Targeted Topical Delivery of Retinoids in the Management of Acne Vulgaris: Current Formulations and Novel Delivery Systems

 ,
,
Abstract
:
1. Introduction
2. Current Treatment of Acne Vulgaris
- Mild Acne: First line treatment should consist of a topical retinoid—adapalene, isotretinoin, tretinoin, or tazarotene. Gel formulations are recommended for patients with oily skin, while creams are recommended for those with dry or sensitive skin. If minimal improvement is seen after 6 weeks of topical retinoid treatment, add topical benzoyl peroxide, clindamycin or erythromycin.
- Moderate Acne: A topical retinoid or benzoyl peroxide (BPO) is to be applied as per the mild acne guideline, and the strength of the preparation may be increased. It is also recommended that an oral antibiotic is added, such as minocycline, doxycycline or erythromycin. For female patients, hormonal contraceptive therapy may also be added to regulate androgen production.
- Severe Acne: Topical tretinoin is the preferred retinoid to use in moderate to severe cases, combined with one of the aforementioned antibiotics at a higher strength. If still unresponsive, oral isotretinoin therapy is the drug of choice for severe cystic acne.
3. Topical Retinoids: Efficacy, Safety and Tolerability
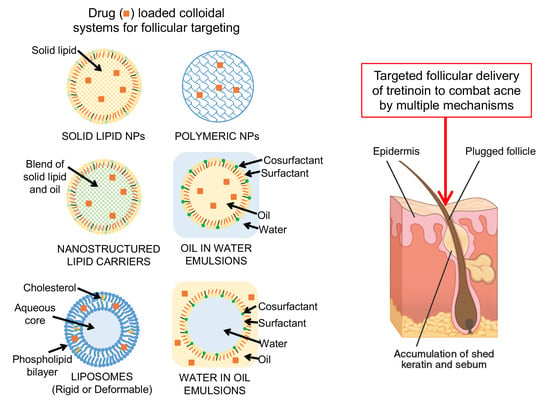
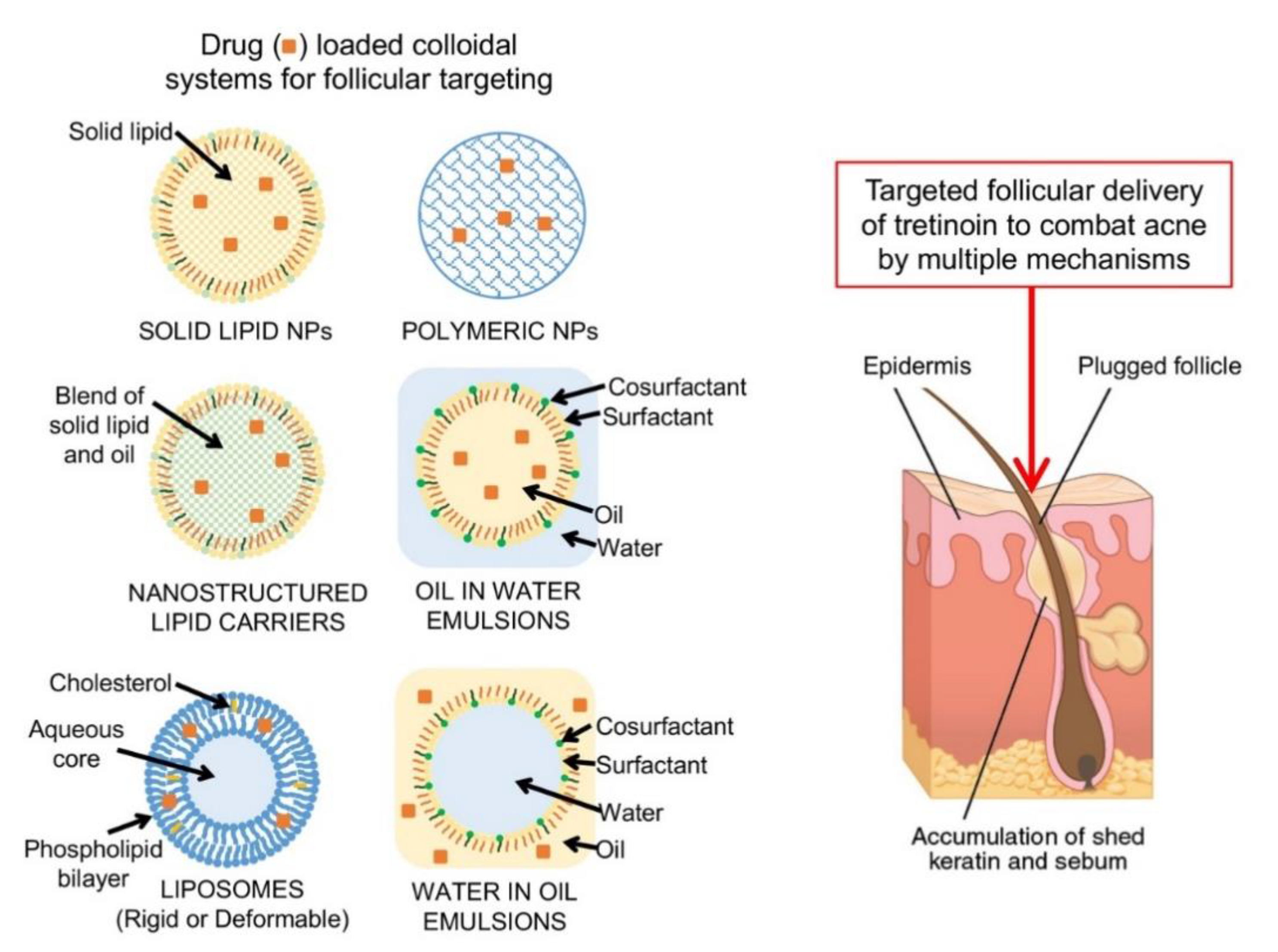
4. Targeted Topical Delivery to the Follicles: A Role for Colloidal Delivery Systems
5. Targeted Topical Delivery of Retinoids: Strategies to Improve Efficacy, Safety and Tolerability
5.1. Tretinoin
5.2. Tazarotene
5.3. Adapalene
5.4. Isotretinoin
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Purdy, S.; de Berker, D. Acne vulgaris. BMJ Clin. Evid. 2011, 346, f2634. [Google Scholar]
- Gebauer, K. Acne in adolescents. Aust. Fam. Physician 2017, 46, 892–895. [Google Scholar] [PubMed]
- Zaenglein, A.L.; Thiboutot, D.M. Acne vulgaris. In Dermatology, 3rd ed.; Bolognia, J., Jorizzo, J., Schaffer, J., Eds.; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Tanghetti, E.A.; Kawata, A.K.; Daniels, S.R.; Yeomans, K.; Burk, C.T.; Callender, V.D. Understanding the Burden of Adult Female Acne. J. Clin. Aesthetic Dermatol. 2014, 7, 22–30. [Google Scholar]
- Dreno, B.; Thiboutot, D.; Layton, A.M.; Berson, D.; Perez, M.; Kang, S.; Global Alliance to Improve Outcomes in, A. Large-scale international study enhances understanding of an emerging acne population: Adult females. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1096–1106. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, A.M.; Gallo, R.L. Host-microbiome interactions and recent progress into understanding the biology of Acne vulgaris. Microbiome 2018, 6, 177. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.; Watterson, S.; Layton, A.M.; Bjourson, A.J.; Barnard, E.; McDowell, A. Propionibacterium acnes and Acne Vulgaris: New Insights from the Integration of Population Genetic, Multi-Omic, Biochemical and Host-Microbe Studies. Microorganisms 2019, 7, 128. [Google Scholar] [CrossRef] [PubMed]
- Tanghetti, E.A. The Role of Inflammation in the Pathology of Acne. J. Clin. Aesthetic Dermatol. 2013, 6, 27–35. [Google Scholar]
- Amirthanandan, S. Therapeutic Guidelines: Dermatology. Version 3. Aust. Prescr. 2009, 32, 139. [Google Scholar] [CrossRef] [Green Version]
- Thiboutot, D.M.; Dréno, B.; Abanmi, A.; Alexis, A.F.; Araviiskaia, E.; Cabal, M.I.B.; Bettoli, V.; Casintahan, F.; Chow, S.; Da Costa, A.; et al. Practical management of acne for clinicians: An international consensus from the Global Alliance to Improve Outcomes in Acne. J. Am. Acad. Dermatol. 2018, 78, S1–S23. [Google Scholar] [CrossRef]
- Zaenglein, A.L.; Pathy, A.L.; Schlosser, B.J.; Alikhan, A.; Baldwin, H.E.; Berson, D.S.; Bowe, W.P.; Graber, E.M.; Harper, J.C.; Kang, S.; et al. Guidelines of care for the management of acne vulgaris. J. Am. Acad. Dermatol. 2016, 74, 945–973. [Google Scholar] [CrossRef]
- Fox, L.; Csongradi, C.; Aucamp, M.; Du Plessis, J.; Gerber, M. Treatment Modalities for Acne. Molecules 2016, 21, 1063. [Google Scholar] [CrossRef] [PubMed]
- Kraft, J.; Freiman, A. Management of acne. Can. Med. Assoc. J. 2011, 183, e430–e435. [Google Scholar] [CrossRef] [PubMed]
- Gollnick, H.P.M. From new findings in acne pathogenesis to new approaches in treatment. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kolli, S.S.; Pecone, D.; Pona, A.; Cline, A.; Feldman, S.R. Topical Retinoids in Acne Vulgaris: A Systematic Review. Am. J. Clin. Dermatol. 2019, 20, 345–365. [Google Scholar] [CrossRef] [PubMed]
- Thiboutot, D.; Arsonnaud, S.; Soto, P. Efficacy and tolerability of adapalene 0.3% gel compared to tazarotene 0.1% gel in the treatment of acne vulgaris. J. Drugs Dermatol. 2008, 7, 3–10. [Google Scholar]
- Tirado-Sanchez, A.; Espindola, Y.S.; Ponce-Olivera, R.M.; Bonifaz, A. Efficacy and safety of adapalene gel 0.1% and 0.3% and tretinoin gel 0.05% for acne vulgaris: Results of a single-center, randomized, double-blinded, placebo-controlled clinical trial on Mexican patients (skin type III–IV). J. Cosmet. Dermatol. 2013, 12, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Dreno, B.; Thiboutot, D.; Gollnick, H.; Finlay, A.Y.; Layton, A.; Leyden, J.J.; Leutenegger, E.; Perez, M. Large-scale worldwide observational study of adherence with acne therapy. Int. J. Dermatol. 2010, 49, 448–456. [Google Scholar] [CrossRef]
- Queille-Roussel, C.; Poncet, M.; Mesaros, S.; Clucas, A.; Baker, M.; Soloff, A.-M. Comparison of the cumulative irritation potential of adapalene gel and cream with that of erythromycin/tretinoin solution and gel and erythromycin/isotretinoin gel. Clin. Ther. 2001, 23, 205–212. [Google Scholar] [CrossRef]
- Leyden, J.J.; Nighland, M.; Rossi, A.B.; Ramaswamy, R. Irritation potential of tretinoin gel microsphere pump versus adapalene plus benzoyl peroxide gel. J. Drugs Dermatol. 2010, 9, 998–1003. [Google Scholar]
- Griffiths, C.; Kang, S.; Ellis, C.N.; Kim, K.J.; Finkel, L.J.; Ortiz-Ferrer, L.C.; White, G.M.; Hamilton, T.; Voorhees, J.J. Two concentrations of topical tretinoin (retinoic acid) cause similar improvement of photoaging but different degrees of irritation. A double-blind, vehicle-controlled comparison of 0.1% and 0.025% tretinoin creams. Arch. Dermatol. 1995, 131, 1037–1044. [Google Scholar] [CrossRef]
- Eskandar, N.G.; Simovic, S.; Prestidge, C.A. Chemical stability and phase distribution of all-trans-retinol in nanoparticle-coated emulsions. Int. J. Pharm. 2009, 376, 186–194. [Google Scholar] [CrossRef]
- NIH. PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov (accessed on 1 August 2019).
- ChEMBL. Available online: https://www.ebi.ac.uk/chembl (accessed on 1 August 2019).
- DrugBank Database. Available online: https://www.drugbank.ca/ (accessed on 1 August 2019).
- NIH DailyMed. Available online: https://dailymed.nlm.nih.gov (accessed on 1 August 2019).
- Buckley, N. Australian Medicines Handbook; Australasian Society of Clinical and Experimental Pharmacologists and Toxicologists: Hamilton Central, Australia, 2018. [Google Scholar]
- Ghose, A.K.; Crippen, G.M. Atomic Physicochemical Parameters for Three-Dimensional Structure-Directed Quantitative Structure-Activity Relationships, I. Partition Coefficients as a Measure of Hydrophobicity. J. Comput. Chem. 1986, 7, 565–577. [Google Scholar] [CrossRef]
- Cheng, T.; Zhao, Y.; Li, X.; Lin, F.; Xu, Y.; Zhang, X.; Li, Y.; Wang, R.; Lai, L. Computation of Octanol−Water Partition Coefficients by Guiding an Additive Model with Knowledge. J. Chem. Inf. Model 2007, 47, 2140–2148. [Google Scholar] [CrossRef]
- Vogt, A.; Hadam, S.; Heiderhoff, M.; Audring, H.; Lademann, J.; Sterry, W.; Blume-Peytavi, U. Morphometry of human terminal and vellus hair follicles. Exp. Dermatol. 2007, 16, 946–950. [Google Scholar] [CrossRef]
- Meidan, V.M.; Bonner, M.C.; Michniak, B.B. Transfollicular drug delivery—Is it a reality? Int. J. Pharm. 2005, 306, 1–14. [Google Scholar] [CrossRef]
- Lademann, J.; Otberg, N.; Richter, H.; Weigmann, H.; Lindemann, U.; Schaefer, H.; Sterry, W. Investigation of follicular penetration of topically applied substances. Skin Pharmacol. Appl. Skin Physiol. 2000, 14, 17–22. [Google Scholar] [CrossRef]
- Wosicka, H.; Cal, K. Targeting to the hair follicles: Current status and potential. J. Dermatol. Sci. 2010, 57, 83–89. [Google Scholar] [CrossRef]
- Downing, D.T.; Stewart, M.E.; Strauss, J.S. Changes in Sebum Secretion and the Sebaceous Gland. Dermatol. Clin. 1986, 4, 419–423. [Google Scholar] [CrossRef]
- Grams, Y.Y.; Alaruikka, S.; Lashley, L.; Caussin, J.; Whitehead, L.; Bouwstra, J. Permeant lipophilicity and vehicle composition influence accumulation of dyes in hair follicles of human skin. Eur. J. Pharm. Sci. 2003, 18, 329–336. [Google Scholar] [CrossRef]
- Lu, G.W.; Ciotti, S.N.; Valiveti, S.; Grice, J.E.; Cross, S.E. Taregting the pilosebaceous gland. In Dermatologic, Cosmeceutic and Cosmetic Development; Walters, K.A., Roberts, M.S., Eds.; Informa Healthcare: New York, NY, USA, 2008; pp. 169–188. [Google Scholar]
- Lademann, J.; Weigmann, H.-J.; Rickmeyer, C.; Barthelmes, H.; Schaefer, H.; Mueller, G.; Sterry, W. Penetration of Titanium Dioxide Microparticles in a Sunscreen Formulation into the Horny Layer and the Follicular Orifice. Skin Pharmacol. Physiol. 1999, 12, 247–256. [Google Scholar] [CrossRef]
- Patzelt, A.; Richter, H.; Knorr, F.; Schäfer, U.; Lehr, C.-M.; Dähne, L.; Sterry, W.; Lademann, J. Selective follicular targeting by modification of the particle sizes. J. Control. Release 2011, 150, 45–48. [Google Scholar] [CrossRef]
- Radtke, M.; Patzelt, A.; Knorr, F.; Lademann, J.; Netz, R.R. Ratchet effect for nanoparticle transport in hair follicles. Eur. J. Pharm. Biopharm. 2017, 116, 125–130. [Google Scholar] [CrossRef]
- Nastiti, C.M.R.R.; Ponto, T.; Abd, E.; Grice, J.E.; Benson, H.A.E.; Roberts, M.S. Topical Nano and Microemulsions for Skin Delivery. Pharmaceutics 2017, 9, 37. [Google Scholar] [CrossRef]
- Roberts, M.; Mohammed, Y.; Namjoshi, S.; Yousef, S.; Alinaghi, A.; Haridass, I.; Abd, E.; Leite-Silva, V.; Benson, H.; Grice, J.; et al. Topical and cutaneous delivery using nanosystems. J. Control. Release 2017, 247, 86–105. [Google Scholar] [CrossRef] [Green Version]
- Nastiti, C.M.; Mohammed, Y.; Telaprolu, K.C.; Liang, X.; Grice, J.E.; Roberts, M.S.; Benson, H.A. Evaluation of Quantum Dot Skin Penetration in Porcine Skin: Effect of Age and Anatomical Site of Topical Application. Skin Pharmacol. Physiol. 2019, 32, 182–191. [Google Scholar] [CrossRef]
- Garcia-Fuentes, M.; Alonso, M.J. Chitosan-based drug nanocarriers: Where do we stand? J. Control. Release 2012, 161, 496–504. [Google Scholar] [CrossRef]
- Patzelt, A.; Mak, W.C.; Jung, S.; Knorr, F.; Meinke, M.C.; Richter, H.; Rühl, E.; Cheung, K.Y.; Tran, N.B.N.N.; Lademann, J. Do nanoparticles have a future in dermal drug delivery? J. Control. Release 2017, 246, 174–182. [Google Scholar] [CrossRef]
- Müller, R.H.; Radtke, M.A.; Wissing, S. Solid lipid nanoparticles (SLN) and nanostructured lipid carriers (NLC) in cosmetic and dermatological preparations. Adv. Drug Deliv. Rev. 2002, 54, S131–S155. [Google Scholar] [CrossRef]
- Jenning, V.; Gysler, A.; Schäfer-Korting, M.; Gohla, S.H. Vitamin A loaded solid lipid nanoparticles for topical use: Occlusive properties and drug targeting to the upper skin. Eur. J. Pharm. Biopharm. 2000, 49, 211–218. [Google Scholar] [CrossRef]
- Khurana, S.; Bedi, P.; Jain, N. Preparation and evaluation of solid lipid nanoparticles based nanogel for dermal delivery of meloxicam. Chem. Phys. Lipids 2013, 175, 65–72. [Google Scholar] [CrossRef]
- Xia, Q.; Saupe, A.; Muller, R.H.; Souto, E.B. Nanostructured lipid carriers as novel carrier for sunscreen formulations. Int. J. Cosmet. Sci. 2007, 29, 473–482. [Google Scholar] [CrossRef]
- Benson, H.A. Elastic Liposomes for Topical and Transdermal Drug Delivery. Methods Mol. Biol. 2017, 1522, 107–117. [Google Scholar] [CrossRef]
- Tayeb, H.H.; Sainsbury, F. Nanoemulsions in drug delivery: formulation to medical application. Nanomedicine 2018, 13, 2507–2525. [Google Scholar] [CrossRef]
- Rahman, S.A.; Abdelmalak, N.S.; Badawi, A.; Elbayoumy, T.; Sabry, N.; El Ramly, A. Formulation of tretinoin-loaded topical proniosomes for treatment of acne: In-vitro characterization, skin irritation test and comparative clinical study. Drug Deliv. 2015, 22, 731–739. [Google Scholar] [CrossRef]
- Rahman, S.A.; Abdelmalak, N.S.; Badawi, A.; Elbayoumy, T.; Sabry, N.; El Ramly, A. Tretinoin-loaded liposomal formulations: From lab to comparative clinical study in acne patients. Drug Deliv. 2016, 23, 1184–1193. [Google Scholar] [CrossRef]
- Szuts, E.Z.; Hárosi, F.I. Solubility of retinoids in water. Arch. Biochem. Biophys. 1991, 287, 297–304. [Google Scholar] [CrossRef]
- Voelker, R. Tretinoin in New Lotion Formula. JAMA 2018, 320, 1309. [Google Scholar] [CrossRef]
- Kircik, L.H.; Draelos, Z.D.; Berson, D.S. Polymeric Emulsion Technology Applied to Tretinoin. J. Drugs Dermatol. 2019, 18, s148–s154. [Google Scholar]
- Torok, H.M.; Pillai, R. Safety and efficacy of micronized tretinoin gel (0.05%) in treating adolescent acne. J. Drugs Dermatol. 2011, 10, 647–652. [Google Scholar]
- Kircik, L.H.; Baldwin, H.; Guenin, E.; Bhatt, V. Novel tretinoin 0.05% lotion for the once-daily treatment of moderate-to-severe acne vulgaris in an adult and adolescent female population. Int. J. Women Dermatol. 2019, 5, 199. [Google Scholar] [CrossRef]
- Harper, J.C.; Roberts, W.E.; Zeichner, J.A.; Guenin, E.; Bhatt, V.; Pillai, R. Novel tretinoin 0.05% lotion for the once-daily treatment of moderate-to-severe acne vulgaris: Assessment of safety and tolerability in subgroups. J. Dermatol. Treat. 2019, 1–8. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Sugarman, J.L.; Guenin, E.; Harris, S.; Bhatt, V. Novel tretinoin 0.05% lotion for the once-daily treatment of moderate-to-severe acne vulgaris in a preadolescent population. Pediatr. Dermatol. 2019, 36, 193–199. [Google Scholar] [CrossRef]
- Cook-Bolden, F.E.; Weinkle, S.H.; Guenin, E.; Bhatt, V. Novel Tretinoin 0.05% Lotion for Once-Daily Treatment of Moderate-to-Severe Acne Vulgaris in a Hispanic Population. J. Drugs Dermatol. 2019, 18, 32–38. [Google Scholar]
- Tyring, S.K.; Kircik, L.H.; Pariser, D.M.; Guenin, E.; Bhatt, V.; Pillai, R. Novel Tretinoin 0.05% Lotion for the Once-Daily Treatment of Moderate-to-Severe Acne Vulgaris: Assessment of Efficacy and Safety in Patients Aged 9 Years and Older. J. Drugs Dermatol. 2018, 17, 1084–1091. [Google Scholar]
- Webster, G.; Cargill, D.I.; Quiring, J.; Vogelson, C.T.; Slade, H.B. A combined analysis of 2 randomized clinical studies of tretinoin gel 0.05% for the treatment of acne. Cutis 2009, 83, 146–154. [Google Scholar]
- Embil, K.; Nacht, S. The Microsponge® Delivery System (MDS): A topical delivery system with reduced irritancy incorporating multiple triggering mechanisms for the release of actives. J. Microencapsul. 1996, 13, 575–588. [Google Scholar] [CrossRef]
- Wester, R.C.; Patel, R.; Nacht, S.; Leyden, J.; Melendres, J.; Maibach, H. Controlled release of benzoyl peroxide from a porous microsphere polymeric system can reduce topical irritancy. J. Am. Acad. Dermatol. 1991, 24, 720–726. [Google Scholar] [CrossRef]
- Nighland, M.; Grossman, R. Tretinoin microsphere gel in facial acne vulgaris: A meta-analysis. J. Drugs Dermatol. 2008, 7, 2–8. [Google Scholar]
- Raminelli, A.C.P.; Romero, V.; Semreen, M.H.; Leonardi, G.R. Nanotechnological Advances for Cutaneous Release of Tretinoin: An Approach to Minimize Side Effects and Improve Therapeutic Efficacy. Curr. Med. Chem. 2018, 25, 3703–3718. [Google Scholar] [CrossRef]
- Nasrollahi, S.A.; Hassanzade, H.; Moradi, A.; Sabouri, M.; Samadi, A.; Kashani, M.N.; Firooz, A. Safety Assessment of Tretinoin Loaded Nano Emulsion and Nanostructured Lipid Carriers: A Non-invasive Trial on Human Volunteers. Curr. Drug Deliv. 2017, 14, 575–580. [Google Scholar] [CrossRef]
- Sabouri, M.; Samadi, A.; Ahmad Nasrollahi, S.; Farboud, E.S.; Mirrahimi, B.; Hassanzadeh, H.; Nassiri Kashani, M.; Dinarvand, R.; Firooz, A. Tretinoin Loaded Nanoemulsion for Acne Vulgaris: Fabrication, Physicochemical and Clinical Efficacy Assessments. Skin Pharmacol. Physiol. 2018, 31, 316–323. [Google Scholar] [CrossRef]
- Sinico, C.; Manconi, M.; Peppi, M.; Lai, F.; Valenti, D.; Fadda, A.M. Liposomes as carriers for dermal delivery of tretinoin: In vitro evaluation of drug permeation and vesicle–skin interaction. J. Control. Release 2005, 103, 123–136. [Google Scholar] [CrossRef]
- Bavarsad, N.; Akhgari, A.; Seifmanesh, S.; Salimi, A.; Rezaie, A. Statistical optimization of tretinoin-loaded penetration-enhancer vesicles (PEV) for topical delivery. DARU J. Pharm. Sci. 2016, 24, 65. [Google Scholar] [CrossRef]
- Manca, M.L.; Manconi, M.; Nácher, A.; Carbone, C.; Valenti, D.; Maccioni, A.M.; Sinico, C.; Fadda, A.M. Development of novel diolein–niosomes for cutaneous delivery of tretinoin: Influence of formulation and in vitro assessment. Int. J. Pharm. 2014, 477, 176–186. [Google Scholar] [CrossRef]
- Manconi, M.; Sinico, C.; Valenti, D.; Lai, F.; Fadda, A.M. Niosomes as carriers for tretinoin: III. A study into the in vitro cutaneous delivery of vesicle-incorporated tretinoin. Int. J. Pharm. 2006, 311, 11–19. [Google Scholar] [CrossRef]
- Ascenso, A.; Salgado, A.; Euletério, C.; Praça, F.G.; Bentley, M.V.L.B.; Marques, H.C.; Oliveira, H.; Santos, C.; Simões, S. In vitro and in vivo topical delivery studies of tretinoin-loaded ultradeformable vesicles. Eur. J. Pharm. Biopharm. 2014, 88, 48–55. [Google Scholar] [CrossRef]
- Lai, F.; Pireddu, R.; Corrias, F.; Fadda, A.M.; Valenti, D.; Pini, E.; Sinico, C. Nanosuspension improves tretinoin photostability and delivery to the skin. Int. J. Pharm. 2013, 458, 104–109. [Google Scholar] [CrossRef]
- Ridolfi, D.M.; Marcato, P.D.; Justo, G.Z.; Cordi, L.; Machado, D.; Durán, N. Chitosan-solid lipid nanoparticles as carriers for topical delivery of tretinoin. Colloids Surf. B Biointerfaces 2012, 93, 36–40. [Google Scholar] [CrossRef]
- Ourique, A.F.; Melero, A.; Silva, C.D.B.D.; Schaefer, U.F.; Pohlmann, A.R.; Guterres, S.S.; Lehr, C.-M.; Kostka, K.-H.; Beck, R.C.R. Improved photostability and reduced skin permeation of tretinoin: Development of a semisolid nanomedicine. Eur. J. Pharm. Biopharm. 2011, 79, 95–101. [Google Scholar] [CrossRef]
- Raza, K.; Singh, B.; Lohan, S.; Sharma, G.; Negi, P.; Yachha, Y.; Katare, O.P. Nano-lipoidal carriers of tretinoin with enhanced percutaneous absorption, photostability, biocompatibility and anti-psoriatic activity. Int. J. Pharm. 2013, 456, 65–72. [Google Scholar] [CrossRef]
- Smith, J.A.; Narahari, S.; Hill, D.; Feldman, S.R. Tazarotene foam, 0.1%, for the treatment of acne. Expert Opin. Drug Saf. 2016, 15, 99–103. [Google Scholar] [CrossRef]
- Aggarwal, G.; Nagpal, M.; Kaur, G. Development and Comparison of Nanosponge and Niosome based Gel for the Topical Delivery of Tazarotene. Pharm. Nanotechnol. 2016, 4, 213–228. [Google Scholar] [CrossRef]
- Prasad, V.; Chaurasia, S. Performance evaluation of non-ionic surfactant based tazarotene encapsulated proniosomal gel for the treatment of psoriasis. Mater. Sci. Eng. C 2017, 79, 168–176. [Google Scholar] [CrossRef]
- Patel, M.R.; Patel, R.B.; Parikh, J.R.; Patel, B.G. Novel microemulsion-based gel formulation of tazarotene for therapy of acne. Pharm. Dev. Technol. 2016, 21, 921–932. [Google Scholar] [CrossRef]
- Nasr, M.; Abdel-Hamid, S. Optimizing the dermal accumulation of a tazarotene microemulsion using skin deposition modeling. Drug Dev. Ind. Pharm. 2016, 42, 636–643. [Google Scholar] [CrossRef]
- Najafi-Taher, R.; Ghaemi, B.; Amani, A. Delivery of adapalene using a novel topical gel based on tea tree oil nano-emulsion: Permeation, antibacterial and safety assessments. Eur. J. Pharm. Sci. 2018, 120, 142–151. [Google Scholar] [CrossRef]
- Kandekar, S.G.; Lapteva, M.; Kalia, Y.N.; Sancho, S.D.R. Selective delivery of adapalene to the human hair follicle under finite dose conditions using polymeric micelle nanocarriers. Nanoscale 2018, 10, 1099–1110. [Google Scholar] [CrossRef]
- Jain, S.; Kale, D.P.; Swami, R.; Katiyar, S.S. Codelivery of benzoyl peroxide & adapalene using modified liposomal gel for improved acne therapy. Nanomedicine 2018, 13, 1481–1493. [Google Scholar]
- Ramezanli, T.; Zhang, Z.; Michniak-Kohn, B.B. Development and characterization of polymeric nanoparticle-based formulation of adapalene for topical acne therapy. Nanomedicine 2017, 13, 143–152. [Google Scholar] [CrossRef]
- Kumar, V.; Banga, A.K. Intradermal and follicular delivery of adapalene liposomes. Drug Dev. Ind. Pharm. 2016, 42, 871–879. [Google Scholar] [CrossRef]
- Jain, A.K.; Jain, A.; Garg, N.K.; Agarwal, A.; Jain, A.; Jain, S.A.; Tyagi, R.K.; Jain, R.K.; Agrawal, H.; Agrawal, G.P. Adapalene loaded solid lipid nanoparticles gel: An effective approach for acne treatment. Colloids Surf. B Biointerfaces 2014, 121, 222–229. [Google Scholar] [CrossRef]
- Guo, C.; Khengar, R.H.; Sun, M.; Wang, Z.; Fan, A.; Zhao, Y. Acid-Responsive Polymeric Nanocarriers for Topical Adapalene Delivery. Pharm. Res. 2014, 31, 3051–3059. [Google Scholar] [CrossRef]
- Jain, A.; Garg, N.K.; Jain, A.; Kesharwani, P.; Jain, A.K.; Nirbhavane, P.; Tyagi, R.K. A synergistic approach of adapalene-loaded nanostructured lipid carriers, and vitamin C co-administration for treating acne. Drug Dev. Ind. Pharm. 2016, 42, 897–905. [Google Scholar] [CrossRef]
- Sallam, M.A.; Boscá, M.T.M. Mechanistic Analysis of Human Skin Distribution and Follicular Targeting of Adapalene-Loaded Biodegradable Nanospheres With an Insight into Hydrogel Matrix Influence, In Vitro Skin Irritation, and In Vivo Tolerability. J. Pharm. Sci. 2017, 106, 3140–3149. [Google Scholar] [CrossRef]
- Nadal, J.M.; Camargo, G.D.A.; Novatski, A.; Macenhan, W.R.; Dias, D.T.; Barboza, F.M.; Lyra, A.; Roik, J.R.; De Paula, J.P.; Somer, A.; et al. Adapalene-loaded poly(ε-caprolactone) microparticles: Physicochemical characterization and in vitro penetration by photoacoustic spectroscopy. PLoS ONE 2019, 14, e0213625. [Google Scholar] [CrossRef]
- Ramezanli, T.; Michniak-Kohn, B.B. Development and Characterization of a Topical Gel Formulation of Adapalene-TyroSpheres and Assessment of Its Clinical Efficacy. Mol. Pharm. 2018, 15, 3813–3822. [Google Scholar] [CrossRef]
- Bhatia, G.; Zhou, Y.; Banga, A.K. Adapalene Microemulsion for Transfollicular Drug Delivery. J. Pharm. Sci. 2013, 102, 2622–2631. [Google Scholar] [CrossRef]
- Brammann, C.; Mueller-Goymann, C.C. Incorporation of benzoyl peroxide nanocrystals into adapalene-loaded solid lipid microparticles: Part I—Nanocrystalline benzoyl peroxide. Int. J. Pharm. 2019, 564, 171–179. [Google Scholar] [CrossRef]
- Raza, K.; Singh, B.; Singla, N.; Negi, P.; Singal, P.; Katare, O.P. Nano-lipoidal carriers of isotretinoin with anti-aging potential: Formulation, characterization and biochemical evaluation. J. Drug Target. 2013, 21, 435–442. [Google Scholar] [CrossRef]
- Rigopoulos, D.; Larios, G.; Katsambas, A.D. The role of isotretinoin in acne therapy: Why not as first-line therapy? Facts and controversies. Clin. Dermatol. 2010, 28, 24–30. [Google Scholar] [CrossRef]
- Golmohammadzadeh, S.; Mortezania, S.; Jaafari, M.R. Improved photostability, reduced skin permeation and irritation of isotretinoin by solid lipid nanoparticles. Acta Pharm. 2012, 62, 547–562. [Google Scholar]
- Raza, K.; Singh, B.; Singal, P.; Wadhwa, S.; Katare, O.P. Systematically optimized biocompatible isotretinoin-loaded solid lipid nanoparticles (SLNs) for topical treatment of acne. Colloids Surf. B Biointerfaces 2013, 105, 67–74. [Google Scholar] [CrossRef]
- Gürbüz, A.; Özhan, G.; Gungor, S.; Erdal, M.S. Colloidal carriers of isotretinoin for topical acne treatment: Skin uptake, ATR-FTIR and in vitro cytotoxicity studies. Arch. Dermatol. Res. 2015, 307, 607–615. [Google Scholar] [CrossRef]
- Farah, H.A.; Brown, M.B.; McAuley, W.J. Heat Enhanced Follicular Delivery of Isotretinoin to the Skin. Pharm. Res. 2019, 36, 124. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
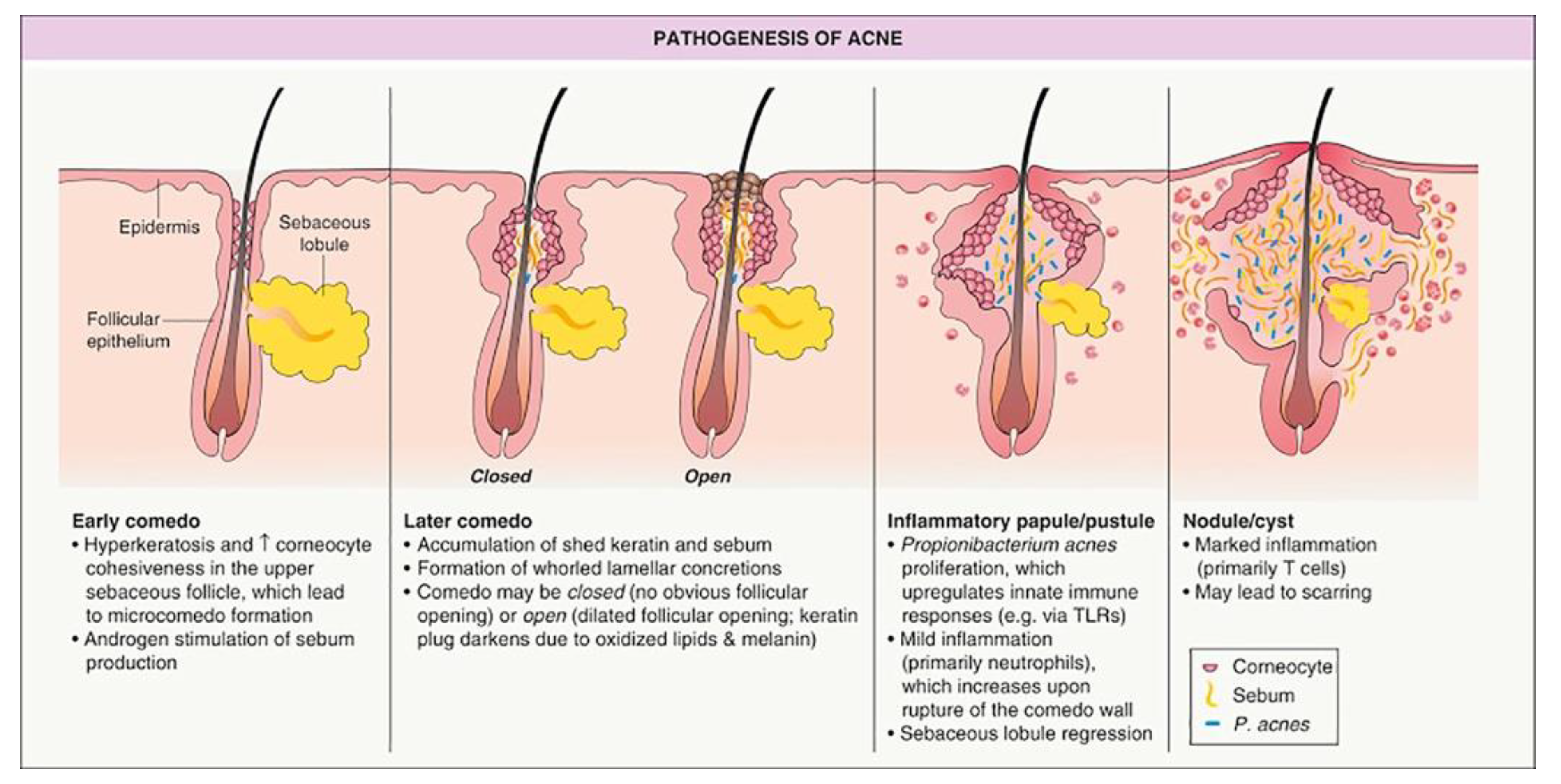
| Type of Lesion | Definition |
|---|---|
| Comedone | Keratin-filled plugs that present superficially on the skin. They can be characterised as open or closed.
|
| Papule | A small, raised lesion that is solid to touch and does not contain fluid. |
| Pustule | A pus-filled lesion caused by increased follicular inflammation and accumulation of inflammatory cells. |
| Cyst | A deeper skin lesion characterised by an enclosed dilated follicle filled with keratin. |
| Nodule | A progression from a cyst, caused by destruction of the integrity of the follicle wall and further inflammation; resulting in a large, solid lesion filled with keratin and pus. |
| Retinoid | Molecular Weight (g/mol) | logP | pKa | Solubility | Available Dosage Forms | Examples of Available Products |
|---|---|---|---|---|---|---|
| Tretinoin | 300.442 | 6.3 logPo/w 5.6 ALogP 6.3 XLogP | 4.76 | Practically insoluble in water (0.025 mg/L at 25 °C), mineral oil and glycerol. Slightly soluble in polyethylene glycol 400 and ethanol. | Cream 0.1%, 0.05%, 0.02%, 0.025% Gel 0.1%, 0.05%, 0.025% Liquid 0.05% Lotion 0.05% Microsphere gel 0.1%, 0.04%, 0.06%, 0.08% | Cream: Retrieve®, Stevia-A®, Retin-A®, Renova®, Rejuva-A® Gel: Retin-A®, Atralin® Liquid: Retin-A® Lotion: Altreno® Microsphere gel: Retin-A Micro® Range of generic products from multiple manufacturers |
| Tazarotene | 351.464 | 5.6 logPo/w 4.43 ALogP 4.9 XLogP | 1.23 | Soluble in water (0.75 mg/L) | Cream 0.1% and 0.05% Gel 0.1% and 0.05% Foam 0.1% | Cream: Zorac®, Tazorac®, Avage® Gel: Zorac®, Tazorac® Foam: Fabior® Range of generic products from multiple manufacturers |
| Adapalene | 412.529 | 8.6 logPo/w 6.68 ALogP 7.7 XLogP | 4.23 | Practically insoluble in water (4.01 μg/L) | Cream 0.1% Gel 0.1% and 0.3% Lotion 0.1% Adapalene 0.1% + BPO 2.5% Adapalene 0.3% + BPO 2.5% | Differin® cream, gel and lotion, and Differin XP gel; also Adaferine® and Differine® internationally Range of generic products from multiple manufacturers Epiduo® gel Epiduo Forte® gel Range of generic products |
| Isotretinoin | 300.442 | 5.66 and 6.3 logPo/w 5.6 ALogP 6.3 XLogP | ~4–5 | Insoluble in water (0.126 mg/L at 25 °C). Sparingly soluble in alcohol | Gel 0.05% isotretinoin Combination 0.05% isotretinoin + 2% erythromycin | Isotrex® gel Isotrexin® gel |
| Formulation Design | Formulation Composition | Methods for Assessing Skin Delivery/Efficacy/Irritation | Physical Characterisation | Delivery/Efficacy/Irritation Outcomes | Reference |
|---|---|---|---|---|---|
| Tretinoin | |||||
| Nanoemulsion (NanoE), nanosuspension (NanoS) | NanoE: Isopropyl myristate 10% Glycerol 2.26%, Soybean lecithin 1.20% Water 86.5%; Tretinoin 0.035% NanoS: Soybean Lecithin 0.0035%, Water 99.9%; Tretinoin 0.035% | Franz diffusion cells/new born piglet skin, tape stripping method (10 strips). | Particle size and (PI): NanoE: ~175 nm (0.09) initially; ~745 nm (0.69) after 90-day stability test NanoS: Approx. 330 nm (0.25) across study period Zeta potential: NanoE: −69.7 mV NanoS: −53.2 mV | Tretinoin delivery as % applied dose: NanoE: Stratum corneum: 6.51 ± 0.82 Epidermis: 4.34 ± 1.12 Dermis: 2.26 ± 1.35 Receptor: 6.64 ± 1.80 NanoS: Stratum corneum: 6.86 ± 1.10 Epidermis: 3.09 ± 0.81 Dermis: 1.65 ± 1.19 Receptor: 0.28 ± 0.10 Nanosuspension is more suitable for targeted delivery with minimal systemic absorption, and has better photostability. | [74] |
| Nanoemulsion (NE) | NE: Caprylic/capric triglyceride 10%, Tween 80 3%, water with preservatives; 0.05% tretinoin Commercial cream (identity undisclosed) as control. | Physical and stability characterisation. No release or skin permeation evaluation. Human split-face study: Ten patients, applied NE and marketed cream to each side of the face daily for 6 weeks. Assessments: TEWL, sebum production, lesions counted and porphyrin assessed by Visiopor® PP 34 N camera (indicates presence of P. acnes). | Particle size (nm ± SD), PI, zeta potential: 116.2 ± 0.07, 0.105 ± 0.006, −47.1 ± 11.17 mV Stability: after 6 months, no statistical difference in measured parameters (p > 0.05). | Significant lesion reduction after 6 weeks of NE use, no significant lesion reduction with marketed tretinoin emulsion. All parameters related to porphyrin production (size, quantity, value of fluorescent spots) were significantly lower in the NE use compared to conventional tretinoin cream. | [68] |
| Nanoemulsion (NE) and Nanostructured Lipid Carriers (NLC) | NE: isopropyl myristate 10%, polysorbate 80 2%, Water; Tretinoin 0.05% NLC: isopropyl myristate 9%, cetyl alcohol 1%, polysorbate 80 2%, Water; Tretinoin 0.05% | 20 human volunteers applied NE and NLC to 2 sites on volar forearm for one week. Hydration, trans-epidermal water loss (TEWL), erythema index and pH were measured. No permeation or efficacy determination. | NE Particle size (nm ± SD); PI; Zeta potential 116.2 ± 1.48; 0.105 ± 0.028; −47.1 ± 5.23 NLC Particle size; PI; Zeta potential 123.3 ± 1.83; 0.098 ± 0.041; −32.8 ± 3.67 | No reported side effects. P values for changes in Hydration, TEWL, erythema index and pH, compared to control measurements taken prior to topical administration: NE: 0.646, 0.139, 0.386 and 0.169, respectively NLC: 0.508, 0.051, 0.139 and 0.333, respectively. p value comparison between NE and NLC for the 4 factors: 0.066, 0.721, 0.386, and 0.241. No statistically difference between formulations. | [67] |
| Liposomes | F13: Phospholipid: cholesterol: dicetylphosphate at ratio 9:1:0.01, dispersed in 1% Carbopol 934 gel; 0.025% tretinoin compared to marketed gel (not disclosed) | Formulation development: 16 formulations evaluated for physical characteristics and release profile (no skin permeation profile determined). Optimised formulation (F13) tested for irritancy (applied to 10 human volunteer’s forearms for 6 h) and efficacy (applied to face of 12 patients with severe acne for 4 weeks) in human volunteers. | F13: particle size 318 ± 28 (nm ± SD); PI 0.434; zeta potential −41.2 ± 1.2; E% 73%. Tretinoin release was 46 ± 5.6% over 5 h. Formulation development trends: adding cholesterol decreased particle size and increased entrapment efficiency (E%). Adding dicetylphosphate increased tretinoin release; no effect on particle size or E%. | Irritation: F13 had significantly lower erythema score (0.2 ± 0.42) compared to same strength tretinoin gel without liposomes (1.8 ± 0.67) and marketed gel (1.4 ± 0.31). Clinical efficacy: F13 had significantly (p > 0.05) better improvement in total acne lesions at 1, 2 and 3 weeks compared to marketed gel | [52] |
| Liposomes | PC (Phospholipon®90) or hydrogenated PC (Phospholipon®90H), cholesterol and tretinoin in a molar ratio of 5:0.6:2 Liposomes were negatively or positively charged by inclusion of dicetylphosphate (DCP: −ve) or stearylamine (SA: +ve) at 2:1 ratio with tretinoin Multilamellar vesicles (MLV) and unilamellar vesicles (ULV: by sonicaltion of MLV). Comparison with three controls: hydroalcoholic solution (WEt), oil solution and Retin-A® cream. | Physical characterisation, tretinoin release (silicone membrane), skin permeation and retention (newborn pig skin) with tape stripping, using Franz diffusion cells TEM of skin to identify liposomes | Particle size (nm ± SD), E% (± SD): MLV P90/SA: 598 ± 67, 71.80 ± 5.1% P90H/SA: 1163 ± 84, 70.01 ± 2.1% P90/DCP: 536 ± 49, 97.32 ± 1.8% P90H/DCP: 993 ± 122, 96.75 ± 2.2% ULV: P90/SA: 297 ± 74, 93.03 ± 1.7% P90H/SA: 205 ± 53, 91.91 ± 1.9% P90/DCP: 293 ± 53, 75.98 ± 2.5% P90H/DCP: 135 ± 56, 78.53 ± 2.6% PI MLV: 0.4 to 0.6; ULV: 0.2 to 0.3 | Tretinoin release trends: −ve > +ve; non-hydrogenated > hydrogenated Skin permeation ranking at 9 h: WEt > P90H/SA > Oil > P90H/DCP > Retin-A > P90/SA > P90/DCP Skin retention ranking at 9 h: P90H/DCP ≈ P90/DCP > P90H/SA > P90/SA > WEt ≈ Oil > Retin-A Local accumulation efficiency ranking (LAC: Retention/permeation): P90/DCP > P90H/DCP > P90/SA > P90H/SA > Oil > Retin-A > WEt Conclusion: negative charge better for skin targeting. TEM did not show any presence of liposomes within the skin layers. | [69] |
| Liposomes, ethosomes, solid lipid nanoparticles (SLN), nanostructured lipid carriers (NLC) | Liposomes: Phosphatidylcholine 400 mg and cholesterol 100 mg, normal saline Ethosomes: Phosphatidylcholine 400 mg, Ethanol ml, normal saline SLN: Phosphatidylcholine 200 mg, Compritol 888 200 mg, Tween 80 1.2 g, Ethanol 0.8 g, water NLC: as SLN except Compritol 888 140 mg, Isopropyl myristate 60 mg All contained tretinoin 0.05%, butyl hydroxy toluene (2.5 mg: antioxidant) and were dispersed in 1.5% Carbopol 934 gel Retin-A® cream as control. | Physical characterisation including photostability and permeation profiles (Franz diffusion cells/ mouse skin with full skin extraction). Skin histology following daily application to mice for 2 weeks and efficacy (anti-psoriatic activity in mouse tail model) following daily application for 3 weeks were evaluated. | Particle size (nm), zeta potential (mV), E% for – Liposomes: 182, 0.67, 65.01 ± 2.31% Ethosomes: 120, −15.6, 76.42 ± 3.92% SLN: 82.3, −20.1, 86.25 ± 4.36% NLC: 79.5, −23.5, 92.13 ± 3.29% | Skin permeation flux (µg·h−1 cm−2): liposomal gel 8.03 ± 0.50 ethosomal gel 9.17 ± 0.61 SLN gel 10.49 ± 0.99 NLC gel 10.89 ± 0.79 Retin-A gel 6.11 ± 0.09 Skin Retention (%): Liposomal gel 8.12 ± 0.09 Ethosomal gel 3.31 ± 0.11 SLN gel 4.28 ± 0.08 NLC gel 5.62 ± 0.12 Retin-A gel 1.52 ± 0.04 Skin histology at 2 weeks: Liposome, SLN and NLC formulations well tolerated; ethosomal gel some inflammation; Retin-A showed greatest inflammation. Author conclusions: For deep skin disorders (i.e., acne) SLN = NLC = ethosomes >> liposomes. For superficial skin disorders (i.e., psoriasis) liposomes = SLN = NLC >> ethosomes. | [77] |
| Ultra-deformable vesicles (UDV) | Phosphatidylcholine (PC) and Tween 80 (combined to produce either 15 or 20% lipid solution) Tretinoin 0.05% compared to Ketrel® cream 0.05% | Tretinoin release and permeation profiles (Franz diffusion cells/ fresh pig ear skin with tape stripping). Cytotoxicity study: human keratinocyte HaCaT cell line. Skin irritation: Draize test in mice. | Particle size: 131 ± 10 (nm ± SD) Zeta potential:−5.9 ± 0.6 | UDV gave sustained and controlled release. Skin penetration and permeation: Tretinoin predominantly in stratum corneum, less in epidermis/dermis (0.372 and 0.050 µg µg/cm2 respectively) with none detected in receptor over 24 h. Cytotoxicity: UDV not cytotoxic at 0.05% tretinoin. Skin irritation: UDV had significantly lower erythema score (<0.5) than marketed formulation. | [73] |
| Proniosomes | P8: Span 60 and cholesterol at ratio 3:1, sorbitol (1 g/mol total Span/cholesterol content), dispersed in 1% Carbopol 934 gel; Tretinoin 0.025% compared to marketed gel (Acretin gel 0.025%) | Formulation development: 9 formulations evaluated for physical characteristics and release profile (no skin permeation profile determined). Optimised formulation (P8) tested for irritancy (applied to 10 human volunteer’s forearms for 6 h) and efficacy (applied to face of 12 patients with severe acne for 4 weeks) in human volunteers. | P8: particle size 330 ± 46 (nm ± SD); PI 0.46; zeta potential −41.2 ± 1.2; EE 94%. Tretinoin release was 46 ± 5.6% over 5 h. Formulation development trends: particle size increased and E% decreased for Span 40 compared to Span 60, and as cholesterol to surfactant ratio increased. | Skin irritation: P8 had significantly lower erythema score (0.14 ± 0.37) compared to same strength tretinoin gel without niosomes (1.7 ± 0.76) and marketed gel (1.5 ± 0.53). Clinical efficacy: P8 had significantly (p > 0.05) better improvement in total acne lesions at all time points up to 4 weeks compared to marketed gel | [51] |
| Niosomes | MLV and ULV niosomes prepared from octyl-decyl polyglucoside (Oramix CG110®) or decyl polyglucoside (Oramix NS10®) to compared effect of lipophilicity and with a −ve (DCP) or +ve (SA) charge. All niosomes contained polyoxyethylene (4) lauryl ether (Brij 30®) and cholesterol. Liposomes contained PC (P90) and cholesterol. All formulations prepared as saturated tretinoin concentrations and 20% of saturated concentration. | Physical characterisation, tretinoin skin permeation and retention (newborn pig skin) with tape stripping, using Franz diffusion cells | Tretinoin saturated ULV particle size range (nm ± SD): 225 ± 29 to 366 ± 46 and E% 75.98 ± 2.5% to 99.50 ± 0.9% Tretinoin saturated MLV size range (nm ± SD): 536 ± 49 to 923 ± 49 and E% 71.80 ± 5.1% to 98.47 ± 0.8% Tretinoin unsaturated ULV size range (nm ± SD): 87 ± 32 to 229 ± 49 Tretinoin unsaturated MLV size range (nm ± SD): 219 ± 59 to 393 ± 53 | For each composition MLV > ULV for tretinoin permeation and ULV > MLV for retention and LAC Tretinoin penetration ranged from 0.221 to 1.104 µg/cm2 (NS10/DCP and (CG110/SA) and retention from 12.81 to 79.47 (CG110/DCP and BR30/DCP). LAC ranking: NS10/DCP ≈ BR30/DCP >> NS10/SA ≈ BR30/SA ≈ P90/DCP > P90/SA >CG110/DCP > CG110/SA >Retin-A | [72] |
| Niosomes (NSV) and liposomes with Labrasol (as PE) | NSV: diolein (Plurol® Oleique CC), cholesterol (5:1) Lab-NSV: diolein, Labrasol (1:1) Liposomes: Phospholipon® 50 Lab-liposomes (Lab-PEV): PC, Labrasol (1.2:1) All formulations 0.25 mg/mL tretinoin | Physical characterisation including stability study (90 days at 4 °C), skin permeation and deposition in stratum corneum (tape stripping), epidermis and dermis using Franz diffusion cells with human abdominal skin. CLSM of fluorescent-labelled vesicles with hydrophilic and lipophilic markers. | Particle size (nm ± SD), Zeta potential (mV), E%: NSV: 156 ± 4, −48 ± 1, 15 ± 9% Lab-NSV: 245 ± 52, −57 ± 2, 79 ± 7% Liposomes: 112 ± 5, −65 ± 5, 96 ± 4% Lab-PEV: 148 ± 18, −82 ± 4, 100 ± 3% Stability: <10% change in all physical measures | Drug deposition in total skin as a % of total applied dose: Liposomes: ~18 Lab-NSVs: ~13 Lab-PEVs: ~9 Diolein-NSVs: ~7 Highest drug deposition was in stratum corneum for all formulations. The addition of labrasol resulted in better drug delivery than addition of diolein. CLSM: Maximum deposition of both markers on stratum corneum surface; lipophilic marker showed no intact vesicles in skin; accumulation of Lab-NSV in hair follicles | [71] |
| Penetration enhancer containing vesicles (PEV) | PC vesicles with addition of different hydrophilic penetration enhancers: Oramix NS10, Labrasol, Transcutol P, Propylene glycol (PG) Tretinoin cream (pharmacy compounded; undisclosed formulation) as comparator. | Physical characterisation including 90-day stability test, ex vivo skin permeation and “retention” (calculated by difference of amount applied and penetrated), using Franz diffusion cells. Histological examination was performed on excised mouse skin. | Particle size ranged from 125 to 164 nm; Zeta potential from −58 to −69 mV; E% ranged from 82 to 91%. Stability: particle size and zeta potential of vesicles with Labrasol and Transcutol remained constant, NS10 and PG vesicles 40% increase in mean diameter. | Tretinoin penetration was higher for PEV than tretinoin cream and “skin retention” lower or similar; LAC was best for tretinoin cream. Note the methodology for “skin retention” is unreliable. Authors reported better histological outcomes for PEV but methodology unreliable as this was performed on excised skin. | [70] |
| SLN with and without chitosan | SLN: myristyl myristate as lipid, with/without chitosan | Physical characterisation including stability study (at 4 °C protected from light), cytotoxicity study (HaCaT cell lines exposed for 24 h then analysed by MTT reduction assay), antimicrobial activity (minimum inhibitory concentration [MIC] on). | Particle size (nm ± SD), PI, zeta potential (mV), E% (± SD): SLN-tretinoin: 162.7 ± 1.4, 0.133 ± 0.014, −31.9 ± 2.0mV, 96.8 ± 1.2% SLN-chitosan-tretinoin: 284.8 ± 15.0, 0.376 ± 0.033, 55.9 ± 3.1, 99.6 ± 0.3% Good stability over one year. | Cytotoxicity: SLN-tretinoin caused 28% decrease in cell viability, SLN-chitosan-tretinoin did not cause cytotoxicity. Antimicrobial activity: SLN-tretinoin had no antibacterial activity, SLN-chitosan-tretinoin activity against microorganisms—MIC (in units of chitosan concentration) of 0.04 and 0.3 mg/mL for P. acnes and S. aureus respectively | [75] |
| Tazarotene | |||||
| Microemulsion (ME) | Multiple ME formulations evaluated, MBG8 selected as optimal based on physical and permeation profile. MBG 8: 10% Labrafac CC 15% Labrasol - Cremophor RH 40 (1:1) 15% Capmul MCM 60% water. ME Gel: above with Carbopol 971P NF 2% Comparator: Tazret® gel 0.05% | Physical characterisation and 6-month stability assessment, permeation through excised rat skin in Franz cells with PBS/95% ethanol (7:3) receptor phase with skin extraction at 12 h. Skin irritation (Draize patch test) on rabbits | Physical parameters at day 0 and 6 months: Particle size (nm): 20.01 ± 1.28 and 22.08 ± 1.17 Polydispersity Index: 0.117 ± 0.034 and 0.119 ± 0.042 Zeta potential: −3.66 ± 0.23 mV and −3.50 ± 0.22 mV E%: 99.89 ± 2.66% and 99.79 ± 2.66% Viscosity (cp): 37 ± 0.05 and 38 ± 0.057 | The permeation profile of MBG8 and Tazret gel were not statistically different but MBG8 had higher skin retention of tazarotene (47.33 ± 0.82 mg, 9.5% of applied dose, compared to 35.00 ± 1.73 mg, 7% of applied dose). MBG8 gel showed no irritation compared to commercial gel which caused moderate erythema. | [81] |
| Adapalene | |||||
| Microemulsion (ME) | ME A: 19% oleic acid 38% Tween 20 38% Transcutol 5% Deionized water ME B: 18% oleic acid 36% Tween 20 36% Transcutol 10% Deionized water ME C: 17% oleic acid 34% Tween 20 34% Transcutol 15% Deionized water ME D: 15% oleic acid 30% Tween 20 30% Transcutol 25% Deionized water Control: solution in oleic acid. All with 0.1% adapalene | Physical characterisation, skin permeation using porcine ear skin on Franz cells with tape stripping (~20 times), follicular casting and extraction from epidermis/dermis. CLSM of ME D distribution in stratum corneum and hair follicles. | Particle size (nm): ME A: 181.09 ± 0.63 ME B: 173.05 ± 1.89 ME C: 144.36 ± 1.01 ME D: 118.01 ± 1.96 ME A, B and C W/O; ME D bi-continuous | Adapalene permeation into stratum corneum and follicles increased with increase in ME water content. ME D had 17-fold greater adapalene follicular deposition than control. CLSM: fluorescence labelled adapalene in ME D penetrated to the base of the hair follicle. The control sample had poor penetration. | [94] |
| Nanoemulsion (NE) | Multiple formulations evaluated. Optimal Tea tree oil NE gel: 6% Tea tree oil 10% dimethylsulfoxide 20% Tween 80 and Span 80 (75:25) 1% Carbopol 934 0.1% adapalene Comparator: marketed adapalene gel 0.1%; adapalene solution in acetonitrile:THF (5:1) | Physical characterisation including stability Permeation and distribution studies using rat skin and PBS:Acetonitrile:THF (3:10:2) as receptor phase. Skin irritation study: applied to NZ white rabbit skin and observed over 72 h Systemic absorption study in rats: applied once a day for 90 days—adapalene content in blood analysed at 45 and 90 days, liver at 90 days. | Particle size, zeta potential: 105 ± 5 nm, 0.073 mV Stability at room temperature for 2 months: all formulations remained transparent; slight increase in mean droplet diameter. | Permeation and distribution: NE; dermis > epidermis > receptor Marketed product: epidermis > dermis > receptor Adapalene solution: receptor > epidermis > dermis [the solvent used will damage the skin barrier so this is not an appropriate control] The use of shaved rat skin and the Franz cell receptor compartment solution of PBS (pH 5.6):Acetonitrile:THF (3:10:2) raises significant questions regarding the validity of this study. This is not a suitable model for human skin. Irritation: NE did not cause any irritation or erythema. Systemic absorption: none detected. | [83] |
| Micelles | Micelles composed of d-α-Tocopheryl polyethylene glycol 1000 succinate (TPGS), a water-soluble, nonionic amphiphilic derivative of vitamin E conjugated with polyethylene glycol 1000. Range of concentrations investigated. Optimal formulation: Micelle solution—TPGS 138 mg/mL, adapalene 0.02% Micelle gel—as above with 1.5% sodium carboxymethyl cellulose Comparators: Differin® gel and Differin® cream—both 0.1% (w/w) | Physical characterisation, stability study of micelle solution and gel at 4 °C for 4 weeks, adapalene delivery into porcine ear skin or human skin in Franz cells over 12 h by extraction from skin and hair follicles, and deposition in hair follicles visualised by CLSM | Particle size <20 nm, PI 0.12 −0.17, E% 87.00 ± 2.31% Stability study: adapalene content and particle size constant over 4 weeks | Delivery (ng/cm2) after infinite dose [and finite dose] applied to pig ear skin for 12 h: Micelle solution: 907 ± 244 [230 ± 47] Micelle gel: 951 ± 382 [194 ± 38] Differin gel: 832 ± 183 [498 ± 60] Differin cream: 112 ± 30 [98 ± 39] (Micelle and Differin gel equivalent and significantly more than Differin cream—despite Differin 5x adapalene dose of micelles). Delivery to human skin was statistically equivalent to pig skin data. Delivery to pileosebaceous units in human skin (% of applied dose): Micelle solution: 19.2 ± 6.5% Micelle gel: 18.4 ± 9.7% Differin gel: 5.82 ± 2.32% Differin cream: 2.02 ± 0.64% | [84] |
| Liposomes | Optimized formulation: Lipid mixture: Phospholipon 90H® 72% and cholesterol 28%, 1% adapalene Comparators: Differin gel; 1% adapalene solution in PEG 400. | Physical characterisation, 3-month stability at 25 °C, 4 °C and −25 °C, in vitro skin permeation and deposition with pig ear skin on Franz cells, followed by tape stripping, cyanoacrylate casting of follicles and skin extraction. CLSM for visualising liposome location. | SLN particle size (nm), E%: 86.66 ± 3.5, 97.01 ± 1.84% Stability: little change in particle size or E% at 4 and −25 °C, but 4x increase in diameter and E% changed from 97% to 85% at 25 °C. | Adapalene permeation (µg/cm2) into hair follicles: Liposome formulation: 6.72 ± 0.83 Differin gel: 3.33 ± 0.26 Adapalene solution: 1.62 ± 0.054 Adapalene permeation (µg/cm2) into epidermis/dermis: Liposome formulation: 1.75 ± 0.33 Differin gel: negligible Adapalene solution: 0.92 ± 0.26 CLSM: adapalene-loaded liposomes were located in the follicle and associated with the hair shaft | [87] |
| Solid lipid nanoparticles (SLN) | SLN: tristearin 1%, soya lecithin 0.3%, Tween 80 0.2% with adapalene 0.1%. SLN-gel: SLN dispersed in Carbopol 934 1% aqueous gel. Comparator: adapalene solution in undisclosed solvent. | Physical characterization including release using cellulose dialysis membrane. Skin permeation with rat skin in Franz cells (using 80% (v/v) methanol in PBS as receptor phase) over 24 h, followed by separation of skin layers. Histopathology of FITC-labelled SLN after 8 h application to shaved abdominal rat skin. | SLN particle size (nm), zeta potential and E%: 148.3 ± 2.5, −12.0 mV, 89.90 ± 1.2% Adapalene release from SLN: fast burst release initially followed by slower, sustained drug release. | Rat skin permeation of adapalene: SLN and SLN-gel: epidermis > dermis > receptor. Adapalene solution: receptor > epidermis > dermis Histopathology: poor quality images show widespread fluorescence. Note that the skin permeation model is problematic: rat skin is much more permeable than human skin and the receptor phase would damage the skin (and there was no integrity testing of skin membrane). | [88] |
| Polymeric Nanoparticles | Eudragit EPO with adapalene (ratio 5:1), 1% aqueous PVA Comparator adapalene in Transcutol solution | Physical characterisation, drug release and permeation using Franz cells and fresh pig back skin, followed by tape stripping 20 times | Particle size (nm), zeta potential, E%: 125.8 ± 3.5, 18.4 ± 2.9 mV, 3.5 ± 0.3% Nanocarriers were amorphous and adapalene crystallinity decreased upon loading. | Adapalene release: steady state flux through silicone membrane = 6.5 ± 0.6 and 3.9 ± 0.4 μg.cm−2·h−1 for nanoparticles and Transcutol solution respectively. Equivalent amounts of adapalene in stratum corneum after 24 h. | [89] |
| Polymeric microparticles | Poly-ε-caprolactone (PCL) microparticles formulated: F0: adapalene 0% Polysorbate 80 0.5 g PCL 2 g F10: adapalene 10% Polysorbate 80 0.5 g Purified water 200 mL PCL 1.8 g Adapalene 0.2 g F20: adapalene 20% Polysorbate 80 0.5 g PCL 1.6 g Adapalene 0.4 g Comparator: physical mixture (PM) of PCL and adapalene at 1:1 ratio | Physical characterization and diffusion across Strat-M membrane with photoacoustic spectroscopy | Particle size (µm), E%: F0: 8 ± 4 µm F10: 8 ± 3 µm, 100.44% F20: 7 ± 3 µm, 99.37% Spherical in shape | Photoacoustic spectroscopy showed that microencapsulation decreased the in vitro transmembrane diffusion of adapalene compared to the physical mixture, with the microparticle formulations predominantly on or in the membrane. | [92] |
| Polymeric nanoparticles (NS) | PCL-NS: poly-ε-caprolactone (PCL) with adapalene (ratio 10:1), 1% PVA as stabiliser PCL-NS dispersed in 2 aqueous gels: NS-HPMC gel: hydroxypropyl methylcellulose (HPMC) 4% NS-HA gel: sodium hyaluronic acid (HA) 1% Comparator: marketed adapalene 0.1% gel | Physical characterisation, ex vivo skin permeation and distribution with human abdominal skin (single male donor) on Franz diffusion cells over 24 h, followed by tape stripping and separation of epidermis and dermis. CLSM of FITC-NS for skin deposition visualisation. Skin compatibility study: human dermal fibroblasts exposed NS for 48 h. Skin irritation: Draize patch test in rabbits for NS gels and marketed gel application over 7 days. | NS particle size (nm), zeta potential and E%: 107.5 ± 8.19, −13.1 mV, 84.73 ± 1.52% Gels provided sustained release of adapalene over 24 h due to hydrophobic NS and hydrophilic gel matrix. | In vitro skin penetration of adapalene in combined skin tissues: NS-HA gel > NS dispersion > NS-HPMC ≈ marketed gel. Penetration to receptor was minimal for all. Skin compatibility: Cells treated with adapalene alone caused a dose related reduction in cell viability. Cells treated with the adapalene NS caused a lower reduction in cell viability. Skin irritation: Adapalene NS in both gel formulations produced no irritation in the first 3 days, and less irritation than marketed adapalene over 7 days. The HA gel produced less irritation than the HPMC gel. | [91] |
| NLC | NLC: 1% w/w tristearin and Labrasol (4:1), 0.3% w/v phospholipid 90NG, 0.2% w/v Tween 80 with Adapalene 100 mg NLC-gel: above with 1% Carbopol 934. NLC-AP gel: above. Comparator: adapalene gel 0.1% w/w (Adapen® gel) | Physical characterisation and skin permeation with rat skin in Franz cells (using 75% (v/v) methanol and DMF (50:1) in PBS as receptor phase) over 24 h, separation of skin layers. | Particle size 268.3 ± 2.5 nm, zeta potential −16.35 ± 0.21, E% 87.29 ± 1.26% | Adapalene deposition in epidermis and dermis was similar for all NLC formulations and significantly higher than Adapen gel. Note that the skin permeation model is problematic: rat skin is much more permeable than human skin and the receptor phase would damage the skin (and there was no integrity testing of skin membrane). | [90] |
| Isotretinoin | |||||
| SLN | Multiple SLN formulations evaluated. SLN optimized formulation: Compritol 888 ATO 674 mg Phospholipon 90G 208.5 mg Tween 80 Isotretinoin 0.05% Comparator: Sotret® gel 0.05% isotretinoin | Physical characterisation and stability at 5, 30 and 65 °C for 12 months, permeation in Franz cells with hairless laca mouse skin, followed by skin extraction. Skin histology following daily application to mice for 2 weeks and efficacy on testosterone induced acne model in mice. | Particle size (nm), PI, zeta potential, E%: 75.3 ± 2.4, 0.139, −22.4 mV, 89.49 ± 4.1% Stability after 12 months: SLN formulation, drug content ranged between 97.45% and 102.13% | Permeation and retention range used for optimisation of SLN: 8.85 to 27.29 µg.cm−2·h−1 and 4.63 to 22.63 µg·cm−2 Skin histology: SLN showed no inflammation; Sotret gel showed inflammation. Testosterone acne model: SLN formulation showed significant improvement in lesion development (p < 0.001) compared to marketed formulation. | [99] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latter, G.; Grice, J.E.; Mohammed, Y.; Roberts, M.S.; Benson, H.A.E. Targeted Topical Delivery of Retinoids in the Management of Acne Vulgaris: Current Formulations and Novel Delivery Systems. Pharmaceutics 2019, 11, 490. https://doi.org/10.3390/pharmaceutics11100490
Latter G, Grice JE, Mohammed Y, Roberts MS, Benson HAE. Targeted Topical Delivery of Retinoids in the Management of Acne Vulgaris: Current Formulations and Novel Delivery Systems. Pharmaceutics. 2019; 11(10):490. https://doi.org/10.3390/pharmaceutics11100490
Chicago/Turabian StyleLatter, Gemma, Jeffrey E. Grice, Yousuf Mohammed, Michael S. Roberts, and Heather A. E. Benson. 2019. "Targeted Topical Delivery of Retinoids in the Management of Acne Vulgaris: Current Formulations and Novel Delivery Systems" Pharmaceutics 11, no. 10: 490. https://doi.org/10.3390/pharmaceutics11100490