
Cytomegalovirus Diseases of the Gastrointestinal Tract in Immunocompetent Patients: A Narrative Review
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
3. Results
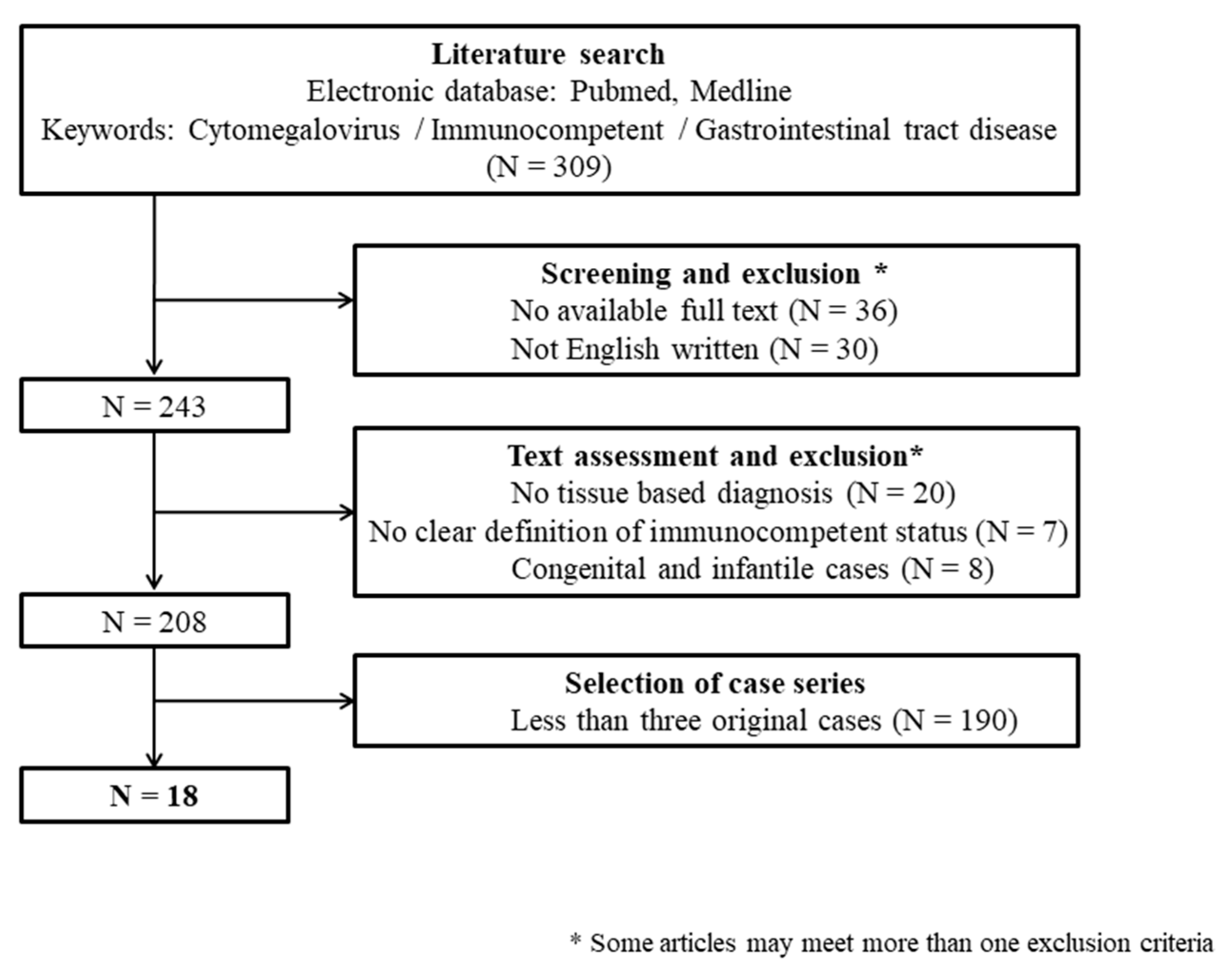
3.1. Literature Search
3.2. Epidemiology
3.3. Clinical Presentations
3.4. Diagnosis
3.5. Treatment
3.6. Outcomes and Prognostic Factors
3.7. Risk Factors, Comorbidities, and Special Populations
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Herbein, G. Tumors and Cytomegalovirus: An Intimate Interplay. Viruses 2022, 14, 812. [Google Scholar] [CrossRef]
- You, D.M.; Johnson, M.D. Cytomegalovirus infection and the gastrointestinal tract. Curr. Gastroenterol. Rep. 2012, 14, 334–342. [Google Scholar] [CrossRef]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef]
- Gandhi, M.K.; Khanna, R. Human cytomegalovirus: Clinical aspects, immune regulation, and emerging treatments. Lancet Infect. Dis. 2004, 4, 725–738. [Google Scholar] [CrossRef]
- Staras, S.A.; Dollard, S.C.; Radford, K.W.; Flanders, W.D.; Pass, R.F.; Cannon, M.J. Seroprevalence of cytomegalovirus infection in the United States, 1988–1994. Clin. Infect. Dis. 2006, 43, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Limaye, A.P.; Kirby, K.A.; Rubenfeld, G.D.; Leisenring, W.M.; Bulger, E.M.; Neff, M.J.; Gibran, N.S.; Huang, M.L.; Santo Hayes, T.K.; Corey, L.; et al. Cytomegalovirus reactivation in critically ill immunocompetent patients. JAMA 2008, 300, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Nakase, H.; Herfarth, H. Cytomegalovirus Colitis, Cytomegalovirus Hepatitis and Systemic Cytomegalovirus Infection: Common Features and Differences. Inflamm. Intest. Dis. 2016, 1, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Lancini, D.; Faddy, H.M.; Flower, R.; Hogan, C. Cytomegalovirus disease in immunocompetent adults. Med. J. Aust. 2014, 201, 578–580. [Google Scholar] [CrossRef]
- Rafailidis, P.I.; Mourtzoukou, E.G.; Varbobitis, I.C.; Falagas, M.E. Severe cytomegalovirus infection in apparently immunocompetent patients: A systematic review. Virol. J. 2008, 5, 47. [Google Scholar] [CrossRef]
- Eddleston, M.; Peacock, S.; Juniper, M.; Warrell, D.A. Severe cytomegalovirus infection in immunocompetent patients. Clin. Infect. Dis. 1997, 24, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Osawa, R.; Singh, N. Cytomegalovirus infection in critically ill patients: A systematic review. Crit. Care 2009, 13, R68. [Google Scholar] [CrossRef] [PubMed]
- Yeh, P.J.; Wu, R.C.; Chiu, C.T.; Lai, M.W.; Chen, C.M.; Pan, Y.B.; Su, M.Y.; Kuo, C.J.; Lin, W.R.; Le, P.H. Cytomegalovirus Diseases of the Gastrointestinal Tract. Viruses 2022, 14, 352. [Google Scholar] [CrossRef]
- Wetwittayakhlang, P.; Rujeerapaiboon, N.; Wetwittayakhlung, P.; Sripongpun, P.; Pruphetkaew, N.; Jandee, S.; Chamroonkul, N.; Piratvisuth, T. Clinical Features, Endoscopic Findings, and Predictive Factors for Mortality in Tissue-Invasive Gastrointestinal Cytomegalovirus Disease between Immunocompetent and Immunocompromised Patients. Gastroenterol. Res. Pract. 2021, 2021, 8886525. [Google Scholar] [CrossRef]
- Fakhreddine, A.Y.; Frenette, C.T.; Konijeti, G.G. A Practical Review of Cytomegalovirus in Gastroenterology and Hepatology. Gastroenterol. Res. Pract. 2019, 2019, 6156581. [Google Scholar] [CrossRef]
- Ljungman, P.; Boeckh, M.; Hirsch, H.H.; Josephson, F.; Lundgren, J.; Nichols, G.; Pikis, A.; Razonable, R.R.; Miller, V.; Griffiths, P.D.; et al. Definitions of Cytomegalovirus Infection and Disease in Transplant Patients for Use in Clinical Trials. Clin. Infect. Dis. 2016, 64, 87–91. [Google Scholar] [CrossRef]
- Goodman, A.L.; Murray, C.D.; Watkins, J.; Griffiths, P.D.; Webster, D.P. CMV in the gut: A critical review of CMV detection in the immunocompetent host with colitis. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 13–18. [Google Scholar] [CrossRef]
- Surawicz, C.M.; Myerson, D. Self-limited cytomegalovirus colitis in immunocompetent individuals. Gastroenterology 1988, 94, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Dreese, J.C.; Poritz, L.S.; Koltun, W.A. Cytomegalovirus enteritis: A highly lethal condition requiring early detection and intervention. Dis. Colon. Rectum 1998, 41, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Ng, F.H.; Chau, T.N.; Cheung, T.C.; Kng, C.; Wong, S.Y.; Ng, W.F.; Lee, K.C.; Chan, E.; Lai, S.T.; Yuen, W.C.; et al. Cytomegalovirus colitis in individuals without apparent cause of immunodeficiency. Dig. Dis. Sci. 1999, 44, 945–952. [Google Scholar] [CrossRef]
- Patra, S.; Samal, S.C.; Chacko, A.; Mathan, V.I.; Mathan, M.M. Cytomegalovirus infection of the human gastrointestinal tract. J. Gastroenterol. Hepatol. 1999, 14, 973–976. [Google Scholar] [CrossRef]
- Maiorana, A.; Baccarini, P.; Foroni, M.; Bellini, N.; Giusti, F. Human cytomegalovirus infection of the gastrointestinal tract in apparently immunocompetent patients. Hum. Pathol. 2003, 34, 1331–1336. [Google Scholar] [CrossRef]
- Ng, K.L.; Ho, J.; Ng, H.S.; Luman, W. Gastrointestinal Cytomegalovirus infection in non-human immunodeficiency virus infected patients. Med. J. Malays. 2003, 58, 337–344. [Google Scholar]
- Reggiani Bonetti, L.; Losi, L.; Di Gregorio, C.; Bertani, A.; Merighi, A.; Bettelli, S.; Scuri, M.; Maiorana, A. Cytomegalovirus infection of the upper gastrointestinal tract: A clinical and pathological study of 30 cases. Scand. J. Gastroenterol. 2011, 46, 1228–1235. [Google Scholar] [CrossRef]
- Siciliano, R.F.; Castelli, J.B.; Randi, B.A.; Vieira, R.D.; Strabelli, T.M. Cytomegalovirus colitis in immunocompetent critically ill patients. Int. J. Infect. Dis. 2014, 20, 71–73. [Google Scholar] [CrossRef]
- Chen, Y.-M.; Hung, Y.-P.; Huang, C.-F.; Lee, N.-Y.; Chen, C.-Y.; Sung, J.-M.; Chang, C.-M.; Chen, P.-L.; Lee, C.-C.; Wu, Y.-H.; et al. Cytomegalovirus disease in nonimmunocompromised, human immunodeficiency virus-negative adults with chronic kidney disease. J. Microbiol. Immunol. Infect. 2014, 47, 345–349. [Google Scholar] [CrossRef]
- Chan, K.-S.; Yang, C.-C.; Chen, C.-M.; Yang, H.-H.; Lee, C.-C.; Chuang, Y.-C.; Yu, W.-L. Cytomegalovirus colitis in intensive care unit patients: Difficulties in clinical diagnosis. J. Crit. Care 2014, 29, 474.e1–474.e6. [Google Scholar] [CrossRef]
- Ko, J.H.; Peck, K.R.; Lee, W.J.; Lee, J.Y.; Cho, S.Y.; Ha, Y.E.; Kang, C.I.; Chung, D.R.; Kim, Y.H.; Lee, N.Y.; et al. Clinical presentation and risk factors for cytomegalovirus colitis in immunocompetent adult patients. Clin. Infect. Dis. 2015, 60, e20–e26. [Google Scholar] [CrossRef]
- Bernard, S.; Germi, R.; Lupo, J.; Laverrière, M.H.; Masse, V.; Morand, P.; Gavazzi, G. Symptomatic cytomegalovirus gastrointestinal infection with positive quantitative real-time PCR findings in apparently immunocompetent patients: A case series. Clin. Microbiol. Infect. 2015, 21, 1121.e1–1121.e7. [Google Scholar] [CrossRef]
- Marques, S.; Carmo, J.; Pinto, D.; Bispo, M.; Ramos, S.; Chagas, C. Cytomegalovirus Disease of the Upper Gastrointestinal Tract: A 10-Year Retrospective Study. GE Port. J. Gastroenterol. 2017, 24, 262–268. [Google Scholar] [CrossRef]
- Chaemsupaphan, T.; Limsrivilai, J.; Thongdee, C.; Sudcharoen, A.; Pongpaibul, A.; Pausawasdi, N.; Charatcharoenwitthaya, P. Patient characteristics, clinical manifestations, prognosis, and factors associated with gastrointestinal cytomegalovirus infection in immunocompetent patients. BMC Gastroenterol. 2020, 20, 22. [Google Scholar] [CrossRef]
- Yoon, J.; Lee, J.; Kim, D.S.; Lee, J.W.; Hong, S.W.; Hwang, H.W.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Ye, B.D.; et al. Endoscopic features and clinical outcomes of cytomegalovirus gastroenterocolitis in immunocompetent patients. Sci. Rep. 2021, 11, 6284. [Google Scholar] [CrossRef]
- Verma, A.; Girish, M.I.; Dahale, A.S.; Dalal, A.; Sachdeva, S. CMV Colitis in Immunocompetent Patients—A Case Series. J. Dig. Endosc. 2021, 12, 245–246. [Google Scholar] [CrossRef]
- Frantzeskaki, F.G.; Karampi, E.S.; Kottaridi, C.; Alepaki, M.; Routsi, C.; Tzanela, M.; Vassiliadi, D.A.; Douka, E.; Tsaousi, S.; Gennimata, V.; et al. Cytomegalovirus reactivation in a general, nonimmunosuppressed intensive care unit population: Incidence, risk factors, associations with organ dysfunction, and inflammatory biomarkers. J. Crit. Care 2015, 30, 276–281. [Google Scholar] [CrossRef]
- Lin, Y.H.; Yeh, C.J.; Chen, Y.J.; Chang, M.C.; Su, I.H.; Cheng, H.T. Recurrent cytomegalovirus colitis with megacolon in an immunocompetent elderly man. J. Med. Virol. 2010, 82, 638–641. [Google Scholar] [CrossRef]
- Cho, J.H.; Choi, J.H. Cytomegalovirus ileo-pancolitis presenting as toxic megacolon in an immunocompetent patient: A case report. World J. Clin. Cases 2020, 8, 552–559. [Google Scholar] [CrossRef]
- Buckner, F.S.; Pomeroy, C. Cytomegalovirus disease of the gastrointestinal tract in patients without AIDS. Clin. Infect. Dis. 1993, 17, 644–656. [Google Scholar] [CrossRef]
- Petrogiannopoulos, C.L.; Kalogeropoulos, S.G.; Dandakis, D.C.; Hartzoulakis, G.A.; Karahalios, G.N.; Flevaris, C.P.; Zacharof, A.K. Cytomegalovirus enteritis in an immunocompetent host. Chemotherapy 2004, 50, 276–278. [Google Scholar] [CrossRef]
- Yun, E.J.; Han, J.K.; Choi, B.I. Cytomegalovirus proctitis in a diabetic. Abdom. Imaging 1999, 24, 39–41. [Google Scholar] [CrossRef]
- Ashida, Y.; Kashihara, T.; Masuda, E.; Doi, Y.; Murayama, Y.; Okuno, M.; Kimura, F. A case of cytomegalovirus proctitis associated with both rectovaginal and rectovesical fistulae. Gastroenterol. Endosc. 2006, 48, 1577–1584. [Google Scholar] [CrossRef]
- Alam, I.; Shanoon, D.; Alhamdani, A.; Boyd, A.; Griffiths, A.P.; Baxter, J.N. Severe proctitis, perforation, and fatal rectal bleeding secondary to cytomegalovirus in an immunocompetent patient: Report of a case. Surg. Today 2007, 37, 66–69. [Google Scholar] [CrossRef]
- Cha, J.M.; Lee, J.I.; Choe, J.W.; Joo, K.R.; Jung, S.W.; Shin, H.P.; Choi, S.I. Cytomegalovirus enteritis causing ileal perforation in an elderly immunocompetent individual. Yonsei Med. J. 2010, 51, 279–283. [Google Scholar] [CrossRef]
- Tejedor Cerdeña, M.A.; Velasco Guardado, A.; Fernández Prodomingo, A.; Concepción Piñero Pérez, M.C.; Calderón, R.; Prieto Bermejo, A.B.; Sánchez Garrido, A.; Martínez Moreno, J.; Geijo Martínez, F.; Blanco Múñez, O.J.; et al. Cytomegalovirus ileitis in an immunocompetent patient. Rev. Esp. Enferm. Dig. 2011, 103, 154–156. [Google Scholar] [CrossRef]
- Dinesh, B.V.; Selvaraju, K.; Kumar, S.; Thota, S. Cytomegalovirus-induced colonic stricture presenting as acute intestinal obstruction in an immunocompetent adult. BMJ Case Rep. 2013, 2013, bcr2013200944. [Google Scholar] [CrossRef]
- Park, J.-W.; Kim, K.; Yoon, S.-W.; Kim, D. Cytomegalovirus Enteritis in an Immunocompetent Patient Causing Small Bowel Obstruction and Superior Mesenteric Artery Thrombosis: A Case Report. J. Korean Soc. Radiol. 2014, 71, 26. [Google Scholar] [CrossRef]
- Hasegawa, T.; Aomatsu, K.; Nakamura, M.; Aomatsu, N.; Aomatsu, K. Cytomegalovirus colitis followed by ischemic colitis in a non-immunocompromised adult: A case report. World J. Gastroenterol. 2015, 21, 3750–3754. [Google Scholar] [CrossRef]
- Chidlovskii, E.; Deroux, A.; Bernard, S.; Couturier, P. Cytomegalovirus colitis mimicking rectal carcinoma in an immunocompetent elderly woman. BMJ Case Rep. 2016, 2016, bcr2016214694. [Google Scholar] [CrossRef]
- Krajicek, E.; Shivashankar, R.; Hansel, S. Cytomegalovirus and the Seemingly Immunocompetent Host: A Case of a Perforating Gastric Ulcer. ACG Case Rep. J. 2017, 4, e27. [Google Scholar] [CrossRef]
- D’Cruz, R.T.; Lau, C.C.; Thamboo, T.P. Severe ischemic cytomegalovirus proctocolitis with multiple perforation. Arch. Virol. 2018, 163, 1927–1931. [Google Scholar] [CrossRef]
- Stilwell, K.T.; Estes, J.; Kurtz, M.T.; Francis, J.M.; Lynch, D.T.; Patel, A.A. CMV Ileitis: To Treat or Not to Treat? Implications of Initiating Biologic Therapy for Concurrent Crohn’s Disease. Case Rep. Gastrointest. Med. 2019, 2019, 4513795. [Google Scholar] [CrossRef]
- Santacruz, C.C.; Carlin, P.S.; Rancano, R.S.; Medina, L.O.; Miguel, J.C. Segmental cytomegalovirus colitis mimicking sigmoid tumor in an immunocompetent patient. Turk. J. Gastroenterol. 2019, 30, 932–934. [Google Scholar] [CrossRef]
- Kanafani, Z.; Sharara, A.; Shabb, N.; Kanj, S. Cytomegalovirus Appendicitis Following Acute Epstein-Barr Virus Infection in an Immunocompetent Patient. Scand. J. Infect. Dis. 2004, 36, 505–507. [Google Scholar] [CrossRef]
- Pasticci, M.B.; Corsi, S.; Spigarelli, F.; Correnti, S.; Francisci, D.; Castronari, R.; Baldin, P.; Prosperini, A.; Baldelli, F.; Cenci, E.; et al. Acute appendicitis due to Cytomegalovirus in an apparently immunocompetent patient: A case report. J. Med. Case Rep. 2014, 8, 92. [Google Scholar] [CrossRef]
- Canterino, J.E.; McCormack, M.; Gurung, A.; Passarelli, J.; Landry, M.L.; Golden, M. Cytomegalovirus appendicitis in an immunocompetent host. J. Clin. Virol. 2016, 78, 9–11. [Google Scholar] [CrossRef]
- Morunglav, M.; Theate, I.; Bertin, G.; Hantson, P. CMV enteritis causing massive intestinal hemorrhage in an elderly patient. Case Rep. Med. 2010, 2010, 385795. [Google Scholar] [CrossRef]
- D’Alessandro, M.; Buoncompagni, A.; Minoia, F.; Coccia, M.C.; Martini, A.; Picco, P. Cytomegalovirus-related necrotising vasculitis mimicking Henoch-Schönlein syndrome. Clin. Exp. Rheumatol. 2014, 32, S73–S75. [Google Scholar]
- Puerta, A.; Priego, P.; Galindo, J. Cytomegalovirus: Associated ischemic colitis in an immunocompetent patient. Rev. Esp. Enferm. Dig. 2017, 109, 671. [Google Scholar] [CrossRef]
- Nakase, H.; Itani, T.; Mimura, J.; Takeuchi, R.; Kawasaki, T.; Komori, H.; Hashimoto, K.; Chiba, T. Transient protein-losing enteropathy associated with cytomegalovirus infection in a noncompromised host: A case report. Am. J. Gastroenterol. 1998, 93, 1005–1006. [Google Scholar] [CrossRef]
- Suter, W.R.; Neuweiler, J.; Borovicka, J.; Binek, J.; Fantin, A.C.; Meyenberger, C. Cytomegalovirus-Induced Transient Protein-Losing Hypertrophic Gastropathy in an Immunocompetent Adult. Digestion 2000, 62, 276–279. [Google Scholar] [CrossRef]
- Setakhr, V.; Muller, G.; Hoang, P.; Lambert, A.S.; Geubel, A. Cytomegalovirus-associated protein losing gastropathy in an immunocompetent adult: A case report. Acta Gastroenterol. Belg. 2007, 70, 296–299. [Google Scholar]
- Canan, O.; Ozçay, F.; Bilezikçi, B. Ménétrier’s disease and severe gastric ulcers associated with cytomegalovirus infection in an immunocompetent child: A case report. Turk. J. Pediatr. 2008, 50, 291–295. [Google Scholar]
- Lalazar, G.; Doviner, V.; Ben-Chetrit, E. Unfolding the Diagnosis. N. Engl. J. Med. 2014, 370, 1344–1348. [Google Scholar] [CrossRef]
- Perrineau, S.; Cazals-Hatem, D.; Zarrouk, V.; Fantin, B.; de Lastours, V. Cytomegalovirus-associated protein-losing enteropathy in a healthy man. Med. Mal. Infect. 2017, 47, 562–565. [Google Scholar] [CrossRef]
- Ochiai, Y.; Hoteya, S.; Kono, K.; Takazawa, Y.; Matsui, A.; Kikuchi, D. Cytomegalovirus ileitis with protein-losing enteropathy in an immunocompetent adult. Clin. J. Gastroenterol. 2021, 14, 1060–1066. [Google Scholar] [CrossRef]
- Solito, S.; Marino, M.; Pevere, S.; Scardino, G.; MacChini, F.; Vadalà Di Prampero, S.F.; Zilli, M. Gastroparesis and pancytopenia due to cytomegalovirus infection in an immunocompetent host. Dig. Liver Dis. 2018, 50, e189–e190. [Google Scholar] [CrossRef]
- Kim, B.S.; Park, S.Y.; Kim, D.H.; Kim, N.I.; Yoon, J.H.; Ju, J.K.; Park, C.H.; Kim, H.S.; Choi, S.K. Cytomegalovirus colitis induced segmental colonic hypoganglionosis in an immunocompetent patient: A case report. World J. Clin. Cases 2021, 9, 5631–5636. [Google Scholar] [CrossRef]
- Kurtz, M.; Morgan, M. Concomitant Clostridium difficile colitis and cytomegalovirus colitis in an immunocompetent elderly female. BMJ Case Rep. 2012, 2012, bcr2012007273. [Google Scholar] [CrossRef]
- Chen, S.; Lalazar, G.; Barak, O.; Adar, T.; Doviner, V.; Mizrahi, M. Protein-Loosing Entropathy Induced by Unique Combination of CMV and HP in an Immunocompetent Patient. Case Rep. Med. 2012, 2012, 361892. [Google Scholar] [CrossRef]
- Dumitru, I.M.; Dumitru, E.; Resul, G.; Curtali, L.; Paris, S.; Rugina, S. Concomitant CMV and Clostridium difficile colitis in an immunocompetent patient treated with Ganciclovir and fecal transplantation. J. Gastrointestin Liver Dis. 2014, 23, 221–222. [Google Scholar]
- Claeys, M.; Cool, M.; Lambrecht, G.L.; Hertveldt, K.; Alliet, G.; Deboever, G. CMV gastritis in the immunocompetent host. Acta Gastroenterol. Belg. 2015, 78, 244–245. [Google Scholar]
- Chen, P.-H.; Lu, I.T.; Lee, B.-J.; Wang, C.-Y.; Lee, C.-K. Age can be a Problem: Clostridium difficile and Cytomegalovirus Colitis Coinfection in an Immunocompetent 90-year-old Patient. Int. J. Gerontol. 2015, 9, 130–132. [Google Scholar] [CrossRef]
- Harano, Y.; Kotajima, L.; Arioka, H. Case of cytomegalovirus colitis in an immunocompetent patient: A rare cause of abdominal pain and diarrhea in the elderly. Int. J. Gen. Med. 2015, 8, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Nasa, M.; Patel, N.; Lipi, L.; Sud, R. Gastrointestinal Histoplasmosis and CMV Co-Infection in an Immunocompetent Host. J. Assoc. Physicians India 2017, 65, 94–95. [Google Scholar]
- Yamamoto, S.; Sakai, Y. Acute gastritis caused by concurrent infection with Epstein-Barr virus and cytomegalovirus in an immunocompetent adult. Clin. J. Gastroenterol. 2019, 12, 274–278. [Google Scholar] [CrossRef]
- Seminari, E.; Fronti, E.; Contardi, G.; Broglia, F.; Scevola, D.; Fiorina, L.; Baldanti, F. Colitis in an elderly immunocompetent patient. J. Clin. Virol. 2012, 55, 187–190. [Google Scholar] [CrossRef]
- Bernardes, C.; Quaresma, F.; Capela, T.; Saiote, J. Severe Cytomegalovirus ileitis preceded by acute bacterial enteritis in an immunocompetent patient. Acta Gastroenterol. Belg. 2018, 81, 109–110. [Google Scholar] [PubMed]
- Chan, K.S.; Lee, W.Y.; Yu, W.L. Coexisting cytomegalovirus infection in immunocompetent patients with Clostridium difficile colitis. J. Microbiol. Immunol. Infect. 2016, 49, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, A.A.; Tietze, C.C.; Peterson, K.A.; Go, M.F. Cytomegalovirus clostridium colitis disease in an immunocompetent patient. South. Med. J. 2009, 102, 775–776. [Google Scholar] [CrossRef]
- McCurdy, J.; Enders, F.; Khanna, S.; Bruining, D.; Jones, A.; Killian, J.; Tariq, R.; Smyrk, T.; Loftus, E. Increased Rates of Clostridium difficile Infection and Poor Outcomes in Patients with IBD with Cytomegalovirus. Inflamm. Bowel Dis. 2016, 22, 2688–2693. [Google Scholar] [CrossRef]
- Li, Y.; Xu, H.; Xu, T.; Xiao, M.; Tang, H.; Wu, D.; Tan, B.; Li, J.; Yang, H.; Lv, H.; et al. Case–Control Study of Inflammatory Bowel Disease Patients with and without Clostridium difficile Infection and Poor Outcomes in Patients Coinfected with C. difficile and Cytomegalovirus. Dig. Dis. Sci. 2018, 63, 3074–3083. [Google Scholar] [CrossRef]
- Xu, H.; Tang, H.; Xu, T.; Xiao, M.; Li, J.; Tan, B.; Yang, H.; Lv, H.; Li, Y.; Qian, J. Retrospective analysis of Clostridium difficile infection in patients with ulcerative colitis in a tertiary hospital in China. BMC Gastroenterol. 2019, 19, 3. [Google Scholar] [CrossRef]
- Porta, A.; Avanzini, A.; Bellini, M.; Crossignani, R.M.; Fiocchi, S.; Martinelli, S.; Parola, L. Neonatal gastrointestinal involvement and congenital cytomegalovirus. Pediatr. Med. Chir. 2016, 38, 134. [Google Scholar] [CrossRef]
- Sue, P.K.; Salazar-Austin, N.M.; McDonald, O.G.; Rishi, A.; Cornish, T.C.; Arav-Boger, R. Cytomegalovirus Enterocolitis in Immunocompetent Young Children: A Report of Two Cases and Review of the Literature. Pediatr. Infect. Dis. J. 2016, 35, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Barbati, F.; Marrani, E.; Indolfi, G.; Lionetti, P.; Trapani, S. Menetrier disease and Cytomegalovirus infection in paediatric age: Report of three cases and a review of the literature. Eur. J. Pediatr. 2021, 180, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Affolter, K.; Boynton, K.; Chen, X.; Valentine, J.; Peterson, K. CMV Disease in IBD: Comparison of Diagnostic Tests and Correlation with Disease Outcome. Inflamm. Bowel Dis. 2018, 24, 1539–1546. [Google Scholar] [CrossRef]
- Yerushalmy-Feler, A.; Padlipsky, J.; Cohen, S. Diagnosis and Management of CMV Colitis. Curr. Infect. Dis. Rep. 2019, 21, 5. [Google Scholar] [CrossRef] [PubMed]
- Hazır-Konya, H.; Avkan-Oğuz, V.; Akpınar, H.; Sağol, Ö.; Sayıner, A. Investigation of Cytomegalovirus in Intestinal Tissue in a Country With High CMV Seroprevalence. Turk. J. Gastroenterol. 2021, 32, 123–132. [Google Scholar] [CrossRef]
- Burston, J.; van Hal, S.; Dubedat, S.; Lee, A. Inclusions or bystanders? CMV PCR sensitivity and specificity in tissue samples. J. Clin. Virol. 2017, 90, 38–39. [Google Scholar] [CrossRef]
- Yan, Z.; Wang, L.; Dennis, J.; Doern, C.; Baker, J.; Park, J.Y. Clinical significance of isolated cytomegalovirus-infected gastrointestinal cells. Int. J. Surg. Pathol. 2014, 22, 492–498. [Google Scholar] [CrossRef]
- Mourad, F.H.; Hashash, J.G.; Kariyawasam, V.C.; Leong, R.W. Ulcerative Colitis and Cytomegalovirus Infection: From A to Z. J. Crohn’s Colitis 2020, 14, 1162–1171. [Google Scholar] [CrossRef]
- Mills, A.M.; Guo, F.P.; Copland, A.P.; Pai, R.K.; Pinsky, B.A. A comparison of CMV detection in gastrointestinal mucosal biopsies using immunohistochemistry and PCR performed on formalin-fixed, paraffin-embedded tissue. Am. J. Surg. Pathol. 2013, 37, 995–1000. [Google Scholar] [CrossRef]
- Solomon, I.H.; Hornick, J.L.; Laga, A.C. Immunohistochemistry Is Rarely Justified for the Diagnosis of Viral Infections. Am. J. Clin. Pathol. 2017, 147, 96–104. [Google Scholar] [CrossRef]
- Guo, L.; DeRoche, T.C.; Salih, Z.T.; Qasem, S.A. Routine Hematoxylin and Eosin Stain Is Specific for the Diagnosis of Cytomegalovirus Infection in Gastrointestinal Biopsy Specimens. Int. J. Surg. Pathol. 2018, 26, 500–506. [Google Scholar] [CrossRef]
- Juric-Sekhar, G.; Upton, M.P.; Swanson, P.E.; Westerhoff, M. Cytomegalovirus (CMV) in gastrointestinal mucosal biopsies: Should a pathologist perform CMV immunohistochemistry if the clinician requests it? Hum. Pathol. 2017, 60, 11–15. [Google Scholar] [CrossRef]
- Kawasaki, S.; Osawa, S.; Sugimoto, K.; Uotani, T.; Nishino, M.; Yamada, T.; Sugimoto, M.; Furuta, T.; Ikuma, M. Cecal vanishing tumor associated with cytomegalovirus infection in an immunocompetent elderly adult. World J. Gastrointest. Oncol. 2010, 2, 417–420. [Google Scholar] [CrossRef]
- Agaimy, A.; Mudter, J.; Märkl, B.; Chetty, R. Cytomegalovirus infection presenting as isolated inflammatory polyps of the gastrointestinal tract. Pathology 2011, 43, 440–446. [Google Scholar] [CrossRef]
- Xiong, X.; Liu, F.; Zhao, W.; Ji, X.; Chen, W.; Zou, H.; Li, F. Cytomegalovirus infective gastritis in an immunocompetent host misdiagnosed as malignancy on upper gastrointestinal endoscopy: A case report and review of literature. Hum. Pathol. 2019, 92, 107–112. [Google Scholar] [CrossRef]
- Vegunta, A.S.; Dasar, S.K.; Joshi, S.K.; Rao, R.V. Spontaneous Partial Vanishing Cytomegalovirus Pseudotumour of Colon in an Immunocompetent Patient. J. Clin. Diagn. Res. 2015, 9, Td07–Td09. [Google Scholar] [CrossRef] [PubMed]
- Hakki, M. Moving Past Ganciclovir and Foscarnet: Advances in CMV Therapy. Curr. Hematol. Malig. Rep. 2020, 15, 90–102. [Google Scholar] [CrossRef]
- Vaziri, S.; Pezhman, Z.; Sayyad, B.; Mansouri, F.; Janbakhsh, A.; Afsharian, M.; Najafi, F. Efficacy of valganciclovir and ganciclovir for cytomegalovirus disease in solid organ transplants: A meta-analysis. J. Res. Med. Sci. 2014, 19, 1185–1192. [Google Scholar]
- Upadhyayula, S.; Michaels, M.G. Ganciclovir, Foscarnet, and Cidofovir: Antiviral Drugs Not Just for Cytomegalovirus. J. Pediatr. Infect. Dis. Soc. 2013, 2, 286–290. [Google Scholar] [CrossRef]
- Klauber, E.; Briski, L.E.; Khatib, R. Cytomegalovirus colitis in the immunocompetent host: An overview. Scand. J. Infect. Dis. 1998, 30, 559–564. [Google Scholar] [CrossRef]
- Karigane, D.; Takaya, S.; Seki, Y.; Mastumoto, Y.; Onose, A.; Kosakai, A.; Sugaya, N.; Mori, T. Cytomegalovirus enteritis in immunocompetent subjects: A case report and review of the literature. J. Infect. Chemother. 2014, 20, 325–329. [Google Scholar] [CrossRef]
- Galiatsatos, P.; Shrier, I.; Lamoureux, E.; Szilagyi, A. Meta-analysis of outcome of cytomegalovirus colitis in immunocompetent hosts. Dig. Dis. Sci. 2005, 50, 609–616. [Google Scholar] [CrossRef]
- Naylor, K.; Li, G.; Vallejo, A.N.; Lee, W.W.; Koetz, K.; Bryl, E.; Witkowski, J.; Fulbright, J.; Weyand, C.M.; Goronzy, J.J. The influence of age on T cell generation and TCR diversity. J. Immunol. 2005, 174, 7446–7452. [Google Scholar] [CrossRef]
- Nikolich-Žugich, J.; van Lier, R.A.W. Cytomegalovirus (CMV) research in immune senescence comes of age: Overview of the 6th International Workshop on CMV and Immunosenescence. Geroscience 2017, 39, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Solana, R.; Tarazona, R.; Aiello, A.E.; Akbar, A.N.; Appay, V.; Beswick, M.; Bosch, J.A.; Campos, C.; Cantisán, S.; Cicin-Sain, L.; et al. CMV and Immunosenescence: From basics to clinics. Immun. Ageing 2012, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Hartzell, S.; Bin, S.; Cantarelli, C.; Haverly, M.; Manrique, J.; Angeletti, A.; Manna, G.; Murphy, B.; Zhang, W.; Levitsky, J.; et al. Kidney Failure Associates With T Cell Exhaustion and Imbalanced Follicular Helper T Cells. Front. Immunol. 2020, 11, 583702. [Google Scholar] [CrossRef] [PubMed]
- Betjes, M.G.H. Immune cell dysfunction and inflammation in end-stage renal disease. Nat. Rev. Nephrol. 2013, 9, 255–265. [Google Scholar] [CrossRef]
- Cohen, G. Immune Dysfunction in Uremia 2020. Toxins 2020, 12, 439. [Google Scholar] [CrossRef] [PubMed]
- Janssen, A.W.M.; Stienstra, R.; Jaeger, M.; van Gool, A.J.; Joosten, L.A.B.; Netea, M.G.; Riksen, N.P.; Tack, C.J. Understanding the increased risk of infections in diabetes: Innate and adaptive immune responses in type 1 diabetes. Metabolism 2021, 121, 154795. [Google Scholar] [CrossRef]
- Carey, I.M.; Critchley, J.A.; DeWilde, S.; Harris, T.; Hosking, F.J.; Cook, D.G. Risk of Infection in Type 1 and Type 2 Diabetes Compared With the General Population: A Matched Cohort Study. Diabetes Care 2018, 41, 513–521. [Google Scholar] [CrossRef]
- Lontchi-Yimagou, E.; Feutseu, C.; Kenmoe, S.; Djomkam Zune, A.L.; Kinyuy Ekali, S.F.; Nguewa, J.L.; Choukem, S.P.; Mbanya, J.C.; Gautier, J.F.; Sobngwi, E. Non-autoimmune diabetes mellitus and the risk of virus infections: A systematic review and meta-analysis of case-control and cohort studies. Sci. Rep. 2021, 11, 8968. [Google Scholar] [CrossRef] [PubMed]
- Al-Omari, A.; Aljamaan, F.; Alhazzani, W.; Salih, S.; Arabi, Y. Cytomegalovirus infection in immunocompetent critically ill adults: Literature review. Ann. Intensive Care 2016, 6, 110. [Google Scholar] [CrossRef] [PubMed]
- Sager, K.; Alam, S.; Bond, A.; Chinnappan, L.; Probert, C.S. Review article: Cytomegalovirus and inflammatory bowel disease. Aliment. Pharmacol. Ther. 2015, 41, 725–733. [Google Scholar] [CrossRef]
- Luangsirithanya, P.; Treewaree, S.; Pongpaibul, A.; Pausawasdi, N.; Limsrivilai, J. Cytomegalovirus enterocolitis with subsequent diagnosis of coexisting new-onset inflammatory bowel disease: Two case reports and review of the literature. Medicine 2021, 100, e24914. [Google Scholar] [CrossRef]
- Costa, D.; Fernandes, D.; Furtado, A.; Santa Cruz, A. Cytomegalovirus duodenitis in immunocompetent patients: What else should we look for? BMJ Case Rep. 2017, 2017, bcr2017219679. [Google Scholar] [CrossRef]
- Ng, S.C.; Noursadeghi, M.; von Herbay, A.; Vaizey, C.; Pitcher, M.C.; Flanagan, K.L. Cytomegalovirus ileitis associated with goblet cell carcinoid tumour of the appendix. J. Infect. 2007, 54, e153–e156. [Google Scholar] [CrossRef] [PubMed]
- Murakami, D.; Harada, H.; Yamato, M.; Amano, Y. Cytomegalovirus-associated esophagitis on early esophageal cancer in immunocompetent host: A case report. Gut Pathog. 2021, 13, 24. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (Year) | Disease Location | Age (Years) Sex | Endoscopy | Patho. | CMV Status | AVT | Survi. | Risk Factors | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Old | Ren | DM | MV | Sep | IBD | Can | |||||||||||||||
| ES | ST | SI | CO | MX | U | P | I | Remarks | |||||||||||||
| 1 | Surawicz et al., 1988 [17] | 3 | 25 (M), 37 (F), 71 (F) 1 M, 2 F | 2 | - | 1 | HE ± IHC | Infection in 2 NA in 1 | 0/3 | 3/3 | 1 | ||||||||||
| Anal intercourse in two; sigmoid volvulus with colectomy; and stricture in one. All were self-limited. | |||||||||||||||||||||
| 2 | Page et al., 1998 [18] | 1 | 2 | 2 | 5 | NA NA | - | - | - | Biopsy proven | NA | 5/10 | 2/10 | 4 | |||||||
| Mortality was significantly greater in the normal patient (immunocompetent) group. | |||||||||||||||||||||
| 3 | Ng et al., 1999 [19] | 10 | Median, 70; Range, 59–92; 1 M, 9 F | 6 | 1 | 3 | HE ± IHC | NA | 3/10 | 6/10 | 7 | 2 | 3 | ||||||||
| Preceding events (AMI in two, Shigella enteritis in two). One needed surgery, and three had local complications (fistula). | |||||||||||||||||||||
| 4 | Patra et al., 1999 [20] | 1 | 16 | NA * NA * | 6 | - | 11 | HE | NA | NA | NA | ||||||||||
| All immunocompetent patients were critically ill. Immunocompromised patients had a higher ratio of ulcers (70–35%) and more atypical inclusion bodies (90–47%). | |||||||||||||||||||||
| 5 | Maiorana et al., 2003 [21] | 1 | 4 | 6 | Mean, 72; Range, 52–86; 9 M, 2 F | 9 | - | 2 | HE + IHC | IgG (+): 6/6 IgM (−): 6/6 Viremia: NA | 3/11 | 7/11 | 8 | 2 | 4 | ||||||
| Four immunocompetent patients had malignancies of various organs (diagnosed 2–5 months later). | |||||||||||||||||||||
| 6 | Ng et al., 2003 [22] | 1 | 4 | 1 a | Mean, 74; Range, 60–81; 2 M, 4 F | 4 | - | 2 | HE ± IHC | NA | 3/6 | 4/6 | 5 | 2 | 3 | 1 | |||||
| Total: 14 non-HIV patients, of whom only six qualified for immunocompetent status. | |||||||||||||||||||||
| 7 | Bonetti et al., 2011 [23] | 4 | 11 | Mean, 71; Range, 37–91; 7 M, 8 F | 9 | 2 | 4 | HE + IHC | IgG (+): 3/NA IgM (+): 7/NA Viremia: NA | NA | 15/15 | 1 | |||||||||
| Four immunocompetent patients had malignancies of various organs (diagnosed 5–16 months later). Immunocompromised patients are more likely to have multiple segments or multiple sites of involvement. There were no differences in the frequency or localization of gastric mucosal thickenings between the two groups. | |||||||||||||||||||||
| 8 | Siciliano et al., 2014 [24] | 2 | 12 | Mean, 64; Range, 38–82; 6 M, 8 F | - | - | - | HE + IHC | NA | 13/14 | 4/14 | 8 | 7 | 5 | 10 | 13 | |||||
| All patients developed septic or cardiogenic shock (on average, two episodes) before CMV disease. The mean in-hospital stay was 44 days, with an average of 29 days in the ICU. The in-hospital mortality rate was 71.4%. Cardiomyopathy was noted in 64.2% of patients. | |||||||||||||||||||||
| 9 | Chen et al., 2014 [25] | 1 | 2 | 10 | Mean, 68; Range, 47–77; 7 M, 6 F | 8 | 2 | 3 | HE ± IHC | IgM (+): 1 Antigenemia: 1 | 12/13 | 9/13 | 9 | 13 | 7 | ||||||
| All cases had CKD; one had HSP. AVT: average of 23 ± 14 days (range, 7–42 days). Two patients died of CMV-related colonic perforation. | |||||||||||||||||||||
| 10 | Chan et al., 2014 [26] | 4 | Mean, 74; Range, 65–84; 3 M, 1 F | 2 | 1 | 1 | HE ± IHC | Viremia: 4 | 4/4 | 1/4 | 4 | 2 | 2 | ||||||||
| There was biopsy-proven CMV colitis in eight patients, and only four were identified as having immune status risks. Three (75%) were diagnosed via a clinician-ordered CMV stain. Stool and blood CMV-PCR were applied to diagnose “probable” cases, and stool PCR was positive in 7 of 10 tested patients. | |||||||||||||||||||||
| 11 | Ko et al., 2015 [27] | 51 | Mean ± SD, 65 ± 14; 24 M, 27 F | 49 | 2 | - | HE + IHC or PCR | IgG (+): 100% IgM (+): 8.3% | 39/51 | 47/51 | NA b | 16 | 15 | 11 c | |||||||
| The 30-day mortality rate was 7.8% (all-cause, none related to CMV colitis directly). Risk factors for developing CMV colitis include steroid usage and RBC transfusions within one month. | |||||||||||||||||||||
| 12 | Bernard et al., 2015 [28] | 5 | 1 | 7 | Mean, 75; Range, 54–88; 5 M, 8 F | 10 | - | 3 | PCR | Reactivation: 10 Viremia: 1 (out of 4) | 6/13 | 13/13 | 11 | 2 | 3 | 2 | 2 | ||||
| Only one case had a positive histology finding. The mean value of CMV DNA load in GI biopsies was 3845 copies/μg total DNA. Clinical features were similar to patients diagnosed with histology methods in prior studies. | |||||||||||||||||||||
| 13 | Marques et al., 2017 [29] | 1 | 2 | 51 (M), 86 (F), 87 (F) 1 M, 2 F | 2 | - | 1 | HE ± IHC | NA | 2/3 | 2/3 | 2 | 1 | ||||||||
| In this upper GI tract cohort, 25% were immunocompetent. One had a history of ischemic stroke, and one had decompensated alcoholic liver cirrhosis and DM. | |||||||||||||||||||||
| 14 | Chaemsupaphan et al., 2020 [30] | 4 | 10 | 15 | 47 | Mean ± SD 73 ± 13.9 31 M, 25 F | 47 | 6 | - d | HE ± IHC | Viremia: 16 (out of 27) | 39/51 | 36/56 | NA b | 35 | 20 | 20 | NA e | |||
| AVT is an independent protective factor *. Predictors of six-month mortality: age, inpatient status, ICU *. Patients in the immunocompetent group were older, had more ICU needs at diagnosis, had more viremia-negative cases, were less treated, and had higher six-month mortality (39% vs. 22%). | |||||||||||||||||||||
| 15 | Wetwittayakhlang et al., 2021 [13] | 5 | 4 | 17 | 59 | 4 | Median, 70; IQR, 63–79; 51 M, 38 F | 58 | 3 | 28 | HE ± IHC | NA | 80/89 | 64/89 | 59 | 56 | 12 | 34 | 30 | 4 | |
| AVT > 14 days was a protective factor for survival (Peto-Peto test, p < 0.001) *. The immunocompetent group was older, had more GI bleeding, shorter symptom-onset duration, and had more involvement in SI and less in ES/MX. There was no difference in in-hospital mortality regarding immunity. | |||||||||||||||||||||
| 16 | Yoon et al., 2021 [31] | 60 | 26 f | Median, 68; IQR, 60–74; 53 M, 33 F | 55 | - | 31 | HE ± IHC ± PCR | Viremia: 25 (out of 46) | 51/86 | 78/86 | NA b | 15 | 34 | 34 | 36 | |||||
| Sixty-eight cases (79.1%) had comorbidities. Endoscopic features were not associated with clinical outcomes. CRP is an independent risk factor for surgery and in-hospital mortality. | |||||||||||||||||||||
| 17 | Verma et al., 2021 [32] | 4 | 45 (M), 52 (M), 55 (F), 65 (F) 2 M, 2 F | 4 | - | - | HE + IHC ± PCR | NA | 3/4 | 3/4 | 1 | 2 | |||||||||
| One case had a history of coronavirus disease 2019. One was positive for tissue CMV PCR. One patient died of a myocardial infarction before receiving AVT. | |||||||||||||||||||||
| 18 | Yeh et al., 2022 [12] | 12 | 32 | 9 | 127 | Mean ± SD, 65.3 ± 17.6; 105 M, 75 F | 148 | 22 | 10 | HE + IHC | IgG (+): 97.2% IgM (+): 16.9% Antigenemia: 42.9% Viremia: 65.9% | 99/180 | 152/180 | 108 | 79 | 75 | 42 | 28 | 20 | ||
| Immunocompetent patients receiving Combo therapy had the best survival curve. Combo AVT (oral plus intravenous) ≥ 14 days resulted in better outcomes for both immunocompromised and immunocompetent patients. | |||||||||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, P.-J.; Wu, R.-C.; Chen, C.-L.; Chiu, C.-T.; Lai, M.-W.; Chen, C.-C.; Chiu, C.-H.; Pan, Y.-B.; Lin, W.-R.; Le, P.-H. Cytomegalovirus Diseases of the Gastrointestinal Tract in Immunocompetent Patients: A Narrative Review. Viruses 2024, 16, 346. https://doi.org/10.3390/v16030346
Yeh P-J, Wu R-C, Chen C-L, Chiu C-T, Lai M-W, Chen C-C, Chiu C-H, Pan Y-B, Lin W-R, Le P-H. Cytomegalovirus Diseases of the Gastrointestinal Tract in Immunocompetent Patients: A Narrative Review. Viruses. 2024; 16(3):346. https://doi.org/10.3390/v16030346
Chicago/Turabian StyleYeh, Pai-Jui, Ren-Chin Wu, Chyi-Liang Chen, Cheng-Tang Chiu, Ming-Wei Lai, Chien-Chang Chen, Cheng-Hsun Chiu, Yu-Bin Pan, Wey-Ran Lin, and Puo-Hsien Le. 2024. "Cytomegalovirus Diseases of the Gastrointestinal Tract in Immunocompetent Patients: A Narrative Review" Viruses 16, no. 3: 346. https://doi.org/10.3390/v16030346