
Early Effects of Low Molecular Weight Heparin Therapy with Soft-Mist Inhaler for COVID-19-Induced Hypoxemia: A Phase IIb Trial

 , ,
, ,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
- i.
- To alleviate COVID-19-induced hypoxemia and improve patient respiratory capacity.
- ii.
- To reduce the death toll by hypoxemia to the lowest possible level.
- iii.
- To eliminate the side effects associated with the current protocols.
- iv.
- To reduce intubation rates.
- v.
- To improve clinical care capability and reduce cross-contamination risk to health personnel.
- vi.
- To achieve the highest drug concentration in lungs [20].
2. Materials and Methods
2.1. Material
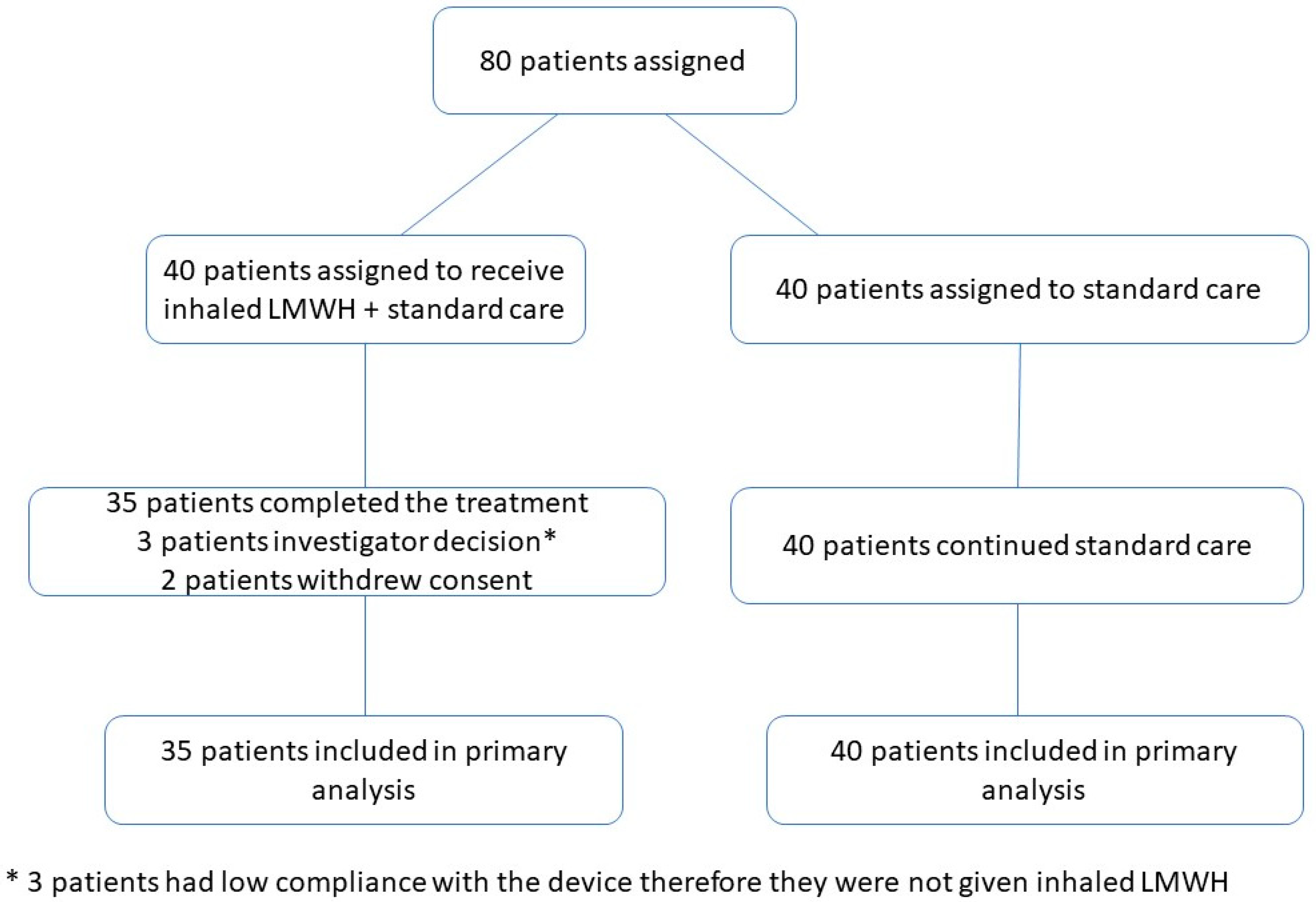
2.2. Clinical Study Design and Patients
2.3. Outcomes
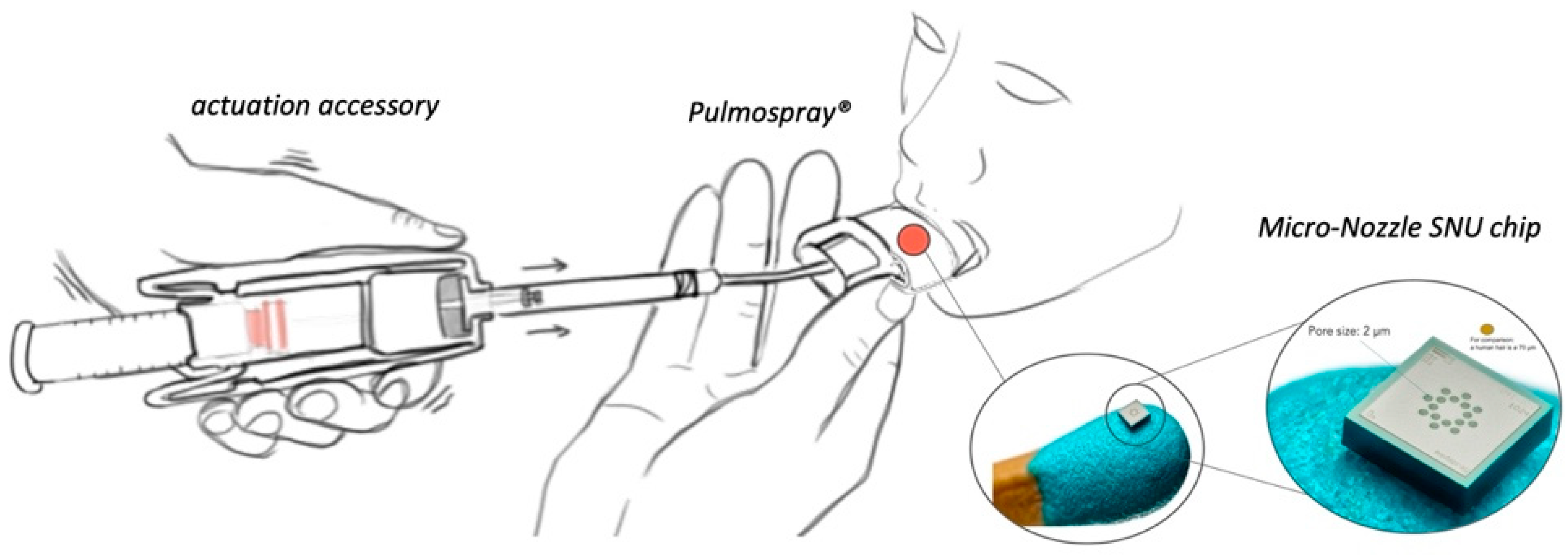
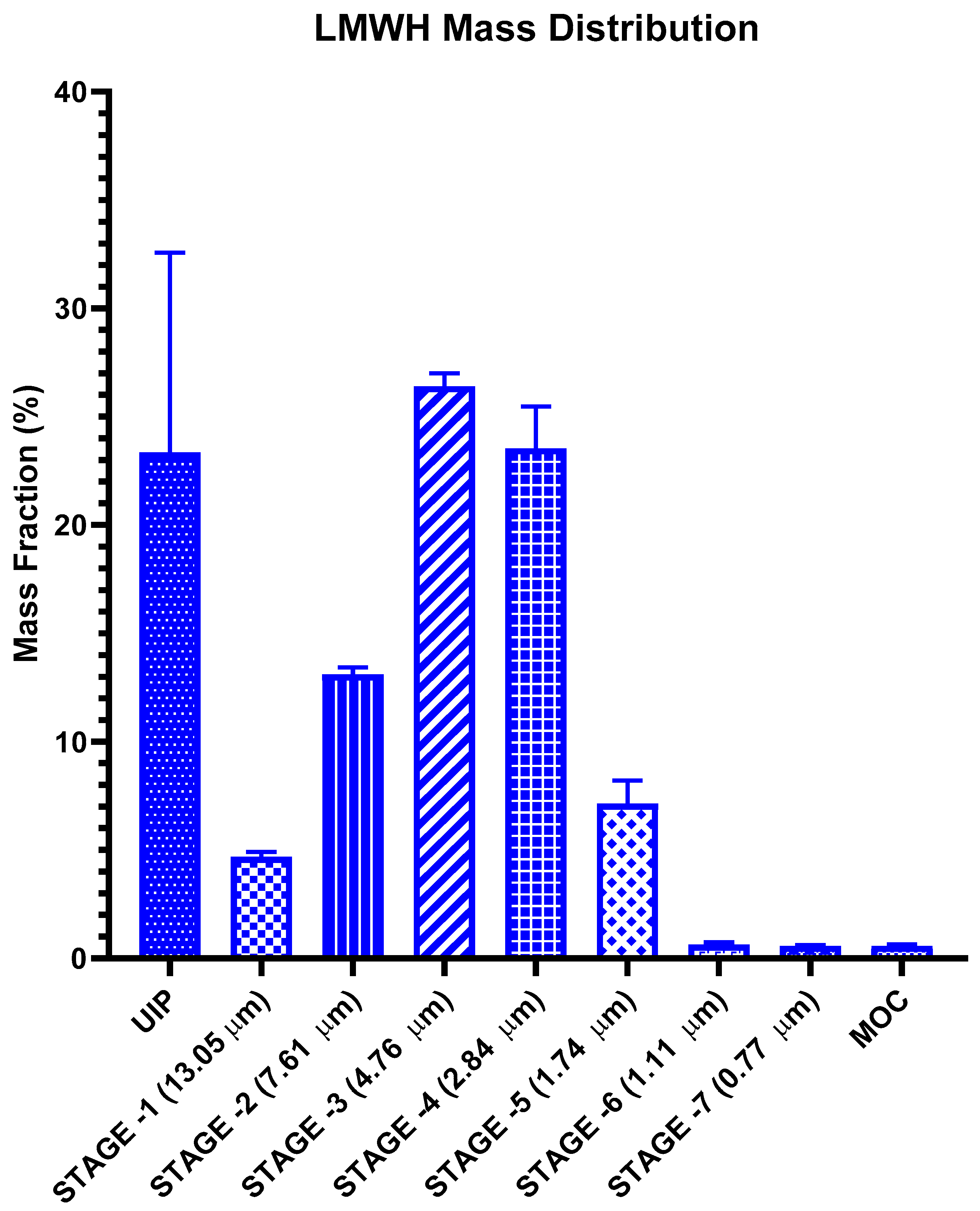
2.4. Mechanism and In Vitro Lung Deposition Studies of Pulmospray®
2.5. Data and Statistical Analysis
3. Results
3.1. Clinical Study Results
3.2. In Vitro Lung Deposition Study Results
4. Discussion
- (1)
- This study focused on LMWH to eliminate the need for mechanical ventilation by pro-actively curing hypoxemia itself.
- (2)
- The specifically designed device of delivery met the mechanical requirements for targeted delivery with the highest retention rate.
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Wang, C.; Wang, Z.; Wang, G.; Lau, J.Y.-N.; Zhang, K.; Li, W. COVID-19 in Early 2021: Current Status and Looking Forward. Signal Transduct. Target. Ther. 2021, 6, 1–14. [Google Scholar] [CrossRef]
- van Haren, F.M.P.; Richardson, A.; Yoon, H.; Artigas, A.; Laffey, J.G.; Dixon, B.; Smith, R.; Vilaseca, A.B.; Barbera, R.A.; Ismail, T.I.; et al. INHALEd Nebulised Unfractionated HEParin for the Treatment of Hospitalised Patients with COVID-19 (INHALE-HEP): Protocol and Statistical Analysis Plan for an Investigator-initiated International Metatrial of Randomised Studies. Br. J. Clin. Pharmacol. 2021, 87, 3075–3091. [Google Scholar] [CrossRef]
- Xie, J.; Covassin, N.; Fan, Z.; Singh, P.; Gao, W.; Li, G.; Kara, T.; Somers, V.K. Association Between Hypoxemia and Mortality in Patients with COVID-19. Mayo Clin. Proc. 2020, 95, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Dhont, S.; Derom, E.; Van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The Pathophysiology of ‘Happy’ Hypoxemia in COVID-19. Respir. Res. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Navas-Blanco, J.R.; Dudaryk, R. Management of Respiratory Distress Syndrome Due to COVID-19 Infection. BMC Anesthesiol. 2020, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Tingting, W.; Li, J.; Sullivan, M.A.; Wang, C.; Wang, H.; Deng, B.; Zhang, Y. Comprehensive Landscape of Heparin Therapy for COVID-19. Carbohydr. Polym. 2021, 254, 1–10. [Google Scholar] [CrossRef]
- Mishra, G.P.; Mulani, J. Corticosteroids for COVID-19: The Search for an Optimum Duration of Therapy. Lancet Respir. Med. 2021, 9, e8. [Google Scholar] [CrossRef]
- Vicenzi, E.; Canducci, F.; Pinna, D.; Mancini, N.; Carletti, S.; Lazzarin, A.; Bordignon, C.; Poli, G.; Clementi, M. Coronaviridae and SARS-Associated Coronavirus Strain HSR1. Emerg. Infect. Dis. 2004, 10, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, J.; Yang, N.; Deng, J.; Liu, K.; Yang, P.; Zhang, G.; Jiang, C. Inhibition of SARS Pseudovirus Cell Entry by Lactoferrin Binding to Heparan Sulfate Proteoglycans. PLoS ONE 2011, 6, e23710. [Google Scholar] [CrossRef]
- Ghezzi, S.; Cooper, L.; Rubio, A.; Pagani, I.; Capobianchi, M.R.; Ippolito, G.; Pelletier, J.; Meneghetti, M.C.Z.; Lima, M.A.; Skidmore, M.A.; et al. Heparin Prevents Zika Virus Induced-Cytopathic Effects in Human Neural Progenitor Cells. Antivir. Res. 2017, 140, 13–17. [Google Scholar] [CrossRef] [Green Version]
- WuDunn, D.; Spear, P.G. Initial Interaction of Herpes Simplex Virus with Cells Is Binding to Heparan Sulfate. J. Virol. 1989, 63, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Skidmore, M.A.; Kajaste-Rudnitski, A.; Wells, N.M.; Guimond, S.E.; Rudd, T.R.; Yates, E.A.; Vicenzi, E. Inhibition of Influenza H5N1 Invasion by Modified Heparin Derivatives. Med. Chem. Commun. 2015, 6, 640–646. [Google Scholar] [CrossRef]
- Harrop, H.A.; Rider, C.C. Heparin and Its Derivatives Bind to HIV-1 Recombinant Envelope Glycoproteins, Rather than to Recombinant HIV-1 Receptor, CD4. Glycobiology 1998, 8, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Rusnati, M.; Coltrini, D.; Oreste, P.; Zoppetti, G.; Albini, A.; Noonan, D.; d’Adda di Fagagna, F.; Giacca, M.; Presta, M. Interaction of HIV-1 Tat Protein with Heparin. J. Biol. Chem. 1997, 272, 11313–11320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mycroft-West, C.J.; Su, D.; Pagani, I.; Rudd, T.R.; Elli, S.; Gandhi, N.S.; Guimond, S.E.; Miller, G.J.; Meneghetti, M.C.Z.; Nader, H.B.; et al. Heparin Inhibits Cellular Invasion by SARS-CoV-2: Structural Dependence of the Interaction of the Spike S1 Receptor-Binding Domain with Heparin. Thromb. Haemost. 2020, 120, 1700–1715. [Google Scholar] [CrossRef]
- Hippensteel, J.A.; LaRiviere, W.B.; Colbert, J.F.; Langouët-Astrié, C.J.; Schmidt, E.P. Heparin as a Therapy for COVID-19: Current Evidence and Future Possibilities. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2020, 319, L211–L217. [Google Scholar] [CrossRef]
- Tandon, R.; Sharp, J.S.; Zhang, F.; Pomin, V.H.; Ashpole, N.M.; Mitra, D.; McCandless, M.G.; Jin, W.; Liu, H.; Sharma, P.; et al. Effective Inhibition of SARS-CoV-2 Entry by Heparin and Enoxaparin Derivatives. J. Virol. 2021, 95, e01987-20. [Google Scholar] [CrossRef] [PubMed]
- Billett, H.H.; Reyes-Gil, M.; Szymanski, J.; Ikemura, K.; Stahl, L.R.; Lo, Y.; Rahman, S.; Gonzalez-Lugo, J.D.; Kushnir, M.; Barouqa, M.; et al. Anticoagulation in COVID-19: Effect of Enoxaparin, Heparin, and Apixaban on Mortality. Thromb. Haemost. 2020, 120, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
- Conzelmann, C.; Müller, J.A.; Perkhofer, L.; Sparrer, K.M.J.; Zelikin, A.N.; Münch, J.; Kleger, A. Inhaled and Systemic Heparin as a Repurposed Direct Antiviral Drug for Prevention and Treatment of COVID-19. Clin. Med. J. R. Coll. Physicians Lond. 2020, 20, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Labiris, N.R.; Dolovich, M.B. Pulmonary Drug Delivery. Part I: Physiological Factors Affecting Therapeutic Effectiveness of Aerosolized Medications. J. Clin. Pharmacol. 2003, 56, 588–599. [Google Scholar] [CrossRef]
- Yildiz-Pekoz, A.; Ozsoy, Y. Inhaled Heparin: Therapeutic Efficacy and Recent Formulations. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Chow, S.-C.; Wang, H.; Shao, J. Sample Size Calculations in Clinical Research, 2nd ed.; Chow, S.-C., Jones, B., Liu, J., Peace, K.E., Eds.; Chapman and Hall/CRC: New York, NY, USA, 2008; Volume 64, p. 89. ISBN 9780898716252. [Google Scholar]
- Republic of Turkey Ministry of Health. Covid-19 Adult Treatment Guideline. Available online: https://covid19.saglik.gov.tr/Eklenti/40719/0/covid-19rehberieriskinhastayonetimivetedavipdf.pdf (accessed on 14 October 2021).
- Wachtel, H.; Kattenbeck, S.; Dunne, S.; Disse, B. The Respimat® Development Story: Patient-Centered Innovation. Pulm. Ther. 2017, 3, 19–30. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines and Healthcare (EDQM). Section 2.9.18—Preparations for inhalation: Aerodynamic assessment of fine particles. In European Pharmacopeia; Council of Europe: Strasbourg, France, 2009. [Google Scholar]
- Dixon, B.; Schultz, M.J.; Hofstra, J.J.; Campbell, D.J.; Santamaria, J.D. Nebulized Heparin Reduces Levels of Pulmonary Coagulation Activation in Acute Lung Injury. Crit. Care 2010, 14, 445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuinman, P.R.; Dixon, B.; Levi, M.; Juffermans, N.P.; Schultz, M.J. Nebulized Anticoagulants for Acute Lung Injury—A Systematic Review of Preclinical and Clinical Investigations. Crit. Care 2012, 16, R70. [Google Scholar] [CrossRef] [Green Version]
- Guan, M.; Zeng, X.; Shi, R.; Zheng, Y.; Fan, W.; Su, W. Aerosolization Performance, Antitussive Effect and Local Toxicity of Naringenin-Hydroxypropyl-β-Cyclodextrin Inhalation Solution for Pulmonary Delivery. AAPS PharmSciTech 2021, 22, 20. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin Definition of ARDS: An Expanded Rationale, Justification, and Supplementary Material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef]
- Matthay, M.A.; Thompson, B.T.; Ware, L.B. The Berlin Definition of Acute Respiratory Distress Syndrome: Should Patients Receiving High-Flow Nasal Oxygen Be Included? Lancet Respir. Med. 2021, 2600, 26–29. [Google Scholar] [CrossRef]
- Máca, J.; Jor, O.; Holub, M.; Sklienka, P.; Burša, F.; Burda, M.; Janout, V.; Ševčík, P. Past and Present ARDS Mortality Rates: A Systematic Review. Respir. Care 2017, 62, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Dixon, B.; Smith, R.J.; Campbell, D.J.; Moran, J.L.; Doig, G.S.; Rechnitzer, T.; MacIsaac, C.M.; Simpson, N.; van Haren, F.M.P.; Ghosh, A.N.; et al. Nebulised Heparin for Patients with or at Risk of Acute Respiratory Distress Syndrome: A Multicentre, Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet Respir. Med. 2021, 9, 360–372. [Google Scholar] [CrossRef]
- Leiner, S.; Cipolla, D.; Eicher, J.; De Kruijf, W.; Wachtel, H. Soft Mist Sprays. In Pharmaceutical Inhalation Aerosol Technology; Hickey, A.J., da Rocha, S.R., Eds.; CRC Press: Boca Raton, FL, USA, 2017; Volume 35. [Google Scholar]
- Newman, S.P. AEROSOLS. In Encyclopedia of Respiratory Medicine; Laurent, G.J., Shapiro, S.D., Eds.; Academic Press Elsevier: New York, NY, USA, 2006; ISBN 9780123864543. [Google Scholar]
- ClinicalTrials.gov Search of: Heparin|Covid19-List Results. Available online: https://clinicaltrials.gov/ct2/results?cond=Covid19&term=heparin&cntry=&state=&city=&dist= (accessed on 26 August 2021).
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant Treatment Is Associated with Decreased Mortality in Severe Coronavirus Disease 2019 Patients with Coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Buijsers, B.; Yanginlar, C.; Maciej-Hulme, M.L.; de Mast, Q.; van der Vlag, J. Beneficial Non-Anticoagulant Mechanisms Underlying Heparin Treatment of COVID-19 Patients. EBioMedicine 2020, 59, 1–6. [Google Scholar] [CrossRef]
- Young, E. The Anti-Inflammatory Effects of Heparin and Related Compounds. Thromb. Res. 2008, 122, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Buijsers, B.; Yanginlar, C.; de Nooijer, A.; Grondman, I.; Maciej-Hulme, M.L.; Jonkman, I.; Janssen, N.A.F.; Rother, N.; de Graaf, M.; Pickkers, P.; et al. Increased Plasma Heparanase Activity in COVID-19 Patients. Front. Immunol. 2020, 11, 2572. [Google Scholar] [CrossRef] [PubMed]
- LaRivière, W.B.; Schmidt, E.P. The Pulmonary Endothelial Glycocalyx in ARDS: A Critical Role for Heparan Sulfate. In Current Topics in Membranes; Elsevier Inc.: Philadelphia, PA, USA, 2018; Volume 82, ISBN 9780128158067. [Google Scholar]
- Wang, F.; Zhang, N.; Li, B.; Liu, L.; Ding, L.; Wang, Y.; Zhu, Y.; Mo, X.; Cao, Q. Heparin Defends against the Toxicity of Circulating Histones in Sepsis. Front. Biosci. 2015, 20, 1259–1270. [Google Scholar] [CrossRef] [Green Version]
- Zhu, C.; Liang, Y.; Li, X.; Chen, N.; Ma, X. Unfractionated Heparin Attenuates Histone-Mediated Cytotoxicity in Vitro and Prevents Intestinal Microcirculatory Dysfunction in Histone-Infused Rats. J. Trauma Acute Care Surg. 2019, 87, 614–622. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Written Informed Consent |
| Positive RT-PCR 1 test of nasopharyngeal swab for COVID- 19, and pneumonia confirmed by a CT 2. | |
| Negative RT-PCR test of nasopharyngeal swab for COVID- 19, but radiological and biochemical examinations unambiguously suggest COVID-19, when other possible diagnoses have been excluded. | |
| Exclusion Criteria | Patients who are pregnant |
| History of heparin and associated drug allergies |
| Severity Level | Definition |
|---|---|
| 0: Room Air | If the patient can breathe comfortably in room air. |
| 1: Nasal Cannula | If peripheral oxygen saturation improves with an oxygen therapy up to 6 L/min via nasal cannula. |
| 2: Reservoir Oxygen Mask | If condition can be improved with a 500 mL reservoir oxygen mask with 15 L/min oxygen treatment. |
| 3: High Flow Oxygen | If condition can be improved with high flow oxygen therapy. |
| 4: Intubation | If the intubation is the only choice. |
| Degree of Severity | Definition |
|---|---|
| 1 | One lobe less than 25% of lobe area |
| 2 | One lobe more than 25% of lobe area |
| 3 | Unilateral and less than one lobe less than 25% of each lobe area |
| 4 | Unilateral and more than one lobe less than 25% of each lobe area |
| 5 | Bilateral patch lesions on all lobes |
| 6 | Bilateral, all of one but not all lobes |
| 7 | Bilateral, all lobes, diffuse but less than 25% of each lobe area |
| 8 | Bilateral, all lobes, diffuse and 25–50% of each lobe area |
| 9 | Bilateral, all lobes, diffuse and 50–75% of each lobe area |
| 10 | Bilateral, all lobes, diffuse and more than 75% of each lobe area |
| Characteristics | Device Group | Control Group |
|---|---|---|
| Demographics | ||
| Age (y) | 60.02 ± 10.04 | 59.62 ± 14.60 |
| n = 35 | n = 40 | |
| Female | n = 15 (43.0%) | n = 15 (37.5%) |
| Male | n = 20 (57.0%) | n = 25 (62.5%) |
| Body Mass Index (kg/m2) | 29.3 ± 4.5 | 30.4 ± 5.1 |
| n = 35 | n= 40 | |
| Co-Morbidities | ||
| Tobacco Smoking | n = 3 (8.5%) | n = 6 (15.0%) |
| COPD 1 | n = 3 (8.5%) | n = 2 (5.0%) |
| Cardiac Disease | n = 7 (20.0%) | n = 9 (22.5%) |
| Diabetes Mellitus | n = 8 (22.8%) | n = 10 (25.0%) |
| Hypertension | n = 11 (31.4%) | n = 18 (45.0%) |
| Patient Parameters | Device Group | Control Group | p Value | |
|---|---|---|---|---|
| Symptom Distribution n (%) | Cough | 25 (71.4%) | 27 (67.5%) | p > 0.05 |
| Mucus | 10 (28. 5%) | 1 (2.5%) | p < 0.01 | |
| Dyspnea | 32 (91.4%) | 23(57.5%) | p < 0.01 | |
| Hypoxemia | Hypoxemic | 33 (94.3%) | 11 (27.5%) | p < 0.01 |
| vs. Room air n (%) | Normoxemic | 2 (5.7%) | 29 (72.5%) | p < 0.01 |
| Clinical Parameters | Fewer °C ± SD | 36.6 ± 0.4 | 37.4 ± 0.8 | - |
| Sp02 (with 02 supplementation)% ± SD | 95.0 ± 2.5 | 93.8 ± 2.89 | - | |
| CRP 1 median (mg/L) | 41 | 72 | p < 0.01 | |
| CRP 1 min-max mg/L | 1–232 | 2–372 | ||
| Ferritin median (ng/mL) | 698 | 487 | p < 0.01 | |
| Laboratory Parameters | Ferritin min-max (ng/mL) | 102–3713 | 23–5785 | |
| Leukocyte median (103/uL) | 8400 | 5675 | p < 0.01 | |
| Leukocyte min-max (103/uL) | 3000–45,200 | 2250–13,610 | ||
| Neutrophil/Lymphocyte median | 11.28 | 5.22 | p < 0.01 | |
| Neutrophil/Lymphocyte min-max | 1.45–27.66 | 0.97–20.86 | ||
| Patient Classification | Treatment Day 1 | Treatment Day 10 | ||
|---|---|---|---|---|
| Oxygen Supply Method | Device n (%) | Control n (%) | Device n (%) | Control n (%) |
| 0: Room Air | 2 (5.7%) | 16 (40%) | 27 (77.1%) | 29 (72.5%) |
| 1: Nasal Cannula | 13 (39.5%) | 15 (37.5%) | 5 (14.3%) | 6 (15%) |
| 2: Reservoir Oxygen Mask | 12 (31.6%) | 7 (17.5%) | 2 (5.7%) | 1 (2.5%) |
| 3: High Flow Oxygen | 8 (23.7%) | 2 (5%) | 1 (2.9%) | 1 (2.5%) |
| 4: Intubation | 0 (0%) | 0 (0%) | 0 (0%) | 3 (7.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erelel, M.; Kaskal, M.; Akbal-Dagistan, O.; Issever, H.; Dagistanli, A.S.; Balkanci, H.; Oguz, M.S.; Qarayeva, A.; Culha, M.; Erturk, A.; et al. Early Effects of Low Molecular Weight Heparin Therapy with Soft-Mist Inhaler for COVID-19-Induced Hypoxemia: A Phase IIb Trial. Pharmaceutics 2021, 13, 1768. https://doi.org/10.3390/pharmaceutics13111768
Erelel M, Kaskal M, Akbal-Dagistan O, Issever H, Dagistanli AS, Balkanci H, Oguz MS, Qarayeva A, Culha M, Erturk A, et al. Early Effects of Low Molecular Weight Heparin Therapy with Soft-Mist Inhaler for COVID-19-Induced Hypoxemia: A Phase IIb Trial. Pharmaceutics. 2021; 13(11):1768. https://doi.org/10.3390/pharmaceutics13111768
Chicago/Turabian StyleErelel, Mustafa, Mert Kaskal, Ozlem Akbal-Dagistan, Halim Issever, Ahmet Serhan Dagistanli, Hilal Balkanci, Merve Sinem Oguz, Aygun Qarayeva, Meltem Culha, Aybige Erturk, and et al. 2021. "Early Effects of Low Molecular Weight Heparin Therapy with Soft-Mist Inhaler for COVID-19-Induced Hypoxemia: A Phase IIb Trial" Pharmaceutics 13, no. 11: 1768. https://doi.org/10.3390/pharmaceutics13111768