
Maternal Fever and Reduced Fetal Movement as Predictive Risk Factors for Adverse Neonatal Outcome in Cases of Congenital SARS-CoV-2 Infection: A Meta-Analysis of Individual Participant Data from Case Reports and Case Series

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
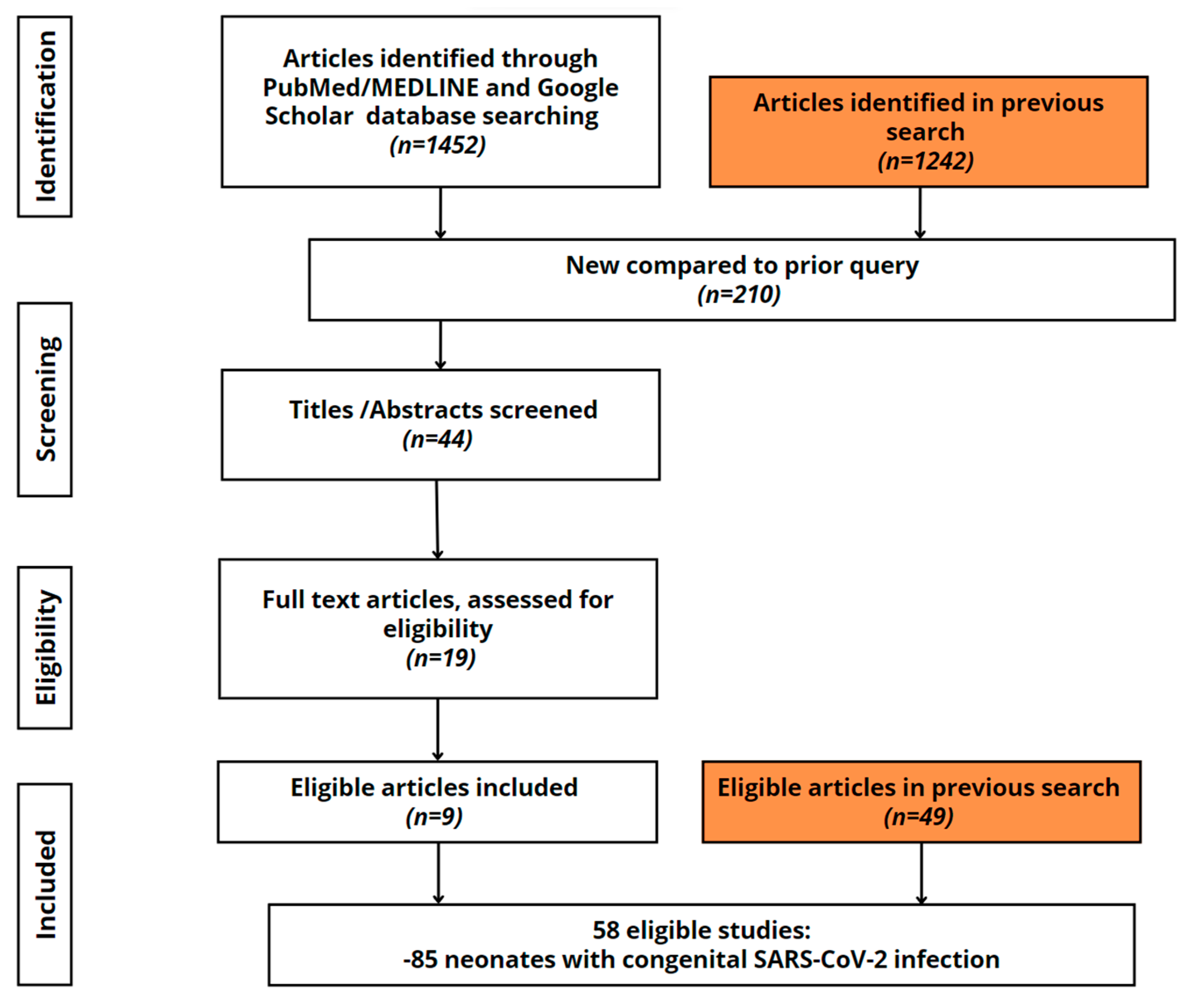
2.1. The Search Strategy
2.2. Updated Eligibility Criteria for the Meta-Analysis
2.3. Definition of Congenital SARS-CoV-2 Infection Following Standard Criteria
2.4. Outcome
2.5. Quality Assessment
2.6. Extraction of Relevant Data
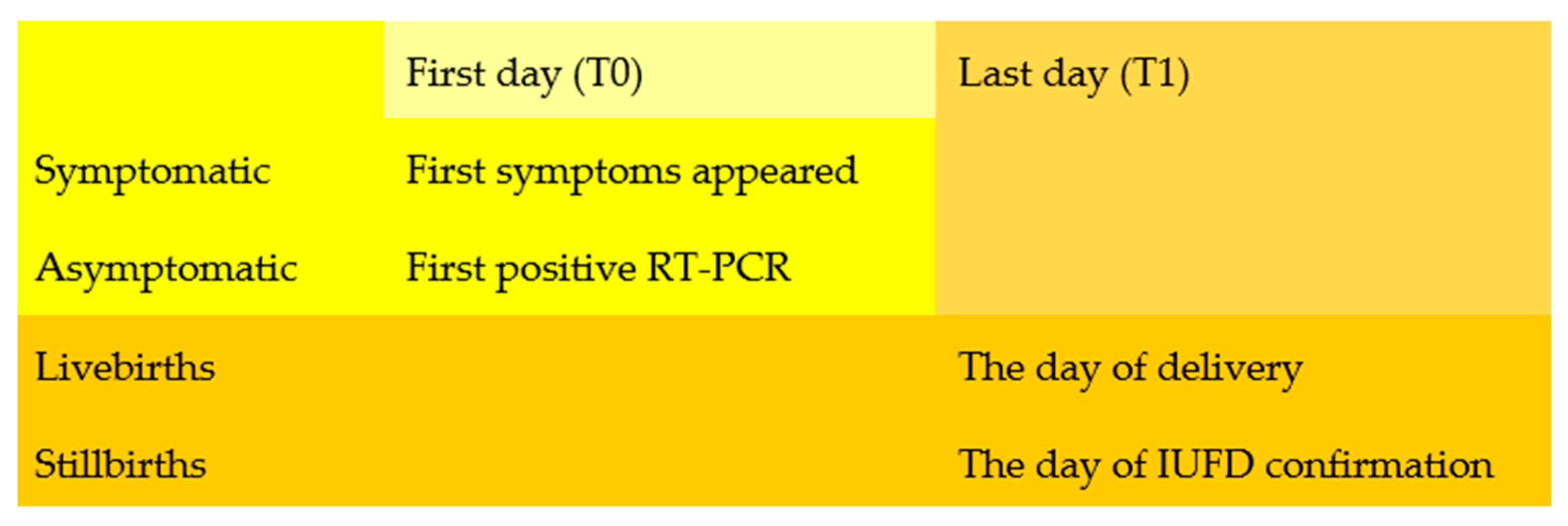
2.7. Special Consideration Regarding the Timelapse between Maternal Infection and Pregnancy Outcome
2.8. Data Analysis
3. Results
3.1. Baseline Maternal and Neonatal Characteristics
3.2. Analyzing Primary Neonatal Adverse Outcome
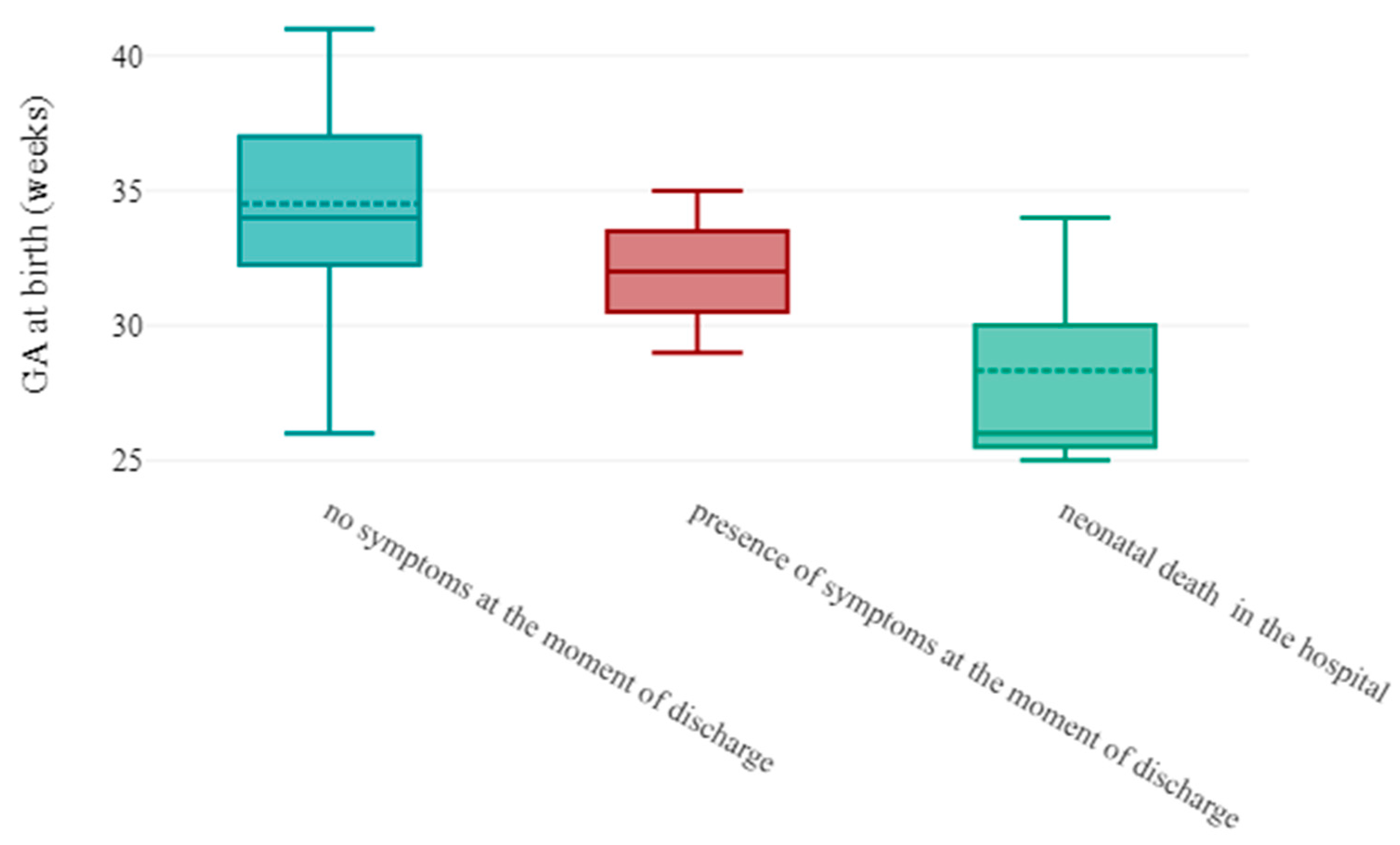
3.3. Analyzing Secondary Neonatal Adverse Outcome
4. Discussions
4.1. Maternal Metrics That Influence Neonatal Outcome
4.2. Obstetrical Metrics That Influence the Neonatal Outcome
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz, M.P.; Santos, E.; Cervantes, M.A.V.; Juárez, M.L. COVID-19, a worldwide public health emergency. Rev. Clin. Esp. Engl. Ed. 2021, 221, 55–61. [Google Scholar] [CrossRef]
- Chavan, M.; Qureshi, H.; Karnati, S.; Kollikonda, S. COVID-19 Vaccination in Pregnancy: The Benefits Outweigh the Risks. J. Obstet. Gynaecol. Can. 2021, 43, 814–816. [Google Scholar] [CrossRef]
- Morello, R.; Pepe, M.; Martino, L.; Lazzareschi, I.; Chiaretti, A.; Gatto, A.; Curatola, A. COVID-19 review shows that benefits of vaccinating children and adolescents appear to outweigh risks of post-vaccination myopericarditis. Acta Paediatr. 2022, 111, 1846–1852. [Google Scholar] [CrossRef]
- Pique-Regi, R.; Romero, R.; Tarca, A.L.; Luca, F.; Xu, Y.; Alazizi, A.; Leng, Y.; Hsu, C.D.; Gomez-Lopez, N. Does the human placenta express the canonical cell entry mediators for SARS-CoV-2? eLife 2020, 9, e58716. [Google Scholar] [CrossRef]
- Patanè, L.; Cadamuro, M.; Massazza, G.; Pirola, S.; Stagnati, V.; Comerio, C.; Carnelli, M.; Arosio, M.; Callegaro, A.P.; Tebaldi, P.; et al. Evidence of vertical transmission of SARS-CoV-2 and interstitial pneumonia in second-trimester twin stillbirth in asymptomatic woman. Case report and review of the literature. Am. J. Obstet. Gynecol. MFM 2022, 4, 100589. [Google Scholar] [CrossRef]
- Shah, P.S.; Diambomba, Y.; Acharya, G.; Morris, S.K.; Bitnun, A. Classification system and case definition for SARS-CoV-2 infection in pregnant women, fetuses, and neonates. Acta Obstet. Gynecol. Scand. 2020, 99, 565–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Definition and Categorization of the Timing of Mother-to-Child Transmission of SARS-CoV-2. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-mother-to-child-transmission-2021.1 (accessed on 7 January 2023).
- Mullins, E.; Hudak, M.L.; Banerjee, J.; Getzlaff, T.; Townson, J.; Barnette, K.; Playle, R.; Perry, A.; Bourne, T.; Lees, C.C. Pregnancy and neonatal outcomes of COVID-19: Coreporting of common outcomes from PAN-COVID and AAP-SONPM registries. Ultrasound Obstet. Gynecol. 2021, 57, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.; Pormohammad, A.; Sheikh Neshin, S.A.; Ghorbani, S.; Bose, D.; Alimohammadi, S.; Basirjafari, S.; Mohammadi, M.; Rasmussen-Ivey, C.; Razizadeh, M.H.; et al. Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: A systematic review and meta-analysis. Rev. Med. Virol. 2021, 31, e2208. [Google Scholar] [CrossRef]
- Edlow, A.G.; Li, J.Z.; Collier, A.-R.Y.; Atyeo, C.; James, K.E.; Boatin, A.A.; Gray, K.J.; Bordt, E.A.; Shook, L.L.; Yonker, L.M.; et al. Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2030455. [Google Scholar] [CrossRef] [PubMed]
- Elósegui, J.J.H.; García, A.L.C.; Risquez, A.C.F.; Quintana, M.B.; Does, J.F.E.M. the maternal-fetal transmission of SARS-CoV-2 occur during pregnancy? Rev. Clin. Esp. 2021, 221, 93–96. [Google Scholar] [CrossRef]
- Grimminck, K.; Santegoets, L.A.M.; Siemens, F.C.; Fraaij, P.L.A.; Reiss, I.K.M.; Schoenmakers, S. No evidence of vertical transmission of SARS-CoV-2 after induction of labour in an immune-suppressed SARS-CoV-2-positive patient. BMJ Case Rep. 2020, 13, e235581. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Yuan, J.; Wang, M.; Yu, Y.; Bian, J.; Fan, C. Case series of 20 pregnant women with 2019 novel coronavirus disease in Wuhan, China. J. Obstet. Gynaecol. Res. 2021, 47, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Bradshaw, C.; Auyeung, N.S.F.; Lumba, R.; Farkas, J.S.; Sweeney, N.B.; Wachtel, E.V.; Bailey, S.M.; Noor, A.; Kunjumon, B.; et al. Outcomes of Maternal-Newborn Dyads After Maternal SARS-CoV-2. Pediatrics 2020, 146, e2020005637. [Google Scholar] [CrossRef]
- Jin, J.H.; Kim, Y.; Yoo, J.; Kim, E.H.; Yoon, S.W. Two Cases of SARS-CoV-2-Positive Mothers and Their Newborns in Korea. Infect. Chemother. 2022, 54, 372–377. [Google Scholar] [CrossRef]
- Pashaei, Z.; SeyedAlinaghi, S.; Qaderi, K.; Barzegary, A.; Karimi, A.; Mirghaderi, S.P.; Mirzapour, P.; Tantuoyir, M.M.; Dadras, O.; Ali, Z.; et al. Prenatal and neonatal complications of COVID-19: A systematic review. Health Sci. Rep. 2022, 5, e510. [Google Scholar] [CrossRef]
- Di Guardo, F.; Di Grazia, F.M.; Di Gregorio, L.M.; Zambrotta, E.; Carrara, G.; Gulino, F.A.; Tuscano, A.; Palumbo, M. Poor maternal-neonatal outcomes in pregnant patients with confirmed SARS-CoV-2 infection: Analysis of 145 cases. Arch. Gynecol. Obstet. 2021, 303, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Bayati, A.; Kumar, R.; Francis, V.; McPherson, P.S. SARS-CoV-2 infects cells after viral entry via clathrin-mediated endocytosis. J. Biol. Chem. 2021, 296, 100306. [Google Scholar] [CrossRef]
- Debelenko, L.; Katsyv, I.; Chong, A.M.; Peruyero, L.; Szabolcs, M.; Uhlemann, A.-C. Trophoblast damage with acute and chronic intervillositis: Disruption of the placental barrier by severe acute respiratory syndrome coronavirus 2. Hum. Pathol. 2021, 109, 69–79. [Google Scholar] [CrossRef]
- Egloff, C.; Vauloup-Fellous, C.; Picone, O.; Mandelbrot, L.; Roques, P. Evidence and possible mechanisms of rare maternal-fetal transmission of SARS-CoV-2. J. Clin. Virol. 2020, 128, 104447. [Google Scholar] [CrossRef]
- Pass, R.F.; Fowler, K.B.; Boppana, S.B.; Britt, W.J.; Stagno, S. Congenital cytomegalovirus infection following first trimester maternal infection: Symptoms at birth and outcome. J. Clin.Virol. 2006, 35, 216–220. [Google Scholar] [CrossRef]
- Akpan, U.S.; Pillarisetty, L.S. Congenital Cytomegalovirus Infection; StatPearls Publishing: St. Petersburg, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541003/ (accessed on 8 April 2023).
- Fernandes, N.D.; Arya, K.; Ward, R. Congenital Herpes Simplex; StatPearls Publishing: St. Petersburg, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507897/ (accessed on 8 April 2023).
- Estrada, F.; Mahant Mahant, A.; Guerguis, S.; Sy, S.; Lu, C.; Reznik, S.E.; Herold, B. Prolonged Preterm Rupture of Membranes Associated with Neonatal Disseminated Herpes Simplex Virus Type 1 at Birth: Is There a Role for Preemptive Test and Treat Strategies in High-Risk Populations? J. Pediatr. Infect. Dis. Soc. 2023, 12, 246–247. [Google Scholar] [CrossRef]
- Allotey, J.; Chatterjee, S.; Kew, T.; Gaetano, A.; Stallings, E.; Fernández-García, S.; Yap, M.; Sheikh, J.; Lawson, H.; Coomar, D. SARS-CoV-2 positivity in offspring and timing of mother-to-child transmission: Living systematic review and meta-analysis. BMJ 2022, 376, e067696. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Blakeway, H.; Samara, A.; O’Brien, P. COVID-19 and stillbirth: Direct vs indirect effect of the pandemic. Ultrasound Obstet. Gynecol. 2022, 59, 288–295. [Google Scholar] [CrossRef]
- Edlow, G.; Castro, V.M.; Shook, L.L.; Kaimal, A.J.; Perlis, R.H. Neurodevelopmental Outcomes at 1 Year in Infants of Mothers Who Tested Positive for SARS-CoV-2 During Pregnancy. JAMA Netw. Open 2022, 5, e2215787. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Costa, S.; Sanguinetti, M.; Cattani, P.; Posteraro, B.; Marchetti, S.; Carducci, B.; Lanzone, A.; Tamburrini, E.; Vento, G. Short- and mid-term multidisciplinary outcomes of newborns exposed to SARS-CoV-2 in utero or during the perinatal period: Preliminary findings. Eur. J. Pediatr. 2022, 181, 1507–1520. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Moza, A.; Duica, F.; Antoniadis, P.; Bernad, E.S.; Lungeanu, D.; Craina, M.; Bernad, B.C.; Paul, C.; Muresan, C.; Nitu, R.; et al. Outcome of Newborns with Confirmed or Possible SARS-CoV-2 Vertical Infection—A Scoping Review. Diagnostics 2023, 13, 245. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. Preferred Reporting Items for Systematic Review and Meta-Analyses of individual participant data: The PRISMA-IPD Statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- Nuthalapaty, F.; Lu, G.; Ramin, S.; Nuthalapaty, E.; Ramin, K.D.; Ramsey, P.S. Is there a preferred gestational age threshold of viability?: A survey of maternal-fetal medicine providers. J. Matern. Fetal Neonatal Med. 2007, 20, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Lo, K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolaides, K.H.; Wright, D.; Syngelaki, A.; Wright, A.; Akolekar, R. Fetal Medicine Foundation fetal and neonatal population weight charts. Ultrasound Obstet. Gynecol. 2018, 52, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DATAtab Team. DATAtab: Online Statistics Calculator; DATAtabe.U.: Graz, Austria, 2023; Available online: https://datatab.net (accessed on 8 April 2023).
- Argueta, L.B.; Lacko, L.A.; Bram, Y.; Tada, T.; Carrau, L.; Rendeiro, A.F.; Zhang, T.; Uhl, S.; Lubor, B.C.; Chandar, V.; et al. Inflammatory responses in the placenta upon SARS-CoV-2 infection late in pregnancy. iScience 2022, 25, 104223. [Google Scholar] [CrossRef]
- Gant, T.F.; Villegas, T.P.; Summerall-Smith, J.; Watkins, B. Intrauterine fetal demise as a result of maternal COVID-19 infection in the third trimester of pregnancy: A case report. Int. J. Surg. Case Rep. 2022, 98, 107492. [Google Scholar] [CrossRef]
- Von Kohorn, I.; Stein, S.R.; Shikani, B.T.; Ramos-Benitez, M.J.; Vannella, K.M.; Hewitt, S.M.; Kleiner, D.E.; Alejo, J.C.; Burbelo, P.; Cohen, J.I.; et al. In Utero Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Pediatr. Infect. Dis. Soc. 2020, 9, 769–771. [Google Scholar] [CrossRef] [PubMed]
- Reagan-Steiner, S.; Bhatnagar, J.; Martines, R.B.; Milligan, N.S.; Gisondo, C.; Williams, F.B.; Lee, E.; Estetter, L.; Bullock, H.; Goldsmith, C.S.; et al. Detection of SARS-CoV-2 in Neonatal Autopsy Tissues and Placenta. Emerg. Infect. Dis. 2022, 28, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.-B.; Turan, S.; Wang, B.; Cojocaru, L.; Harman, C.; Logue, J.; Reece, E.A.; Frieman, M.B.; Yang, P. A SARS-CoV-2 Delta Variant Case Manifesting as Extensive Placental Infection and Fetal Transmission. Gynecol. Obstet. Investig. 2022, 87, 165–172. [Google Scholar] [CrossRef]
- Shook, L.L.; Brigida, S.; Regan, J.; Flynn, J.P.; Mohammadi, A.; Etemad, B.; Siegel, M.R.; Clapp, M.A.; Li, J.Z.; Roberts, D.J.; et al. SARS-CoV-2 Placentitis Associated with B.1.617.2 (Delta) Variant and Fetal Distress or Demise. J. Infect. Dis. 2022, 225, 754–758. [Google Scholar] [CrossRef]
- Zhang, P.; Salafia, C.; Heyman, T.; Salafia, C.; Lederman, S.; Dygulska, B. Detection of severe acute respiratory syndrome coronavirus 2 in placentas with pathology and vertical transmission. Am. J. Obstet. Gynecol. MFM 2020, 2, 100197. [Google Scholar] [CrossRef]
- Bullock, H.A.; Fuchs, E.; Martines, R.B.; Lush, M.; Bollweg, B.; Rutan, A.; Nelson, A.; Brisso, M.; Owusu-Ansah, A.; Sitzman, C. Probable vertical transmission of Alpha variant of concern (B.1.1.7) with evidence of SARS-CoV-2 infection in the syncytiotrophoblast, a case report. Front. Med. 2023, 9, 1099408. [Google Scholar] [CrossRef]
- Guan, M.; Johannesen, E.; Tang, C.Y.; Hsu, A.L.; Barnes, C.L.; Burnam, M.; McElroy, J.A.; Wan, X.-F. Intrauterine Fetal Demise in the Third Trimester of Pregnancy Associated with Mild Infection with the SARS-CoV-2 Delta Variant without Protection From Vaccination. J. Infect. Dis. 2022, 225, 748–753. [Google Scholar] [CrossRef]
- Sessa, R.; Masciullo, L.; Filardo, S.; Di Pietro, M.; Brandolino, G.; Brunelli, R.; Galoppi, P.; Terrin, G.; Viscardi, M.F.; Anastasi, E.; et al. SARS-CoV-2 vertical transmission in a twin-pregnant woman: A case report. Int. J. Infect. Dis. 2022, 125, 192–194. [Google Scholar] [CrossRef]
- Boncompagni, A.; De Agostini, M.; Lugli, L.; Ternelli, G.; Colonna, V.; Biagioni, E.; Bonasoni, M.P.; Salviato, T.; Gabrielli, L.; Falconi, M.; et al. Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn. Microorganisms 2022, 10, 1718. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Costa, S.; Sanguinetti, M.; Cattani, P.; Posteraro, B.; Marchetti, S.; Carducci, B.; Lanzone, A.; Tamburrini, E.; Vento, G.; et al. Neonatal Late Onset Infection with Severe Acute Respiratory Syndrome Coronavirus 2. Am. J. Perinatol. 2020, 37, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Facchetti, F.; Bugatti, M.; Drera, E.; Tripodo, C.; Sartori, E.; Cancila, V.; Papaccio, M.; Castellani, R.; Casola, S.; Boniotti, M.B.; et al. SARS-CoV-2 vertical transmission with adverse effects on the newborn revealed through integrated immunohistochemical, electron microscopy and molecular analyses of Placenta. EBioMedicine 2020, 59, 102951. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 vertical transmission during pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef]
- Marzollo, R.; Aversa, S.; Prefumo, F.; Saccani, B.; Perez, C.R.; Sartori, E.; Motta, M. Possible Coronavirus Disease 2019 Pandemic and Pregnancy: Vertical Transmission Is Not Excluded. Pediatr. Infect. Dis. J. 2020, 39, e261–e262. [Google Scholar] [CrossRef]
- Marinho, P.S.; da Cunha, A.J.L.A.; Chimelli, L.; Avvad-Portari, E.; Andreiuolo, F.D.M.; de Oliveira-Szejnfeld, P.S.; Mendes, M.A.; Gomes, I.C.; Souza, L.R.Q.; Guimarães, M.Z.; et al. Case Report: SARS-CoV-2 Mother-to-Child Transmission and Fetal Death Associated with Severe Placental Thromboembolism. Front. Med. 2021, 8, 677001. [Google Scholar] [CrossRef]
- Fusco, M.A.; Mantini, V.; de Souza Salmont Júnior, J.; de Carvalho Gomes, R.G.; de Oliveira Lima, A.R.; de Oliveira Clarim, H.L.; Ferreira, E.C.; de Abreu Almeida, S.S.; Salmont, C.G.; de Sousa Rizzo-Valente, V.; et al. Assessment of SARS-CoV-2 Vertical Transmission through Nested RT-PCR Testing of Neonatal Samples: Three Case Reports. J. Pediatr. Perinatol. Child Health 2022, 6, 370–376. [Google Scholar]
- Rebello, M.; Fascina, L.P.; Annicchino, G.; Pinho, J.R.R.; Yoshida, R.D.A.M.; Zacharias, R.S.B. Vertical transmission of SARS-CoV-2 from infected pregnant mother to the neonate detected by cord blood real-time polymerase chain reaction (RT-PCR). Pediatr. Res. 2021, 89, 1592–1593. [Google Scholar] [CrossRef]
- Richtmann, R.; Torloni, M.R.; Oyamada Otani, A.R.; Levi, J.E.; Crema Tobara, M.; de Almeida Silva, C.; Dias, L.; Miglioli-Galvão, L.; Martins Silva, P.; Macoto Kondo, M.; et al. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: A case series. Case Rep. Womens Health 2020, 27, e00243. [Google Scholar] [CrossRef]
- Ferreira, M.D.F.C.; Pavon, J.A.R.; Napoleão, A.C.B.; Figueiredo, G.M.D.P.; Florêncio, P.C.B.; Arantes, R.B.d.S.; Rizzo, P.S.; Carmo, M.A.M.V.; Nakazato, L.; Dutra, V.; et al. Clinical and genomic data of SARS-CoV-2 detected in maternal-fetal interface during the first wave of infection in Brazil. Microbes Infect. 2022, 24, 104949. [Google Scholar] [CrossRef]
- Bouachba, A.; Allias, F.; Nadaud, B.; Massardier, J.; Mekki, Y.; Bouscambert Duchamp, M.; Fourniere, B.D.L.; Huissoud, C.; Trecourt, A.; Collardeau-Frachon, S. Placental lesions and SARS-CoV-2 infection: Diffuse placenta damage associated to poor fetal outcome. Placenta 2021, 112, 97–104. [Google Scholar] [CrossRef]
- Lesieur, E.; Torrents, J.; Fina, F.; Zandotti, C.; Blanc, J.; Collardeau-Frachon, S.; Gazin, C.; Sirgant, D.; Mezouar, S.; OtmaniIdrissi, M.; et al. Congenital Infection of Severe Acute Respiratory Syndrome Coronavirus 2 with Intrauterine Fetal Death: A Clinicopathological Study with Molecular Analysis. Clin. Infect. Dis. 2022, 75, e1092–e1100. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Escourrou, G.; Rosenblatt, J.; Jouannic, J.M.; Laurent-Bellue, A.; De Luca, D. Factors associated with SARS-CoV-2 transplacental transmission. Am. J. Obstet. Gynecol. 2022, 227, 541–543.e11. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Choobdar, F.A.; Ghassemzadeh, M.; Attarian, M.; Abbariki, E.; Nateghian, A.; Ghanbari, B.; Hamzehi, S.S.; Hashemi, M.R.; Azarbin, Z. Transplacental Transmission of SARS-CoV-2 Infection: A Case Report from Iran. Arch. Pediatr. Infect Dis. 2021, 9, e108582. [Google Scholar] [CrossRef]
- Farhadi, R.; Mehrpisheh, S.; Ghaffari, V.; Haghshenas, M.; Ebadi, A. Clinical course, radiological findings and late outcome in preterm infant with suspected vertical transmission born to a mother with severe COVID-19 pneumonia: A case report. J. Med. Case Rep. 2021, 15, 213. [Google Scholar] [CrossRef]
- Parsa, Y.; Shokri, N.; Jahedbozorgan, T.; Naeiji, Z.; Zadehmodares, S.; Moridi, A. Possible Vertical Transmission of COVID-19 to the Newborn; a Case Report. Arch. Acad. Emerg. Med. 2021, 9, e5. [Google Scholar] [PubMed]
- Zamaniyan, M.; Ebadi, A.; Aghajanpoor, S.; Rahmani, Z.; Haghshenas, M.; Azizi, S. Preterm delivery, maternal death, and vertical transmission in a pregnant woman with COVID-19 infection. Prenat. Diagn. 2020, 40, 1759–1761. [Google Scholar] [CrossRef]
- Kienast, P.; Prayer, D.; Binder, J.; Prayer, F.; Dekan, S.; Langthaler, E.; Sigl, B.; Eichinger, S.; Perkmann-Nagele, N.; Stuempflen, I.; et al. SARS-CoV-2 variant-related abnormalities detected by prenatal MRI: A prospective case–control study. Lancet Reg. Health Eur. 2023, 26, 100587. [Google Scholar] [CrossRef] [PubMed]
- Disse, S.C.; Manuylova, T.; Adam, K.; Lechler, A.; Zant, R.; Klingel, K.; Aepinus, C.; Finkenzeller, T.; Wellmann, S.; Schneble, F. COVID-19 in 28-Week Triplets Caused by Intrauterine Transmission of SARS-CoV-2-Case Report. Front. Pediatr. 2021, 9, 812057. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, N.; Treptow, A.; Schmidt, S.; Hofmann, R.; Raumer-Engler, M.; Heubner, G.; Gröber, K. Neonatal Early-Onset Infection with SARS-CoV-2 in a Newborn Presenting with Encephalitic Symptoms. Pediatr. Infect. Dis. J. 2020, 39, e212. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Ruiz, I.; Sulleiro, E.; Serrano, B.; Fernandez-Buhigas, I.; Rodriguez-Gomez, L.; Sanchez-Nieves Fernandez, D.; Anton-Pagarolas, A.; Esperalba-Esquerra, J.; Frick, M.A.; Camba, F.; et al. Congenital infection of SARS-CoV-2 in live-born neonates: A population-based descriptive study. Clin. Microbiol. Infect. 2021, 27, 1521.e1–1521.e5. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Pontnou, M.; Navarro, A.; Camacho, J.; Crispi, F.; Alguacil-Guillén, M.; Moreno-Baró, A.; Hernandez-Losa, J.; Sesé, M.; Ramón y Cajal, S.; Ruíz, I.G.; et al. Diffuse trophoblast damage is the hallmark of SARS-CoV-2-associated fetal demise. Mod. Pathol. 2021, 34, 9. [Google Scholar] [CrossRef]
- Abadía-Cuchí, N.; Ruiz-Martínez, S.; Fabre, M.; Mateo, P.; RemachaSienes, M.; Ventura Faci, P.; Bueno Sancho, J.; Paules, C. SARS-CoV-2 congenital infection and pre-eclampsia-like syndrome in dichorionic twins: A case report and review of the literature. Int. J. Gynaecol. Obstet. 2021, 154, 370–372. [Google Scholar] [CrossRef]
- Correia, C.R.; Marçal, M.; Vieira, F.; Santos, E.; Novais, C.; Maria, A.T.; Malveiro, D.; Prior, A.R.; Aguiar, M.; Salazar, A.; et al. Congenital SARS-CoV-2 Infection in a Neonate with Severe Acute Respiratory Syndrome. Pediatr. Infect. Dis. J. 2020, 39, e439–e443. [Google Scholar] [CrossRef]
- Rodrigues, M.L.; Gasparinho, G.; Sepúlveda, F.; Matos, T. Signs suggestive of congenital SARS-CoV-2 infection with intrauterine fetal death: A case report. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 508–509. [Google Scholar] [CrossRef]
- Popescu, D.E.; Cioca, A.; Muresan, C.; Navolan, D.; Gui, A.; Pop, O.; Marcovici, T.; Ilie, C.; Craina, M.; Boia, M.A. A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death. Medicina 2021, 57, 667. [Google Scholar] [CrossRef]
- Enache, A.; Ciocan, V.; Muresan, C.O.; Cut, T.G.; Novacescu, D.; Paul, C.; Andreescu, N.; Mihailescu, A.; Raica, M.; Dumache, R. Postmortem Documentation of SARS-CoV-2 in Utero and Postpartum Transmission, through Amniotic Fluid, Placental, and Pulmonary Tissue RT-PCR. Appl. Sci. 2021, 11, 9505. [Google Scholar] [CrossRef]
- Zinserling, V.A.; Bornstein, S.R.; Narkevich, T.A.; Sukhanova, Y.V.; Semenova, N.Y.; Vashukova, M.A.; Steenblock, C. Stillborn child with diffuse SARS-CoV-2 viral infection of multiple organs. IDCases 2021, 26, e01328. [Google Scholar] [CrossRef] [PubMed]
- Sukhikh, G.; Petrova, U.; Prikhodko, A.; Starodubtseva, N.; Chingin, K.; Chen, H.; Bugrova, A.; Kononikhin, A.; Bourmenskaya, O.; Brzhozovskiy, A.; et al. Vertical Transmission of SARS-CoV-2 in Second Trimester Associated with Severe Neonatal Pathology. Viruses 2021, 13, 447. [Google Scholar] [CrossRef] [PubMed]
- Alzamora, M.C.; Paredes, T.; Caceres, D.; Webb, C.M.; Valdez, L.M.; La Rosa, M. Severe COVID-19 during Pregnancy and Possible Vertical Transmission. Am. J. Perinatol. 2020, 37, 861–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babal, P.; Krivosikova, L.; Sarvaicova, L.; Deckov, I.; Szemes, T.; Sedlackova, T.; Palkovic, M.; Kalinakova, A.; Janega, P. Intrauterine Fetal Demise After Uncomplicated COVID-19: What Can We Learn from the Case? Viruses 2021, 13, 2545. [Google Scholar] [CrossRef] [PubMed]
- Daza, M.; Corchuelo, S.; Osorio, J.; Alberto Gómez, L.; Parra, E.; Alarcón, Á.; Mercado, M. Fetal demise and SARS-CoV-2 infection during pregnancy: Histopathological and immunohistochemical findings of three cases referred to the Colombian National Institute of Health. Clin. Infect. Pract. 2023, 17, 100219. [Google Scholar] [CrossRef]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 From an Infected Mother to Her Newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [Green Version]
- Ergon, E.Y.; Akbay, S.; Aytemiz, G.; Çelik, E.C.A.; ÇalıskanPolat, A.; Umit, Z.; Paytoncu, S. A novel case of neonatal acute respiratory distress syndrome with SARS-CoV-2 infection: Potential perinatal transmission. Arch. Argent. Pediatr. 2021, 119, e531–e535. [Google Scholar] [CrossRef]
- Favre, G.; Mazzetti, S.; Gengler, C.; Bertelli, C.; Schneider, J.; Laubscher, B.; Capoccia, R.; Pakniyat, F.; Ben Jazia, I.; Eggel-Hort, B.; et al. Decreased Fetal Movements: A Sign of Placental SARS-CoV-2 Infection with Perinatal Brain Injury. Viruses 2021, 13, 2517. [Google Scholar] [CrossRef]
- Fitzgerald, B.; O’Donoghue, K.; McEntagart, N.; Gillan, J.E.; Kelehan, P.; O’Leary, J.; Downey, P.; Dean, J.; De Gascun, C.F.; Bermingham, J.; et al. Fetal Deaths in Ireland Due to SARS-CoV-2 Placentitis Caused by SARS-CoV-2 Alpha. Arch. Pathol. Lab. Med. 2022, 146, 529–537. [Google Scholar] [CrossRef]
- Karade, S.; Vishal, A.K.; Sen, S.; Bewal, N.; Gupta, R.M. Probable vertical transmission of severe acute respiratory syndrome coronavirus 2 infection from mother to neonate. Med. J. Armed Forces India 2021, 77 (Suppl. S2), S490–S493. [Google Scholar] [CrossRef]
- Kirtsman, M.; Diambomba, Y.; Poutanen, S.M.; Malinowski, A.K.; Vlachodimitropoulou, E.; Parks, W.T.; Erdman, L.; Morris, S.K.; Shah, P.S. Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. CMAJ 2020, 192, E647–E650. [Google Scholar] [CrossRef]
- Marton, T.; Hargitai, B.; Hunter, K.; Pugh, M.; Murray, P. Massive Perivillous Fibrin Deposition and Chronic Histiocytic Intervillositis a Complication of SARS-CoV-2 Infection. Pediatr. Dev. Pathol. 2021, 24, 450–454. [Google Scholar] [CrossRef]
- Morales, H.S.G.; Cortés, D.V.; Hernández, H.S.; Guiot, M.L.; Torres, G.C.R.; Camacho, F.M.R.; Montoya, G.A.; Maldonado, B.F.; Bárcenas, J.G.; López, G.G.P. Vertical transmission: Evidence of COVID-19 in a twin pregnancy. JBRA Assist. Reprod. 2022, 26, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Leow, M.Y.; Aoyama, R.; Chan, S.M. The evolution of severity of paediatric COVID-19 in Singapore: Vertical transmission and multisystem inflammatory syndrome in children. Ann. Acad. Med. Singap. 2022, 51, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.C.; Chin, L.; Choo, P.P.L.; Paramasivam, U. COVID-19 in a premature infant. BMJ Case Rep. 2021, 14, e243783. [Google Scholar] [CrossRef] [PubMed]
- Pulinx, B.; Kieffer, D.; Michiels, I.; Petermans, S.; Strybol, D.; Delvaux, S.; Baldewijns, M.; Raymaekers, M.; Cartuyvels, R.; Maurissen, W. Vertical transmission of SARS-CoV-2 infection and preterm birth. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2441–2445. [Google Scholar] [CrossRef] [PubMed]
- Sagara, A.; Yamaguchi, M.; Mikami, Y.; Motohara, T.; Ohba, T.; Kondoh, E. Maternal thrombocytopenia precedes fetal death associated with COVID-19. J. Obstet. Gynaecol. Res. 2022, 48, 1475–1479. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Baldewijns, M.; Benachi, A.; Bugatti, M.; Collins, R.R.J.; De Luca, D.; Facchetti, F.; Linn, R.L.; Marcelis, L.; Morotti, D.; et al. Chronic Histiocytic Intervillositis with Trophoblast Necrosis Is a Risk Factor Associated with Placental Infection From Coronavirus Disease 2019 (COVID-19) and Intrauterine Maternal-Fetal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Transmission in Live-Born and Stillborn Infants. Arch. Pathol. Lab. Med. 2021, 145, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Shaiba, L.A.; Hadid, A.; Altirkawi, K.A.; Bakheet, H.M.; Alherz, A.M.; Hussain, S.A.; Sobaih, B.H.; Alnemri, A.M.; Almaghrabi, R.; Ahmed, M.; et al. Case Report: Neonatal Multi-System Inflammatory Syndrome Associated with SARS-CoV-2 Exposure in Two Cases From Saudi Arabia. Front. Pediatr. 2021, 9, 652857. [Google Scholar] [CrossRef]
- Zaigham, M.; Gisselsson, D.; Sand, A.; Wikström, A.-K.; von Wowern, E.; Schwartz, D.A.; Iorizzo, L.; Nelander, M.; Blomberg, M.; Papadogiannakis, N.; et al. Clinical-pathological features in placentas of pregnancies with SARS-CoV-2 infection and adverse outcome: Case series with and without congenital transmission. BJOG 2022, 129, 1361–1374. [Google Scholar] [CrossRef]
- Chatzakis, C.; Ville, Y.; Makrydimas, G.; Dinas, K.; Zavlanos, A.; Sotiriadis, A. Timing of primary maternal cytomegalovirus infection and rates of vertical transmission and fetal consequences. Am. J. Obstet. Gynecol. 2020, 223, 870–883.e11. [Google Scholar] [CrossRef]
- Stock, S.J.; Carruthers, J.; Calvert, C.; Denny, C.; Donaghy, J.; Goulding, A.; Hopcroft, L.E.M.; Hopkins, L.; McLaughlin, T.; Pan, J.; et al. SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland. Nat. Med. 2022, 28, 3. [Google Scholar] [CrossRef]
- Maidji, E.; Percivalle, E.; Gerna, G.; Fisher, S.; Pereira, L. Transmission of human cytomegalovirus from infected uterine microvascular endothelial cells to differentiating/invasive placental cytotrophoblasts. Virology 2002, 304, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Valdés, G.; Neves, L.A.A.; Anton, L.; Corthorn, J.; Chacón, C.; Germain, A.M.; Merrill, D.C.; Ferrario, C.M.; Sarao, R.; Penninger, J.; et al. Distribution of angiotensin-(1-7) and ACE2 in human placentas of normal and pathological pregnancies. Placenta 2006, 27, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Mithal, L.B.; Otero, S.; Simons, L.M.; Hultquist, J.F.; Miller, E.S.; Ozer, E.A.; Shanes, E.D.; Goldstein, J. Low-level SARS-CoV-2 viremia coincident with COVID placentitis and stillbirth. Placenta 2022, 121, 79–81. [Google Scholar] [CrossRef]
- Myhre, L.; Prebensen, C.; Jonassen, C.M.; Berdal, J.E.; Omland, T. SARS-CoV-2 Viremia Is Associated with Inflammatory, But Not Cardiovascular Biomarkers, in Patients Hospitalized for COVID-19. J. Am. Heart Assoc. 2021, 10, e019756. [Google Scholar] [CrossRef]
- Figueiredo, C.P.; Fontes-Dantas, F.L.; da Poian, A.T.; Clarke, J.R. SARS-CoV-2-associated cytokine storm during pregnancy as a possible risk factor for neuropsychiatric disorder development in post-pandemic infants. Neuropharmacology 2021, 201, 108841. [Google Scholar] [CrossRef]
- Frøen, F. A kick from within—Fetal movement counting and the cancelled progress in antenatal care. J. Perinat. Med. 2004, 32, 13–24. [Google Scholar] [CrossRef]
- Stacey, T.; Thompson, J.M.D.; Mitchell, E.A.; Ekeroma, A.; Zuccollo, J.; McCowan, L.M.E. Maternal Perception of Fetal Activity and Late Stillbirth Risk: Findings from the Auckland Stillbirth Study. Birth 2011, 38, 311–316. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Ventura, S.J.; Osterman, M.J.; Kirmeyer, S.; Mathews, T.J.; Wilson, E.C. Births: Final Data for 2009; National Vital Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2011; Volume 60.
- Heazell, A.E.P.; Budd, J.; Li, M.; Cronin, R.; Bradford, B.; McCowan, L.M.E.; Mitchell, E.A.; Stacey, T.; Martin, B.; Roberts, D.; et al. Alterations in maternally perceived fetal movement and their association with late stillbirth: Findings from the Midland and North of England stillbirth case–control study. BMJ Open 2018, 8, e020031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morken, N.-H.; Klungsøyr, K.; Skjaerven, R. Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: A nationwide population-based cohort study. BMC Pregnancy Childbirth 2014, 14, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernad, S.I.; Bernad, E.S.; Barbat, T.; Barbu, D.; Albulescu, V. Assessment of the placental blood flow in the normally developing and growth-restricted fetus. In Proceedings of the 22nd European Congress of Perinatal Medicine, Granada, Spain, 26–29 May 2010; pp. 127–130, ISBN 978-88-6521-027-7. [Google Scholar]
- Murad, M.H.; Asi, N.; Alsawas, M.; Alahdab, F. New evidence pyramid. BMJ Evid. Based Med. 2016, 21, 125–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The WAPM (World Association of Perinatal Medicine) Working Group on COVID-19. Maternal and perinatal outcomes of pregnant women with SARS-CoV-2 infection. Ultrasound Obstet. Gynecol. 2021, 57, 232–241. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evidence of in-Utero Exposure | Evidence of Viral Persistence (24–48 h after Birth) | Type of Vertical Transmission | ||
|---|---|---|---|---|
| At Birth | <12 h after Birth | <24 h after Birth | ||
Positive RT-PCR from
| Positive RT-PCR from sterile sample | Confirmed intrauterine exposure according to the WHO classification system | ||
| Positive RT-PCR from non-sterile sample OR positive serology | Possible intrauterine exposure according to the WHO classification system | |||
Positive RT-PCR from
| - | - | Confirmed intrauterine exposure according to the Shah classification system | |
Positive RT-PCR from
| - | - | Possible intrauterine exposure according to the Shah classification system | |
| Evidence of in-Utero Exposure (<24 h) | Evidence of Viral Persistence | Type of Vertical Transmission | |
|---|---|---|---|
| (24–48 h after Birth) | 48 h–7 Days after Birth | ||
| YES. At least one sampling performed that is negative. | Positive RT-PCR from sterile sample | - | Confirmed intrapartum exposure according to the WHO classification system |
| Positive RT-PCR from non-sterile sample | Positive RT-PCR from non-sterile | ||
| NO. No sampling was performed in the first 24 h of life. | Positive RT-PCR from sterile sample | - | Possible intrapartum exposure according to WHO classification system |
| Positive RT-PCR from non-sterile sample | Positive RT-PCR from non-sterile | ||
| Fetal Tissue Sampling | Fetal Annexe Sampling | Type of Vertical Transmission |
|---|---|---|
| YES. Positive RT-PCR or ISH | - | Confirmed intrauterine exposure according to the WHO classification system |
| YES. Positive fetal swab or IHC | - | Possible intrauterine exposure according to the WHO classification system |
| NO | YES. Positive placenta (RT-PCR, ISH, swab) OR positive amniotic fluid |
| Maternal Metrics | Neonatal Outcome | p-Value (b),(c) | ||
|---|---|---|---|---|
| Livebirths | Stillbirths | |||
| Asymptomatic | Symptomatic | |||
| Variables | N = 24 | N = 24 | N = 37 | |
| Age (a),(b) | 30.78 ± 5.13 | 32 ± 5.62 | 30 ± 5.93 | 0.59 |
| Symptomatic mother at the moment of delivery (a),(c) | 13 (54.16%) | 19 (79.16%) | 21 (56.75%) | 0.18 |
| Presence of neurologic-related COVID-19 symptoms (c),(d) | 2 (8.3%) | 4 (16.66%) | 4 (10.81%) | 0.76 |
| Presence of fever (c),(d) | 9 (37.5%) | 17 (70.83%) | 21 (56.75%) | 0.13 |
| (c) Asymptomatic vs. symptomatic, p-value = 0.037 * | ||||
| Presence of respiratory symptoms (c),(d) | 10 (41.65%) | 16 (66.66%) | 14 (37.83%) | 0.81 |
| Flu-like symptoms (c),(d) | 4 (16.66%) | 3(12.5%) | 6 (16.21%) | 0.9 |
| Presence of severe pneumonia (c),(d) | 2 (8.3%) | 3 (12.5%) | 3 (8.10%) | 0.88 |
| Comorbidities (c),(d) | 10 (41.65%) | 11 (45.8%) | 10 (27.02%) | 0.26 |
| Reduced fetal movement (c),(d) | 1 (4.16%) | 3 (12.5%) | 15 (40.54%) | 0.002* |
| (c) Livebirths vs. stillbirths, p-value = 0.001 * | ||||
| Painful uterine contractions (c),(d) | 44 (16.66%) | 4 (16.66%) | 8 (21.26%) | 0.96 |
| Premature rupture of membranes (c),(d) | 11 (4.16%) | 2 (8.3%) | - | 0.5 |
| Vaginal bleeding (c),(d) | 2 (8.3%) | 1 (4.16%) | 3 (8.10%) | 0.85 |
| Transaminitis (c),(d) | 11 (4.16%) | 1 (4.16%) | 1 (2.7%) | 0.64 |
| Thrombocytopenia (c),(d) | 2 (8.3%) | 6 (25%) | 7 (18.91%) | 0.44 |
| Antibiotic treatment (c),(d) | 3 (12.5%) | 5 (20.83%) | 2 (5.40%) | 0.91 |
| Antiviral treatment (c),(d) | 2 (8.3%) | 4 (16.66%) | - | 0.28 |
| Anticoagulant treatment (c),(d) | 1 (4.16%) | 1 (4.16%) | 2 (5.40%) | 0.43 |
| Fetal lung maturation (c),(d) | 5 (20.83%) | 4 (16.66%) | - | 0.117 |
| ICU admission (c),(d) | 11 (4.16%) | 2 (8.3%) | 1 (2.7%) | 0.64 |
| Invasive mechanical ventilation (c) | - | 2 (8.3%) | - | - |
| Obstetrical Metrics | Neonatal Outcome | p-Value (b),(c) | ||
|---|---|---|---|---|
| Livebirths | Stillbirths | |||
| Asymptomatic | Symptomatic | |||
| Variable (a),(b) | N = 24 | N = 24 | N = 37 | |
| GA at T0 (a) | 33 (32–38) | 33.5 (29–35) | 31 (27–34) | 0.015 * |
| (b) Livebirths vs. stillbirths, p-value = 0.018 * | ||||
| GA at T1 (a) | 34 | 34 | 32 | 0.017 * |
| 34.83 ± 3.73 | 33.17 ± 4.13 | 31.17 ± 4.13 | ||
| (b) Livebirths vs. stillbirths, p-value = 0.016 * | ||||
| ΔT (a) | 7 (4.5–11.5) | 7.5 (4.2–11.5) | 10 (6–14) | 0.33 |
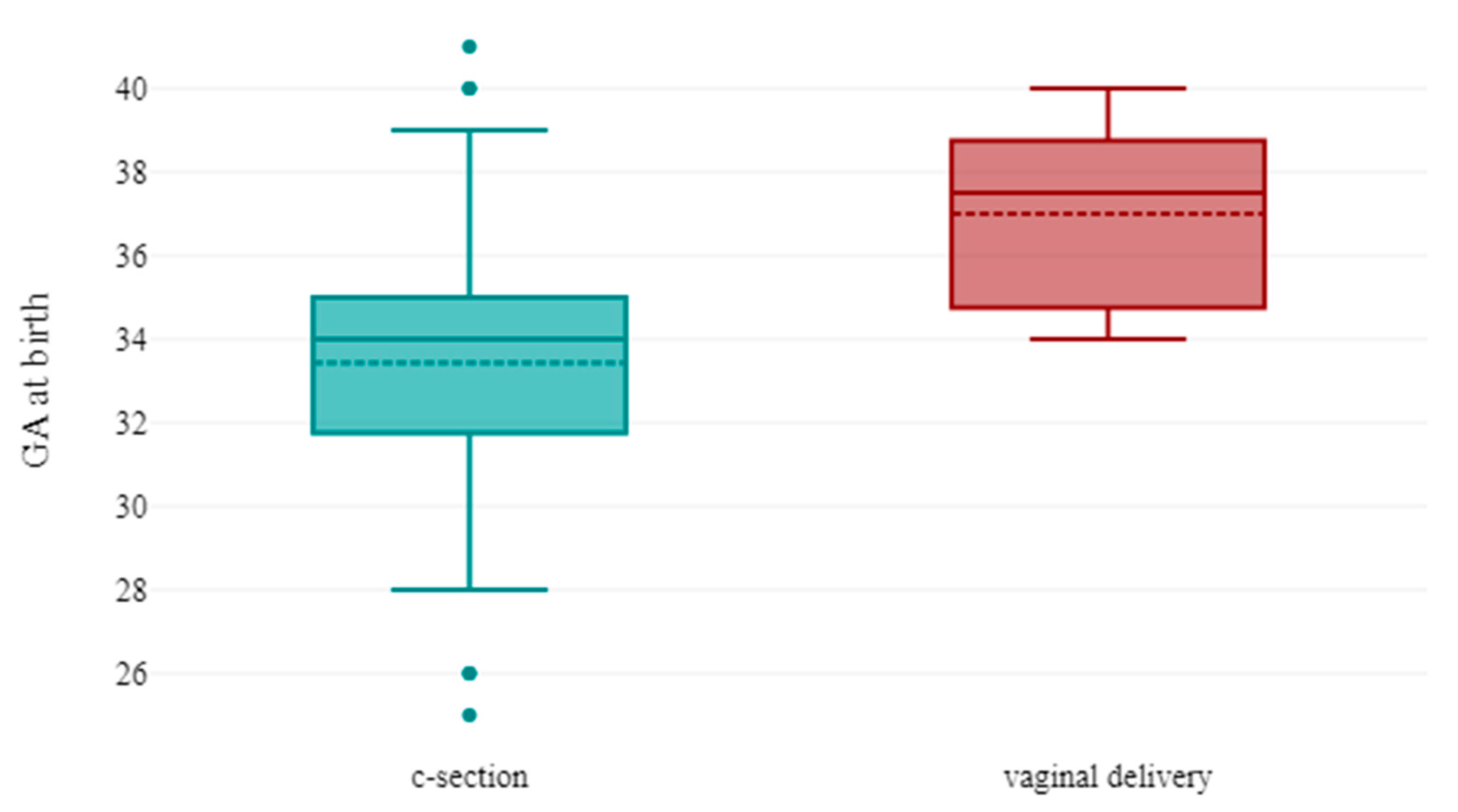
| c-section (overall) (b) | 21 (87.5%) | 19 (79.16%) | - | 0.66 |
| c-section for intrauterine fetal distress (b) | 11 (45.8%) | 8 (33.33%) | - | 0.43 |
| c-section for severe maternal COVID-19 disease (b) | - | 3 (12.5%) | - | - |
| Neonatal Metrics | Neonatal Outcome | p-Value (a),(b) | ||
|---|---|---|---|---|
| Livebirths | Stillbirths | |||
| Asymptomatic | Symptomatic | |||
| Variable (a) | N = 24 | N = 24 | N = 37 | |
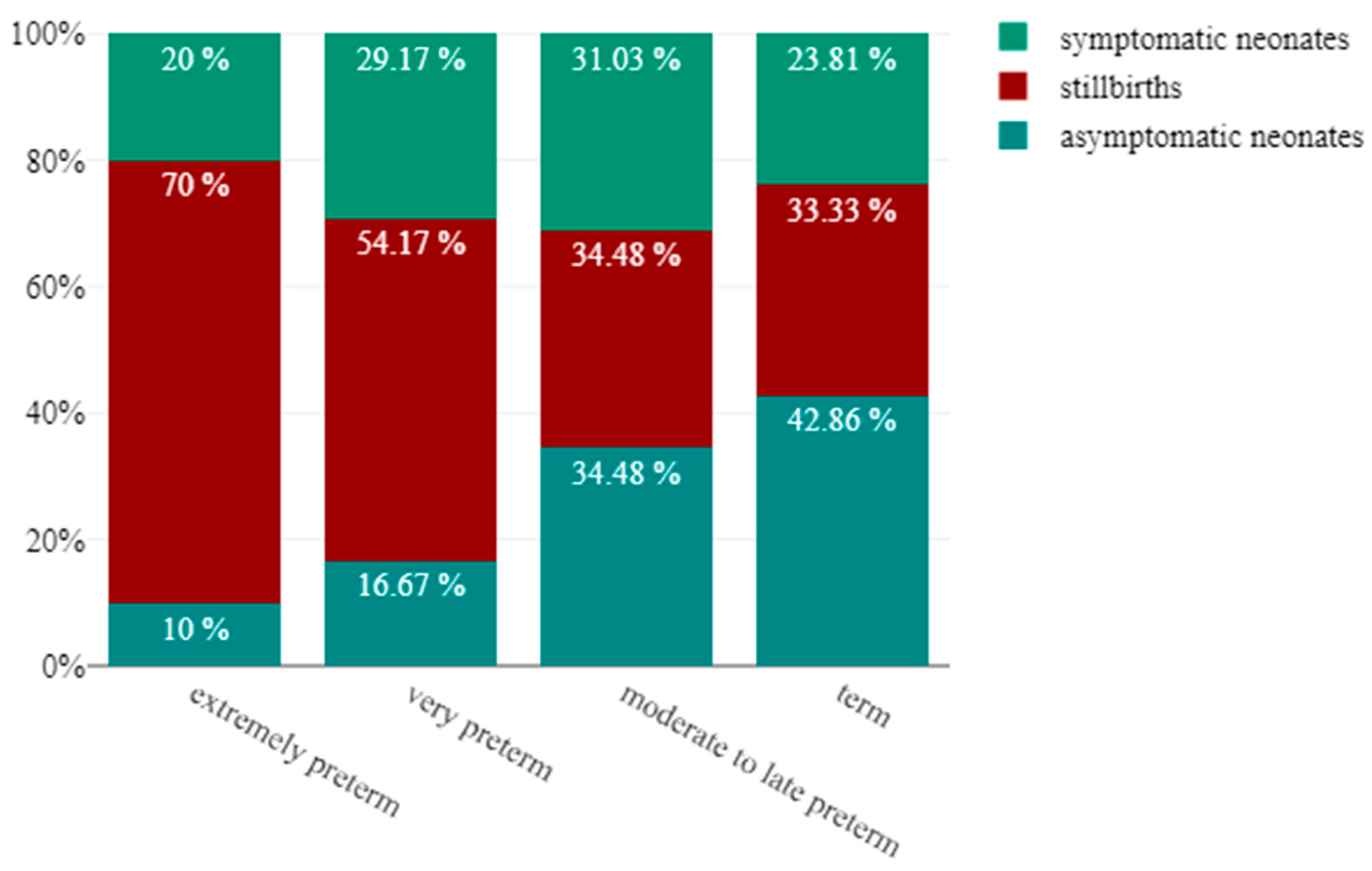
| Prematurity classification according to WHO [87] | ||||
| Preterm birth overall (a) | 15 | 18 | 30 | 0.23 |
| Extremely preterm (a) | 1 (4.17%) | 2 (8.7%) | 7 (18.92%) | 0.26 |
| Very preterm (a) | 4 (16.67%) | 7 (30.43%) | 13 (35.14%) | |
| Moderate to late preterm (a) | 10 (41.67%) | 9 (39.13%) | 10 (27.03%) | |
| Term (a) | 9 (37.5%%) | 5 (21.74%) | 7 (18.92%) | |
| 5 min Apgar Score (a) | 9 (7–10) | 8.5 (7–9) | - | 0.22 |
| Birthweight (g) (b) | 1860 (1393–2441) | 2267.5 (1575–2886) | 2109.5 (1205–2765) | 0.78 |
| Distribution according to weight centile | ||||
| IUGR (a) | 2 (8.7%) | 3 (12.5%) | 2 (5.4%) | 0.9 |
| sIUGR (a) | 5 (21.74%) | 2 (8.7%) | 2 (5.4%) | 0.2 |
| Female newborns (a) | 9 (39.13%) | 10 (41.66%) | 17 (45.97%) | 0.11 |
| Neonatal death (a) | - | 2 (8.7%) | - | - |
| Neonates with secondary adverse outcome (a) | - | 3 (12.5%) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernad, E.S.; Duica, F.; Antoniadis, P.; Moza, A.; Lungeanu, D.; Craina, M.; Bernad, B.C.; Maghet, E.; Vasilache, I.-A.; Maghiari, A.L.; et al. Maternal Fever and Reduced Fetal Movement as Predictive Risk Factors for Adverse Neonatal Outcome in Cases of Congenital SARS-CoV-2 Infection: A Meta-Analysis of Individual Participant Data from Case Reports and Case Series. Viruses 2023, 15, 1615. https://doi.org/10.3390/v15071615
Bernad ES, Duica F, Antoniadis P, Moza A, Lungeanu D, Craina M, Bernad BC, Maghet E, Vasilache I-A, Maghiari AL, et al. Maternal Fever and Reduced Fetal Movement as Predictive Risk Factors for Adverse Neonatal Outcome in Cases of Congenital SARS-CoV-2 Infection: A Meta-Analysis of Individual Participant Data from Case Reports and Case Series. Viruses. 2023; 15(7):1615. https://doi.org/10.3390/v15071615
Chicago/Turabian StyleBernad, Elena S., Florentina Duica, Panagiotis Antoniadis, Andreea Moza, Diana Lungeanu, Marius Craina, Brenda C. Bernad, Edida Maghet, Ingrid-Andrada Vasilache, Anca Laura Maghiari, and et al. 2023. "Maternal Fever and Reduced Fetal Movement as Predictive Risk Factors for Adverse Neonatal Outcome in Cases of Congenital SARS-CoV-2 Infection: A Meta-Analysis of Individual Participant Data from Case Reports and Case Series" Viruses 15, no. 7: 1615. https://doi.org/10.3390/v15071615