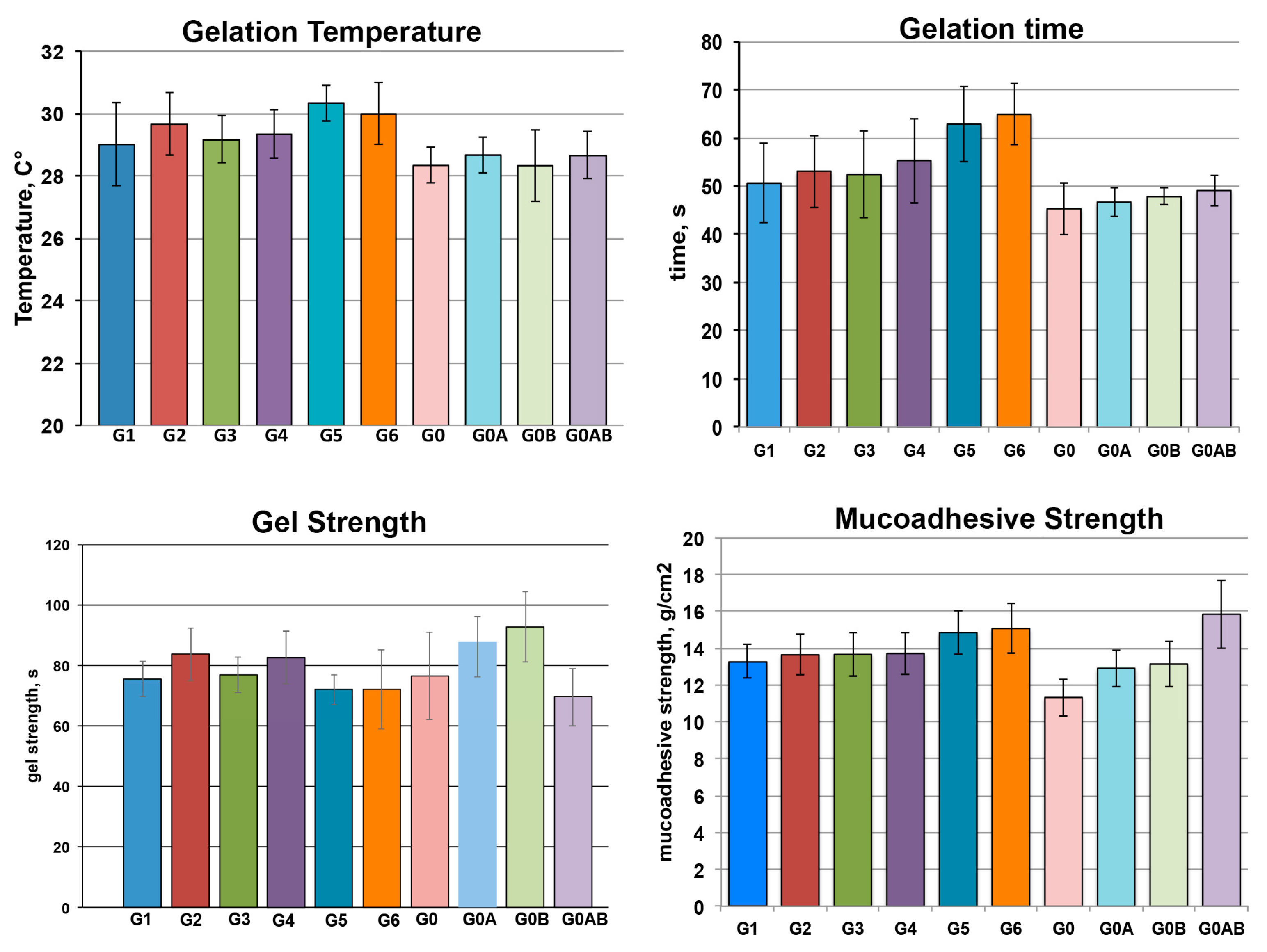
3.2. Preparation and Characterization of Drug-Loaded Gel Formulations
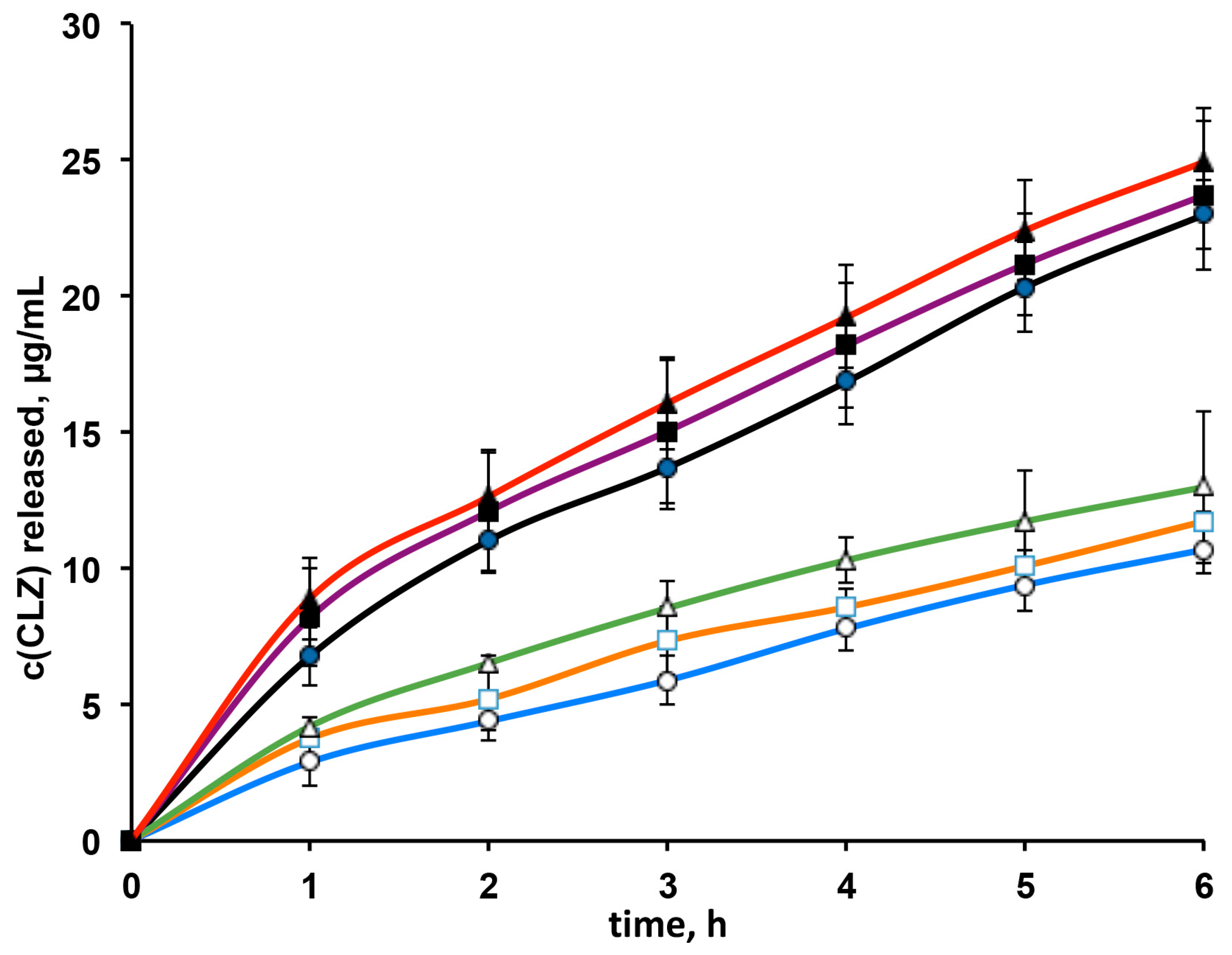
3.3. In Vitro Drug Release Studies
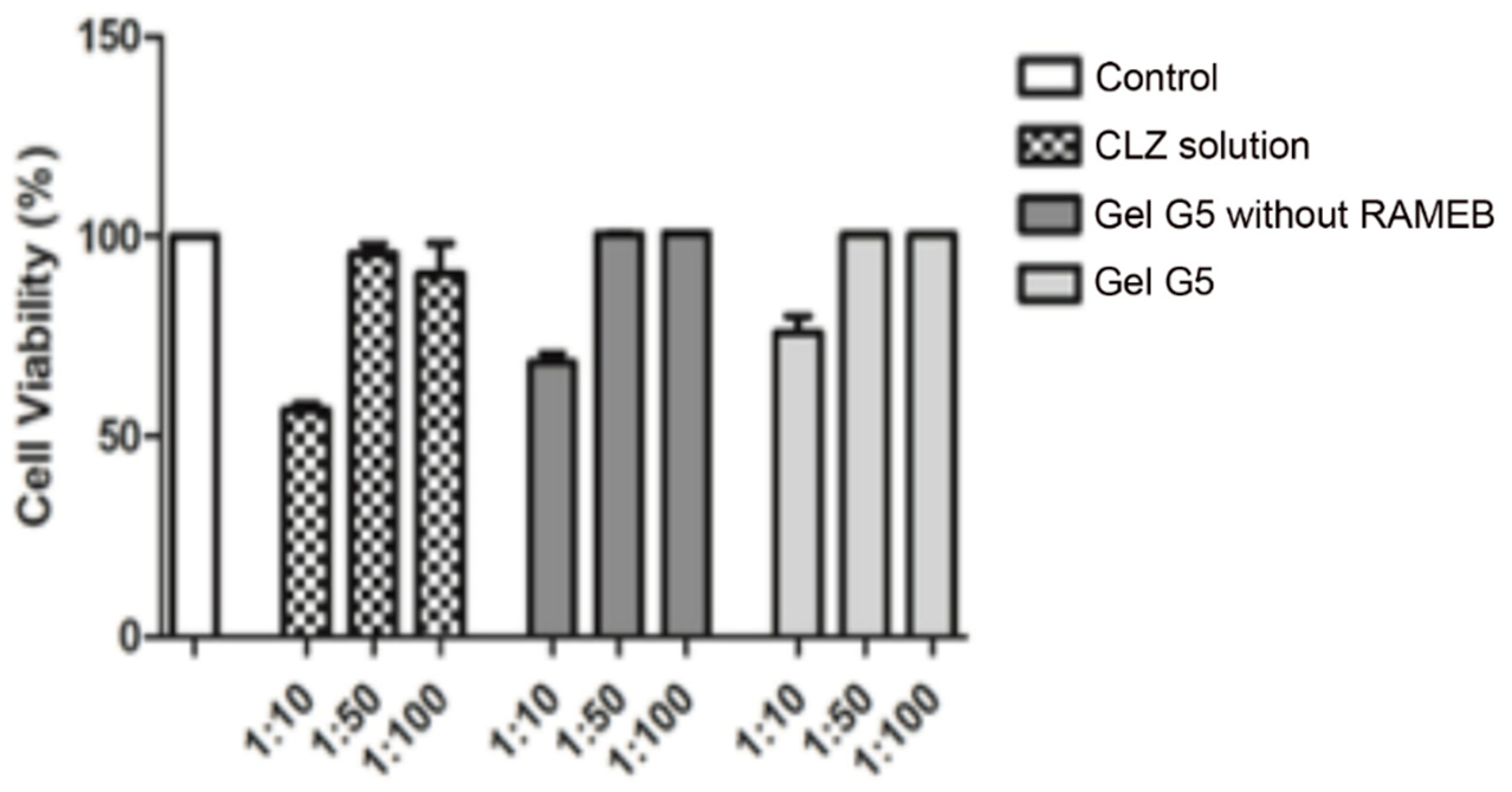
3.4. Cytotoxicity and Transport Studies through Caco-2 Cells
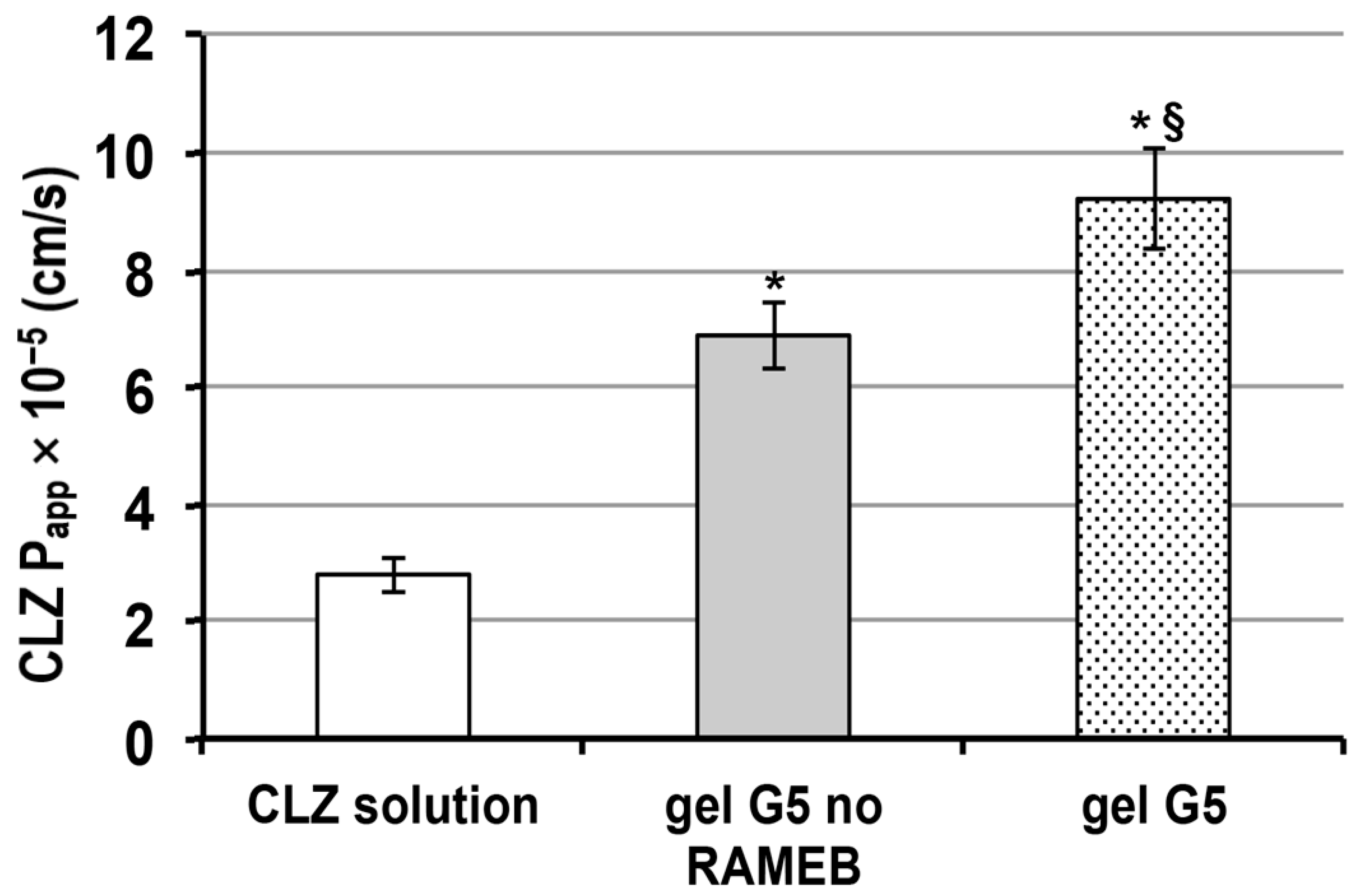
3.5. Transport Experiments with Caco-2 Cells
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- WHO Mental Health: Neurological Disorders. Available online: https://www.who.int/news-room/q-a-detail/mental-health-neurological-disorders (accessed on 16 May 2016).
- Rey, E.; Tréluyer, J.M.; Pons, G. Pharmacokinetic optimization of benzodiazepine therapy for acute seizures. Focus on delivery routes. Clin. Pharmacokinet. 1999, 36, 409–424. [Google Scholar] [CrossRef]
- Martindale, W.; Sweetman, S.C. Martindale: The Complete Drug Reference, 33rd ed.; Pharmaceutical Press: London, UK, 2002; pp. 347–348. [Google Scholar]
- Lockey, A.S. Emergency department drug therapy for status epilepticus in adults. Emerg. Med. J. 2002, 19, 96–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koubeissi, M. Intravenous Clonazepam in Status Epilepticus. Epilepsy Curr. 2016, 16, 89–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vyas, T.K.; Babbar, A.; Sharma, R.K.; Singh, S.; Misra, A. Intranasal Mucoadhesive Microemulsions of Clonazepam: Preliminary Studies on Brain Targeting. J. Pharm. Sci. 2006, 95, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Roche. KLONOPIN Tablets (Clonazepam) KLONOPIN Wafers (Clonazepam ODT). Available online: http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/017533s045,020813s005lbl.pdf (accessed on 13 April 2021).
- Pires, A.; Fortuna, A.; Alves, G.; Falcão, A. Intranasal Drug Delivery: How, Why and What for? J. Pharm. Pharm. Sci. 2009, 12, 288–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, L.-A.; Merkel, O.; Popp, A. Intranasal drug delivery: Opportunities and toxicologic challenges during drug development. Drug Deliv. Transl. Res. 2021, 1–23. [Google Scholar] [CrossRef]
- Kumar, H.; Mishra, G.; Sharma, A.K.; Gothwal, A.; Kesharwani, P.; Gupta, U. Intranasal Drug Delivery: A Non-Invasive Approach for the Better Delivery of Neurotherapeutics. Pharm. Nanotechnol. 2018, 5, 1. [Google Scholar] [CrossRef]
- Erdőa, F.; Bors, L.A.; Farkasa, D.; Bajzaa, Á.; Gizurarsonb, S. Evaluation of intranasal delivery route of drug administration for brain targeting. Brain Res. Bull. 2018, 143, 155–170. [Google Scholar] [CrossRef]
- Kapoor, M.; Cloyd, J.C.; Siegel, R.A. A review of intranasal formulations for the treatment of seizure emergencies. J. Control. Release 2016, 237, 147–159. [Google Scholar] [CrossRef]
- Boddu, S.H.S.; Kumari, S. A Short Review on the Intranasal Delivery of Diazepam for Treating Acute Repetitive Seizures. Pharmaceutics 2020, 12, 1167. [Google Scholar] [CrossRef]
- Wengst, A.; Reichl, S. RPMI 2650 epithelial model and three-dimensional reconstructed human nasal mucosa as in vitro models for nasal permeation studies. Eur. J. Pharm. Biopharm. 2010, 74, 290–297. [Google Scholar] [CrossRef]
- Wolburg, H.; Wolburg-Buchholz, K.; Sam, H.; Horvát, S.; Deli, M.A.; Mack, A.F. Epithelial and endothelial barriers in the olfactory region of the nasal cavity of the rat. Histochem. Cell Biol. 2008, 130, 127–140. [Google Scholar] [CrossRef]
- Karavasili, C.; Fatouros, D.G. Smart materials: In situ gel-forming systems for nasal delivery. Drug Discov. Today 2016, 21, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Sabale, A.S.; Kulkarni, A.D. Nasal in situ gel: Novel approach for nasal drug delivery. J. Drug Deliv. Ther. 2020, 10, 183–197. [Google Scholar] [CrossRef]
- Wang, Q.; Zuo, Z.; Cheung, C.K.C.; Leung, S.S.Y. Updates on thermosensitive hydrogel for nasal, ocular and cutaneous delivery. Int. J. Pharm. 2019, 559, 86–101. [Google Scholar] [CrossRef] [PubMed]
- Shelke, S.; Shahi, S.; Jalalpure, S.; Dhamecha, D.; Shengule, S. Formulation and evaluation of thermoreversible mucoadhesive in-situ gel for intranasal delivery of naratriptan hydrochloride. J. Drug Deliv. Sci. Technol. 2015, 29, 238–244. [Google Scholar] [CrossRef]
- Kempwade, A.; Taranalli, A. Formulation and evaluation of thermoreversible, mucoadhesive in situ intranasal gel of rizatriptan benzoate. J. Sol-Gel Sci. Technol. 2014, 72, 43–48. [Google Scholar] [CrossRef]
- Gu, F.; Fan, H.; Cong, Z.; Li, S.; Wang, Y.; Wu, C. Preparation, characterization, and in vivo pharmacokinetics of thermosensitive in situ nasal gel of donepezil hydrochloride. Acta Pharm. 2020, 70, 411–422. [Google Scholar] [CrossRef] [Green Version]
- Russo, E.; Villa, C. Poloxamer Hydrogels for Biomedical Applications. Pharmaceutics 2019, 11, 671. [Google Scholar] [CrossRef] [Green Version]
- Dumortier, G.; Grossiord, J.L.; Agnely, F.; Chaumeil, J.C. A Review of Poloxamer 407 Pharmaceutical and Pharmacological Characteristics. Pharm. Res. 2006, 23, 2709–2728. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.M.; Kumar, A.; Pathak, K. Mucoadhesive in situ nasal gelling drug delivery systems for modulated drug delivery. Expert Opin. Drug Deliv. 2013, 10, 115–130. [Google Scholar] [CrossRef]
- Zahir-Jouzdani, F.; Wolf, J.D.; Atyabi, F.; Bernkop-Schnürch, A. In situ gelling and mucoadhesive polymers: Why do they need each other? Expert Opin. Drug Deliv. 2018, 15, 1007–1019. [Google Scholar] [CrossRef]
- Casettari, L.; Illum, L. Chitosan in nasal delivery systems for therapeutic drugs. J. Control. Release 2014, 190, 189–200. [Google Scholar] [CrossRef]
- Iacob, A.; Lupascu, F.; Apotrosoaei, M.; Vasincu, I.; Tauser, R.; Lupascu, D.; Giusca, S.; Caruntu, I.-D.; Profire, L. Recent Biomedical Approaches for Chitosan Based Materials as Drug Delivery Nanocarriers. Pharmaceutics 2021, 13, 587. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.-H.; Jones, S.A.; Forbes, B.; Martin, G.P.; Brown, M. Hyaluronan: Pharmaceutical Characterization and Drug Delivery. Drug Deliv. 2005, 12, 327–342. [Google Scholar] [CrossRef]
- Jin, Y.-J.; Ubonvan, T.; Kim, D.-D. Hyaluronic Acid in Drug Delivery Systems. J. Pharm. Investig. 2010, 40, 33–43. [Google Scholar] [CrossRef]
- Jacob, S.; Nair, A.B. Cyclodextrin complexes: Perspective from drug delivery and formulation. Drug Dev. Res. 2018, 79, 201–217. [Google Scholar] [CrossRef]
- Mennini, N.; Bragagni, M.; Maestrelli, F.; Mura, P. Physico-chemical characterization in solution and in the solid state of clonazepam complexes with native and chemically-modified cyclodextrins. J. Pharm. Biomed. Anal. 2014, 89, 142–149. [Google Scholar] [CrossRef]
- Marttin, E.; Verhoef, J.C.; Merkus, F.W.H.M. Efficacy, Safety and Mechanism of Cyclodextrins as Absorption Enhancers in Nasal Delivery of Peptide and Protein Drugs. J. Drug Target. 1998, 6, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Gänger, S.; Schindowski, K. Tailoring Formulations for Intranasal Nose-to-Brain Delivery: A Review on Architecture, Physico-Chemical Characteristics and Mucociliary Clearance of the Nasal Olfactory Mucosa. Pharmaceutics 2018, 10, 116. [Google Scholar] [CrossRef] [Green Version]
- Merkus, F.W.H.M.; Verhoef, J.C.; Martin, E.; Romeijn, S.G.; van der Kuy, P.H.M.; Hermens, W.A.J.J.; Schipper, N.G.M. Cyclodextrins in nasal drug delivery. Adv. Drug Del. Rev. 1999, 36, 41–57. [Google Scholar] [CrossRef]
- Basu, S.; Bandyopadhyay, A.K. Development and Characterization of Mucoadhesive In Situ Nasal Gel of Midazolam Prepared with Ficus carica Mucilage. AAPS PharmSciTech 2010, 11, 1223–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jose, S.; Ansa, C.R.; Cinu, T.A.; Chacko, A.J.; Aleykutty, N.A.; Ferreira, S.V.; Souto, E.B. Thermo-sensitive gels containing lorazepam microspheres for intranasal brain targeting. Int. J. Pharm. 2013, 441, 516–526. [Google Scholar] [CrossRef]
- Nour, S.A.; Abdelmalak, N.; Naguib, M.J.; Rashed, H.; Ibrahim, A.B. Intranasal brain-targeted clonazepam polymeric micelles for immediate control of status epilepticus: In vitro optimization, ex vivo determination of cytotoxicity, in vivo biodistribution and pharmacodynamics studies. Drug Deliv. 2016, 23, 3681–3695. [Google Scholar] [CrossRef] [Green Version]
- Shaji, J.; Poddar, A.; Iyer, S. Brain-Targeted Nasal Clonazepam Microspheres. Indian J. Pharm. Sci. 2019, 71, 715–718. [Google Scholar]
- Gratieri, T.; Gelfuso, G.M.; Rocha, E.; Sarmento, V.H.; de Freitas, O.; Lopez, R.F.V. A poloxamer/chitosan in situ forming gel with prolonged retention time for ocular delivery. Eur. J. Pharm. Biopharm. 2010, 75, 186–193. [Google Scholar] [CrossRef]
- Cho, H.-J.; Balakrishnan, P.; Park, E.-K.; Song, K.-W.; Hong, S.-S.; Jang, T.-Y.; Kim, K.-S.; Chung, S.-J.; Shim, C.-K.; Kim, D.-D. Poloxamer/Cyclodextrin/Chitosan-Based Thermoreversible Gel for Intranasal Delivery of Fexofenadine Hydrochloride. J. Pharm. Sci. 2011, 100, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Mayol, L.; Quaglia, F.; Borzacchiello, A.; Ambrosio, L.; Rotonda, M.L. A novel poloxamers/hyaluronic acid in situ forming hydrogel for drug delivery: Rheological, mucoadhesive and in vitro release properties. Eur. J. Pharm. Biopharm. 2008, 70, 199–206. [Google Scholar] [CrossRef]
- Jung, Y.-S.; Park, W.; Park, H.; Lee, D.-K.; Na, K. Thermo-sensitive injectable hydrogel based on the physical mixing of hyaluronic acid and Pluronic F-127 for sustained NSAID delivery. Carbohydr. Polym. 2017, 156, 403–408. [Google Scholar] [CrossRef]
- Soriano-Ruiz, J.L.; Calpena-Campmany, A.C.; Silva-Abreu, M.; Halbout-Bellowa, L.; DE Febrer, N.B.; Rodríguez-Lagunas, M.J.; Clares-Naveros, B. Design and evaluation of a multifunctional thermosensitive poloxamer-chitosan-hyaluronic acid gel for the treatment of skin burns. Int. J. Biol. Macromol. 2020, 142, 412–422. [Google Scholar] [CrossRef]
- Cornell, J. Experiments with Mixtures: Designs, Models, and the Analysis of Mixture Data; J. Wiley & Sons: New York, NY, USA, 2002. [Google Scholar]
- Mura, P.; Mennini, N.; Nativi, C.; Richichi, B. In situ mucoadhesive-thermosensitive liposomal gel as a novel vehicle for nasal extended delivery of opiorphin. Eur. J. Pharm. Biopharm. 2018, 122, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Yong, C.S.; Choi, J.S.; Quan, Q.-Z.; Rhee, J.-D.; Kim, C.-K.; Lim, S.-J.; Kim, K.-M.; Oh, P.-S.; Choi, H.-G. Effect of sodium chloride on the gelation temperature, gel strength and bioadhesive force of poloxamer gels containing diclofenac sodium. Int. J. Pharm. 2001, 226, 195–205. [Google Scholar] [CrossRef]
- Salade, L.; Wauthoz, N.; Goole, J.; Amighi, K. How to characterize a nasal product. The state of the art of in vitro and ex vivo specific methods. Int. J. Pharm. 2019, 561, 47–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Patil, K.; Bobade, N.; Yeole, P.; Gaikwad, R. Formulation of intranasal mucoadhesive temperature-mediated in situ gel containing ropinirole and evaluation of brain targeting efficiency in rats. J. Drug Target. 2010, 18, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Piazzini, V.; Rosseti, C.; Bigagli, E.; Luceri, C.; Bilia, A.R.; Bergonzi, M.C. Prediction of Permeation and Cellular Transport of Silybum marianum Extract Formulated in a Nanoemulsion by Using PAMPA and Caco-2 Cell Models. Planta Medica 2017, 83, 1184–1193. [Google Scholar] [CrossRef]
- Kemink, J.; Bergstrom, C.A.S. Caco-2 cell conditions enabling studies of drug absorption from digestible lipid-based formulations. Pharm. Res. 2018, 35, 74. [Google Scholar] [CrossRef] [Green Version]
- Godbole, M.D.; There, P.W.; Dangre, P.V. Formulation and optimization of prolonged release nasal in situ gel for treatment of migraine. Indo Am. J. Pharm. Res. 2014, 4, 1320–1332. [Google Scholar]
- England, R.J.A.; Homer, J.J.; Knight, L.C.; Ell, S.R. Nasal pH measurement: A reliable and repeatable parameter. Clin. Otolaryngol. 1999, 24, 67–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varshosaz, J.; Tabbakhian, M.; Salmani, Z. Designing of a Thermosensitive Chitosan/Poloxamer In Situ Gel for Ocular Delivery of Ciprofloxacin. Open Drug Deliv. J. 2008, 2, 61–70. [Google Scholar] [CrossRef]
- Bonacucina, G.; Spina, M.; Misici-Falzi, M.; Cespi, M.; Pucciarelli, S.; Angeletti, M.; Palmieri, G.F. Effect of hydroxypropyl β-cyclodextrin on the self-assembling and thermogelation properties of Poloxamer 407. Eur. J. Pharm. Sci. 2007, 32, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Gil Choi, S.; Lee, S.-E.; Kang, B.-S.; Ng, C.L.; Davaa, E.; Park, J.-S. Thermosensitive and Mucoadhesive Sol-Gel Composites of Paclitaxel/Dimethyl-β-Cyclodextrin for Buccal Delivery. PLoS ONE 2014, 9, e109090. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Shen, Y.; Wang, W.; Sun, C.; Li, C.; Xiong, Y.; Tu, J. Preparation and in vitro characterization of thermosensitive and mucoadhesive hydrogels for nasal delivery of phenylephrine hydrochloride. Eur. J. Pharm. Biopharm. 2014, 88, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Maggio, E.T. Absorption enhancing excipients in systemic nasal drug delivery. J. Excipients Food Chem. 2014, 5, 100–112. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exp. No | PLX % w/v | HA % w/v | RAMEB % w/v | Chito Gl % w/v | Gel. T °C | Gel Time s | pH |
|---|---|---|---|---|---|---|---|
| 1 | 20 | 0 | 3 | 0.1 | 32.0 | 72 | 5.68 |
| 2 | 24 | 0 | 3 | 0.1 | 28.0 | 43 | 5.53 |
| 3 | 20 | 0 | 5 | 0.1 | 31.0 | 97 | 5.29 |
| 4 | 24 | 0 | 5 | 0.1 | 29.0 | 55 | 5.22 |
| 5 | 20 | 0.50 | 3 | 0.1 | 32.0 | 55 | 6.35 |
| 6 | 24 | 0.50 | 3 | 0.1 | 28.0 | 30 | 6.43 |
| 7 | 20 | 0.50 | 5 | 0.1 | 31.0 | 60 | 6.43 |
| 8 | 24 | 0.50 | 5 | 0.1 | 29.0 | 31 | 6.53 |
| 9 | 22 | 0.25 | 4 | 0.1 | 30.0 | 74 | 6.24 |
| 10 | 22 | 0.25 | 4 | 0.1 | 29.5 | 73 | 6.10 |
| 11 | 22 | 0.25 | 4 | 0.1 | 29.5 | 77 | 6.30 |
| Batch Code | PLX (% w/v) | HA (% w/v) | Chito Gl (% w/v) | RAMEB (% w/v) | CLZ (% w/v) |
|---|---|---|---|---|---|
| G1 | 22 | 0.25 | 0.1 | 3 | 0.060 |
| G2 | 22 | 0.25 | 0.1 | 3 | / |
| G3 | 22 | 0.25 | 0.1 | 4 | 0.080 |
| G4 | 22 | 0.25 | 0.1 | 4 | / |
| G5 | 22 | 0.25 | 0.1 | 5 | 0.095 |
| G6 | 22 | 0.25 | 0.1 | 5 | / |
| G0 | 22 | / | / | / | / |
| G0A | 22 | 0.25 | / | / | / |
| G0B | 22 | / | 0.1 | / | / |
| G0AB | 22 | 0.25 | 0.1 | / | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirri, M.; Maestrelli, F.; Nerli, G.; Mennini, N.; D’Ambrosio, M.; Luceri, C.; Mura, P.A. Development of a Cyclodextrin-Based Mucoadhesive-Thermosensitive In Situ Gel for Clonazepam Intranasal Delivery. Pharmaceutics 2021, 13, 969. https://doi.org/10.3390/pharmaceutics13070969
Cirri M, Maestrelli F, Nerli G, Mennini N, D’Ambrosio M, Luceri C, Mura PA. Development of a Cyclodextrin-Based Mucoadhesive-Thermosensitive In Situ Gel for Clonazepam Intranasal Delivery. Pharmaceutics. 2021; 13(7):969. https://doi.org/10.3390/pharmaceutics13070969
Chicago/Turabian StyleCirri, Marzia, Francesca Maestrelli, Giulia Nerli, Natascia Mennini, Mario D’Ambrosio, Cristina Luceri, and Paola Angela Mura. 2021. "Development of a Cyclodextrin-Based Mucoadhesive-Thermosensitive In Situ Gel for Clonazepam Intranasal Delivery" Pharmaceutics 13, no. 7: 969. https://doi.org/10.3390/pharmaceutics13070969