
Laboratory Based Surveillance of HIV-1 Acquired Drug Resistance in Cameroon: Implications for Use of Tenofovir-Lamivudine-Dolutegravir (TLD) as Second- or Third-Line Regimens
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Target Population
2.2. Study Site Description
2.3. Sample Size Calculation and Sampling Method
2.4. Selection Criteria
2.5. Enrolment Procedure
2.6. Procedure for GRT
2.7. Sequence Interpretation and Analysis
2.8. Data Interpretation and Statistical Analysis
2.9. Ethical Considerations
3. Results
3.1. Socio-Demographic and Clinical Data
3.2. Immuno-Virological Characteristics
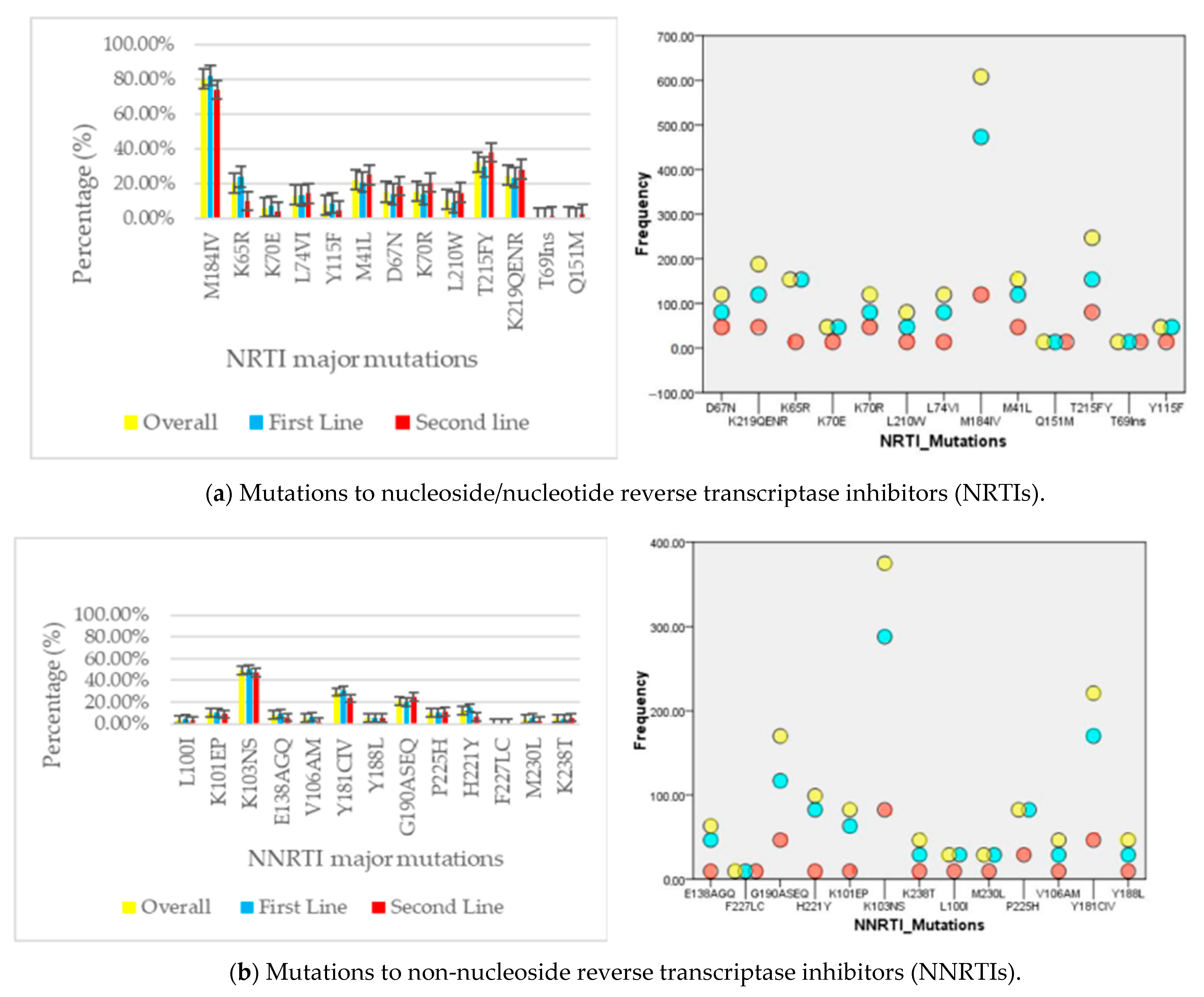
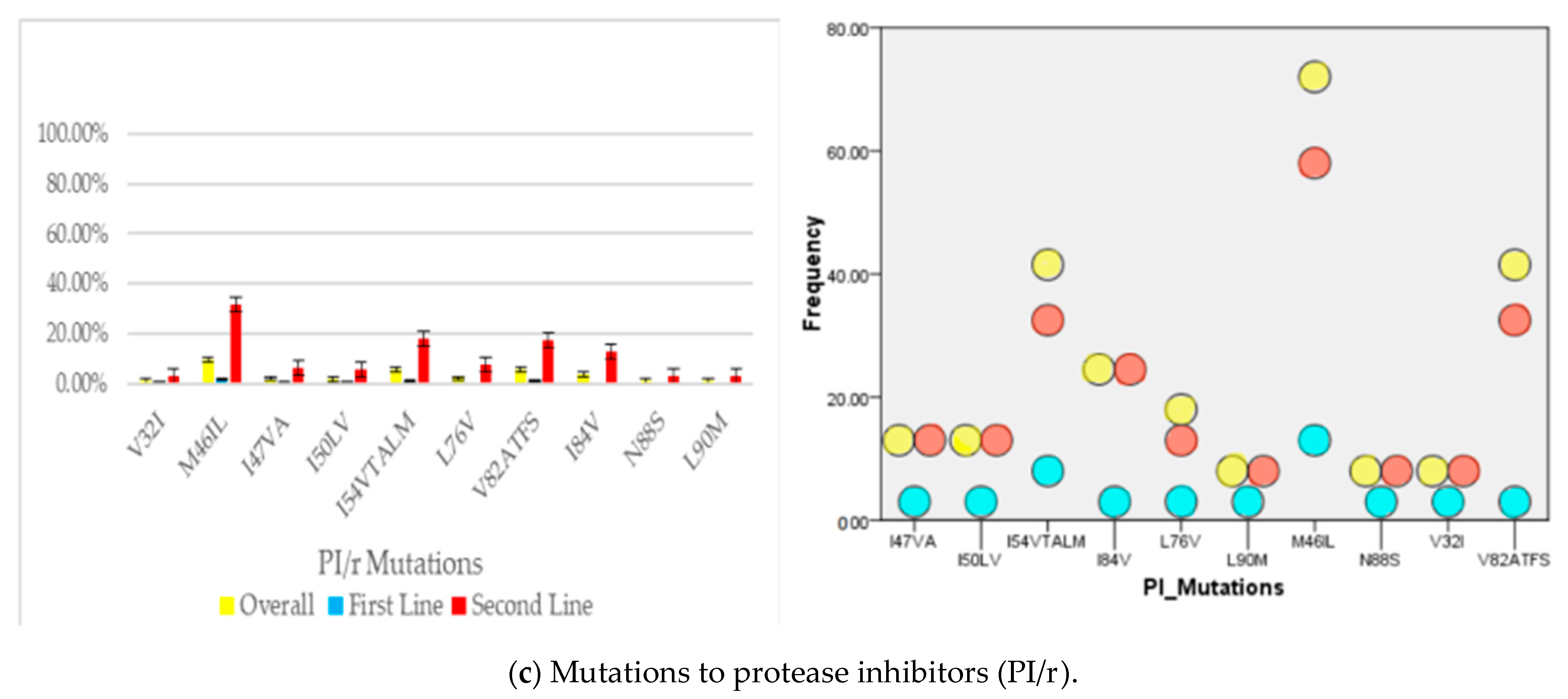
3.3. Acquired Drug Resistance Patterns
3.4. Genetic Diversity
3.5. Potentially Active Drugs
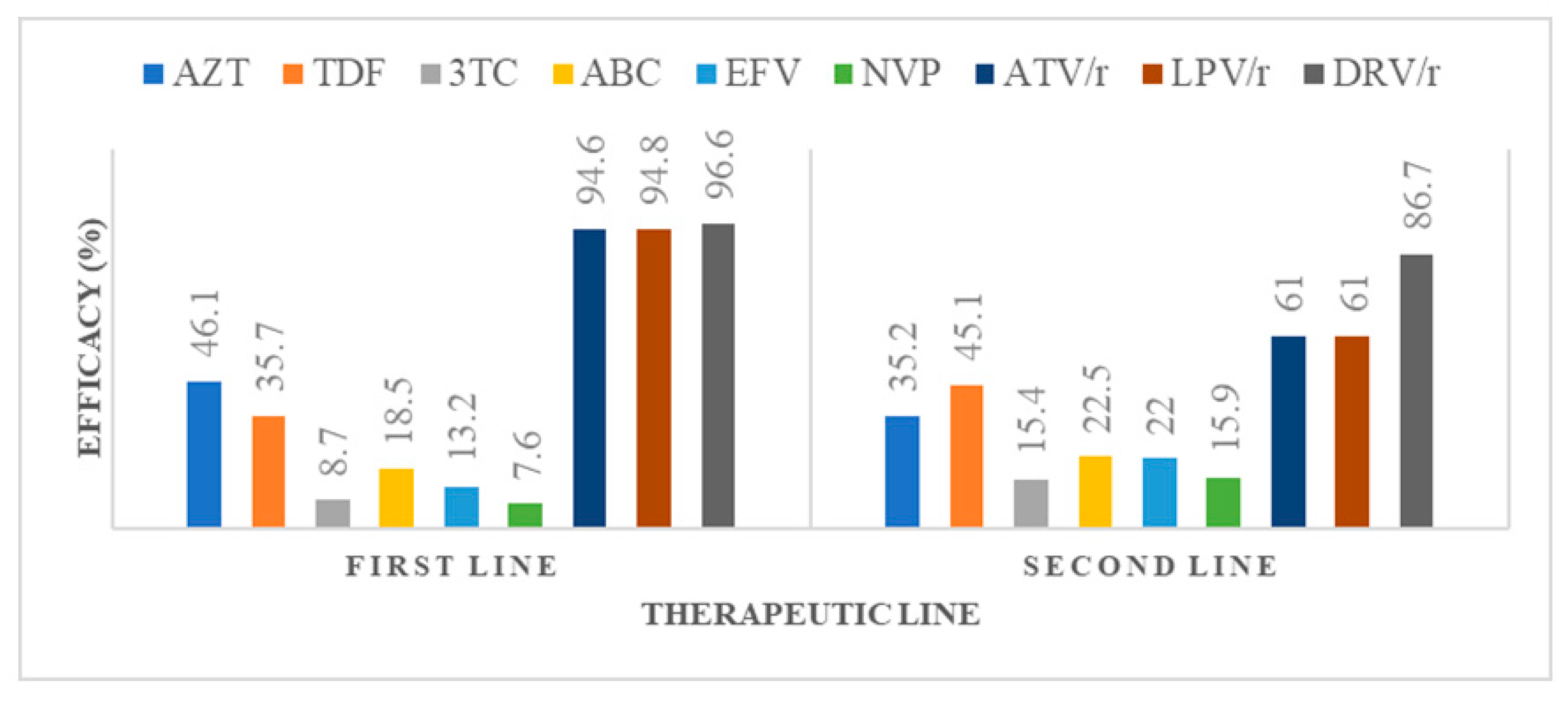
3.5.1. Potential Efficacy of Commonly Used Antiretroviral Drugs after First- and Second-Line Failure
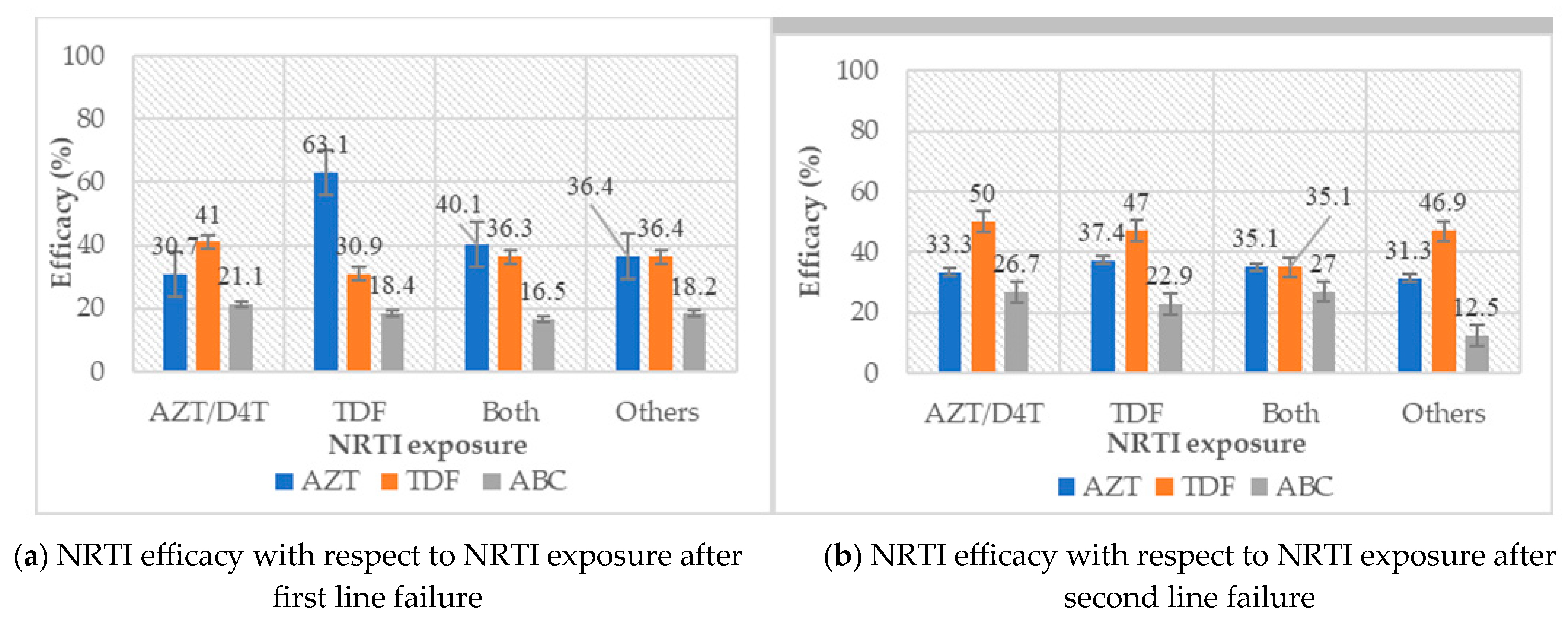
3.5.2. Efficacy of NRTI Molecules with Respect to NRTI Exposure
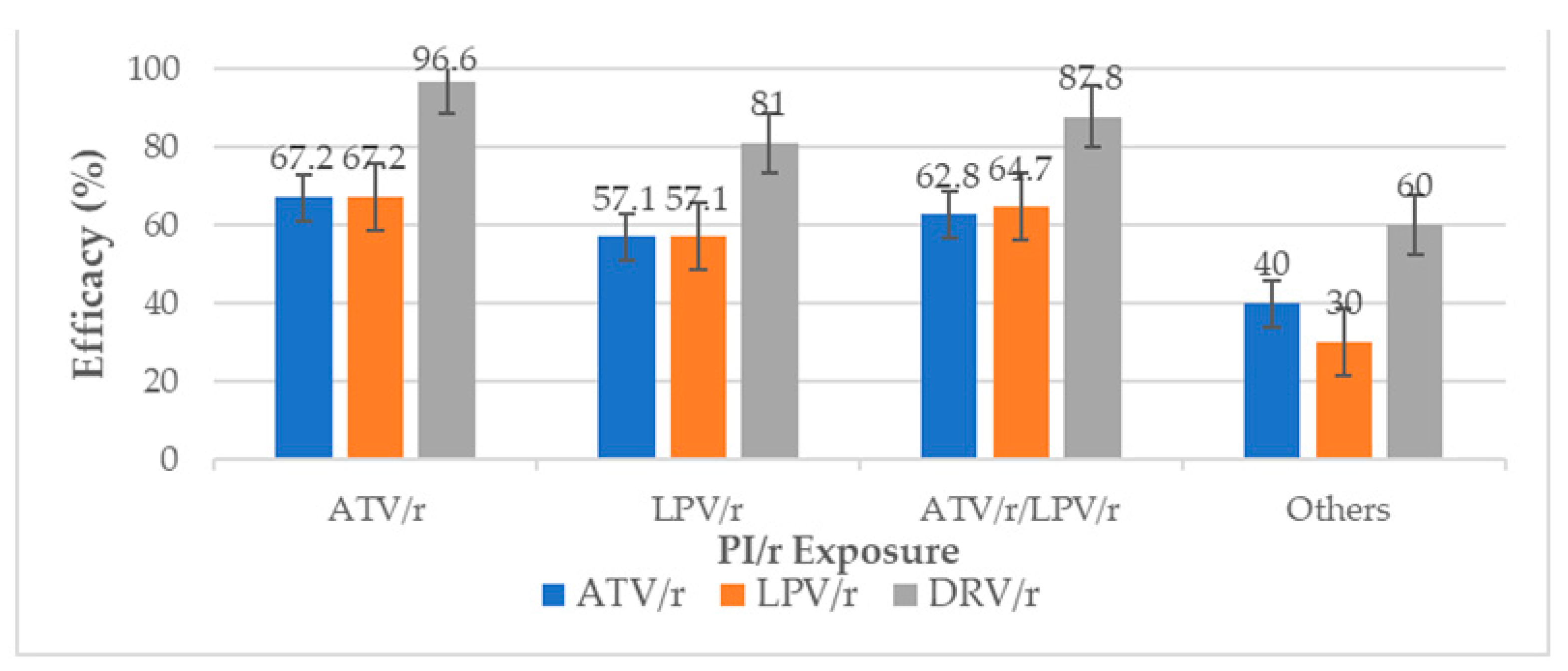
3.5.3. Efficacy of ATV/r, LPV/r and DRV/r with Respect to PI/r Exposure
3.5.4. Predictive Efficacy of TLD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global HIV & AIDS Statistics—Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 9 March 2023).
- HIV Data and Statistics. Available online: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics (accessed on 5 September 2022).
- TimesNews2. HIV Prevalence Rate in Cameroon Drops to 2.7%. TimesNews2. 2019. Available online: http://timesnews2.info/hiv-prevalence-rate-in-cameroon-drops-to-2-7/ (accessed on 21 June 2020).
- Sidibe, M. UNAIDS DATA 2017. 2017, p. 54. Available online: http://aidsinfo.unaids.org (accessed on 2 June 2018).
- The World Bank Group. The World Bank Data—Antiretroviral Therapy Coverage (% of people living with HIV). 2017. Available online: https://data.worldbank.org/indicator/SH.HIV.ARTC.ZS (accessed on 16 December 2017).
- July 31 CSH govDate Last Updated: 2019. Global Statistics. HIV.gov. 2019. Available online: https://www.hiv.gov/hiv-basics/overview/data-and-trends/global-statistics (accessed on 20 June 2020).
- UNAIDS. Global AIDS up Date 2016. Geneva-Switzerland. 2016, pp. 3–4. Available online: https://www.unaids.org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf (accessed on 9 March 2023).
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 drug resistance and resistance testing. Infect. Genet. Evol. 2016, 46, 292–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceccarelli, L.; Salpini, R.; Moudourou, S.; Cento, V.; Santoro, M.M.; Fokam, J.; Takou, D.; Nanfack, A.; Dori, L.; Torimiro, J.; et al. Characterization of drug resistance mutations in naïve and ART-treated patients infected with HIV-1 in Yaounde, Cameroon. J. Med. Virol. 2012, 84, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Tchouwa, G.F. HIV Pre-Treatment Drug Resistance in Cameroon: First Nationwide Study. 2017. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahUKEwjeuPDC1I_bAhVHtRQKHQXqCY4QFggsMAA&url=http%3A%2F%2Fregist2.virology-education.com%2F2017%2FINTEREST%2F58_Tchouwa.pdf&usg=AOvVaw3ptG86_gOoDivwxFsFtlHi (accessed on 18 May 2018).
- WHO. Sentinel Surveys of Acquired HIV Resistance to Dolutegravir among People Receiving Dolutegravir-Containing Antiretroviral Therapy; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach. Available online: https://www.who.int/publications-detail-redirect/9789240031593 (accessed on 9 March 2023).
- Scott, L.J. Dolutegravir/Lamivudine Single-Tablet Regimen: A Review in HIV-1 Infection. Drugs 2020, 80, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, L.; De Vito, A.; Ricci, E.D.; Orofino, G.; Squillace, N.; Menzaghi, B.; Molteni, C.; Gulminetti, R.; De Socio, G.V.; Pellicanò, G.F.; et al. Durability of Dolutegravir-Based Regimens: A 5-Year Prospective Observational Study. AIDS Patient Care STDS 2021, 35, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Ciccullo, A.; Borghi, V.; Giacomelli, A.; Cossu, M.V.; Sterrantino, G.; Latini, A.; Giacometti, A.; De Vito, A.; Gennari, W.; Madeddu, G.; et al. Five Years With Dolutegravir Plus Lamivudine as a Switch Strategy: Much More Than a Positive Finding. J. Acquir. Immune Defic. Syndr. 2021, 88, 234–237. [Google Scholar] [CrossRef]
- Keene, C.M.; Griesel, R.; Zhao, Y.; Gcwabe, Z.; Sayed, K.; Hill, A.; Cassidy, T.; Ngwenya, O.; Jackson, A.; van Zyl, G.; et al. Virologic efficacy of tenofovir, lamivudine and dolutegravir as second-line antiretroviral therapy in adults failing a tenofovir-based first-line regimen. AIDS 2021, 35, 1423–1432. [Google Scholar] [CrossRef]
- Schramm, B.; Temfack, E.; Descamps, D.; Nicholas, S.; Peytavin, G.; Bitilinyu-Bangoh, J.E.; Storto, A.; Lê, M.P.; Abdi, B.; Ousley, J.; et al. Viral suppression and HIV-1 drug resistance 1 year after pragmatic transitioning to dolutegravir first-line therapy in Malawi: A prospective cohort study. Lancet HIV 2022, 9, e544–e553. [Google Scholar] [CrossRef]
- Kouamou, V.; Manasa, J.; Katzenstein, D.; McGregor, A.M.; Ndhlovu, C.E.; Makadzange, A.T. Drug resistance and optimizing dolutegravir regimens for adolescents and young adults failing antiretroviral therapy. AIDS 2019, 33, 1729–1737. [Google Scholar] [CrossRef]
- Woods, C.K.; Brumme, C.J.; Liu, T.F.; Chui, C.K.S.; Chu, A.L.; Wynhoven, B.; Hall, T.A.; Trevino, C.; Shafer, R.W.; Harrigan, P.R. Automating HIV drug resistance genotyping with RECall, a freely accessible sequence analysis tool. J. Clin. Microbiol. 2012, 50, 1936–1942. [Google Scholar] [CrossRef]
- Ayele, G.; Tessema, B.; Amsalu, A.; Ferede, G.; Yismaw, G. Prevalence and associated factors of treatment failure among HIV/AIDS patients on HAART attending University of Gondar Referral Hospital Northwest Ethiopia. BMC Immunol. 2018, 19, 37. [Google Scholar] [CrossRef]
- Zdanowicz, M.M. The Pharmacology of HIV Drug Resistance. Am. J. Pharm. Educ. 2006, 70, 100. [Google Scholar] [CrossRef] [Green Version]
- Emu, B.; Fessel, J.; Schrader, S.; Kumar, P.; Richmond, G.; Win, S.; Weinheimer, S.; Marsolais, C.; Lewis, S. Phase 3 Study of Ibalizumab for Multidrug-Resistant HIV-1. N. Eng. J. Med. 2018, 379, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Muccini, C.; Canetti, D.; Castagna, A.; Spagnuolo, V. Efficacy and Safety Profile of Fostemsavir for the Treatment of People with Human Immunodeficiency Virus-1 (HIV-1): Current Evidence and Place in Therapy. DDDT 2022, 16, 297–304. [Google Scholar] [CrossRef] [PubMed]
- HIV Undetectable=Untransmittable (U=U), or Treatment as Prevention|NIH: National Institute of Allergy and Infectious Diseases. Available online: https://www.niaid.nih.gov/diseases-conditions/treatment-prevention (accessed on 10 May 2023).
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; Degen, O.; Corbelli, G.M.; Estrada, V.; Geretti, A.M.; Beloukas, A.; et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): Final results of a multicentre, prospective, observational study. Lancet 2019, 393, 2428–2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madeddu, G.; De Vito, A.; Cozzi-Lepri, A.; Cingolani, A.; Maggiolo, F.; Perno, C.F.; Gagliardini, R.; Marchetti, G.; Saracino, A.; Monforte, A.D.; et al. Time spent with HIV-RNA ≤ 200 copies/mL in a cohort of people with HIV during the U=U era. AIDS 2021, 35, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Takou, D.; Fokam, J.; Teto, G.; Santoro, M.-M.; Ceccherini-Silberstein, F.; Nanfack, A.J.; Sosso, S.M.; Dambaya, B.; Salpini, R.; Billong, S.C.; et al. HIV-1 drug resistance testing is essential for heavily-treated patients switching from first- to second-line regimens in resource-limited settings: Evidence from routine clinical practice in Cameroon. BMC Infect. Dis. 2019, 19, 246. [Google Scholar] [CrossRef] [Green Version]
- Semengue, E.N.J.; Armenia, D.; Inzaule, S.; Santoro, M.M.; Dambaya, B.; Takou, D.; Teto, G.; Nka, A.D.; Yagai, B.; Fabeni, L.; et al. Baseline integrase drug resistance mutations and conserved regions across HIV-1 clades in Cameroon: Implications for transition to dolutegravir in resource-limited settings. J. Antimicrob. Chemother. 2021, 76, 1277–1285. [Google Scholar] [CrossRef]
- Fokam, J.; Takou, D.; Semengue, E.N.J.; Teto, G.; Beloumou, G.; Dambaya, B.; Santoro, M.-M.; Mossiang, L.; Billong, S.C.; Cham, F.; et al. First case of Dolutegravir and Darunavir/r multi drug-resistant HIV-1 in Cameroon following exposure to Raltegravir: Lessons and implications in the era of transition to Dolutegravir-based regimens. Antimicrob. Resist. Infect. Control 2020, 9, 143. [Google Scholar] [CrossRef]
- Tsai, H.C.; Chen, I.T.; Wu, K.S.; Tseng, Y.T.; Sy, C.L.; Chen, J.K.; Lee, S.S.J.; Chen, Y.S. High rate of HIV-1 drug resistance in treatment failure patients in Taiwan, 2009–2014. Infect. Drug Resist. 2017, 10, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Manasa, J.; Danaviah, S.; Lessells, R.; Elshareef, M.; Tanser, F.; Wilkinson, E.; Pillay, S.; Mthiyane, H.; Mwambi, H.; Pillay, D.; et al. Increasing HIV-1 Drug Resistance Between 2010 and 2012 in Adults Participating in Population-Based HIV Surveillance in Rural KwaZulu-Natal, South Africa. AIDS Res. Hum. Retrovir. 2016, 32, 763–769. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Sanchez, P.G.; Guerra-Palomares, S.E.; Ramirez-GarciaLuna, J.L.; Arguello, J.R.; Noyola, D.E.; Garcia-Sepulveda, C.A. Prevalence of Drug Resistance Mutations in Protease, Reverse Transcriptase, and Integrase Genes of North Central Mexico HIV Isolates. AIDS Res. Hum. Retrovir. 2018, 34, 498–506. [Google Scholar] [CrossRef]
- Chimbetete, C.; Katzenstein, D.; Shamu, T.; Spoerri, A.; Estill, J.; Egger, M.; Keiser, O. HIV-1 Drug Resistance and Third-Line Therapy Outcomes in Patients Failing Second-Line Therapy in Zimbabwe. Open Forum Infect. Dis. 2018, 5, ofy005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, V.; Yeni, P. Non-nucleoside reverse transcriptase inhibitors. Ann. Med. Interne 2000, 151, 260–267. [Google Scholar]
- Mackie, N. Resistance to non-Nucleoside Reverse Transcriptase Inhibitors. In Antiretroviral Resistance in Clinical Practice; Geretti, A.M., Ed.; Mediscript: London, UK, 2006. Available online: http://www.ncbi.nlm.nih.gov/books/NBK2249/ (accessed on 21 June 2020).
- Cao, P.; Su, B.; Wu, J.; Wang, Z.; Yan, J.; Song, C.; Ruan, Y.; Xing, H.; Shao, Y.; Liao, L. Treatment outcomes and HIV drug resistance of patients switching to second-line regimens after long-term first-line antiretroviral therapy: An observational cohort study. Medicine 2018, 97, e11463. [Google Scholar] [CrossRef] [PubMed]
- Maiga, A.I.; Fofana, D.B.; Cisse, M.; Diallo, F.; Maiga, M.Y.; Traore, H.A.; Maiga, I.A.; Sylla, A.; Taiwo, B.; Murphy, R.; et al. Characterization of HIV-1 antiretroviral drug resistance after second-line treatment failure in Mali, a limited-resources setting. J. Antimicrob. Chemother. 2012, 67, 2943–2948. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Participants (n = 759) |
|---|---|
| Age in years, mean ± SD | 42 ± 14 |
| Gender n (%) | |
| Females | 485 (63.9%) |
| Males | 274 (36.1%) |
| Viral load (copies/mL), median (IQR) | 138,666 (28,979–533,066) |
| CD 4 Count (cells/µL), median (IQR) | 153 (50–308) |
| ART Duration in months, median (IQR) | 63 (35.0–105) |
| Therapeutic exposure, n (%) | |
| First-line ART regimens | 575 (75.8%) |
| First-line NRTI exposure | |
| 1 (0.2%) |
| 166 (28.8%) |
| 217 (37.6%) |
| 182 (31.5%) |
| 11 (1.91%) |
| Second-line ART regimens | 184 (24.2%) |
| Second-Line PI/r exposure | |
| 58 (31.9%) |
| 63 (34.6%) |
| 51 (28.0%) |
| 10 (5.5%) |
| Second-line NRTI exposure | |
| 30 (16.5%) |
| 83 (45.6%) |
| 37 (20.3%) |
| 32 (17.6%) |
| CRF02_AG | Non-CRF02_AG | OR, p-Value | Pure | Recombinant | OR, p-Value | |
|---|---|---|---|---|---|---|
| Median viral load (copies/mL) | 150 (38–285) | 158 (55–299) | NA, 0.32 | 159 (56–301) | 150 (38–287) | NA, 0.4 |
| Median CD4 (cells/ µL) | 145,872 (23,805–505,458) | 132,913 (23,998–416,268) | NA, 0.44 | 115,979 (29,008–573,478) | 149,947 (26,664–467,444) | NA, 0.8 |
| HIVDR (%) | 92.8 | 94.9 | 0.7, 0.286 | 96.7 | 92.6 | 2.3, 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fokam, J.; Chenwi, C.A.; Takou, D.; Santoro, M.M.; Tala, V.; Teto, G.; Beloumou, G.; Semengue, E.N.J.; Dambaya, B.; Djupsa, S.; et al. Laboratory Based Surveillance of HIV-1 Acquired Drug Resistance in Cameroon: Implications for Use of Tenofovir-Lamivudine-Dolutegravir (TLD) as Second- or Third-Line Regimens. Viruses 2023, 15, 1683. https://doi.org/10.3390/v15081683
Fokam J, Chenwi CA, Takou D, Santoro MM, Tala V, Teto G, Beloumou G, Semengue ENJ, Dambaya B, Djupsa S, et al. Laboratory Based Surveillance of HIV-1 Acquired Drug Resistance in Cameroon: Implications for Use of Tenofovir-Lamivudine-Dolutegravir (TLD) as Second- or Third-Line Regimens. Viruses. 2023; 15(8):1683. https://doi.org/10.3390/v15081683
Chicago/Turabian StyleFokam, Joseph, Collins Ambe Chenwi, Desire Takou, Maria Mercedes Santoro, Valere Tala, George Teto, Grace Beloumou, Ezechiel Ngoufack Jagni Semengue, Beatrice Dambaya, Sandrine Djupsa, and et al. 2023. "Laboratory Based Surveillance of HIV-1 Acquired Drug Resistance in Cameroon: Implications for Use of Tenofovir-Lamivudine-Dolutegravir (TLD) as Second- or Third-Line Regimens" Viruses 15, no. 8: 1683. https://doi.org/10.3390/v15081683