
Sinonasal Stent Coated with Slow-Release Varnish of Chlorhexidine Has Sustained Protection against Bacterial Biofilm Growth in the Sinonasal Cavity: An In Vitro Study

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Sustained Release Varnish (SRV) Preparation
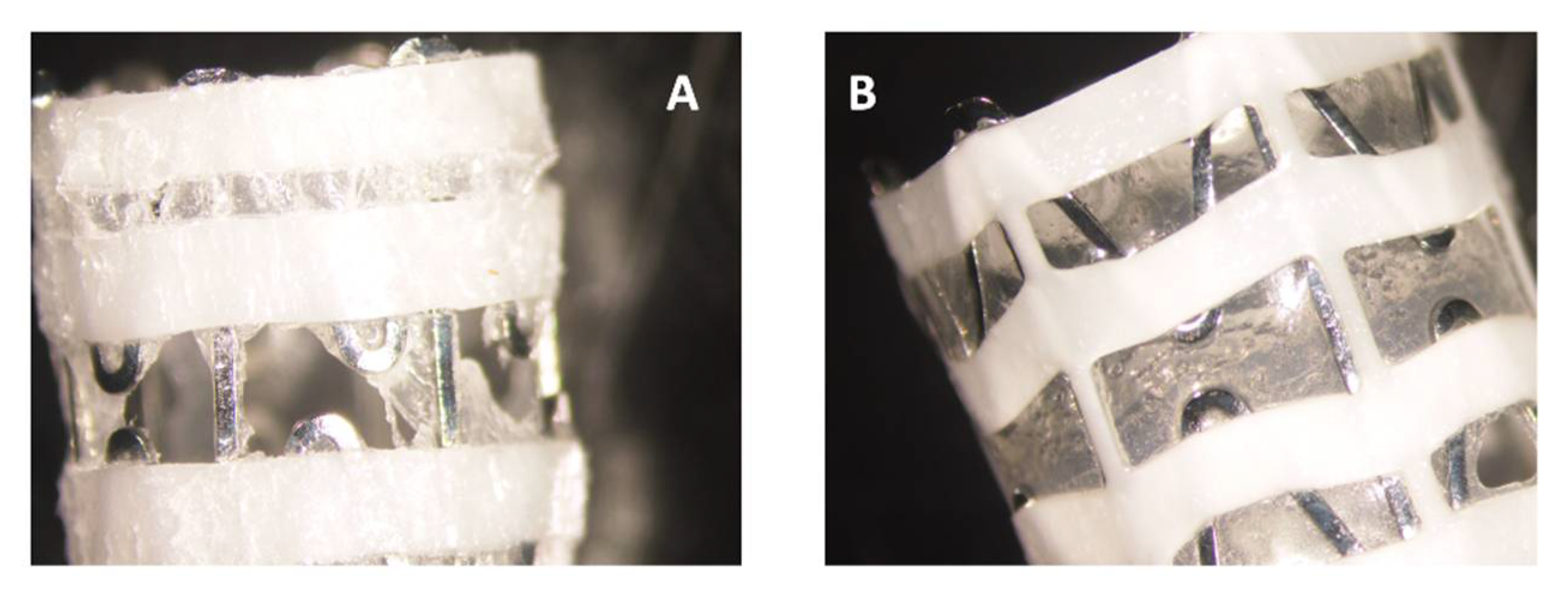
2.2. Coating of the Stents
2.3. Bacterial Strains
2.4. Agar Diffusion Sensitivity Assay
2.5. Planktonic Bacterial Growth and Biofilm Formation
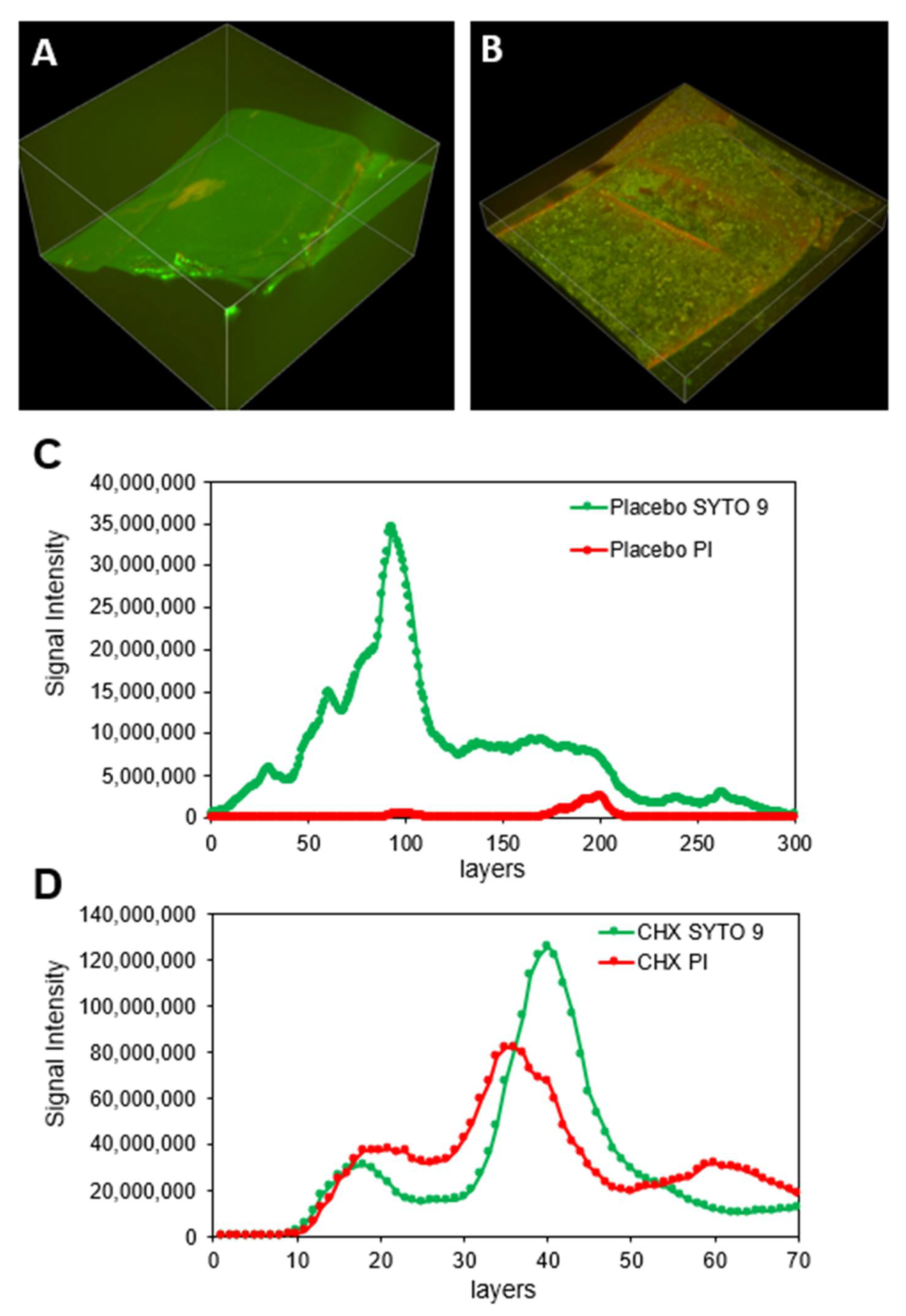
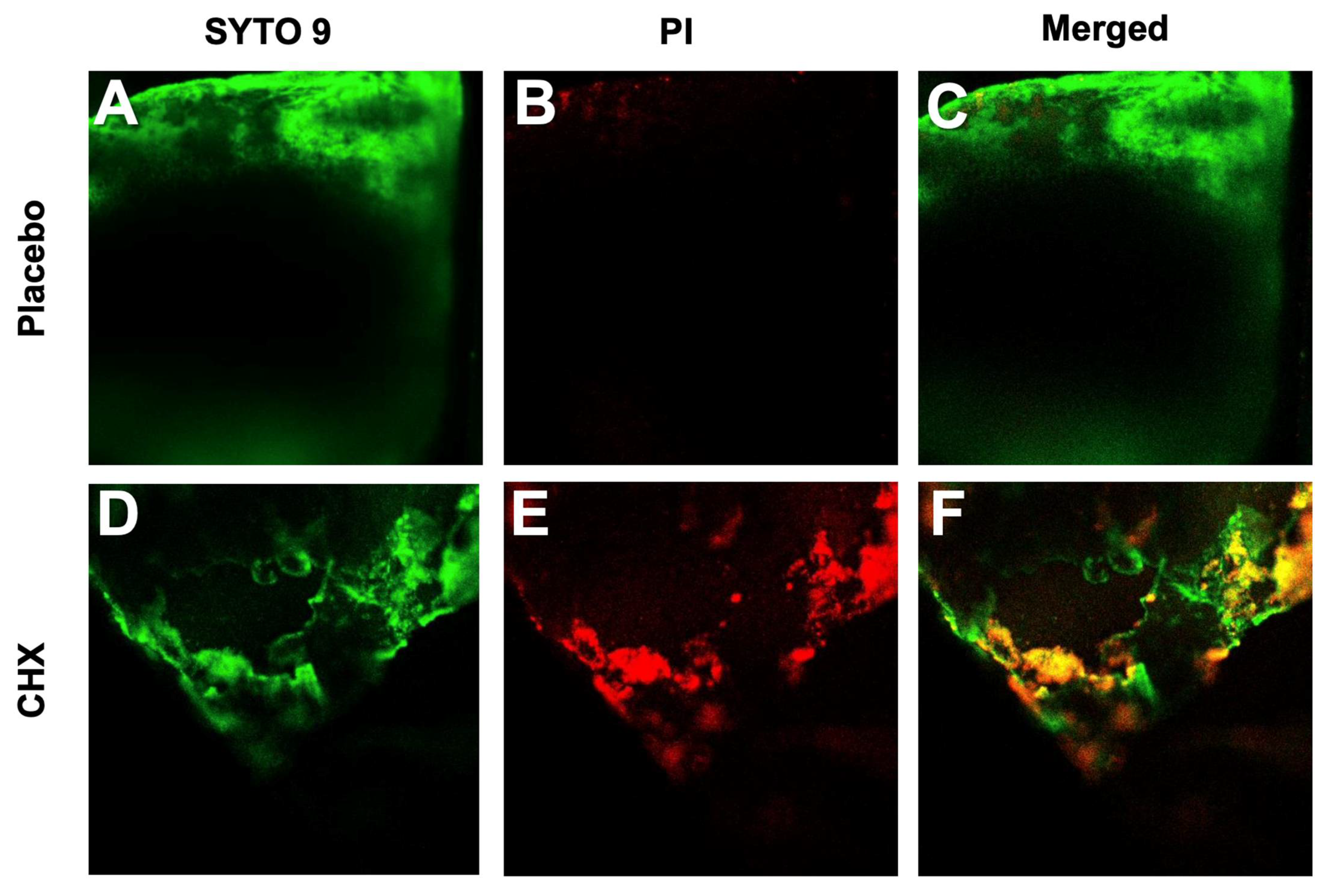
2.6. Evaluation of Biofilm Development by Confocal Laser Scanning Microscopy (CLSM)
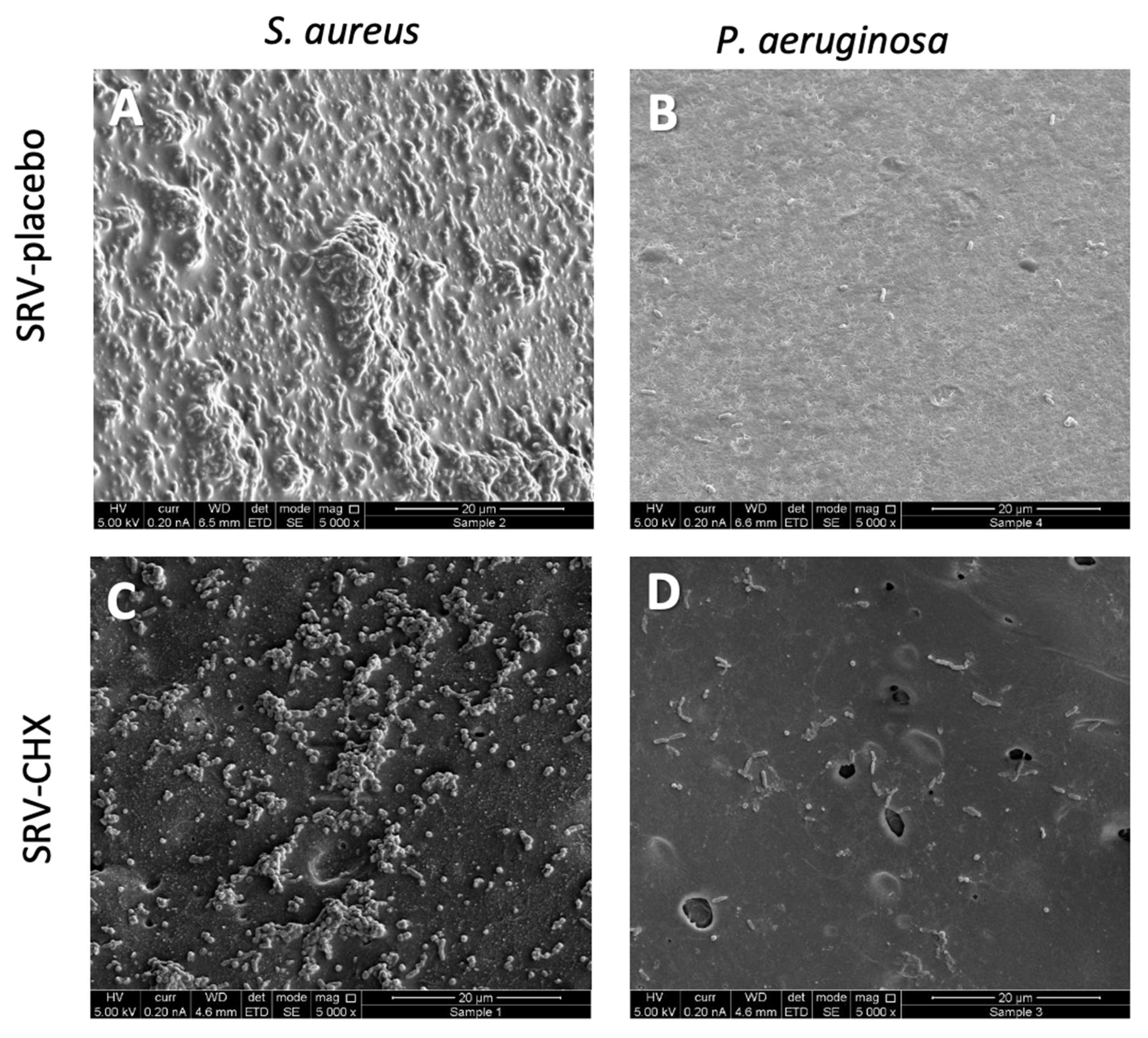
2.7. High-Resolution Scanning Electron Microscopy (HR-SEM)
2.8. Evaluation of Biofilm Metabolic Activity
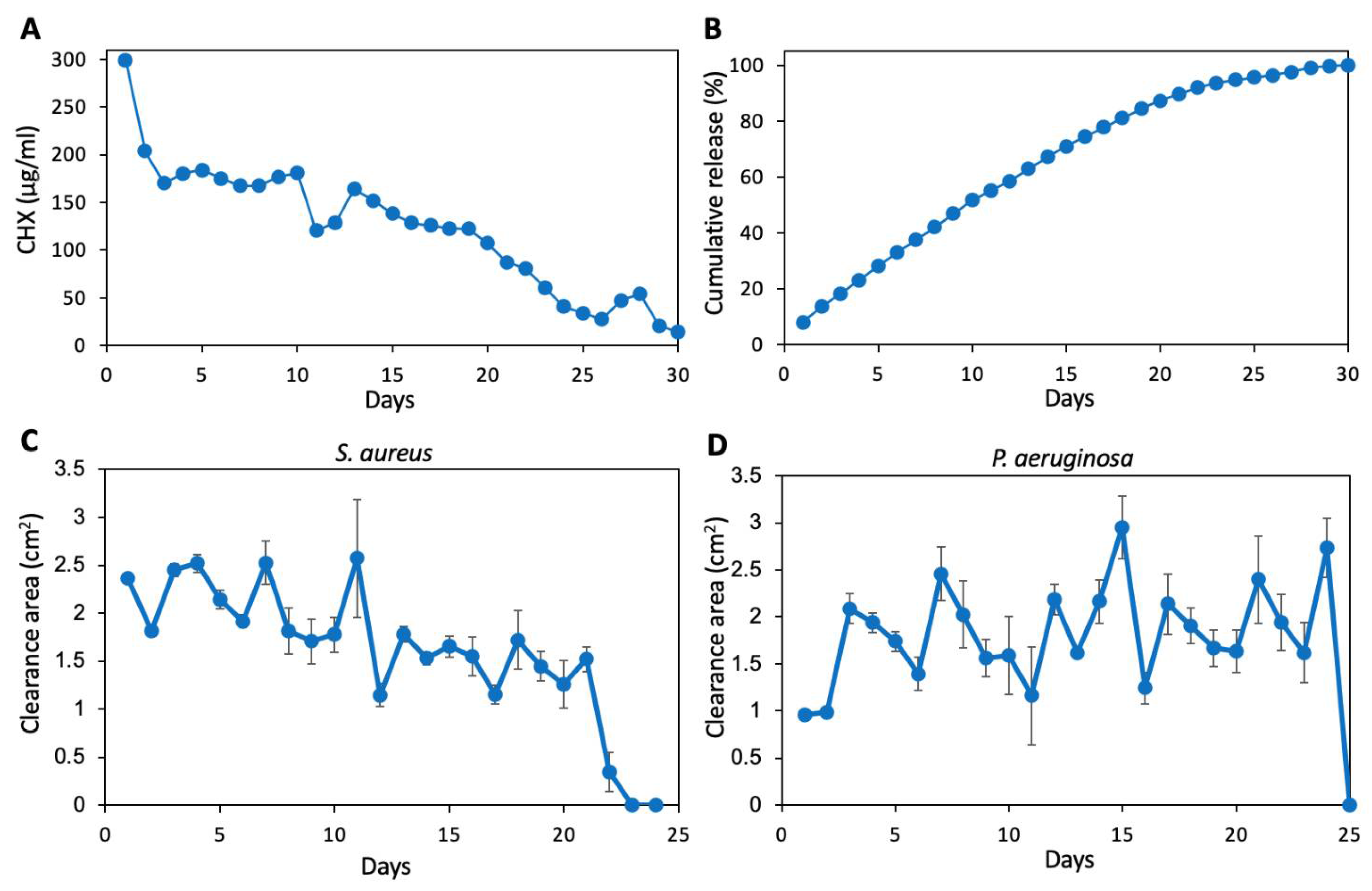
2.9. Determination of CHX Release from Coated SNS at pH 6
2.10. Statistical Analysis
3. Results
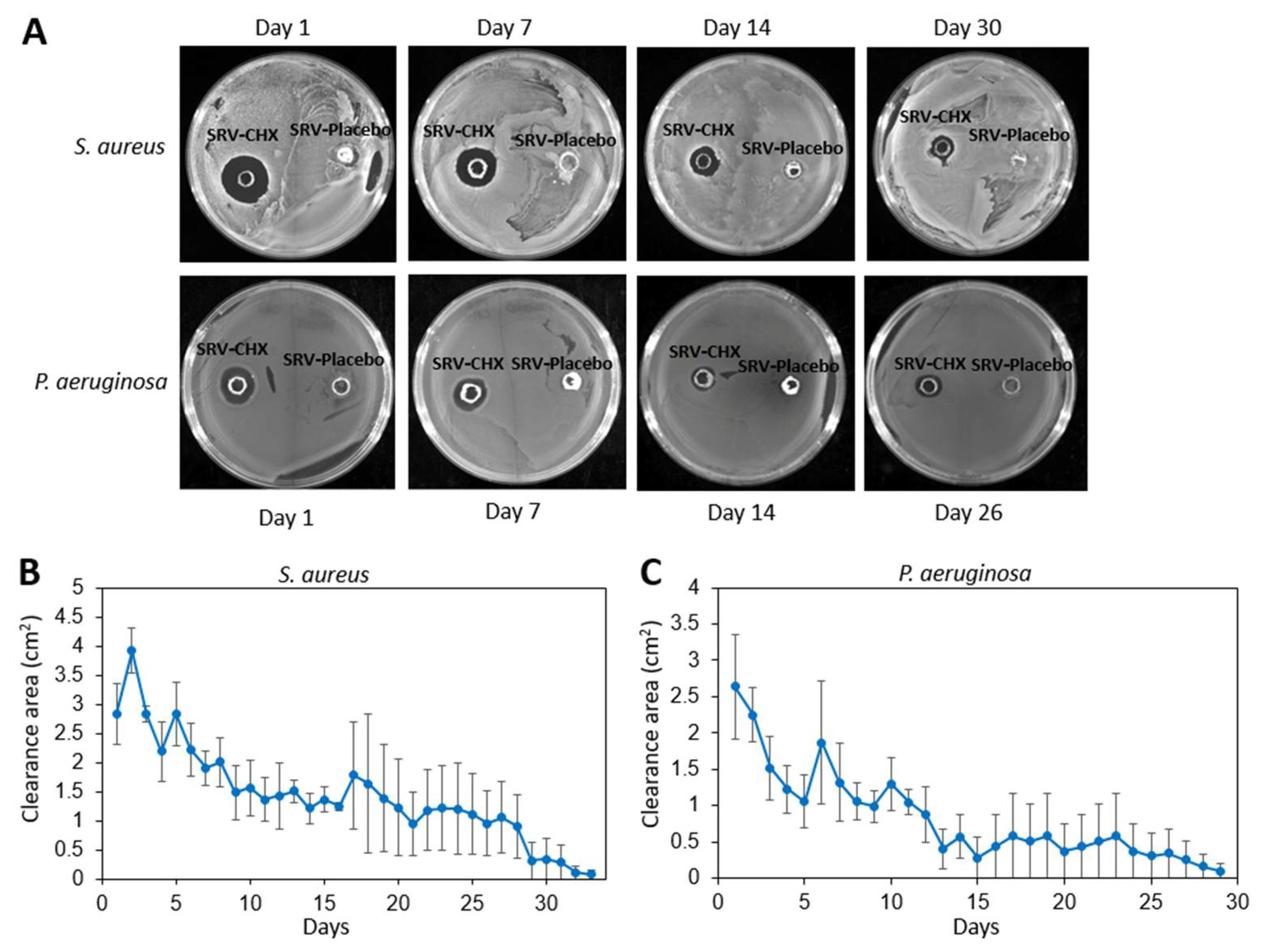
3.1. Agar Disk Diffusion Assay Shows the Prolonged Effect of SRV-CHX on Bacterial Clearance
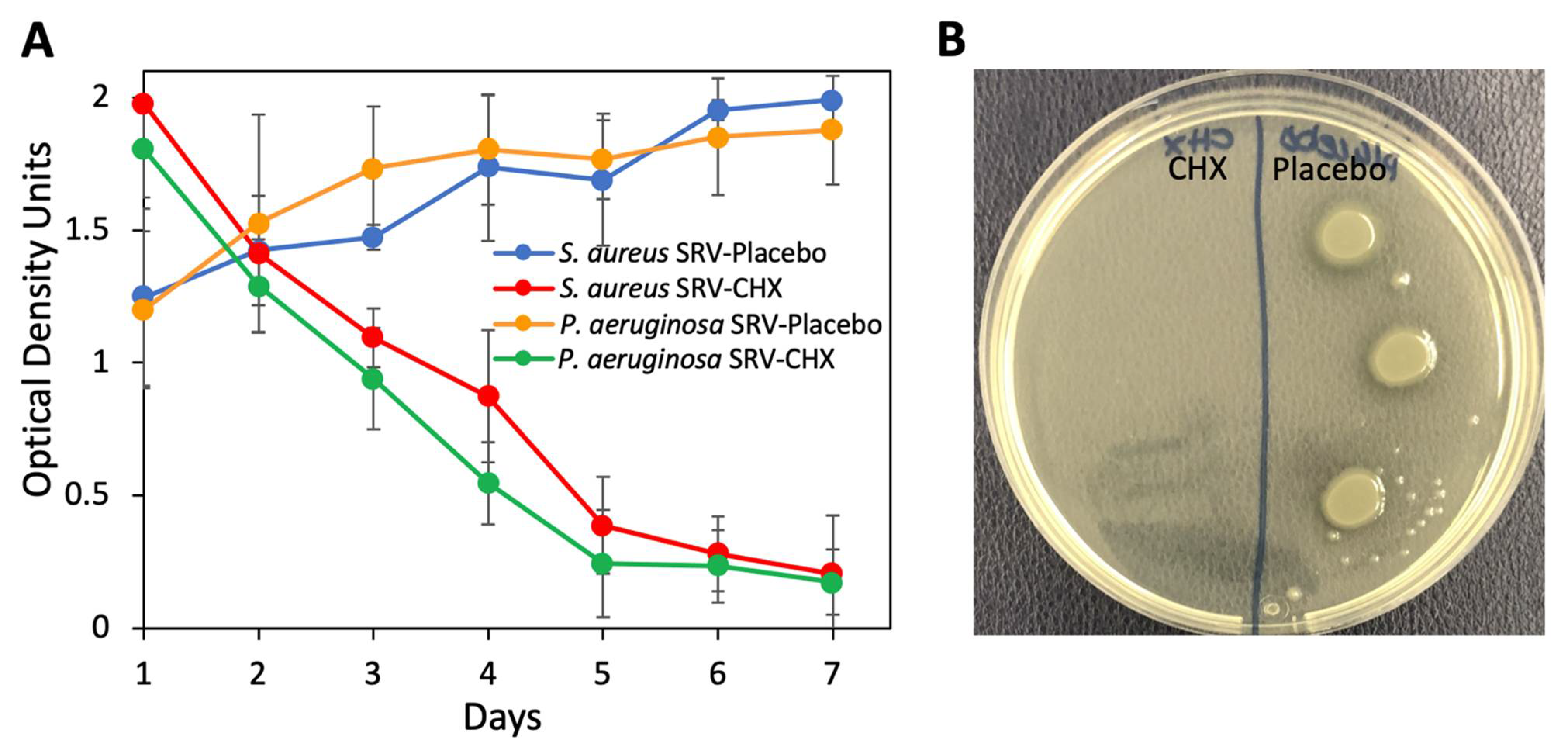
3.2. Antibacterial Effect of Coated Stent on Planktonic Bacterial Growth
3.3. Anti-Bacterial Activity of CHX Released from Coated Stent at pH 6
3.4. Reduced Biofilm Formation on SRV-CHX-Coated SNS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Rudmik, L. Economics of chronic rhinosinusitis. Curr. Allergy Asthma Rep. 2017, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Singhal, D.; Psaltis, A.J.; Foreman, A.; Wormald, P.J. The impact of biofilms on outcomes after endoscopic sinus surgery. Am. J. Rhinol. Allergy 2010, 24, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dong, D.; Cheng, J.; Fan, X.; Zhao, Y. Relationship between biofilms and clinical features in patients with sinus fungal ball. Eur. Arch. Otorhinolaryngol. 2015, 272, 2363–2369. [Google Scholar] [CrossRef]
- Głowacki, R.; Tomaszewski, K.A.; Stręk, P.; Tomaszewska, I.M.; Zgórska-Świerzy, K.; Markiewicz, B.; Składzień, J. The influence of bacterial biofilm on the clinical outcome of chronic rhinosinusitis: A prospective, double-blind, scanning electron microscopy study. Eur. Arch. Otorhinolaryngol. 2014, 271, 1015–1021. [Google Scholar] [CrossRef]
- Zhang, Z.; Adappa, N.D.; Chiu, A.G.; Doghramji, L.J.; Cohen, N.A.; Palmer, J.N. Biofilm-forming bacteria and quality of life improvement after sinus surgery. Int. Forum. Allergy Rhinol. 2015, 5, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Linkin, D.R.; Finkelman, B.S.; O’Malley, B.W., Jr.; Thaler, E.R.; Doghramji, L.; Kennedy, D.W.; Cohen, N.A.; Palmer, J.N. Asthma and biofilm-forming bacteria are independently associated with revision sinus surgeries for chronic rhinosinusitis. J. Allergy Clin. Immunol. 2011, 128, 221–223.e221. [Google Scholar] [CrossRef]
- Rather, M.A.; Gupta, K.; Mandal, M. Microbial biofilm: Formation, architecture, antibiotic resistance, and control strategies. Braz. J. Microbiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Tajudeen, B.A.; Schwartz, J.S.; Palmer, J.N. Understanding biofilms in chronic sinusitis. Curr. Allergy Asthma Rep. 2016, 16, 10. [Google Scholar] [CrossRef]
- Welp, A.L.; Bomberger, J.M. Bacterial community interactions during chronic respiratory disease. Front. Cell Infect. Microbiol. 2020, 10, 213. [Google Scholar] [CrossRef]
- Maina, I.W.; Patel, N.N.; Cohen, N.A. Understanding the role of biofilms and superantigens in chronic rhinosinusitis. Curr. Otorhinolaryngol. Rep. 2018, 6, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Dlugaszewska, J.; Leszczynska, M.; Lenkowski, M.; Tatarska, A.; Pastusiak, T.; Szyfter, W. The pathophysiological role of bacterial biofilms in chronic sinusitis. Eur. Arch. Otorhinolaryngol. 2016, 273, 1989–1994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foreman, A.; Psaltis, A.J.; Tan, L.W.; Wormald, P.J. Characterization of bacterial and fungal biofilms in chronic rhinosinusitis. Am. J. Rhinol. Allergy 2009, 23, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Prince, A.A.; Steiger, J.D.; Khalid, A.N.; Dogrhamji, L.; Reger, C.; Eau Claire, S.; Chiu, A.G.; Kennedy, D.W.; Palmer, J.N.; Cohen, N.A. Prevalence of biofilm-forming bacteria in chronic rhinosinusitis. Am. J. Rhinol. 2008, 22, 239–245. [Google Scholar] [CrossRef]
- Szaleniec, J.; Gibała, A.; Pobiega, M.; Parasion, S.; Składzień, J.; Stręk, P.; Gosiewski, T.; Szaleniec, M. Exacerbations of chronic rhinosinusitis-microbiology and perspectives of phage therapy. Antibiotics 2019, 8, 175. [Google Scholar] [CrossRef] [Green Version]
- Ezzat, W.F.; Fawaz, S.A.; Rabie, H.; Hamdy, T.A.; Shokry, Y.A. Effect of topical ofloxacin on bacterial biofilms in refractory post-sinus surgery rhino-sinusitis. Eur. Arch. Otorhinolaryngol. 2015, 272, 2355–2361. [Google Scholar] [CrossRef]
- Steinberg, D.; Friedman, M. Sustained-release drug delivery of antimicrobials in controlling of supragingival oral biofilms. Expert Opin. Drug Deliv. 2017, 14, 571–581. [Google Scholar] [CrossRef]
- Gefter Shenderovich, J.; Zaks, B.; Kirmayer, D.; Lavy, E.; Steinberg, D.; Friedman, M. Chlorhexidine sustained-release varnishes for catheter coating—Dissolution kinetics and antibiofilm properties. Eur. J. Pharm. Sci. 2018, 112, 1–7. [Google Scholar] [CrossRef]
- Segers, P.; Speekenbrink, R.G.; Ubbink, D.T.; van Ogtrop, M.L.; de Mol, B.A. Prevention of nosocomial infection in cardiac surgery by decontamination of the nasopharynx and oropharynx with chlorhexidine gluconate: A randomized controlled trial. JAMA 2006, 296, 2460–2466. [Google Scholar] [CrossRef]
- Steinberg, D.; Friedman, M. Development of sustained-release devices for modulation of dental plaque biofilm and treatment of oral infectious diseases. Drug Dev. Res. 2000, 50, 555–565. [Google Scholar] [CrossRef]
- Ben-Knaz Wakshlak, R.; Pedahzur, R.; Avnir, D. Antibacterial activity of chlorhexidine-killed bacteria: The zombie cell effect. ACS Omega 2019, 4, 20868–20872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grigor’eva, A.; Bardasheva, A.; Tupitsyna, A.; Amirkhanov, N.; Tikunova, N.; Pyshnyi, D.; Ryabchikova, E. Changes in the ultrastructure of staphylococcus aureus treated with cationic peptides and chlorhexidine. Microorganisms 2020, 8, 1991. [Google Scholar] [CrossRef] [PubMed]
- Strus, M.; Walczewska, M.; Machul, A.; Mikołajczyk, D.; Marcinkiewicz, J. Taurine haloamines and biofilm. Part I: Antimicrobial activity of taurine bromamine and chlorhexidine against biofilm forming Pseudomonas aeruginosa. Adv. Exp. Med. Biol. 2015, 803, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Alvendal, C.; Mohanty, S.; Bohm-Starke, N.; Brauner, A. Anti-biofilm activity of chlorhexidine digluconate against Candida albicans vaginal isolates. PLoS ONE 2020, 15, e0238428. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhou, B.; Wang, D.; Zang, H.; Zhang, H.; Wang, H.; Wang, S.; Cheng, L.; Li, J.; Wu, W.; et al. Comparison of bioabsorbable steroid-eluting sinus stents versus nasopore after endoscopic sinus surgery: A multicenter, randomized, controlled, single-blinded clinical trial. Ear. Nose Throat J. 2020, 1–8. [Google Scholar] [CrossRef]
- Duanis-Assaf, D.; Kenan, E.; Sionov, R.; Steinberg, D.; Shemesh, M. Proteolytic activity of Bacillus subtilis upon κ-Casein undermines its “caries-safe” effect. Microorganisms 2020, 8, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, M.; Shenderovich, J.; Lavy, E.; Friedman, M.; Steinberg, D. A sustained-release membrane of thiazolidinedione-8: Effect on formation of a Candida/bacteria mixed biofilm on hydroxyapatite in a continuous flow model. Biomed. Res. Int. 2017, 2017, 3510124. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.G.; Kim, J.H.; Kim, S.W.; Kim, S.W.; Jin, K.S.; Cho, J.H.; Kang, J.M.; Park, S.Y. Nasal pH in patients with chronic rhinosinusitis before and after endoscopic sinus surgery. Am. J. Otolaryngol. 2013, 34, 505–507. [Google Scholar] [CrossRef]
- Varoni, E.; Tarce, M.; Lodi, G.; Carrassi, A. Chlorhexidine (CHX) in dentistry: State of the art. Minerva Stomatol. 2012, 61, 399–419. [Google Scholar]
- Bendouah, Z.; Barbeau, J.; Hamad, W.A.; Desrosiers, M. Biofilm formation by Staphylococcus aureus and Pseudomonas aeruginosa is associated with an unfavorable evolution after surgery for chronic sinusitis and nasal polyposis. Otolaryngol. Head Neck Surg. 2006, 134, 991–996. [Google Scholar] [CrossRef]
- Friedman, M.; Golomb, G. New sustained release dosage form of chlorhexidine for dental use. I. Development and kinetics of release. J. Periodontal. Res. 1982, 17, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Cankaya, H.; Ozen, S.; Kiroğlu, F.; Yurttaş, V. Effects of topical chlorhexidine applied to the rabbit nasal mucosa. Auris Nasus Larynx 2003, 30, 65–69. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cataldo Russomando, A.; Vogt Sionov, R.; Friedman, M.; Gati, I.; Eliashar, R.; Steinberg, D.; Gross, M. Sinonasal Stent Coated with Slow-Release Varnish of Chlorhexidine Has Sustained Protection against Bacterial Biofilm Growth in the Sinonasal Cavity: An In Vitro Study. Pharmaceutics 2021, 13, 1783. https://doi.org/10.3390/pharmaceutics13111783
Cataldo Russomando A, Vogt Sionov R, Friedman M, Gati I, Eliashar R, Steinberg D, Gross M. Sinonasal Stent Coated with Slow-Release Varnish of Chlorhexidine Has Sustained Protection against Bacterial Biofilm Growth in the Sinonasal Cavity: An In Vitro Study. Pharmaceutics. 2021; 13(11):1783. https://doi.org/10.3390/pharmaceutics13111783
Chicago/Turabian StyleCataldo Russomando, Alessandra, Ronit Vogt Sionov, Michael Friedman, Irith Gati, Ron Eliashar, Doron Steinberg, and Menachem Gross. 2021. "Sinonasal Stent Coated with Slow-Release Varnish of Chlorhexidine Has Sustained Protection against Bacterial Biofilm Growth in the Sinonasal Cavity: An In Vitro Study" Pharmaceutics 13, no. 11: 1783. https://doi.org/10.3390/pharmaceutics13111783