Frequency of CYP3A5 Genetic Polymorphisms and Tacrolimus Pharmacokinetics in Pediatric Liver Transplantation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dosage and Treatment Scheme
2.2. Monitoring and Quantification of Tacrolimus Blood Levels
2.3. Collected Information
2.4. DNA Isolation and Genotyping
2.5. Ethical Aspects
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Undre, N.; Stevenson, P.; Schäfer, A. Pharmacokinetics of tacrolimus: Clinically relevant aspects. Transplant. Proc. 1999, 31, 21–24. [Google Scholar] [CrossRef]
- Wallemacq, P.; Armstrong, V.W.; Brunet, M.; Haufroid, V.; Holt, D.W.; Johnston, A.; Kuypers, D.; Le Meur, Y.; Marquet, P.; Oellerich, M.; et al. Opportunities to Optimize Tacrolimus Therapy in Solid Organ Transplantation: Report of the European Consensus Conference. Ther. Drug Monit. 2009, 31, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staatz, C.E.; Tett, S.E. Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation. Clin. Pharmacokinet. 2004, 43, 623–653. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; McLeod, H.L.; Weinshilboum, R.M. Genomics and drug response. N. Engl. J. Med. 2011, 364, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hesselink, D.A.; van Schaik, R.H.; van der Heiden, I.P.; van der Werf, M.; Gregoor, P.J.; Lindemans, J.; Weimar, W.; van Gelder, T. Genetic polymorphisms of the CYP3A4, CYP3A5, and MDR-1 genes and pharmacokinetics of the calcineurin inhibitors cyclosporine and tacrolimus. Clin. Pharmacol. Ther. 2003, 74, 245–254. [Google Scholar] [CrossRef]
- Buendía, J.A.; Otamendi, E.; Kravetz, M.C.; Cairo, F.; Ruf, A.; de Davila, M.; Powazniak, Y.; Nafissi, J.; Lazarowski, A.; Bramuglia, G.; et al. Combinational Effect of CYP3A5 and MDR-1 Polymorphisms on Tacrolimus Pharmacokinetics in Liver Transplant Patients. Exp. Clin. Transplant 2015, 13, 441–448. [Google Scholar]
- Lamba, J.K.; Lin, Y.S.; Schuetz, E.G.; Thummel, K.E. Genetic contribution to variable human CYP3A-mediated metabolism. Adv. Drug Deliv. Rev. 2002, 54, 1271–1294. [Google Scholar] [CrossRef]
- Buendia, J.A.; Bramuglia, G.; Staatz, C.E. Effects of combinational CYP3A5 6986A>G polymorphism in graft liver and native intestine on the pharmacokinetics of tacrolimus in liver transplant patients: a meta-analysis. Ther. Drug Monit. 2014, 36, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.E.; Herrero, M.J.; Boso, V.; García-Eliz, M.; Poveda, J.L.; Librero, J.; Aliño, S.F. Meta-analysis and systematic review of the effect of the donor and recipient CYP3A5 6986A>G genotype on tacrolimus dose requirements in liver transplantation. Pharmacogenet. Genom. 2013, 23, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Allen, U.; Farmer, D.; Shemesh, E.; Kelly, D.A.; Bucuvalas, J.C.; Alonso, E.M.; Karpen, S.J.; Green, M.; McDonald, R.A. Long-term medical management of the pediatric patient after liver transplantation: 2013 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transplant. 2013, 19, 798–825. [Google Scholar]
- Kuehl, P.; Zhang, J.; Lin, Y.; Lamba, J.; Assem, M.; Schuetz, J.; Watkins, P.B.; Daly, A.; Wrighton, S.A.; Hall, S.D.; et al. Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat. Genet. 2001, 27, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Lavandera, J.; Parera, V.; Rossetti, M.V.; Batlle, A.; Buzaleh, A.M. Identificación de polimorfismos del CYP3A5 y CYP2B6 en infección por VIH asociada a Porfiria Cutánea Tardía en la población Argentina. In Proceedings of the Reunion Cienfitica anual de la Sociedad Argentina de Investigación Clínica (SAIC), Buenos Aires, Argentina, 1 August 2010; Sociedad Argentina de Investigación Clínica (SAIC): Buenos Aires, Argentina, 2010. [Google Scholar]
- Larriba, J.; Imperiali, N.; Groppa, R.; Giordani, C.; Algranatti, S.; Redal, M. Pharmacogenetics of Immunosuppressant Polymorphism of CYP3A5 in Renal Transplant Recipients. Transplant. Proc. 2010, 42, 257–259. [Google Scholar] [CrossRef]
- Ferraris, J.R.; Argibay, P.F.; Costa, L.; Jimenez, G.; Coccia, P.A.; Ghezzi, L.F.; Ferraris, V.; Belloso, W.H.; Redal, M.A.; Larriba, J.M. Influence of CYP3A5 polymorphism on tacrolimus maintenance doses and serum levels after renal transplantation: Age dependency and pharmacological interaction with steroids. Pediatr. Transplant. 2011, 15, 525–532. [Google Scholar] [CrossRef]
- Arrieta, O.; Cardona, A.F.; Bramuglia, G.F.; Gallo, A.; Campos-Parra, A.D.; Serrano, S.; Castro, M.; Avilés, A.; Amorin, E.; Kirchuk, R.; et al. Genotyping Non-small Cell Lung Cancer (NSCLC) in Latin America. J. Thorac. Oncol. 2011, 6, 1955–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roco, A.M.P.; Quinones, L.A.; García-Martín, E.M.; Squicciarini, V.P.; Miranda, C.E.P.; Garay, J.M.; Farfán, N.P.; Saavedra, I.N.P.; Caceres, D.D.M.; Ibarra, C.; et al. Frequencies of 23 functionally significant variant alleles related with metabolism of antineoplastic drugs in the chilean population: comparison with caucasian and asian populations. Front. Genet. 2012, 3, 229. [Google Scholar] [CrossRef] [Green Version]
- Xue, F.; Han, L.; Chen, Y.; Xi, Z.; Li, Q.; Xu, N.; Xia, Y.; Streicher, K.; Zhang, J.; Xia, Q. CYP3A5genotypes affect tacrolimus pharmacokinetics and infectious complications in Chinese pediatric liver transplant patients. Pediatr. Transplant. 2014, 18, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-Y.; Li, J.-L.; Meng, F.-H.; Wang, X.-D.; Li, J.; Liu, L.-S.; Wang, C.-X.; Chen, S.; Li, J.; Meng, F.; et al. Individualization of tacrolimus dosage basing on cytochrome P450 3A5 polymorphism—A prospective, randomized, controlled study. Clin. Transplant. 2013, 27, E272–E281. [Google Scholar] [CrossRef] [PubMed]
- Starkel, P.; Laurent, S.; Petit, M.; Berge, V.V.D.; Lambotte, L.; Horsmans, Y. Early down-regulation of cytochrome P450 3A and 2E1 in the regenerating rat liver is not related to the loss of liver mass or the process of cellular proliferation. Liver Int. 2000, 20, 405–410. [Google Scholar] [CrossRef] [PubMed]



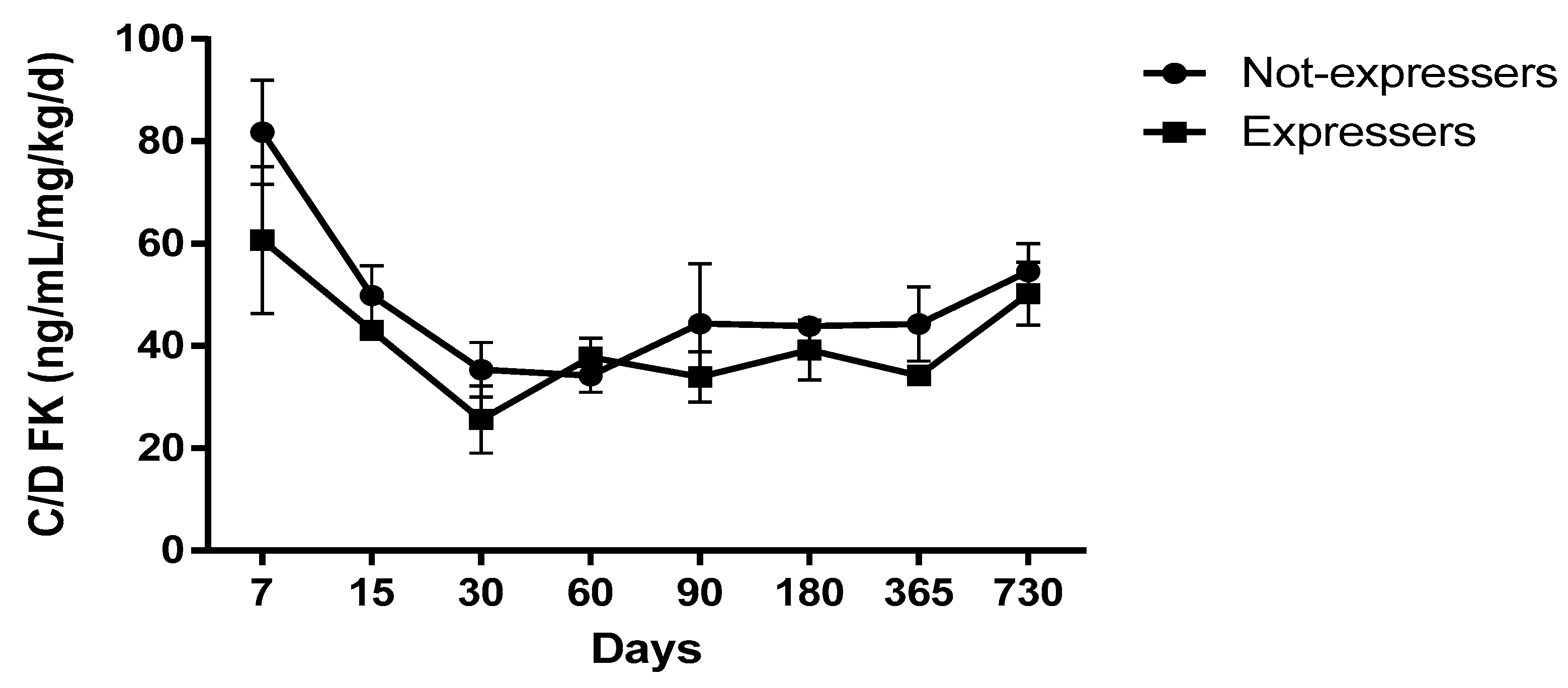{kind=link}
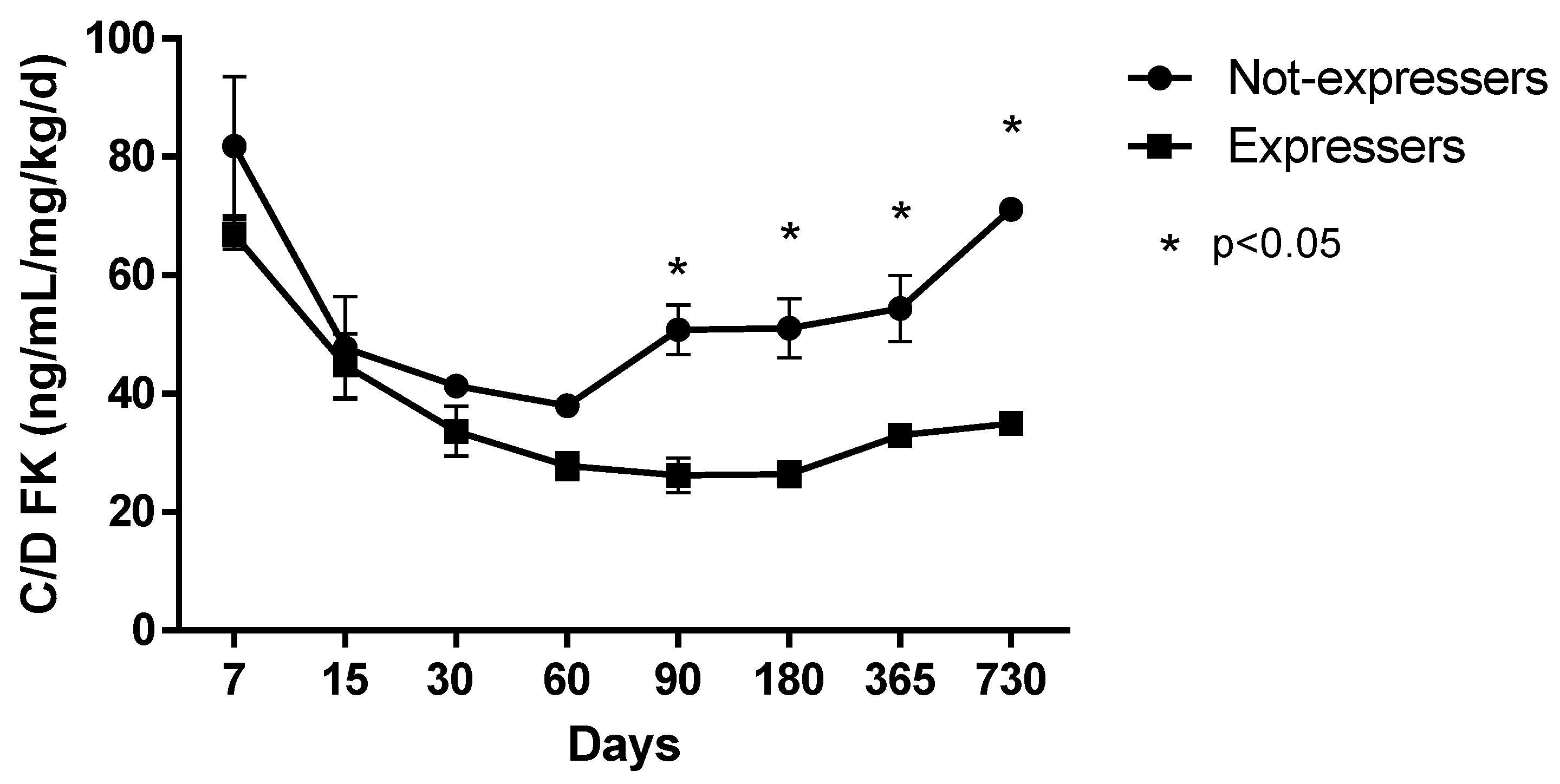{kind=link}
| Feature | n (%) |
|---|---|
| Female | 46 (59.74) |
| Age at transplantation (years, ±SD) | 5.32 (5.42) |
| Weight (kg, ±DE) | 21.84(17.89) |
| Origin | |
| Argentina | 64(83.11) |
| Bolivia | 2(2.60) |
| Paraguay | 9(11.69) |
| Other | 2(2.59) |
| Primary disease | |
| Biliary atresia | 32(41.55) |
| Fulminant hepatitis | 16(20.77) |
| Autoimmune hepatitis | 11(14.28) |
| Hepatoblastoma | 8(10.38) |
| Others | 10(12.98) |
| Kind of Donor | |
| Cadaveric | 55(71.42) |
| Live | 22(28.57) |
| Kind of Graft | |
| Full | 26(33.76) |
| Technical variant | 51(66.23) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buendía, J.A.; Halac, E.; Bosaleh, A.; Garcia de Davila, M.T.; Imvertasa, O.; Bramuglia, G. Frequency of CYP3A5 Genetic Polymorphisms and Tacrolimus Pharmacokinetics in Pediatric Liver Transplantation. Pharmaceutics 2020, 12, 898. https://doi.org/10.3390/pharmaceutics12090898
Buendía JA, Halac E, Bosaleh A, Garcia de Davila MT, Imvertasa O, Bramuglia G. Frequency of CYP3A5 Genetic Polymorphisms and Tacrolimus Pharmacokinetics in Pediatric Liver Transplantation. Pharmaceutics. 2020; 12(9):898. https://doi.org/10.3390/pharmaceutics12090898
Chicago/Turabian StyleBuendía, Jefferson Antonio, Esteban Halac, Andrea Bosaleh, María T. Garcia de Davila, Oscar Imvertasa, and Guillermo Bramuglia. 2020. "Frequency of CYP3A5 Genetic Polymorphisms and Tacrolimus Pharmacokinetics in Pediatric Liver Transplantation" Pharmaceutics 12, no. 9: 898. https://doi.org/10.3390/pharmaceutics12090898