
Molecular and Clinical Epidemiology of SARS-CoV-2 Infection among Vaccinated and Unvaccinated Individuals in a Large Healthcare Organization from New Jersey
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
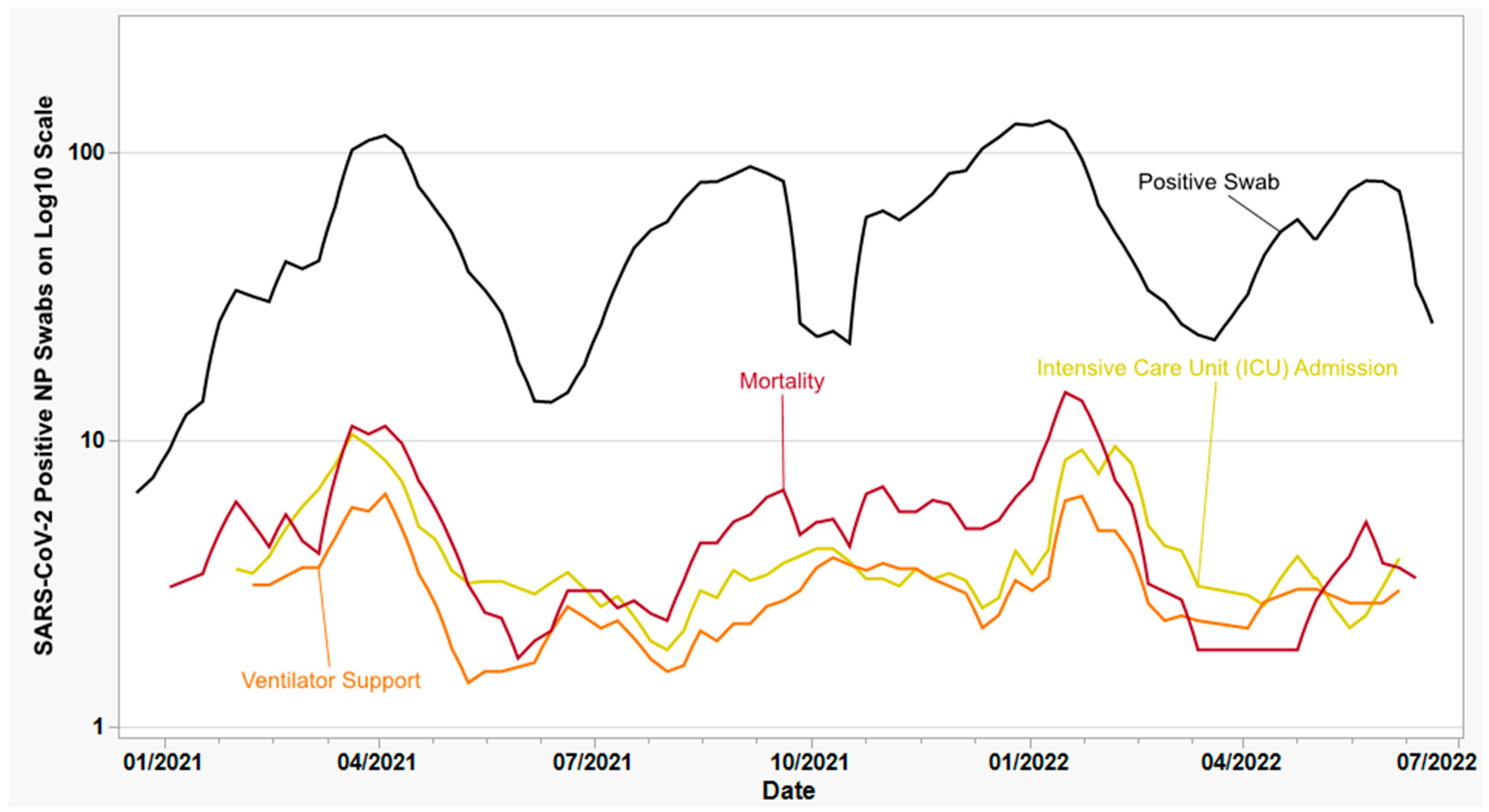
3.1. SARS-CoV-2 Sample Collection and Selection
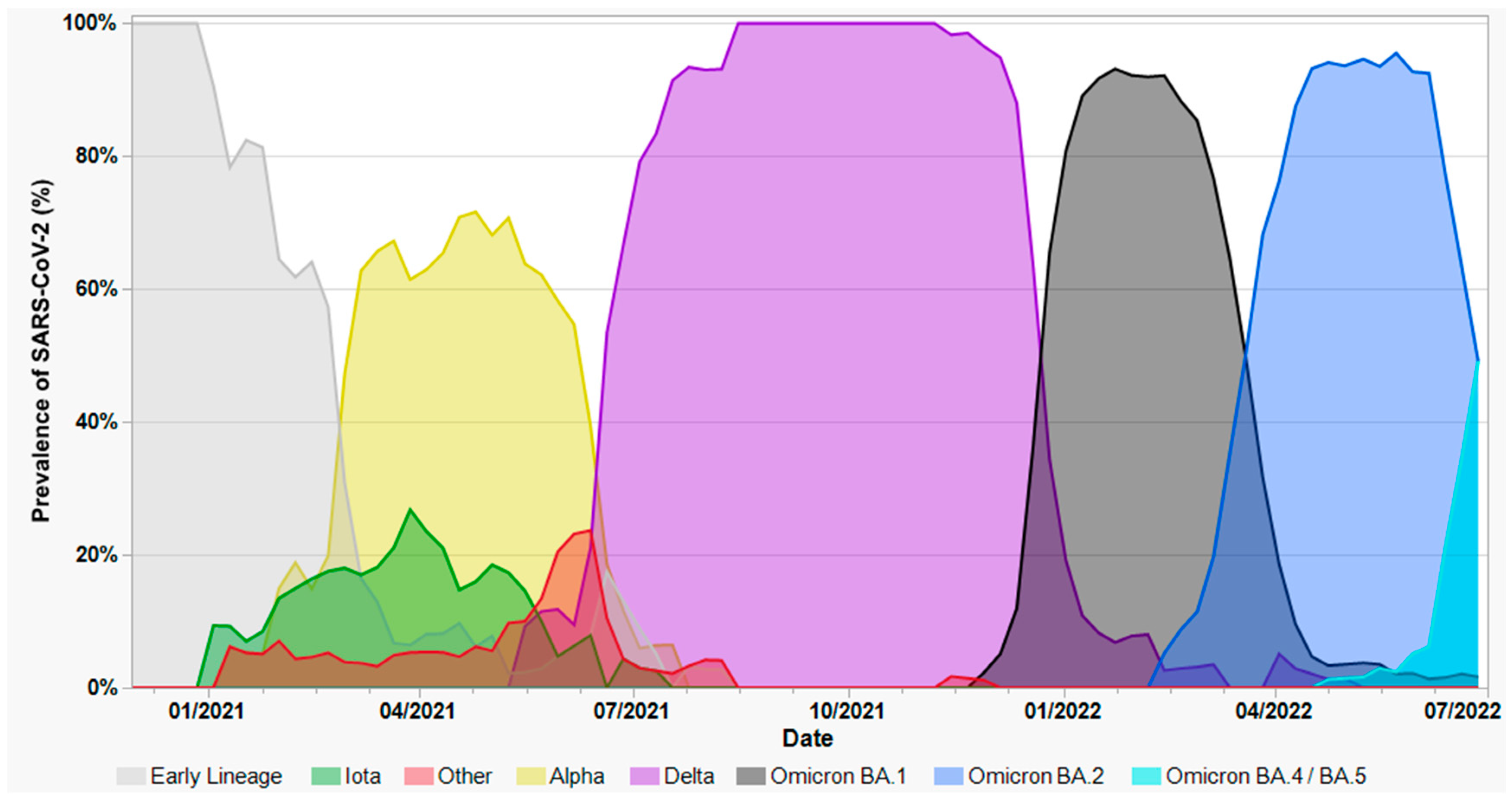
3.2. Variant Screening of SARS-CoV-2-Positive Nasopharyngeal Swabs
3.3. Whole Genome Sequencing of SARS-CoV-2-Positive Nasopharyngeal Swabs
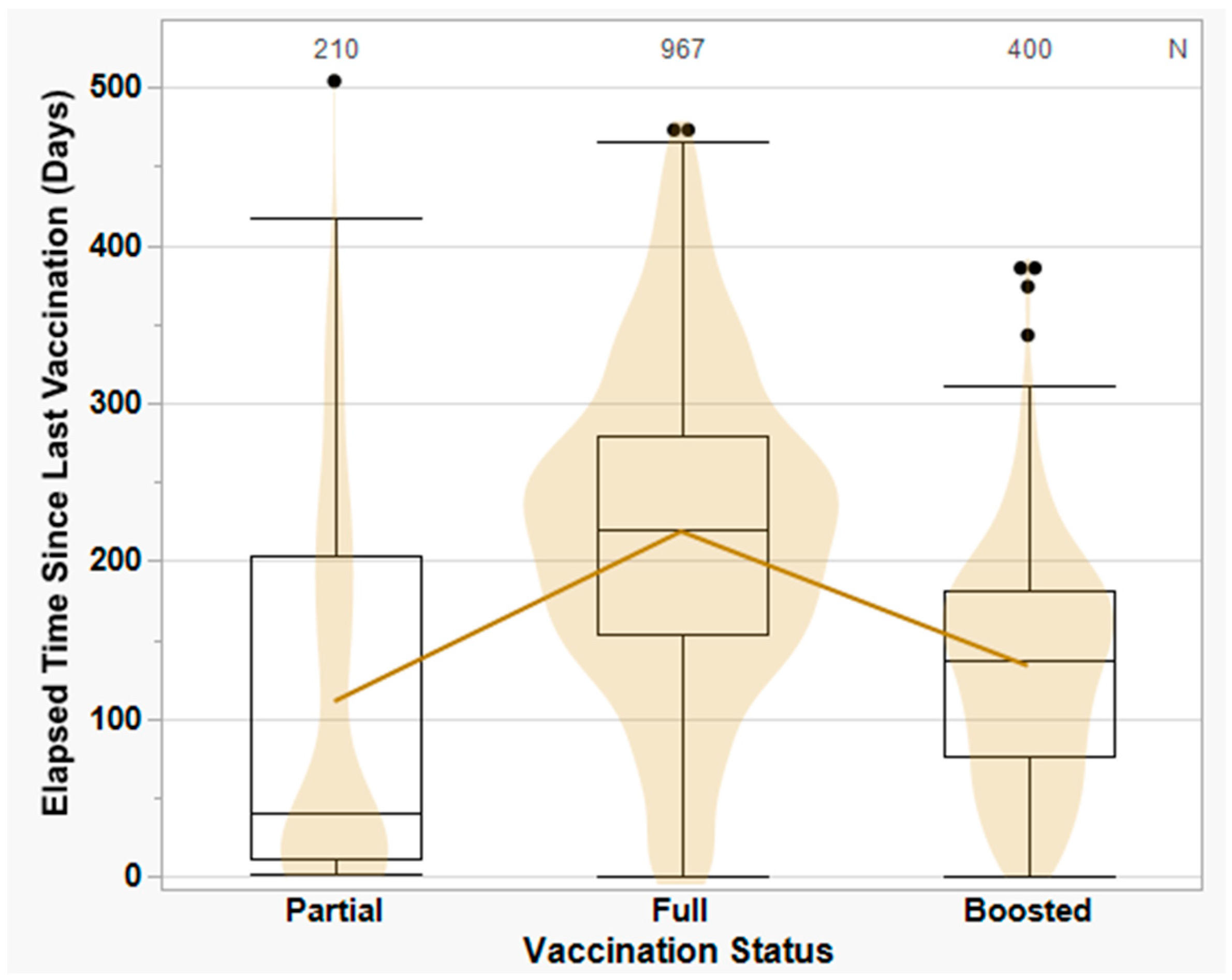
3.4. COVID-19 Vaccination Status and Vaccine-Breakthrough Infections
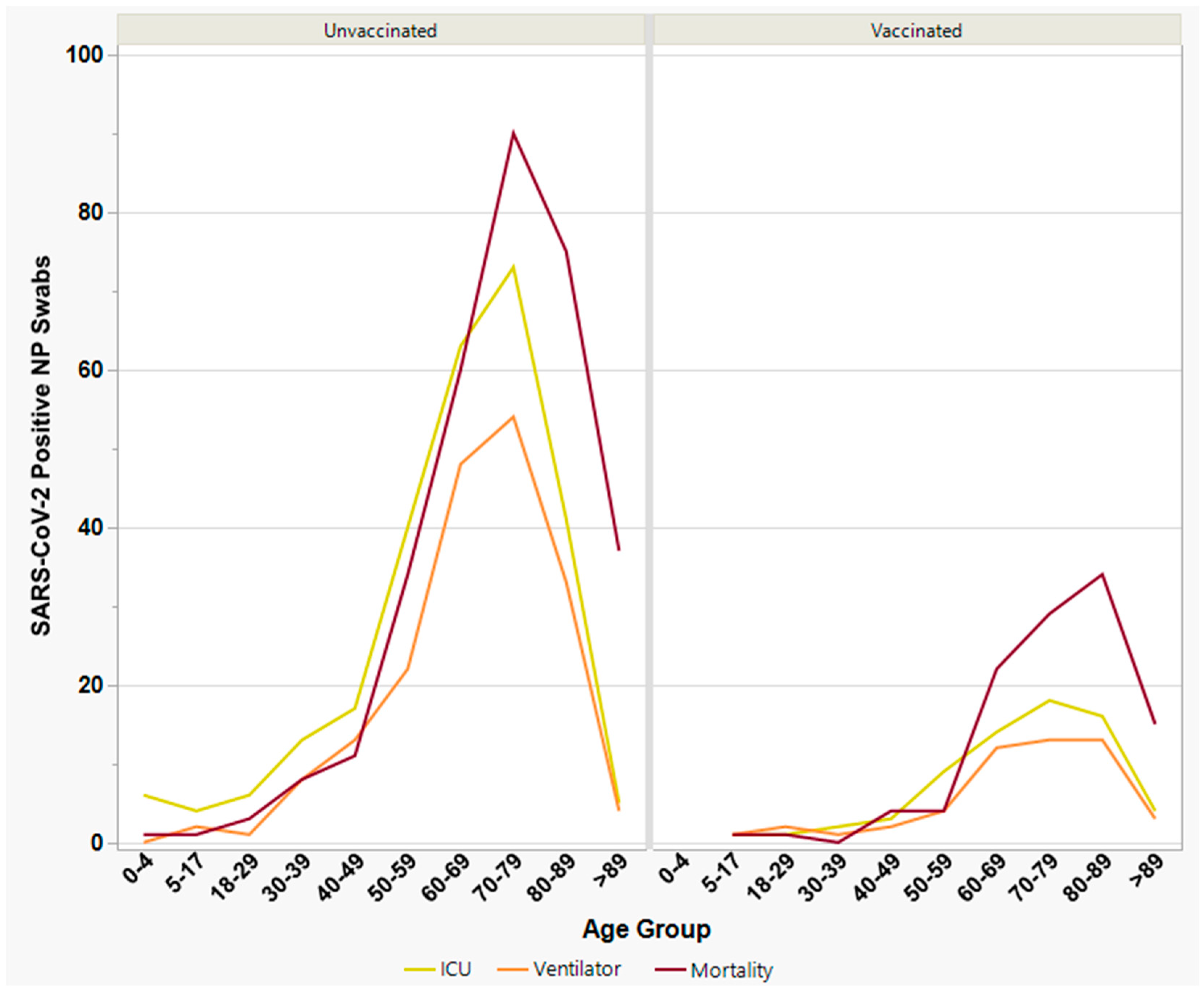
3.5. Severe Clinical Outcomes among Vaccinated vs. Unvaccinated Individuals
3.5.1. Intensive Care Unit (ICU) Admission Individuals
3.5.2. Ventilator Support
3.5.3. Mortality
3.6. Risk Factors and Comorbidities among Vaccinated vs. Unvaccinated Individuals
3.7. Analysis of SARS-CoV-2 Variants and Severe Clinical
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Joseph, S.; Narayanan, A.K. COVID 19-the 21st Century Pandemic: The Novel Coronavirus Outbreak and the Treatment Strategies. Adv. Pharm. Bull. 2022, 12, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.; Agnihotri, K.; Tripathi, A.; Mukherjee, S.; Agnihotri, N.; Gupta, G. COVID-19: A Worldwide, Zoonotic, Pandemic Outbreak. Altern. Ther. Health Med. 2020, 26, 56–64. [Google Scholar] [PubMed]
- COVID-19 Mortality by State. Available online: https://www.cdc.gov/nchs/pressroom/sosmap/covid19_mortality_final/COVID19.htm (accessed on 30 June 2022).
- New Jersey COVID-19 Information Hub. Available online: https://covid19.nj.gov/ (accessed on 30 June 2022).
- About Hackensack Meridian Health. Available online: https://www.hackensackmeridianhealth.org/en/about-us (accessed on 30 June 2022).
- Erminio, V. Coronavirus in New Jersey: A Timeline of the Outbreak. Available online: https://www.nj.com/coronavirus/2020/03/coronavirus-in-new-jersey-a-timeline-of-the-outbreak.html (accessed on 30 June 2022).
- Center for Discovery & Innovation. Available online: https://hmh-cdi.org/ (accessed on 30 June 2022).
- Zhao, Y.; Cunningham, M.H.; Mediavilla, J.R.; Park, S.; Fitzgerald, S.; Ahn, H.S.; Li, X.; Zhan, C.; Hong, T.; Munk, G.; et al. Diagnosis, clinical characteristics, and outcomes of COVID-19 patients from a large healthcare system in northern New Jersey. Sci. Rep. 2021, 11, 4389. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Lee, A.; Composto, K.; Cunningham, M.H.; Mediavilla, J.R.; Fennessey, S.; Corvelo, A.; Chow, K.F.; Zody, M.; Chen, L.; et al. A novel diagnostic test to screen SARS-CoV-2 variants containing E484K and N501Y mutations. Emerg. Microbes Infect. 2021, 10, 994–997. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K.; et al. Immunogenicity of the Ad26.COV2.S Vaccine for COVID-19. JAMA 2021, 325, 1535–1544. [Google Scholar] [CrossRef]
- Mathema, B.; Chen, L.; Chow, K.F.; Zhao, Y.; Zody, M.C.; Mediavilla, J.R.; Cunningham, M.H.; Composto, K.; Lee, A.; Oschwald, D.M.; et al. Postvaccination SARS-CoV-2 among Health Care Workers in New Jersey: A Genomic Epidemiological Study. Microbiol. Spectr. 2021, 9, e0188221. [Google Scholar] [CrossRef]
- González-Candelas, F.; Shaw, M.A.; Phan, T.; Kulkarni-Kale, U.; Paraskevis, D.; Luciani, F.; Kimura, H.; Sironi, M. One year into the pandemic: Short-term evolution of SARS-CoV-2 and emergence of new lineages. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2021, 92, 104869. [Google Scholar] [CrossRef]
- Li, J.; Lai, S.; Gao, G.F.; Shi, W. The emergence, genomic diversity and global spread of SARS-CoV-2. Nature 2021, 600, 408–418. [Google Scholar] [CrossRef]
- Tosta, S.; Moreno, K.; Schuab, G.; Fonseca, V.; Segovia, F.M.C.; Kashima, S.; Elias, M.C.; Sampaio, S.C.; Ciccozzi, M.; Alcantara, L.C.J.; et al. Global SARS-CoV-2 genomic surveillance: What we have learned (so far). Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2023, 108, 105405. [Google Scholar] [CrossRef]
- Boehm, E.; Kronig, I.; Neher, R.A.; Eckerle, I.; Vetter, P.; Kaiser, L. Novel SARS-CoV-2 variants: The pandemics within the pandemic. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2021, 27, 1109–1117. [Google Scholar] [CrossRef]
- Gupta, D.; Sharma, P.; Singh, M.; Kumar, M.; Ethayathulla, A.S.; Kaur, P. Structural and functional insights into the spike protein mutations of emerging SARS-CoV-2 variants. Cell. Mol. Life Sci. CMLS 2021, 78, 7967–7989. [Google Scholar] [CrossRef] [PubMed]
- Lazarevic, I.; Pravica, V.; Miljanovic, D.; Cupic, M. Immune Evasion of SARS-CoV-2 Emerging Variants: What Have We Learnt So Far? Viruses 2021, 13, 1192. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Bhola, S.; Thakur, P.; Patel, S.K.S.; Kulshrestha, S.; Ratho, R.K.; Kumar, P. Waves and variants of SARS-CoV-2: Understanding the causes and effect of the COVID-19 catastrophe. Infection 2022, 50, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Haider, N.; Abbasi, A.F.; Jaferi, U.; Prakash, S.; Balendra, V. The emerging SARS-CoV-2 variants of concern. Ther. Adv. Infect. Dis. 2021, 8, 20499361211024372. [Google Scholar] [CrossRef] [PubMed]
- Tao, K.; Tzou, P.L.; Nouhin, J.; Gupta, R.K.; de Oliveira, T.; Kosakovsky Pond, S.L.; Fera, D.; Shafer, R.W. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat. Rev. Genet. 2021, 22, 757–773. [Google Scholar] [CrossRef]
- Thye, A.Y.; Law, J.W.; Pusparajah, P.; Letchumanan, V.; Chan, K.G.; Lee, L.H. Emerging SARS-CoV-2 Variants of Concern (VOCs): An Impending Global Crisis. Biomedicines 2021, 9, 1303. [Google Scholar] [CrossRef]
- Kannan, S.; Shaik Syed Ali, P.; Sheeza, A. Omicron (B.1.1.529)—Variant of concern—Molecular profile and epidemiology: A mini review. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 8019–8022. [Google Scholar]
- Saxena, S.K.; Kumar, S.; Ansari, S.; Paweska, J.T.; Maurya, V.K.; Tripathi, A.K.; Abdel-Moneim, A.S. Characterization of the novel SARS-CoV-2 Omicron (B.1.1.529) variant of concern and its global perspective. J. Med. Virol. 2022, 94, 1738–1744. [Google Scholar] [CrossRef]
- Esper, F.P.; Adhikari, T.M.; Tu, Z.J.; Cheng, Y.W.; El-Haddad, K.; Farkas, D.H.; Bosler, D.; Rhoads, D.; Procop, G.W.; Ko, J.S.; et al. Alpha to Omicron: Disease Severity and Clinical Outcomes of Major SARS-CoV-2 Variants. J. Infect. Dis. 2023, 227, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Faust, J.S.; Du, C.; Liang, C.; Mayes, K.D.; Renton, B.; Panthagani, K.; Krumholz, H.M. Excess Mortality in Massachusetts During the Delta and Omicron Waves of COVID-19. JAMA 2022, 328, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Loucera, C.; Perez-Florido, J.; Casimiro-Soriguer, C.S.; Ortuño, F.M.; Carmona, R.; Bostelmann, G.; Martínez-González, L.J.; Muñoyerro-Muñiz, D.; Villegas, R.; Rodriguez-Baño, J.; et al. Assessing the Impact of SARS-CoV-2 Lineages and Mutations on Patient Survival. Viruses 2022, 14, 1893. [Google Scholar] [CrossRef]
- Wrenn, J.O.; Pakala, S.B.; Vestal, G.; Shilts, M.H.; Brown, H.M.; Bowen, S.M.; Strickland, B.A.; Williams, T.; Mallal, S.A.; Jones, I.D.; et al. COVID-19 severity from Omicron and Delta SARS-CoV-2 variants. Influenza Other Respir. Viruses 2022, 16, 832–836. [Google Scholar] [CrossRef]
- DeCuir, J.; Surie, D.; Zhu, Y.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; McNeal, T.; et al. Effectiveness of Monovalent mRNA COVID-19 Vaccination in Preventing COVID-19-Associated Invasive Mechanical Ventilation and Death Among Immunocompetent Adults During the Omicron Variant Period—IVY Network, 19 U.S. States, February 1, 2022–January 31, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Berry, D.A.; Ip, A.; Lewis, B.E.; Berry, S.M.; Berry, N.S.; MrKulic, M.; Gadalla, V.; Sat, B.; Wright, K.; Serna, M.; et al. Development and validation of a prognostic 40-day mortality risk model among hospitalized patients with COVID-19. PLoS ONE 2021, 16, e0255228. [Google Scholar] [CrossRef]
- Fiore, M.C.; Smith, S.S.; Adsit, R.T.; Bolt, D.M.; Conner, K.L.; Bernstein, S.L.; Eng, O.D.; Lazuk, D.; Gonzalez, A.; Jorenby, D.E.; et al. The first 20 months of the COVID-19 pandemic: Mortality, intubation and ICU rates among 104,590 patients hospitalized at 21 United States health systems. PLoS ONE 2022, 17, e0274571. [Google Scholar] [CrossRef]
- Gupta, S.; Hayek, S.S.; Wang, W.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Factors Associated With Death in Critically Ill Patients With Coronavirus Disease 2019 in the US. JAMA Intern. Med. 2020, 180, 1436–1447. [Google Scholar] [CrossRef]
- Lipsitch, M.; Krammer, F.; Regev-Yochay, G.; Lustig, Y.; Balicer, R.D. SARS-CoV-2 breakthrough infections in vaccinated individuals: Measurement, causes and impact. Nat. Rev. Immunol. 2022, 22, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Vet, J.A.; Van der Rijt, B.J.; Blom, H.J. Molecular beacons: Colorful analysis of nucleic acids. Expert Rev. Mol. Diagn. 2002, 2, 77–86. [Google Scholar] [CrossRef]
- Mathema, B.; Chen, L.; Wang, P.; Cunningham, M.H.; Mediavilla, J.R.; Chow, K.F.; Luo, Y.; Zhao, Y.; Composto, K.; Zuckerman, J.; et al. Genomic Epidemiology and Serology Associated with a SARS-CoV-2 R.1 Variant Outbreak in New Jersey. mBio 2022, 13, e0214122. [Google Scholar] [CrossRef] [PubMed]
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, R.A. Nextstrain: Real-time tracking of pathogen evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Toole, Á.; Scher, E.; Underwood, A.; Jackson, B.; Hill, V.; McCrone, J.T.; Colquhoun, R.; Ruis, C.; Abu-Dahab, K.; Taylor, B.; et al. Assignment of epidemiological lineages in an emerging pandemic using the pangolin tool. Virus Evol. 2021, 7, veab064. [Google Scholar] [CrossRef] [PubMed]
- Shu, Y.; McCauley, J. GISAID: Global initiative on sharing all influenza data—From vision to reality. Euro Surveill 2017, 22, 30494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Data Definitions for COVID-19 Vaccinations in the United States. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/reporting-vaccinations.html (accessed on 30 June 2022).
- Washington, N.L.; White, S.; Schiabor-Barrett, K.M.; Cirulli, E.T.; Bolze, A.; Lu, J.T. S gene dropout patterns in SARS-CoV-2 tests suggest spread of the H69del/V70del mutation in the US. MedRxiv 2020. [Google Scholar] [CrossRef]
- Metzger, C.; Lienhard, R.; Seth-Smith, H.M.B.; Roloff, T.; Wegner, F.; Sieber, J.; Bel, M.; Greub, G.; Egli, A. PCR performance in the SARS-CoV-2 Omicron variant of concern? Swiss Med. Wkly. 2021, 151, w30120. [Google Scholar] [CrossRef]
- Robishaw, J.D.; Alter, S.M.; Solano, J.J.; Shih, R.D.; DeMets, D.L.; Maki, D.G.; Hennekens, C.H. Genomic surveillance to combat COVID-19: Challenges and opportunities. Lancet Microbe 2021, 2, e481–e484. [Google Scholar] [CrossRef]
- van Dorp, L.; Houldcroft, C.J.; Richard, D.; Balloux, F. COVID-19, the first pandemic in the post-genomic era. Curr. Opin. Virol. 2021, 50, 40–48. [Google Scholar] [CrossRef]
- Steele, M.K.; Couture, A.; Reed, C.; Iuliano, D.; Whitaker, M.; Fast, H.; Hall, A.J.; MacNeil, A.; Cadwell, B.; Marks, K.J.; et al. Estimated Number of COVID-19 Infections, Hospitalizations, and Deaths Prevented Among Vaccinated Persons in the US, December 2020 to September 2021. JAMA Netw. Open 2022, 5, e2220385. [Google Scholar] [CrossRef]
- Tatsi, E.B.; Filippatos, F.; Michos, A. SARS-CoV-2 variants and effectiveness of vaccines: A review of current evidence. Epidemiol. Infect. 2021, 149, e237. [Google Scholar] [CrossRef]
- Yaqinuddin, A.; Shafqat, A.; Kashir, J.; Alkattan, K. Effect of SARS-CoV-2 Mutations on the Efficacy of Antibody Therapy and Response to Vaccines. Vaccines 2021, 9, 914. [Google Scholar] [CrossRef]
- Adams, K.; Rhoads, J.P.; Surie, D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Huynh, D.; Talbot, H.K.; Casey, J.D.; et al. Vaccine Effectiveness of Primary Series and Booster Doses against Omicron Variant COVID-19-Associated Hospitalization in the United States. MedRxiv 2022. [Google Scholar] [CrossRef]
- DeSilva, M.B.; Mitchell, P.K.; Klein, N.P.; Dixon, B.E.; Tenforde, M.W.; Thompson, M.G.; Naleway, A.L.; Grannis, S.J.; Ong, T.C.; Natarajan, K.; et al. Protection of Two and Three mRNA Vaccine Doses Against Severe Outcomes Among Adults Hospitalized With COVID-19-VISION Network, August 2021 to March 2022. J. Infect. Dis. 2023, 227, 961–969. [Google Scholar] [CrossRef]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 255–263. [Google Scholar]
- Flacco, M.E.; Acuti Martellucci, C.; Baccolini, V.; De Vito, C.; Renzi, E.; Villari, P.; Manzoli, L. COVID-19 vaccines reduce the risk of SARS-CoV-2 reinfection and hospitalization: Meta-analysis. Front. Med. 2022, 9, 1023507. [Google Scholar] [CrossRef] [PubMed]
- Havers, F.P.; Pham, H.; Taylor, C.A.; Whitaker, M.; Patel, K.; Anglin, O.; Kambhampati, A.K.; Milucky, J.; Zell, E.; Moline, H.L.; et al. COVID-19-Associated Hospitalizations Among Vaccinated and Unvaccinated Adults 18 Years or Older in 13 US States, January 2021 to April 2022. JAMA Intern. Med. 2022, 182, 1071–1081. [Google Scholar] [CrossRef]
- Surie, D.; Bonnell, L.; Adams, K.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; et al. Effectiveness of Monovalent mRNA Vaccines Against COVID-19-Associated Hospitalization Among Immunocompetent Adults During BA.1/BA.2 and BA.4/BA.5 Predominant Periods of SARS-CoV-2 Omicron Variant in the United States—IVY Network, 18 States, December 26, 2021–August 31, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1327–1334. [Google Scholar] [PubMed]
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowley, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 139–145. [Google Scholar] [PubMed]
- Worldometers.info United States COVID—Coronavirus Statistics. Available online: https://www.worldometers.info/coronavirus/country/us/ (accessed on 30 June 2022).
- New Jersey COVID-19 Dashboard. Available online: https://www.nj.gov/health/cd/topics/covid2019_dashboard.shtml (accessed on 30 June 2022).
- Sullivan, S.P. 1 in 500 New Jerseyans have died from COVID-19 since pandemic began, data shows. Available online: https://www.nj.com/coronavirus/2020/12/1-in-500-new-jerseyans-have-died-from-covid-19-since-pandemic-began-data-shows.html (accessed on 30 June 2022).
- Barrett, E.S.; Horton, D.B.; Roy, J.; Gennaro, M.L.; Brooks, A.; Tischfield, J.; Greenberg, P.; Andrews, T.; Jagpal, S.; Reilly, N.; et al. Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers in New Jersey, at the onset of the U.S. COVID-19 pandemic. BMC Infect. Dis. 2020, 20, 853. [Google Scholar] [CrossRef]
- Bhavsar, S.M.; Clouser, K.N.; Gadhavi, J.; Anene, O.; Kaur, R.; Lewis, R.; Naganathan, S.; Michalak, Z.; Chen, C.Q.; Shah, P.; et al. COVID-19 in Pediatrics: Characteristics of Hospitalized Children in New Jersey. Hosp. Pediatr. 2021, 11, 79–87. [Google Scholar] [CrossRef]
- Donato, M.L.; Park, S.; Baker, M.; Korngold, R.; Morawski, A.; Geng, X.; Tan, M.; Ip, A.; Goldberg, S.; Rowley, S.; et al. Clinical and laboratory evaluation of patients with SARS-CoV-2 pneumonia treated with high-titer convalescent plasma. JCI Insight 2021, 6, e143196. [Google Scholar] [CrossRef] [PubMed]
- Samuel, A.; Mechineni, A.; Aronow, W.S.; Ismail, M.; Manickam, R. A review of the characteristics and outcomes of 900 COVID-19 patients hospitalized at a Tertiary Care Medical Center in New Jersey, USA. Arch. Med. Sci. Atheroscler. Dis. 2020, 5, e306–e312. [Google Scholar] [CrossRef]
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/region/us/new-jersey (accessed on 30 June 2022).
- Focosi, D.; Quiroga, R.; McConnell, S.; Johnson, M.C.; Casadevall, A. Convergent Evolution in SARS-CoV-2 Spike Creates a Variant Soup from Which New COVID-19 Waves Emerge. Int. J. Mol. Sci. 2023, 24, 2264. [Google Scholar] [CrossRef]
- Chrysostomou, A.C.; Aristokleous, A.; Rodosthenous, J.H.; Christodoulou, C.; Stathi, G.; Kostrikis, L.G. Detection of Circulating SARS-CoV-2 Variants of Concern (VOCs) Using a Multiallelic Spectral Genotyping Assay. Life 2023, 13, 304. [Google Scholar] [CrossRef]
- Jiang, W.; Ji, W.; Zhang, Y.; Xie, Y.; Chen, S.; Jin, Y.; Duan, G. An Update on Detection Technologies for SARS-CoV-2 Variants of Concern. Viruses 2022, 14, 2324. [Google Scholar] [CrossRef]
- Yan, T.; Xu, Y.; Zheng, R.; Zeng, X.; Chen, Z.; Lin, S.; Xia, Z.; Liao, Y.; Zhang, Y.; Li, Q. Accessible and Adaptable Multiplexed Real-Time PCR Approaches to Identify SARS-CoV-2 Variants of Concern. Microbiol. Spectr. 2022, 10, e0322222. [Google Scholar] [CrossRef] [PubMed]
- Cox, M.; Peacock, T.P.; Harvey, W.T.; Hughes, J.; Wright, D.W.; Willett, B.J.; Thomson, E.; Gupta, R.K.; Peacock, S.J.; Robertson, D.L.; et al. SARS-CoV-2 variant evasion of monoclonal antibodies based on in vitro studies. Nat. Rev. Microbiol. 2023, 21, 112–124. [Google Scholar] [CrossRef]
- Murano, K.; Guo, Y.; Siomi, H. The emergence of SARS-CoV-2 variants threatens to decrease the efficacy of neutralizing antibodies and vaccines. Biochem. Soc. Trans. 2021, 49, 2879–2890. [Google Scholar] [CrossRef] [PubMed]
- Sabbatucci, M.; Vitiello, A.; Clemente, S.; Zovi, A.; Boccellino, M.; Ferrara, F.; Cimmino, C.; Langella, R.; Ponzo, A.; Stefanelli, P.; et al. Omicron variant evolution on vaccines and monoclonal antibodies. Inflammopharmacology 2023, 31, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Wahid, M.; Jawed, A.; Mandal, R.K.; Dailah, H.G.; Janahi, E.M.; Dhama, K.; Somvanshi, P.; Haque, S. Variants of SARS-CoV-2, their effects on infection, transmission and neutralization by vaccine-induced antibodies. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5857–5864. [Google Scholar]
- Banada, P.; Green, R.; Banik, S.; Chopoorian, A.; Streck, D.; Jones, R.; Chakravorty, S.; Alland, D. A Simple Reverse Transcriptase PCR Melting-Temperature Assay To Rapidly Screen for Widely Circulating SARS-CoV-2 Variants. J. Clin. Microbiol. 2021, 59, e0084521. [Google Scholar] [CrossRef]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Hsieh, S.S.; Hung, K.S.; Tang, S.H.; Perng, C.L.; et al. Emergency SARS-CoV-2 Variants of Concern: Novel Multiplex Real-Time RT-PCR Assay for Rapid Detection and Surveillance. Microbiol. Spectr. 2022, 10, e0251321. [Google Scholar] [CrossRef]
- Dikdan, R.J.; Marras, S.A.E.; Field, A.P.; Brownlee, A.; Cironi, A.; Hill, D.A.; Tyagi, S. Multiplex PCR Assays for Identifying all Major Severe Acute Respiratory Syndrome Coronavirus 2 Variants. J. Mol. Diagn. JMD 2022, 24, 309–319. [Google Scholar] [CrossRef]
- Moisan, A.; Soares, A.; De Oliveira, F.; Alessandri-Gradt, E.; Lecoquierre, F.; Fourneaux, S.; Plantier, J.C.; Gueudin, M. Evaluation of Analytical and Clinical Performance and Usefulness in a Real-Life Hospital Setting of Two in-House Real-Time RT-PCR Assays to Track SARS-CoV-2 Variants of Concern. Viruses 2023, 15, 1115. [Google Scholar] [CrossRef]
- Bouzid, D.; Visseaux, B.; Kassasseya, C.; Daoud, A.; Fémy, F.; Hermand, C.; Truchot, J.; Beaune, S.; Javaud, N.; Peyrony, O.; et al. Comparison of Patients Infected With Delta Versus Omicron COVID-19 Variants Presenting to Paris Emergency Departments: A Retrospective Cohort Study. Ann. Intern. Med. 2022, 175, 831–837. [Google Scholar] [CrossRef]
- Hause, A.M.; Marquez, P.; Zhang, B.; Myers, T.R.; Gee, J.; Su, J.R.; Parker, C.; Thompson, D.; Panchanathan, S.S.; Shimabukuro, T.T.; et al. COVID-19 mRNA Vaccine Safety Among Children Aged 6 Months-5 Years—United States, June 18, 2022-August 21, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Roy, A. Determinants of COVID-19 vaccination: Evidence from the US pulse survey. PLoS Glob. Public Health 2023, 3, e0001927. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Nguyen, N.; Fouayzi, H.; Crawford, S.; Singh, S.; Dong, M.; Wittenberg, R.; Mazor, K.M. From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey. Public Health Rep. 2023, 138, 681–690. [Google Scholar] [CrossRef]
- Zintel, S.; Flock, C.; Arbogast, A.L.; Forster, A.; von Wagner, C.; Sieverding, M. Gender differences in the intention to get vaccinated against COVID-19: A systematic review and meta-analysis. Z. Fur Gesundheitswissenschaften J. Public Health 2022, 31, 1303–1327. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Zhu, Y.; Chu, M. Role of COVID-19 Vaccines in SARS-CoV-2 Variants. Front. Immunol. 2022, 13, 898192. [Google Scholar] [CrossRef]
- Zeng, B.; Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 vaccines against SARS-CoV-2 variants of concern: A systematic review and meta-analysis. BMC Med. 2022, 20, 200. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Liang, Y.; Yu, D.; Du, B.; Cheng, W.; Li, L.; Yu, Z.; Luo, S.; Zhang, Y.; Wang, H.; et al. A systematic review of Vaccine Breakthrough Infections by SARS-CoV-2 Delta Variant. Int. J. Biol. Sci. 2022, 18, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Klann, J.G.; Strasser, Z.H.; Hutch, M.R.; Kennedy, C.J.; Marwaha, J.S.; Morris, M.; Samayamuthu, M.J.; Pfaff, A.C.; Estiri, H.; South, A.M.; et al. Distinguishing Admissions Specifically for COVID-19 From Incidental SARS-CoV-2 Admissions: National Retrospective Electronic Health Record Study. J. Med. Internet Res. 2022, 24, e37931. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Pradhan, A.; Olsson, P.E. Sex differences in severity and mortality from COVID-19: Are males more vulnerable? Biol. Sex Differ. 2020, 11, 53. [Google Scholar] [CrossRef]
- Chanana, N.; Palmo, T.; Sharma, K.; Kumar, R.; Graham, B.B.; Pasha, Q. Sex-derived attributes contributing to SARS-CoV-2 mortality. Am. J. Physiol. Endocrinol. Metab. 2020, 319, E562–E567. [Google Scholar] [CrossRef]
- Thangavel, H.; Dhanyalayam, D.; Lizardo, K.; Oswal, N.; Dolgov, E.; Perlin, D.S.; Nagajyothi, J.F. Susceptibility of Fat Tissue to SARS-CoV-2 Infection in Female hACE2 Mouse Model. Int. J. Mol. Sci. 2023, 24, 1314. [Google Scholar] [CrossRef]
- Gadi, N.; Wu, S.C.; Spihlman, A.P.; Moulton, V.R. What’s Sex Got to Do With COVID-19? Gender-Based Differences in the Host Immune Response to Coronaviruses. Front. Immunol. 2020, 11, 2147. [Google Scholar] [CrossRef]
- Bwire, G.M. Coronavirus: Why Men are More Vulnerable to COVID-19 Than Women? SN Compr. Clin. Med. 2020, 2, 874–876. [Google Scholar]
- Janssen (Johnson & Johnson) COVID-19 Vaccine. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/janssen/index.html (accessed on 30 June 2022).
- Gupta, A.; Marzook, H.; Ahmad, F. Comorbidities and clinical complications associated with SARS-CoV-2 infection: An overview. Clin. Exp. Med. 2023, 23, 313–331. [Google Scholar] [CrossRef]
- Khan, A.; El Hosseiny, A.; Siam, R. Assessing and Reassessing the Association of Comorbidities and Coinfections in COVID-19 Patients. Cureus 2023, 15, e36683. [Google Scholar]
- Darvishi, M.; Nazer, M.R.; Shahali, H.; Nouri, M. Association of thyroid dysfunction and COVID-19: A systematic review and meta-analysis. Front. Endocrinol. 2022, 13, 947594. [Google Scholar] [CrossRef]
- Almonte, M.; Au, X.Y.; Ali, M.; Rajabalee, N.; Hasan, S.; Shibre, T.; Li, Y.; Kaplan, A.C. Association Between COVID-19 Outcomes and Patient Characteristics: A Study in an Inner-City Community Hospital. Cureus 2021, 13, e17255. [Google Scholar] [CrossRef] [PubMed]
- Duerr, R.; Dimartino, D.; Marier, C.; Zappile, P.; Wang, G.; Lighter, J.; Elbel, B.; Troxel, A.B.; Heguy, A. Dominance of Alpha and Iota variants in SARS-CoV-2 vaccine breakthrough infections in New York City. J. Clin. Investig. 2021, 131, e152702. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, E.J.; Lee, S.W.; Kwon, D. Review of the early reports of the epidemiological characteristics of the B.1.1.7 variant of SARS-CoV-2 and its spread worldwide. Osong Public Health Res. Perspect. 2021, 12, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Manjunath, R.; Gaonkar, S.L.; Saleh, E.A.M.; Husain, K. A comprehensive review on COVID-19 Omicron (B.1.1.529) variant. Saudi J. Biol. Sci. 2022, 29, 103372. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bhattacharya, M.; Nag, S.; Dhama, K.; Chakraborty, C. A Detailed Overview of SARS-CoV-2 Omicron: Its Sub-Variants, Mutations and Pathophysiology, Clinical Characteristics, Immunological Landscape, Immune Escape, and Therapies. Viruses 2023, 15, 167. [Google Scholar] [CrossRef]
- Shrestha, L.B.; Foster, C.; Rawlinson, W.; Tedla, N.; Bull, R.A. Evolution of the SARS-CoV-2 omicron variants BA.1 to BA.5: Implications for immune escape and transmission. Rev. Med. Virol. 2022, 32, e2381. [Google Scholar] [CrossRef]
- Alderson, J.; Batchelor, V.; O’Hanlon, M.; Cifuentes, L.; Richter, F.C.; Kopycinski, J. Overview of approved and upcoming vaccines for SARS-CoV-2: A living review. Oxf. Open Immunol. 2021, 2, iqab010. [Google Scholar] [CrossRef]
- Lai, A.; Bergna, A.; Della Ventura, C.; Zehender, G. Genomic epidemiology and phylogenetics applied to the study of SARS-CoV-2 pandemic. New Microbiol. 2023, 46, 1–8. [Google Scholar]
- Oude Munnink, B.B.; Worp, N.; Nieuwenhuijse, D.F.; Sikkema, R.S.; Haagmans, B.; Fouchier, R.A.M.; Koopmans, M. The next phase of SARS-CoV-2 surveillance: Real-time molecular epidemiology. Nat. Med. 2021, 27, 1518–1524. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variant of Concern | Pango Lineage | Spike Protein Mutations |
|---|---|---|
| Alpha | B.1.1.7 | ΔH69/V70, N501Y |
| Beta a | B.1.351 | E484K, N501Y |
| Gamma a | P.1 (B.1.1.28.1) | E484K, N501Y |
| Delta | B.1.617.2 | L452R, T478K |
| Omicron | B.1.1.529 | T478K, E484A, N501Y, Y505H |
| BA.1 | B.1.1.529.1 | A67V, ΔH69/V70, T478K, E484A, N501Y, Y505H |
| BA.2 | B.1.1.529.2 | T478K, E484A, N501Y, Y505H |
| BA.2.12.1 | B.1.1.529.2.12.1 | L452Q, T478K, E484A, N501Y, Y505H |
| BA.4/BA.5 b | B.1.1.529.4/5 | ΔH69/V70, L452R, T478K, E484A, F486V, N501Y, Y505H |
| Outcome | Total | Unvaccinated | Vaccinated | RRCRUDE | 95% CI | p-Value | RRADJUSTED | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| ICU Admissions, n (%) | 336 (6.7) | 268 (7.8) | 68 (4.3) | 2.07 | [1.51, 2.83] | <0.001 | |||
| Age, median (IQR) | 68 (57–78) | 67 (56–76) | 72 (60–83) | 1.07 | [1.06, 1.08] | <0.001 | 1.07 | [1.06, 1.09] | <0.001 |
| Gender, n (%) | |||||||||
| Male | 197 (58.6) | 154 (57.5) | 43 (63.2) | 1.82 | [1.41, 2.36] | <0.001 | 0.79 | [0.57, 1.09] | 0.16 |
| Female | 139 (41.4) | 114 (42.5) | 25 (36.8) | 0.55 | [0.42, 0.71] | <0.001 | 1.26 | [0.91, 1.75] | 0.16 |
| Race/Ethnicity, n (%) | |||||||||
| Hispanic | 59 (17.6) | 49 (18.3) | 10 (14.7) | 0.95 | [0.51, 1.74] | 0.87 | 0.52 | [0.20, 1.26] | 0.15 |
| Asian | 15 (4.5) | 12 (4.5) | 3 (4.4) | 2.49 | [0.37, 1.70] | 0.08 | 1.05 | [0.29, 4.56] | 0.94 |
| Black | 22 (6.5) | 21 (7.8) | 1 (1.5) | 0.35 | [0.14, 0.79] | 0.02 | 2.84 | [0.61, 41.66] | 0.28 |
| White | 210 (62.5) | 161 (60.1) | 49 (72.1) | 1.48 | [0.94, 2.36] | 0.09 | 0.72 | [0.32, 1.36] | 0.35 |
| Ventilator Support, n (%) | 236 (4.7) | 185 (5.4) | 51 (3.2) | 1.85 | [1.30, 2.69] | <0.001 | |||
| Age, median (IQR) | 70 (60–79) | 69 (60–78) | 72 (64–83) | 1.09 | [1.07, 1.10] | <0.001 | 1.09 | [1.07, 1.10] | <0.001 |
| Gender, n (%) | |||||||||
| Male | 141 (59.7) | 109 (58.9) | 32 (62.7) | 1.90 | [1.40, 2.56] | <0.001 | 0.83 | [0.57, 1.21] | 0.34 |
| Female | 95 (40.3) | 76 (41.1) | 19 (37.3) | 0.53 | [0.39, 0.71] | <0.001 | 1.20 | [0.83, 1.76] | 0.34 |
| Race/Ethnicity, n (%) | |||||||||
| Hispanic | 49 (20.8) | 39 (21.1) | 10 (19.6) | 1.31 | [0.66, 2.57] | 0.44 | 1.04 | [0.48, 2.21] | 0.91 |
| Asian | 10 (4.2) | 8 (4.3) | 2 (3.9) | 1.89 | [0.50, 5.90] | 0.31 | 2.23 | [0.49, 7.93] | 0.25 |
| Black | 17 (7.2) | 17 (9.2) | 0 (0.0) | 0.41 | [0.15, 1.03] | 0.07 | 0.56 | [0.20, 1.46] | 0.26 |
| White | 137 (58.1) | 104 (56.2) | 33 (64.7) | 1.89 | [0.64, 1.89] | 0.75 | 1.06 | [0.58, 1.96] | 0.86 |
| Mortality, n (%) | 430 (8.6) | 320 (9.3) | 110 (7.0) | 1.44 | [1.11, 1.87] | 0.01 | |||
| Age, median (IQR) | 75 (65–85) | 74 (63–85) | 79 (68–87) | 1.14 | [1.13, 1.16] | <0.001 | 1.14 | [1.13, 1.16] | <0.001 |
| Gender, n (%) | |||||||||
| Male | 245 (57.0) | 174 (54.4) | 71 (64.5) | 2.03 | [1.56, 2.66] | <0.001 | 0.7 | [0.53, 0.92] | 0.01 |
| Female | 185 (43.0) | 146 (45.6) | 39 (35.5) | 0.59 | [0.46, 0.74] | <0.001 | 1.43 | [1.09, 1.87] | 0.01 |
| Race/Ethnicity, n (%) | |||||||||
| Hispanic | 58 (13.5) | 44 (13.8) | 14 (12.7) | 1.23 | [0.57, 2.65] | 0.60 | 0.46 | [0.21, 0.99] | 0.05 |
| Asian | 16 (3.7) | 13 (4.1) | 3 (2.7) | 1.76 | [0.42, 5.63] | 0.38 | 1.76 | [0.54, 7.40] | 0.38 |
| Black | 25 (5.8) | 23 (7.2) | 2 (1.8) | 0.22 | [0.04, 0.74] | 0.03 | 2.14 | [0.63, 12.07] | 0.29 |
| White | 304 (70.7) | 220 (68.8) | 84 (76.4) | 3.33 | [1.94, 6.15] | <0.001 | 0.84 | [0.46, 1.44] | 0.55 |
| Comorbidity | Chi-Square Statistic | Significance Bar | p-Value |
|---|---|---|---|
| Heart Disease | 44.54 |  | <0.001 |
| Hypertension | 41.06 | <0.001 | |
| Cancer | 34.45 | <0.001 | |
| Diabetes | 31.02 | <0.001 | |
| Hyperlipidemia | 17.61 | <0.001 | |
| Obesity | 3.1 | 0.10 | |
| Thyroid Disease | 1.82 | 0.20 | |
| Respiratory Disease | 1.47 | 0.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mediavilla, J.R.; Lozy, T.; Lee, A.; Kim, J.; Kan, V.W.; Titova, E.; Amin, A.; Zody, M.C.; Corvelo, A.; Oschwald, D.M.; et al. Molecular and Clinical Epidemiology of SARS-CoV-2 Infection among Vaccinated and Unvaccinated Individuals in a Large Healthcare Organization from New Jersey. Viruses 2023, 15, 1699. https://doi.org/10.3390/v15081699
Mediavilla JR, Lozy T, Lee A, Kim J, Kan VW, Titova E, Amin A, Zody MC, Corvelo A, Oschwald DM, et al. Molecular and Clinical Epidemiology of SARS-CoV-2 Infection among Vaccinated and Unvaccinated Individuals in a Large Healthcare Organization from New Jersey. Viruses. 2023; 15(8):1699. https://doi.org/10.3390/v15081699
Chicago/Turabian StyleMediavilla, José R., Tara Lozy, Annie Lee, Justine Kim, Veronica W. Kan, Elizabeth Titova, Ashish Amin, Michael C. Zody, André Corvelo, Dayna M. Oschwald, and et al. 2023. "Molecular and Clinical Epidemiology of SARS-CoV-2 Infection among Vaccinated and Unvaccinated Individuals in a Large Healthcare Organization from New Jersey" Viruses 15, no. 8: 1699. https://doi.org/10.3390/v15081699