Hydrodynamics of Intravitreal Injections into Liquid Vitreous Substitutes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials, Instrumentation, and Methods
2.1. Materials
2.2. Instrumentation
2.3. Methods
2.3.1. Viscosity Measurements
2.3.2. Surface Tension Measurements
2.3.3. Injection in Different Vitreous Substitutes
2.3.4. Image Processing
3. Results
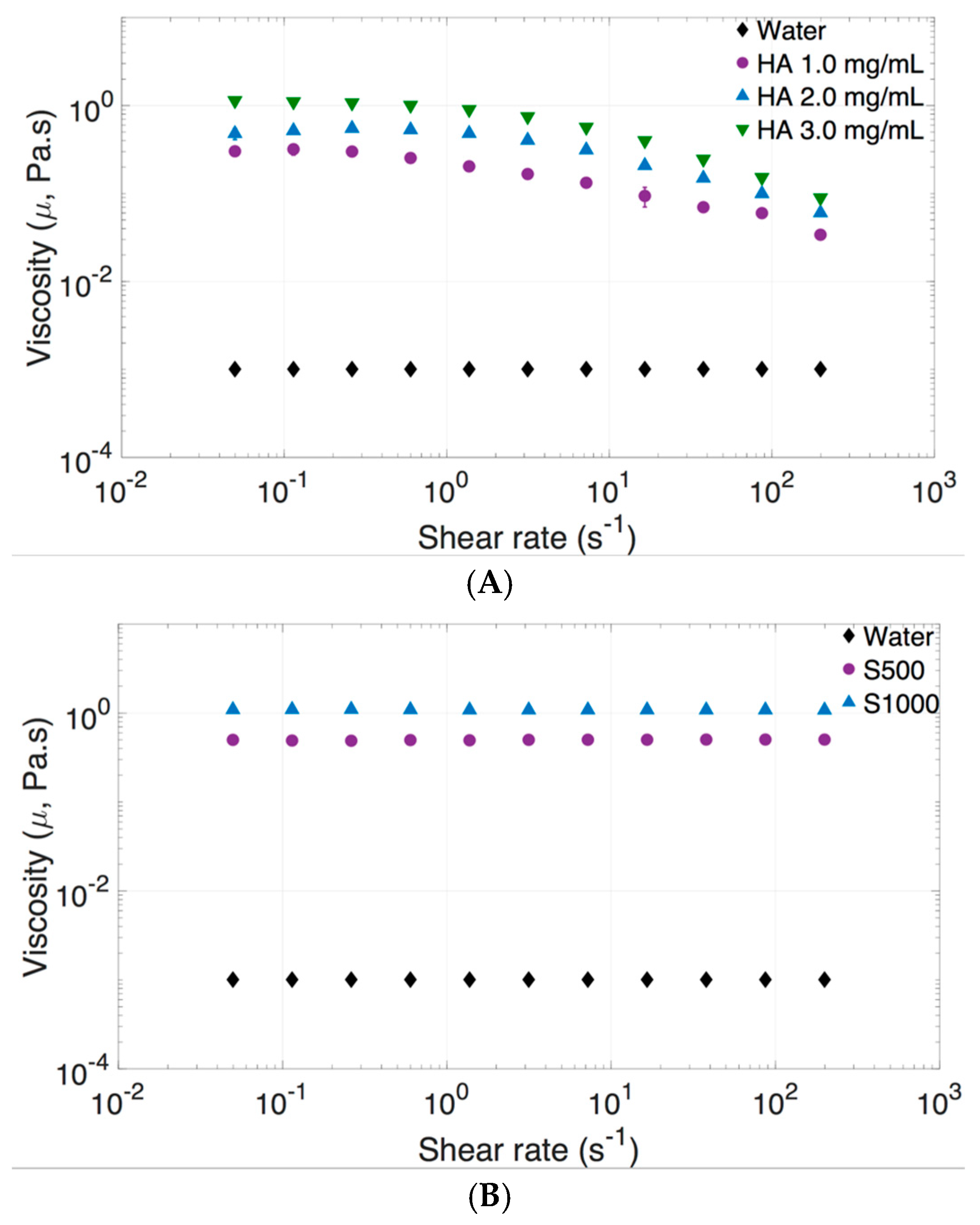
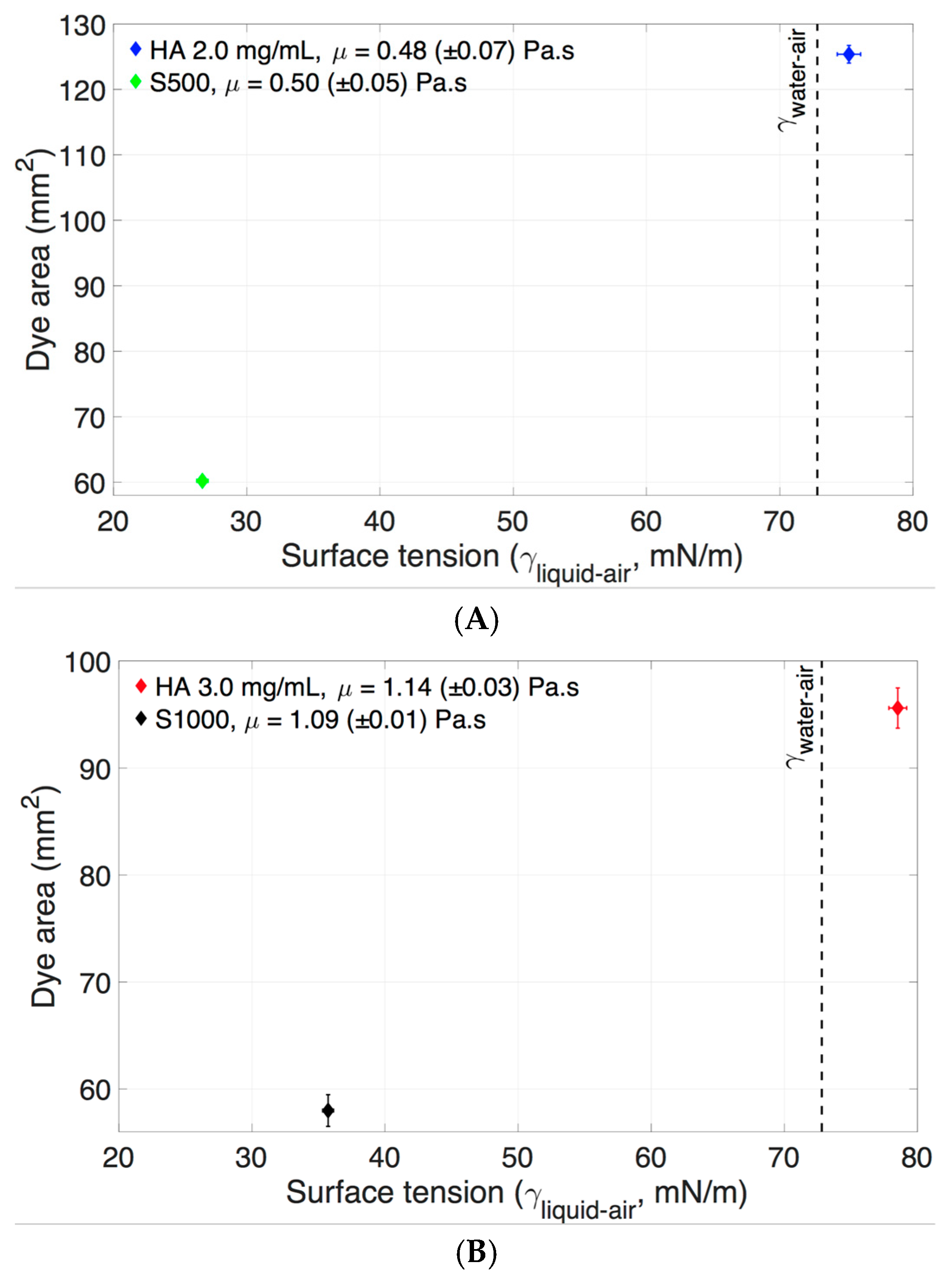
3.1. Dynamic Viscosity, Surface Tension, and Density of Vitreous Substitutes
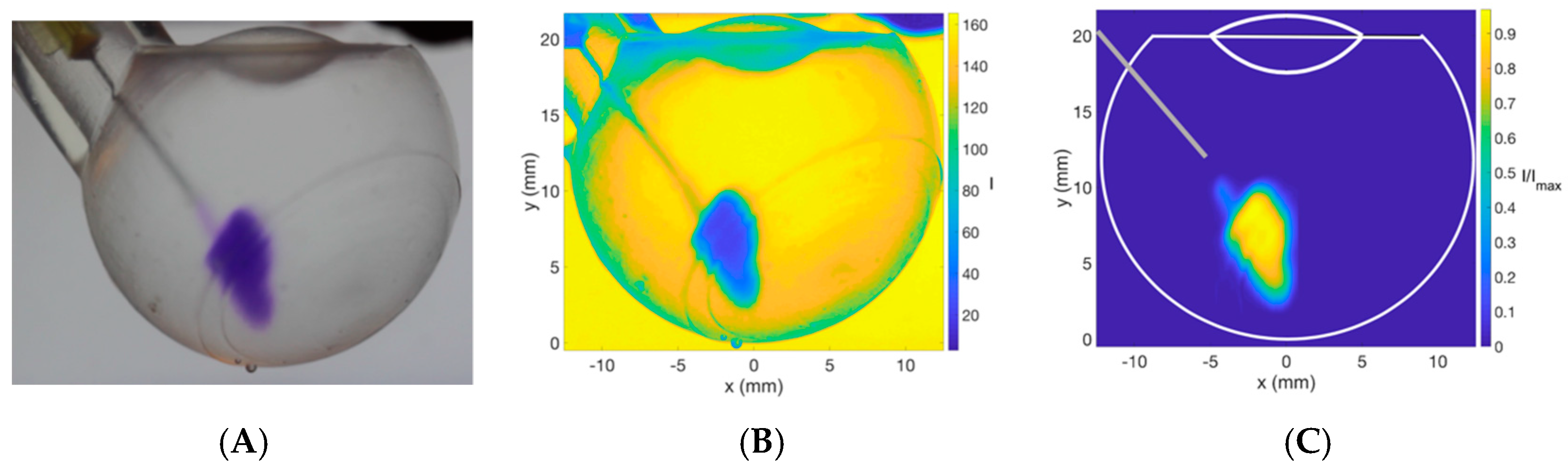
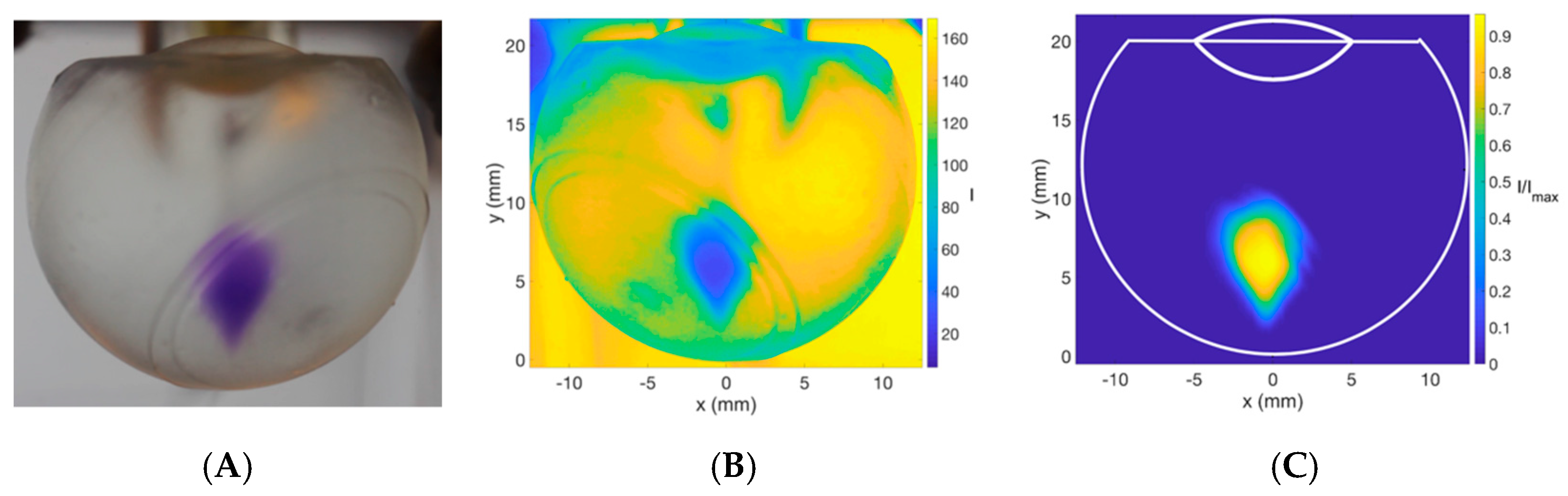
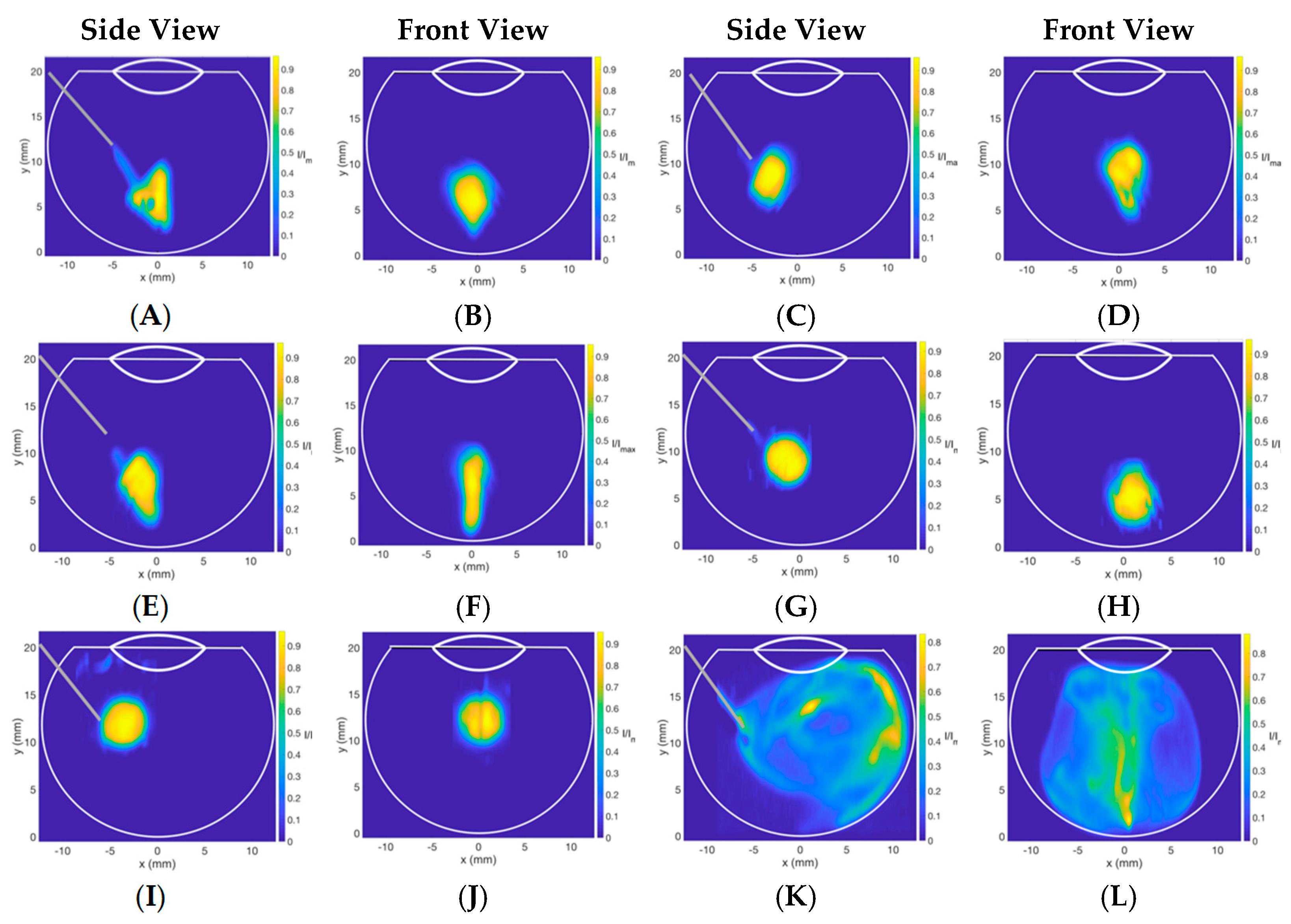
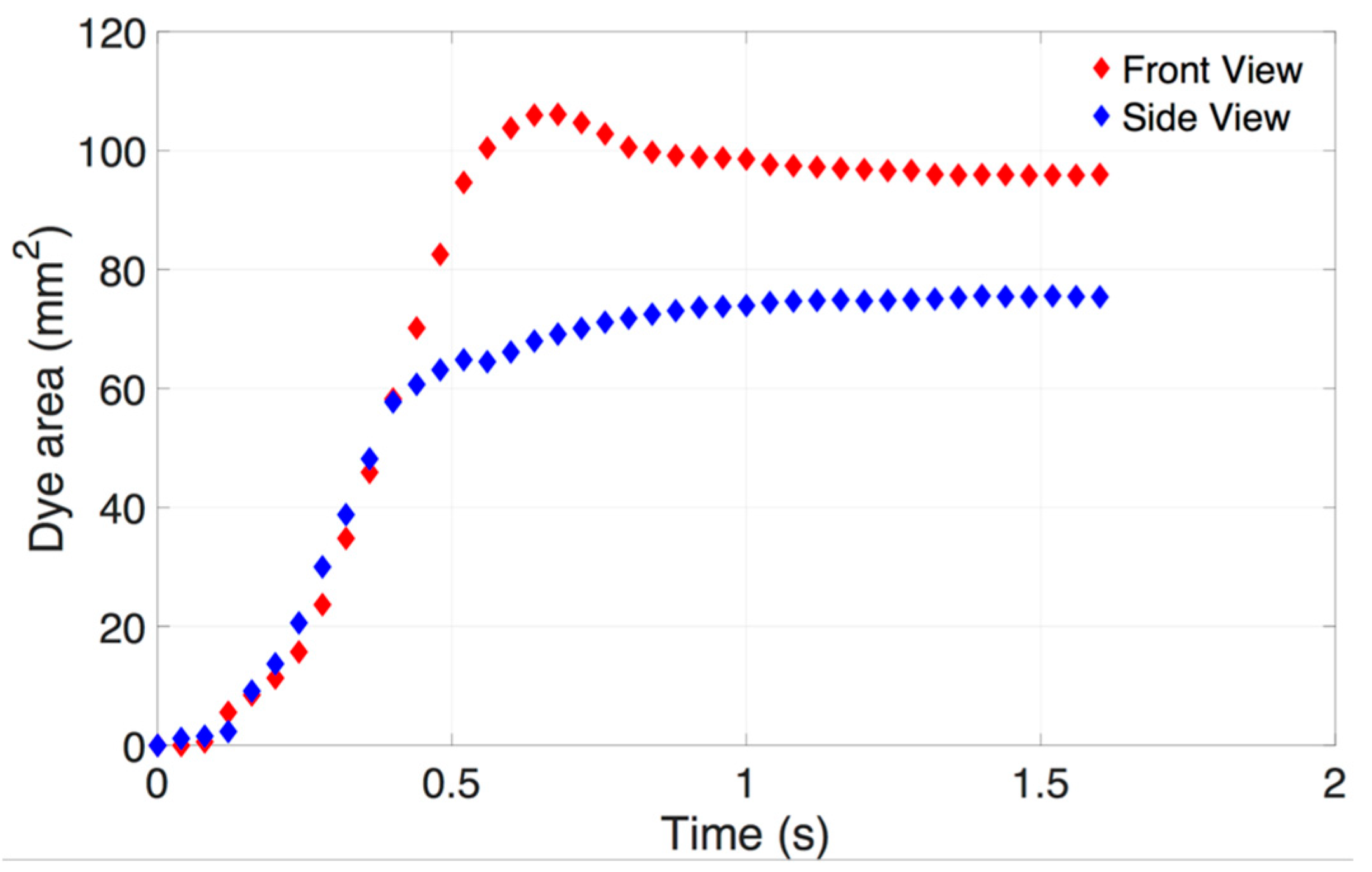
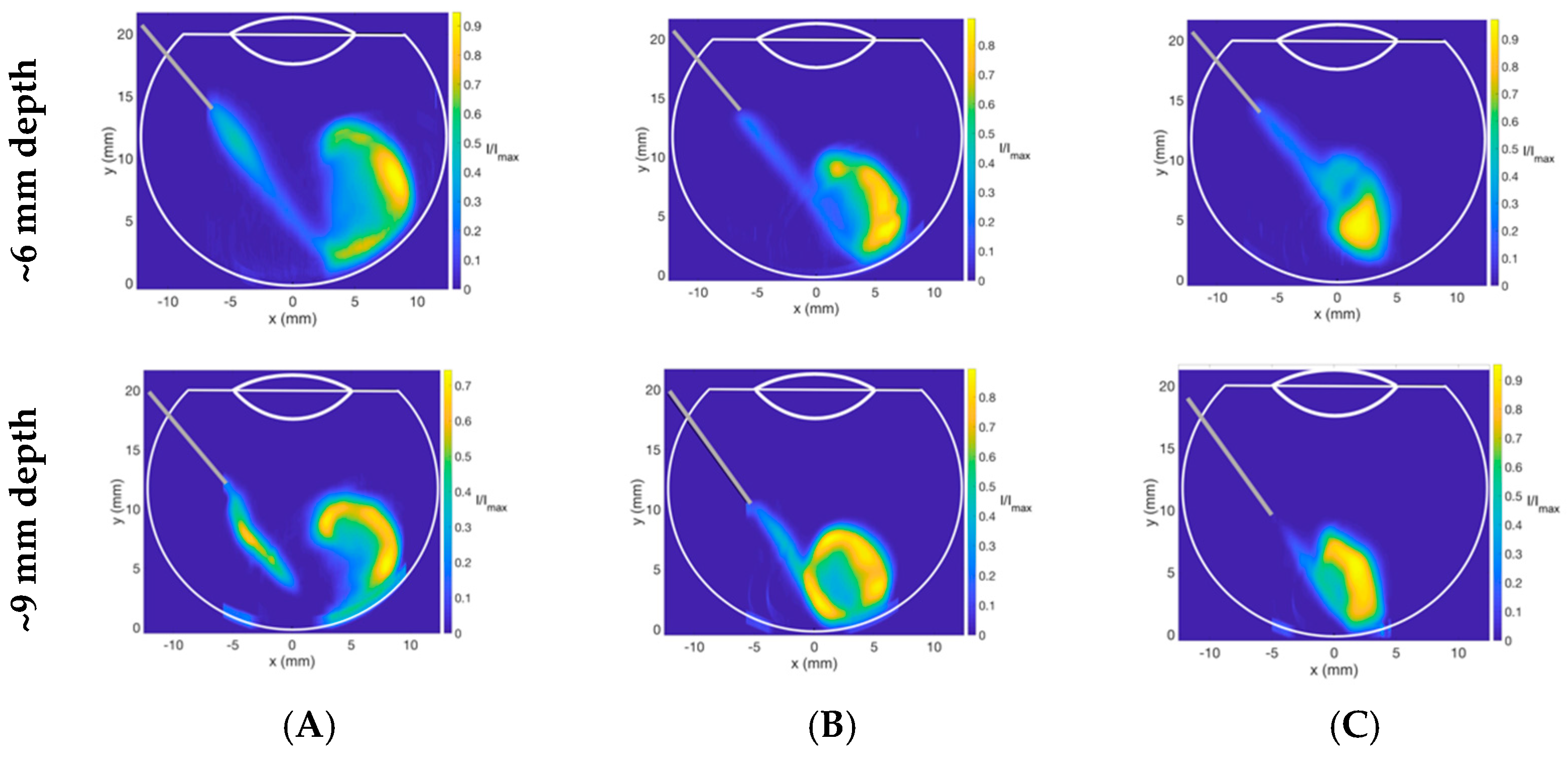
3.2. Dispersion Dynamics of Injectable Dye in Different Vitreous Substitutes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lau, P.E.; Jenkins, K.S.; Layton, C.J. Current Evidence for the Prevention of Endophthalmitis in Anti-VEGF Intravitreal Injections. J Ophthalmol. 2018, 2018, 1–8. Available online: https://www.hindawi.com/journals/joph/2018/8567912/ (accessed on 24 July 2018). [CrossRef] [PubMed]
- Lamminsalo, M.; Taskinen, E.; Karvinen, T.; Subrizi, A.; Murtomäki, L.; Urtti, A.; Ranta, V.P. Extended Pharmacokinetic Model of the Rabbit Eye for Intravitreal and Intracameral Injections of Macromolecules: Quantitative Analysis of Anterior and Posterior Elimination Pathways. Pharm. Res. 2018, 35, 153. Available online: http://link.springer.com/10.1007/s11095-018-2435-0 (accessed on 31 August 2018). [CrossRef] [PubMed] [Green Version]
- CATT Research Group; Martin, D.F.; Maguire, M.G.; Ying, G.; Grunwald, J.E.; Fine, S.L.; Jaffe, G.J. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2011, 364, 1897–1908. Available online: http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:new+england+journal#2%5Cnhttp://europepmc.org/articles/PMC3157322 (accessed on 19 May 2011). [CrossRef] [PubMed]
- Tanzi, M.G. Aflibercept: Bimonthly intravitreal injection for AMD. Pharm. Today 2016, 18, 43. [Google Scholar] [CrossRef]
- Ghosh, J.G.; Nguyen, A.A.; Bigelow, C.E.; Poor, S.; Qiu, Y.; Rangaswamy, N.; Ornberg, R.; Jackson, B.; Mak, H.; Ezell, T.; et al. Long-acting protein drugs for the treatment of ocular diseases. Nat. Commun. 2017, 8, 14837. [Google Scholar] [CrossRef]
- Regeneron. Regeneron Announces FDA Acceptance of sBLA Filing for 12-Week Dosing of Eylea® (aflibercept) Injection for Patients with Wet AMD. Available online: https://investor.regeneron.com/news-releases/news-release-details/regeneron-announces-fda-acceptance-sbla-filing-12-week-dosing (accessed on 26 April 2019).
- Hollingworth, W.; Jones, T.; Reeves, B.C.; Peto, T. A longitudinal study to assess the frequency and cost of antivascular endothelial therapy, and inequalities in access, in England between 2005 and 2015. BMJ Open 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sebag, J. Ageing of the vitreous. Eye 1987, 1, 254–262. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3308528 (accessed on 5 September 2013). [CrossRef]
- Le Goff, M.M.; Bishop, P.N. Adult vitreous structure and postnatal changes. Eye 2008, 22, 1214–1222. Available online: http://www.ncbi.nlm.nih.gov/pubmed/18309340 (accessed on 26 April 2019). [CrossRef] [Green Version]
- Bishop, P.N. Structural macromolecules and supramolecular organisation of the vitreous gel. Prog. Retin. Eye Res. 2000, 19, 323–344. Available online: http://www.ncbi.nlm.nih.gov/pubmed/10749380 (accessed on 26 April 2019). [CrossRef]
- Awwad, S.; Lockwood, A.; Brocchini, S.; Khaw, P.T. The PK-Eye: A Novel In Vitro Ocular Flow Model for Use in Preclinical Drug Development. J. Pharm. Sci. 2015, 104, 3330–3342. [Google Scholar] [CrossRef] [Green Version]
- Loch, C.; Nagel, S.; Guthoff, R.; Seidlitz, A.; Weitschies, W. The Vitreous Model–A new in vitro test method simulating the vitreous body. Biomed Tech. 2012, 57, 281–284. [Google Scholar] [CrossRef]
- Stocchino, A.; Repetto, R.; Cafferata, C. Eye rotation induced dynamics of a Newtonian fluid within the vitreous cavity: The effect of the chamber shape. Phys. Med. Biol. 2007, 52, 2021–2034. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17374925 (accessed on 26 April 2019). [CrossRef]
- Stein, S.; Bogdahn, M.; Rosenbaum, C.; Weitschies, W.; Seidlitz, A. Distribution of fluorescein sodium and triamcinolone acetonide in the simulated liquefied and vitrectomized Vitreous Model with simulated eye movements. Eur. J. Pharm. Sci. 2017, 109, 233–243. [Google Scholar] [CrossRef]
- Del Amo, E.M.; Urtti, A. Rabbit as an animal model for intravitreal pharmacokinetics: Clinical predictability and quality of the published data. Exp. Eye Res. 2015, 137, 111–124. Available online: http://linkinghub.elsevier.com/retrieve/pii/S0014483515001451 (accessed on 26 April 2019). [CrossRef] [Green Version]
- Hubschman, J.P.; Coffee, R.E.; Bourges, J.L.; Yu, F.; Schwartz, S.D. Experimental model of intravitreal injection techniques. Retina 2010, 30, 167–173. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19779317 (accessed on 26 April 2019). [CrossRef]
- Jooybar, E.; Abdekhodaie, M.J.; Farhadi, F.; Cheng, Y.L. Computational modeling of drug distribution in the posterior segment of the eye: Effects of device variables and positions. Math. Biosci. 2014, 255, 11–20. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24946303 (accessed on 12 November 2014). [CrossRef]
- Garg, S.J.; Recchia, F.M. Evolving guidelines for intravitreous injections. Retina 2004, 25, 3–19. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16205582 (accessed on 26 April 2019).
- Raju, J.R.; Weinberg, D.V. Accuracy and precision of intraocular injection volume. Am. J. Ophthalmol. 2002, 133, 564–566. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11931796 (accessed on 26 April 2019). [CrossRef]
- Thrimawithana, T.; Young, S.; Bunt, C. Drug delivery to the posterior segment of the eye. Drug Discov. Today 2011, 16, 270–277. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21167306 (accessed on 5 September 2013). [CrossRef]
- Grzybowski, A.; Told, R.; Sacu, S.; Bandello, F.; Moisseiev, E.; Loewenstein, A.; Schmidt-Erfurth, U. 2018 Update on Intravitreal Injections: Euretina Expert Consensus Recommendations. Ophthalmologica 2018, 239, 181–193. [Google Scholar] [CrossRef]
- Friedrich, S.; Saville, B.; Cheng, Y.L. Drug Distribution in the Vitreous Humor of the Human Eye: The Effects of Aphakia and Changes in Retinal Permeability and Vitreous Diffusivity. J. Ocul. Pharmacol. Ther. 1997, 13, 445–459. Available online: http://www.liebertonline.co (accessed on 26 April 2019). [CrossRef]
- Missel, P.J. Simulating Intravitreal Injections in Anatomically Accurate Models for Rabbit, Monkey, and Human Eyes. Pharm. Res. 2012, 29, 3251–3272. Available online: http://link.springer.com/10.1007/s11095-012-0721-9 (accessed on 26 April 2019). [CrossRef] [Green Version]
- Park, J.; Bungay, P.; Lutz, R. Evaluation of coupled convective–diffusive transport of drugs administered by intravitreal injection and controlled release implant. J. Control Release 2005, 105, 279–295. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15896868 (accessed on 5 September 2013). [CrossRef]
- Kathawate, J.; Acharya, S. Computational modeling of intravitreal drug delivery in the vitreous chamber with different vitreous substitutes. Int. J. Heat Mass Transf. 2008, 51, 5598–5609. Available online: http://linkinghub.elsevier.com/retrieve/pii/S0017931008002718 (accessed on 24 November 2014). [CrossRef]
- Zhang, Y.; Bazzazi, H.; Lima, E.; Silva, R.; Pandey, N.B.; Green, J.J.; Campochiaro, P.A.; Popel, A.S. Three-Dimensional Transport Model for Intravitreal and Suprachoroidal Drug Injection. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5266–5276. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30383198 (accessed on 26 April 2019). [CrossRef] [Green Version]
- Causin, P.; Malgaroli, F. Mathematical assessment of drug build-up in the posterior eye following transscleral delivery. J. Math. Ind. 2016, 6, 9. Available online: http://mathematicsinindustry.springeropen.com/articles/10.1186/s13362-016-0031-7 (accessed on 26 April 2019). [CrossRef] [Green Version]
- Stay, M.S.; Xu, J.; Randolph, T.W.; Barocas, V.H. Computer simulation of convective and diffusive transport of controlled-release drugs in the vitreous humor. Pharm. Res. 2003, 20, 96–102. [Google Scholar] [CrossRef]
- Kim, H.; Lizak, M.J.; Tansey, G.; Csaky, K.G.; Robinson, M.R.; Yuan, P.; Wang, N.S.; Lutz, R.J. Study of ocular transport of drugs released from an intravitreal implant using magnetic resonance imaging. Ann. Biomed. Eng. 2005, 33, 150–164. [Google Scholar] [CrossRef]
- Boyer, D.S.; Faber, D.; Gupta, S.; Patel, S.S.; Tabandeh, H.; Li, X.Y.; Liu, C.C.; Lou, J.; Whitcup, S.M.; Ozurdex CHAMPLAIN Study Group. Dexamethasone Intravitreal Implant for Treatment of Diabetic Macular Edema in Vitrectomized Patients. Retina 2011, 31, 915–923. Available online: https://insights.ovid.com/crossref?an=00006982-201105000-00014 (accessed on 26 April 2019). [CrossRef]
- Lee, S.S.; Ghosn, C.; Yu, Z.; Zacharias, L.C.; Kao, H.; Lanni, C.; Abdelfattah, N.; Kuppermann, B.; Csaky, K.G.; D’Argenio, D.Z.; et al. Vitreous VEGF clearance is increased after vitrectomy. Investig. Ophthalmol. Vis. Sci. 2010, 51, 2135–2138. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20019364 (accessed on 11 December 2014). [CrossRef]
- Kleinberg, T.T.; Tzekov, R.T.; Stein, L.; Ravi, N.; Kaushal, S. Vitreous Substitutes: A Comprehensive Review. Surv. Ophthalmol. 2011, 56, 300–323. [Google Scholar] [CrossRef]
- Chin, H.S.; Park, T.S.; Moon, Y.S.; Oh, J.H. Difference in clearance of intravitreal triamcinolone acetonide between vitrectomized and nonvitrectomized eyes. Retina 2005, 25, 556–560. [Google Scholar] [CrossRef]
- Kakinoki, M.; Sawada, O.; Sawada, T.; Saishin, Y.; Kawamura, H.; Ohji, M. Effect of vitrectomy on aqueous VEGF concentration and pharmacokinetics of bevacizumab in macaque monkeys. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5877–5880. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22836776 (accessed on 26 September 2013). [CrossRef]
- Schindler, R.H.; Chandler, D.; Thresher, R.; Machemer, R. The clearance of intravitreal triamcinolone acetonide. Am. J. Ophthalmol. 1982, 93, 415–417. Available online: http://www.ncbi.nlm.nih.gov/pubmed/7072807 (accessed on 5 September 2014). [CrossRef]
- Mandell, B.A.; Meredith, T.A.; Aguilar, E.; El-Massry, A.; Sawant, A.; Gardner, S. Effects of inflammation and surgery on amikacin levels in the vitreous cavity. Am. J. Ophthalmol. 1993, 115, 770–774. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8506912 (accessed on 8 August 2014). [CrossRef]
- Pflugfelder, S.C.; Hernández, E.; Fliesler, S.J.; Alvarez, J.; Pflugfelder, M.E.; Forster, R.K. Intravitreal vancomycin. Retinal toxicity, clearance, and interaction with gentamicin. Arch. Ophthalmol. 1987, 105, 831–837. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3495255 (accessed on 26 April 2019). [CrossRef]
- Chhablani, J.; Narayanan, R. Anti-VEGF therapy in a silicone oil-filled myopic eye with choroidal neovascularisation. BMJ Case Rep. 2015, 2015, 2014–2015. [Google Scholar] [CrossRef]
- Cascavilla, M.L.; Querques, G.; Querques, L.; Codenotti, M.; Bandello, F. Intravitreal Ranibizumab for myopic choroidal neovascularization after pars plana vitrectomy and silicone oil tamponade. Eur. J. Ophthalmol. 2013, 23, 913–916. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Modarres, M.; Nazari, H. Therapeutic effect of bevacizumab injected into the silicone oil in eyes with neovascular glaucoma after vitrectomy for advanced diabetic retinopathy. Eye 2010, 24, 717–719. [Google Scholar] [CrossRef]
- Salman, A.G. Intrasilicone bevacizumab injection for iris neovascularization after vitrectomy for proliferative diabetic retinopathy. Ophthalmic Res. 2012, 49, 20–24. [Google Scholar] [CrossRef]
- Ghoreishi, S.M.; Behpour, M.; Golestaneh, M. Simultaneous voltammetric determination of Brilliant Blue and Tartrazine in real samples at the surface of a multi-walled carbon nanotube paste electrode. Anal. Methods 2011, 3, 2842–2847. [Google Scholar] [CrossRef]
- Tram, N.K.; Swindle-Reilly, K.E. Rheological Properties and Age-Related Changes of the Human Vitreous Humor. Front. Bioeng. Biotechnol. 2018, 6, 199. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, E.B.; Grumann, A.; Penha, F.M.; Shiroma, H.; Rossi, E.; Meyer, C.H.; Stefano, V.; Maia, M.; Magalhaes, O., Jr.; Farah, M.E. Effect of Needle Type and Injection Technique on Pain Level and Vitreal Reflux in Intravitreal Injection. J. Ocul. Pharmacol. Ther. 2011, 27, 197–203. [Google Scholar] [CrossRef]
- Baldyga, J.; Bourne, J.R. Simplification of micromixing calculations. I. Derivation and application of new model. Chem. Eng. J. 1989, 42, 83–92. Available online: https://linkinghub.elsevier.com/retrieve/pii/0300946789850026 (accessed on 26 April 2019). [CrossRef]
- Frenkel, R.E.P.; Haji, S.A.; La, M.; Frenkel, M.P.C.; Reyes, A. A protocol for the retina surgeon’s safe initial intravitreal injections. Clin. Ophthalmol. 2010, 4, 1279–1285. [Google Scholar] [CrossRef]
- Landers, M.B.; Watson, J.S.; Ulrich, J.N.; Quiroz-Mercado, H. Determination of retinal and vitreous temperature in vitrectomy. Retina 2012, 32, 172–176. [Google Scholar] [CrossRef]
- Shatz, W.; Hass, P.E.; Mathieu, M.; Kim, H.S.; Leach, K.; Zhou, M.; Crawford, Y.; Shen, A.; Wang, K.; Chang, D.P.; et al. Contribution of Antibody Hydrodynamic Size to Vitreal Clearance Revealed through Rabbit Studies Using a Species-Matched Fab. Mol. Pharm. 2016, 13, 2996–3003. Available online: http://pubs.acs.or (accessed on 26 April 2019). [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vitreous Substitute | Viscosity (Pa·s) | Surface Tension (Liquid/Air) (mN/m) |
|---|---|---|
| Distilled water (control) | 0.0010 ± 0.0001 | 72.8 ± 0.1 |
| Sodium hyaluronate (HA) | ||
| 1.0 mg/mL | 0.30 ± 0.02 | 71.0 ± 4.0 |
| 2.0 mg/mL | 0.48 ± 0.07 | 75.2 ± 1.3 |
| 3.0 mg/mL | 1.14 ± 0.03 | 78.5 ± 1.9 |
| Silicone Oil (SO) | ||
| S500 | 0.50 ± 0.05 | 26.7 ± 0.7 |
| S1000 | 1.09 ± 0.01 | 35.7 ± 1.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henein, C.; Awwad, S.; Ibeanu, N.; Vlatakis, S.; Brocchini, S.; Tee Khaw, P.; Bouremel, Y. Hydrodynamics of Intravitreal Injections into Liquid Vitreous Substitutes. Pharmaceutics 2019, 11, 371. https://doi.org/10.3390/pharmaceutics11080371
Henein C, Awwad S, Ibeanu N, Vlatakis S, Brocchini S, Tee Khaw P, Bouremel Y. Hydrodynamics of Intravitreal Injections into Liquid Vitreous Substitutes. Pharmaceutics. 2019; 11(8):371. https://doi.org/10.3390/pharmaceutics11080371
Chicago/Turabian StyleHenein, Christin, Sahar Awwad, Nkiruka Ibeanu, Stavros Vlatakis, Steve Brocchini, Peng Tee Khaw, and Yann Bouremel. 2019. "Hydrodynamics of Intravitreal Injections into Liquid Vitreous Substitutes" Pharmaceutics 11, no. 8: 371. https://doi.org/10.3390/pharmaceutics11080371