


SARS-CoV-2 Infection in Cities from the Southern Region of Bahia State, Brazil: Analysis of Variables Associated in Both Individual and Community Level
 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Laboratory Diagnosis of SARS-CoV-2 Infection
2.3. Data Curation
2.4. Statistical Analysis
2.4.1. Epidemiological and Geographical Indicators
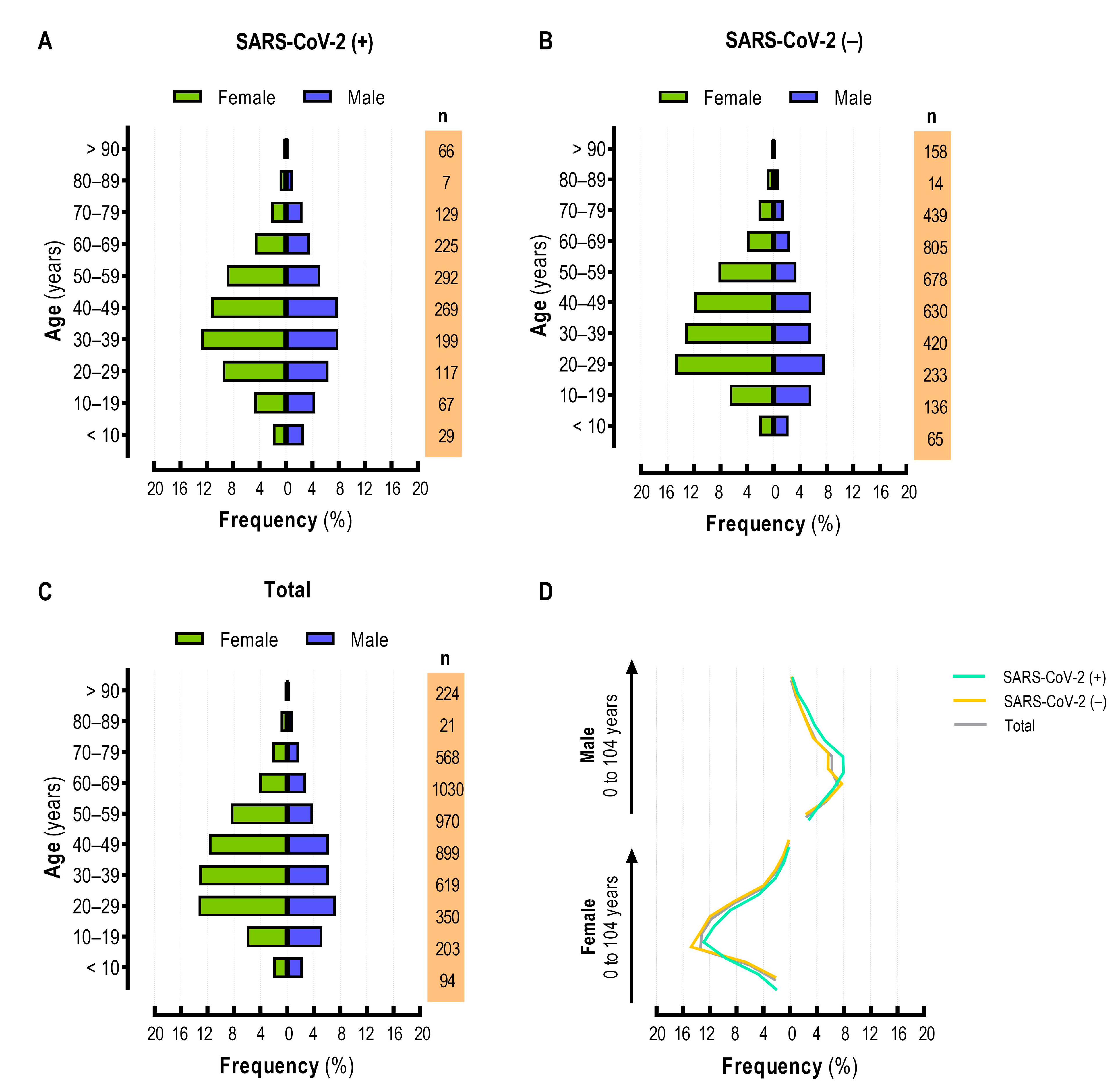
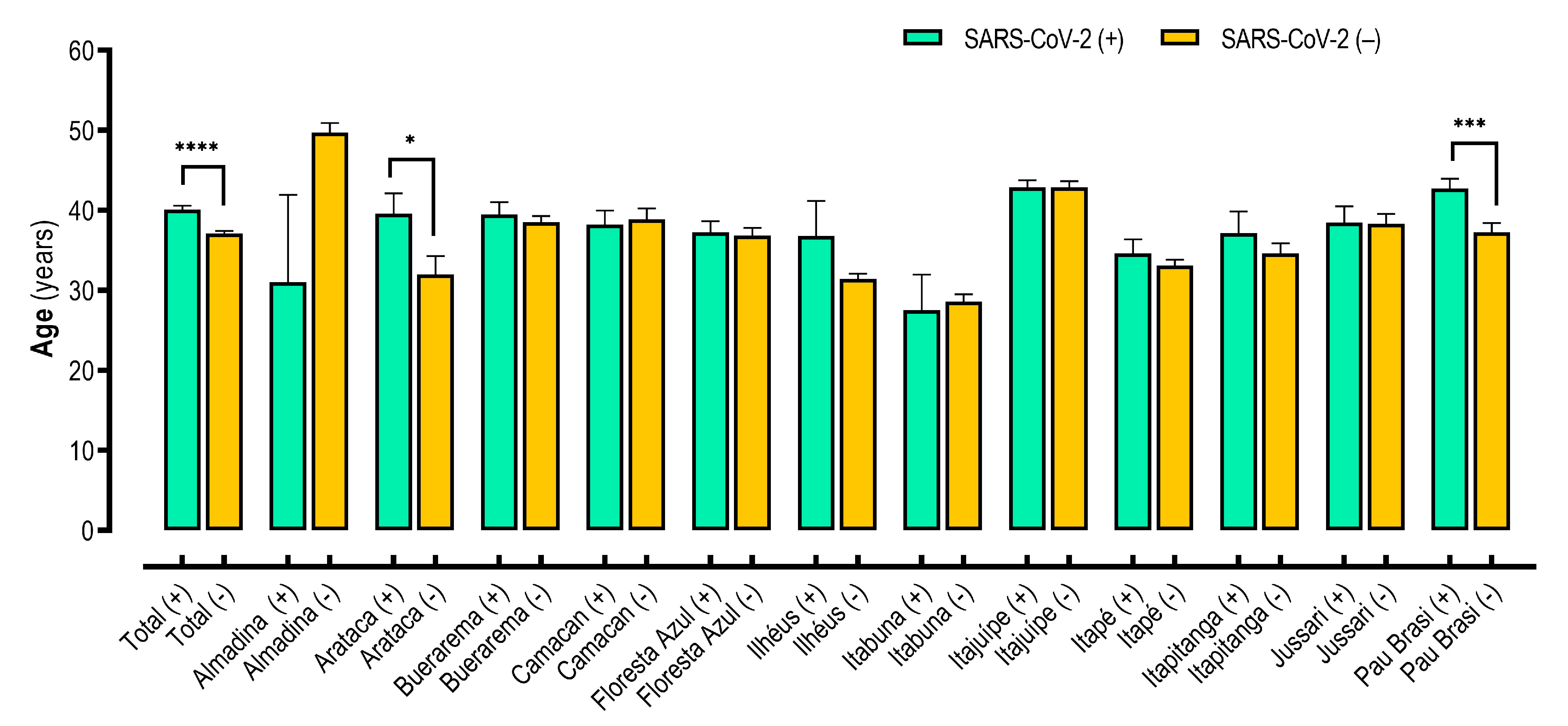
2.4.2. Population Age Pyramid Construction and Age Analysis
2.4.3. Assessment of Factors Associated with SARS-CoV-2 Infection
3. Results
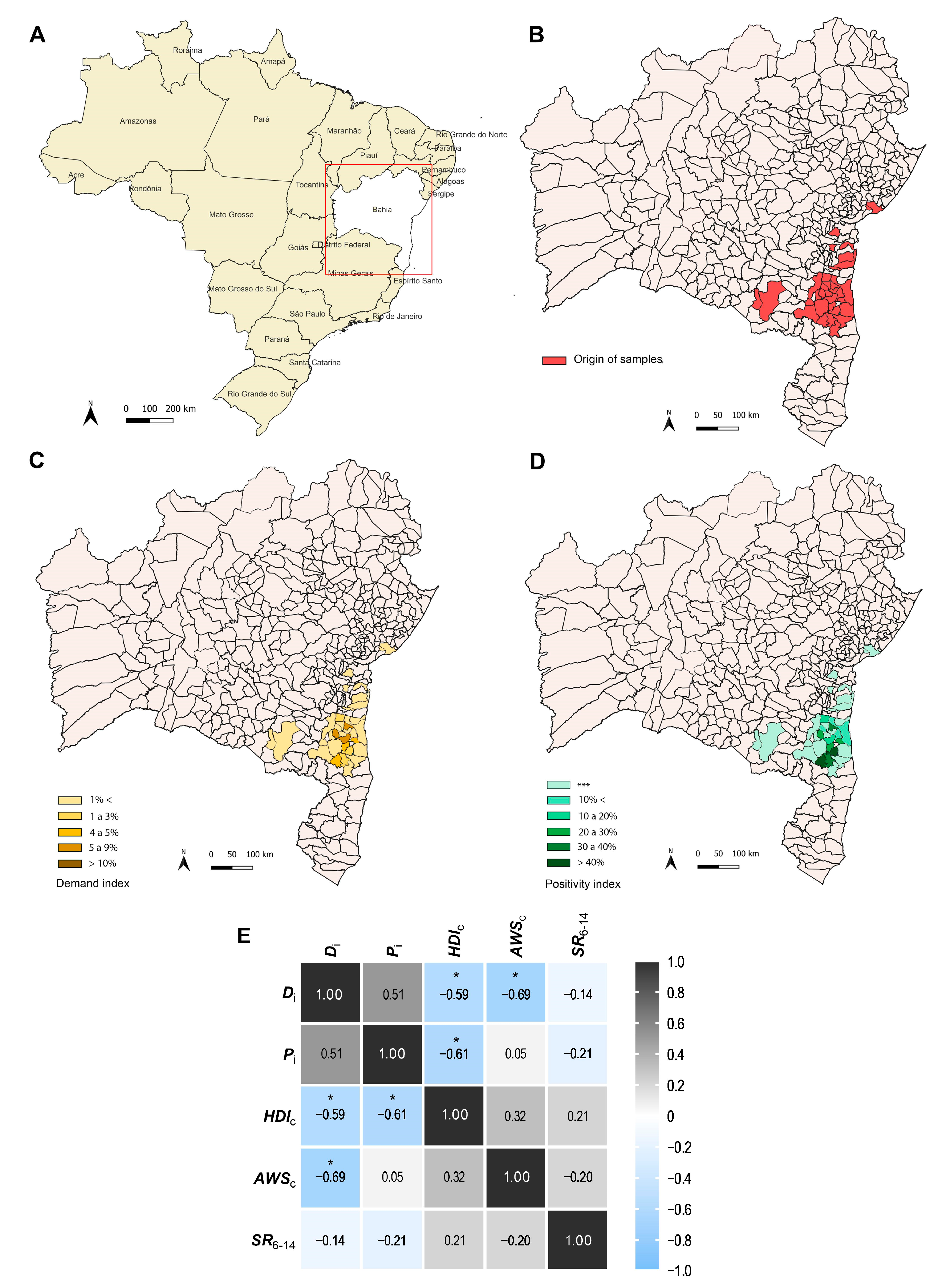
3.1. Geographical Distribution of SARS-CoV-2 Infection in Cities from the Southern Region of Bahia State, Brazil
3.2. Epidemiological Characteristics of Study Population
3.3. Comorbidities and Clinical Symptoms of SARS-CoV-2 Infection
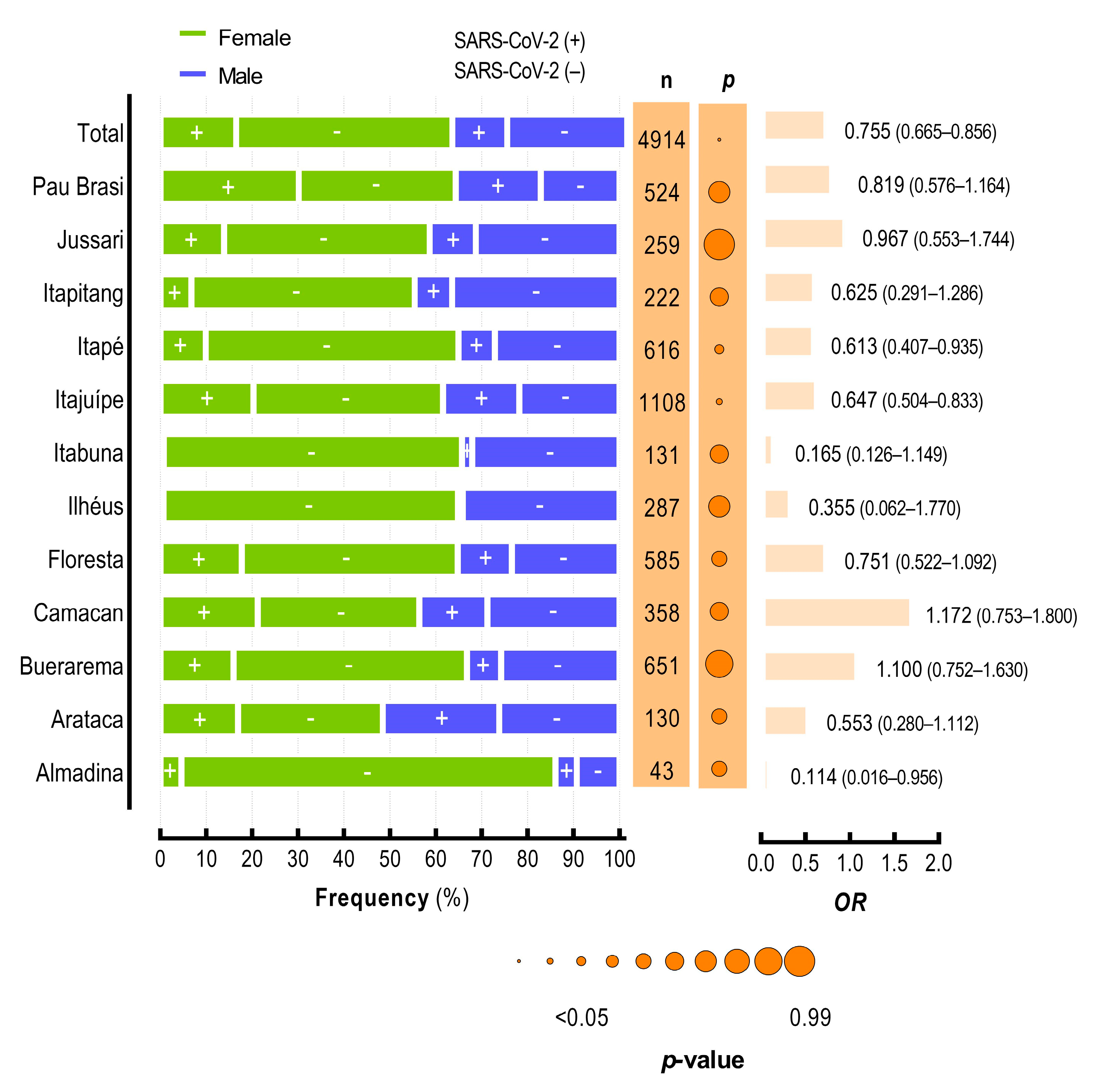
3.4. SARS-CoV-2 Infection at the Community Level in Cities from the Southern Region of Bahia State
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Organização Pan-Americana Da Saúde—PAHO. Histórico Da Pandemia De COVID-19. Available online: https://www.paho.org/pt/covid19/historico-da-pandemia-covid-19 (accessed on 21 November 2022).
- Central Integrada De Comando E Controle Da Saúde. Quadro Geral De Casos Confirmados De COVID-19 NO Estado DA Bahia. Available online: https://bi.saude.ba.gov.br/transparencia (accessed on 22 June 2022).
- SEI-Inicia Atualização Territorial Dos 26 Municípios Do Litoral Sul. Panorama Socioeconômico Territorial. Available online: https://www.sei.ba.gov.br/index.php?option=com_content&view=article&id=1084:sei-inicia-atualizacao-territorial-dos-26-municipios-do-litoral-sul&catid=10&Itemid=565 (accessed on 26 April 2023).
- Feehan, A.K.; Denstel, K.D.; Katzmarzyk, P.T.; Velasco, C.; Burton, J.H.; Price-Haywood, E.G.; Seoane, L. Community versus individual risk of SARS-CoV-2 infection in two municipalities of Louisiana, USA: An assessment of Area Deprivation Index (ADI) paired with seroprevalence data over time. PLoS ONE 2021, 16, e0260164. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, J.F.; Wadhera, R.K.; Lee, D.; Yeh, R.W.; Sommers, B.D. Community-Level Factors Associated with Racial and Ethnic Disparities in COVID-19 Rates in Massachusetts. Health Aff. 2020, 39, 1984–1992. [Google Scholar] [CrossRef]
- McLaren, J. Racial Disparity in COVID-19 Deaths: Seeking Economic Roots with Census data. Natl. Bur. Econ. Res. 2020, 21, 897–919. [Google Scholar] [CrossRef]
- Cromer, S.J.; Lakhani, C.M.; Wexler, D.J.; Burnett-Bowie, S.-A.M.; Udler, M.; Patel, C.J. Geospatial Analysis of Individual and Community-Level Socioeconomic Factors Impacting SARS-CoV-2 Prevalence and Outcomes. medRxiv 2020. [Google Scholar] [CrossRef]
- Werneck, G.L.; Carvalho, M.S. A pandemia de COVID-19 no brasil: Crônica de uma crise sanitária anunciada. Cad. De Saúde Pública 2020, 36, 1–4. [Google Scholar] [CrossRef]
- Ferreira, F.B.; Barbosa Costa, G.; Seva, A.D.P.; Albuquerque, G.R.; Mariano, A.P.M.; Sampaio Lopes, A.T.; Fehlberg, H.F.; Santos de Santana, I.T.; Dos Santos, P.R.; Santos, L.C.; et al. Characteristics and Factors Associated with SARS-CoV-2 Infections in Individuals That Attended Referral Hospitals from Southern Region of Bahia State, Brazil: A Surveillance Network Retrospective Study. Viruses 2021, 13, 2462. [Google Scholar] [CrossRef]
- COVID-19/Vaccine Tracker Taxas De Vacinação, Aprovações e Ensaios Por País. Available online: https://covid19.trackvaccines.org/country/brazil/ (accessed on 10 May 2023).
- UNA-SUS-OMS Declara Fim Da Emergência de Saúde Pública de Importância Internacional referente à COVID. Available online: https://www.unasus.gov.br/noticia/oms-declara-fim-da-emergencia-de-saude-publica-de-importancia-internacional-referente-a-covid-19 (accessed on 15 May 2023).
- Hoffmann, M.; Kleine-weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Hrichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. A entrada de células SARS-CoV-2 depende de ACE2 e TMPRSS2 e é bloqueada por um inibidor de protease clinicamente comprovado. Cell 2020, 181, 271–280.e8. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7102627/ (accessed on 15 November 2022). [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Características clínicas da doença de coronavírus 2019 na China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Cardoso, M.D.S.O.; Travassos, R.M.C.; Milhomens Filho, J.A.; Barbosa, J.V.N.; Lima, J.V.B.; Barbosa, G.d.M.R.A.; Moura, A.C.V.; Alves, T.V.L. COVID-19 e suas complicações cardiovasculares pós infecção. Rev. Ibero-Am. Humanidades Ciências E Educ. 2022, 8, 825–835. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675, Erratum in Nat. Med. 2020, 26, 1491–1493. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, B.A.; Oliveira, L.C.; Sabino, E.C.; Okay, T.S. SARS-CoV-2 and the COVID-19 disease: A mini-review on diagnostic methods. Rev. Inst. Med. Trop. S. Paulo 2020, 62, e44. [Google Scholar] [CrossRef] [PubMed]
- CDC; COVID-19 Response Team. SARS-CoV-2 B.1.1.529 (Omicron) Variant—United States, December 1–8 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1731–1734. [Google Scholar] [CrossRef] [PubMed]
- Mistry, P.; Barmania, F.; Mellet, J.; Peta, K.; Strydom, A.; Viljoen, I.M.; James, W.; Gordon, S.; Pepper, M.S. SARS-CoV-2 Variants, Vaccines, and Host Immunity. Front. Immunol. 2022, 12, 809244. [Google Scholar] [CrossRef] [PubMed]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Hirabara, S.M.; Serdan, T.D.A.; Gorjao, R.; Masi, L.N.; Pithon-Curi, T.C.; Covas, D.T.; Curi, R.; Durigon, E.L. SARS-CoV-2 Variants: Differences and Potential of Immune Evasion. Front. Cell. Infect. Microbiol. 2022, 11, 781429. [Google Scholar] [CrossRef] [PubMed]
- Huiberts, A.J.; de Gier, B.; Hoeve, C.E.; de Melker, H.E.; Hahné, S.J.M.; den Hartog, G.; Grobbee, D.E.; van de Wijgert, J.H.H.M.; van den Hof, S.; Knol, M.J. Vaccine effectiveness of primary and booster COVID-19 vaccinations against SARS-CoV-2 infection in the Netherlands from July 12, 2021 to June 6, 2022: A prospective cohort study. Int. J. Infect. Dis. 2023, 133, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths: A Systematic Review. Annu. Int. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef]
- Garay, E.; Serrano-Coll, H.; Rivero, R.; Gastelbondo, B.; Faccini-Martínez, Á.; Berrocal, J.; Pérez, A.; Badillo, M.; Martínez-Bravo, C.; Botero, Y.; et al. SARS-CoV-2 in eight municipalities of the Colombian tropics: High immunity, clinical and sociodemographic outcomes. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 139–147. [Google Scholar] [CrossRef]
- Santa-Ramírez, H.A.; Wisniak, A.; Pullen, N.; Zaballa, M.E.; Pennacchio, F.; Lorthe, E.; Dumont, R.; Baysson, H.; Guessous, I.; Stringhini, S. Socio-economic determinants of SARS-CoV-2 infection: Results from a population-based cross-sectional serosurvey in Geneva, Switzerland. Front. Public Health 2022, 10, 874252. [Google Scholar] [CrossRef]
- Rozenfeld, Y.; Beam, J.; Maier, H.; Haggerson, W.; Boudreau, K.; Carlson, J.; Medows, R. A model of disparities: Risk factors associated with COVID-19 infection. Int. J. Equity Health 2020, 19, 126. [Google Scholar] [CrossRef] [PubMed]
- Finch, W.H.; Hernández Finch, M.E. Poverty and COVID-19: Rates of incidence and deaths in the United States during the first 10 weeks of the pandemic. Front. Sociol. 2020, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Oliveira, A.M. Poverty and food insecurity may increase as the threat of COVID-19 spreads. Public Health Nutr. 2020, 23, 3236–3240. [Google Scholar] [CrossRef]
- dos Reis, D.M.; Ribeiro Gama, L.P.S.; Teixeira, I.A.; de Paula, F.G.P.; Ferreira, N.N.; Oliveira, R.F.; Álvares Macedo, D.C.L.; Ramos Bahia, M.I.; Silva e Souza, C.L. The influence of sex hormones on the immune response of COVID-19: An integrative review. Rev. Eletrôn. Acervo Saúde 2021, 13, e9073. [Google Scholar] [CrossRef]
- Lipsa, A.; Prabhu, J.S. Gender disparity in COVID-19: Role of sex steroid hormones. Asian Pac. J. Trop. Med. 2021, 14, 5–9. [Google Scholar] [PubMed]
- Han, Y.; Liu, Y.; Zhou, L.; Chen, E.; Liu, P.; Pan, X.; Lu, Y. Epidemiological Assessment of Imported Coronavirus Disease 2019 (COVID-19) Cases in the Most Affected City Outside of Hubei Province, Wenzhou, China. JAMA Netw. Open. 2020, 3, e206785. [Google Scholar] [CrossRef]
- CDC. Factors That Affect Your Risk of Getting Very Sick from COVID-19; Centers for Disease Control and Prevention. Retrieved October, 23, 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/risks-getting-very-sick.html#print (accessed on 11 May 2023).
- Lao, B.; Lima, R.C.; Karnikowski, M.G.O.; Silva, I.C.R. Comorbidities and risk factors identified in people who died from Severe Acute Respiratory Syndrome caused by COVID-19. Revisa 2021, 10, 607–626. [Google Scholar]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical Features of 69 Cases with Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Straburzyński, M.; Kuca-Warnawin, E.; Waliszewska-Prosół, M. COVID-19-related headache and innate immune response—A narrative review. Neurol. I Neurochir. Pol. 2023, 57, 43–52. [Google Scholar] [CrossRef]
- Straburzyński, M.; Nowaczewska, M.; Budrewicz, S.; Waliszewska-Prosół, M. COVID-19-related headache and sinonasal inflammation: A longitudinal study analysing the role of acute rhinosinusitis and ICHD-3 classification difficulties in SARS-CoV-2 infection. Cephalalgia 2022, 42, 218–228. [Google Scholar] [CrossRef]
- Fernandes, Q.; Inchakalody, V.P.; Merhi, M.; Mestiri, S.; Taib, N.; Moustafa Abo El-Ella, D.; Bedhiafi, T.; Raza, A.; Al-Zaidan, L.; Mohsen, M.O.; et al. Emerging COVID-19 variants and their impact on SARS-CoV-2 diagnosis, therapeutics and vaccines. Ann. Med. 2022, 54, 524–540. [Google Scholar] [CrossRef] [PubMed]
- Giovanetti, M.; Slavov, S.N.; Fonseca, V.; Wilkinson, E.; Tegally, H.; Patané, J.S.L.; Viala, V.L.; San, E.J.; Rodrigues, E.S.; Santos, E.V.; et al. Genomic epidemiology of the SARS-CoV-2 epidemic in Brazil. Nat. Microbiol. 2022, 7, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization—WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 15 May 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City † | Di | Pi | HDIc ‡ | AWSc ‡ | SR6–14 ‡ |
|---|---|---|---|---|---|
| Almadina | 0.68 | 9.30 | 0.563 | 2 | 95.30 |
| Arataca | 1.25 | 42.31 | 0.559 | 2.3 | 95.6 |
| Buerarema | 3.50 | 23.35 | 0.613 | 1.70 | 91.50 |
| Camacan | 1.14 | 36.03 | 0.581 | 2.00 | 92.50 |
| Floresta Azul | 5.49 | 29.57 | 0.557 | 1.60 | 92.80 |
| Ilhéus | 0.16 | 1.74 | 0.690 | 2.20 | 96.70 |
| Itabuna | 0.06 | 3.05 | 0.712 | 1.90 | 96.60 |
| Itajuípe | 5.26 | 36.91 | 0.559 | 1.80 | 96.30 |
| Itapé | 5.60 | 17.86 | 0.559 | 1.60 | 96.10 |
| Itapitanga | 2.17 | 14.86 | 0.571 | 1.60 | 97.00 |
| Jussari | 4.00 | 23.94 | 0.567 | 1.70 | 94.50 |
| Pau Brasil | 4.83 | 48.66 | 0.583 | 1.90 | 96.90 |
| SARS-CoV-2 N (%) | |||||
|---|---|---|---|---|---|
| Variables | Total n = 4978 (%) | SARS-CoV-2 (+) n = 1400 (%) | SARS-CoV-2 (−) n = 3578 (%) | OR (CI 95%) | p-Value |
| Age, median (IQR) | 36 (23–50) | 39 (26–52) | 35 (23–49) | - | <0.0001 a |
| Gender | |||||
| Female | 3125 (62.78) | 811 (16.29) | 2314 (46.48) | 0.752 (0.663–0.853) | <0.0001 b |
| Male | 1853 (37.22) | 589 (11.83) | 1264 (25.39) | ||
| Self-declared color/Race | |||||
| Yellow | 151 (3.99) | 39 (1.03) | 112 (2.96) | - | <0.0001 b |
| White | 382 (10.10) | 106 (2.80) | 276 (7.30) | ||
| Indigenous | 99 (2.62) | 54 (1.43) | 45 (1.19) | ||
| Brown | 2776 (73.40) | 748 (19.78) | 2028 (53.62) | ||
| Black | 374 (9.89) | 73 (1.93) | 301 (7.96) | ||
| Not related * | 1196 | 380 | 816 | ||
| Comorbidities | |||||
| Yes | 485 (9.74) | 151 (3.03) | 334 (6.71) | 1.174 (0.956–1.438) | 0.1206 b |
| No | 4493 (90.26) | 1249 (25.09) | 3244 (65.17) | ||
| Symptoms | |||||
| Yes | 3553 (71.37) | 1278 (25.67) | 2275 (45.70) | 6.000 (4.932–7.299) | <0.0001 b |
| No | 1425 (28.63) | 122 (2.45) | 1303 (26.18) | ||
| SARS-CoV-2 N (%) | |||||
|---|---|---|---|---|---|
| Variables | Total n = 4978 (%) | SARS-CoV-2 (+) n = 1400 (%) | SARS-CoV-2 (−) n = 3578 (%) | OR (CI 95%) | p-Value |
| Diabetes | |||||
| Yes | 134 (2.69) | 55 (1.10) | 79 (1.59) | 1.811 (1.278–2.553) | 0.0007 b |
| No | 4844 (97.31) | 1345 (27.02) | 3499 (70.29) | ||
| Cardiovascular disease | |||||
| Yes | 266 (5.39) | 88 (1.71) | 178 (3.58) | 1.281 (0.983–1.663) | 0.0645 b |
| No | 4712 (94.61) | 1312 (26.36) | 3400 (68.30) | ||
| Immunodeficiency | |||||
| Yes | 6 (0.12) | 0 (0.0) | 6 (0.12) | 0.000 (0.000–1.787) | 0.1942 c |
| No | 4972 (99.88) | 1400 (28.12) | 3572 (71.76) | ||
| Kidney disease | |||||
| Yes | 8 (0.16) | 5 (0.10) | 3 (0.06) | 4.271 (1.143–16.16) | 0.0444 c |
| No | 4970 (99.84) | 1395 (28.02) | 3575 (71.82) | ||
| Lung disease | |||||
| Yes | 38 (0.76) | 7 (0.14) | 31 (0.62) | 0.5750 (0.245–1.250) | 0.1817 b |
| No | 4940 (99.24) | 1393 (27.98) | 3547 (71.25) | ||
| HIV | |||||
| Yes | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2.558 (infinity) | > 0.9999 c |
| No | 4978 (100.0) | 1400 (28.1) | 3578 (71.88) | ||
| Cancer | |||||
| Yes | 2 (0.04) | 0 (0.0) | 2 (0.04) | 0.000 (0.000–5.256) | >0.9999 c |
| No | 4976 (99.96) | 1400 (28.1) | 3576 (71.84) | ||
| Other | |||||
| Yes | 130 (2.61) | 31 (0.62) | 99 (1.99) | 0.7958 (0.524–1.202) | 0.3227 b |
| No | 4848 (97.39) | 1369 (27.50) | 3479 (69.89) | ||
| SARS-CoV-2 N (%) | |||||
|---|---|---|---|---|---|
| Variables | Total n = 4978 (%) | SARS-CoV-2 (+) n = 1400 (%) | SARS-CoV-2 (−) n = 3578 (%) | OR (CI 95%) | p Value b |
| Fever | |||||
| Yes | 1583 (33.20) | 721 (15.12) | 862 (18.08) | 3.256 (2.854–3.709) | <0.0001 |
| No | 3185 (66.80) | 651 (13.65) | 2534 (53.15) | ||
| Not related * | 210 | 28 | 182 | ||
| Fatigue | |||||
| Yes | 212 (4.47) | 107 (2.26) | 105 (2.21) | 2.670 (2.015–3.507) | <0.0001 |
| No | 4532 (95.53) | 1252 (26.39) | 3280 (69.14) | ||
| Not related * | 234 | 41 | 193 | ||
| Dry cough | |||||
| Yes | 2252 (47.11) | 860 (17.99) | 1392 (29.12) | 2.399 (2.110–2.727) | <0.0001 |
| No | 2529 (52.89) | 518 (10.83) | 2011 (42.06) | ||
| Not related * | 197 | 22 | 175 | ||
| Myalgia | |||||
| Yes | 128 (2.70) | 68 (1.44) | 60 (1.26) | 2.905 (2.032–4.113) | <0.0001 |
| No | 4621 (97.30) | 1297 (27.31) | 3324 (69.99) | ||
| Not related * | 229 | 35 | 194 | ||
| Dyspnea | |||||
| Yes | 366 (7.72) | 127 (2.68) | 239 (5.04) | 1.357 (1.084–1.699) | 0.0076 |
| No | 4379 (92.28) | 1232 (25.96) | 3147 (66.32) | ||
| Not related * | 233 | 41 | 192 | ||
| Pharyngalgia | |||||
| Yes | 1577 (33.06) | 552 (11.57) | 1025 (21.49) | 1.556 (1.373–1.784) | <0.0001 |
| No | 3193 (6.94) | 817 (17.13) | 2376 (49.81) | ||
| Not related * | 208 | 31 | 177 | ||
| Diarrhea | |||||
| Yes | 213 (4.47) | 73 (1.53) | 140 (2.94) | 1.312 (0.984–1.745) | 0.0659 |
| No | 4543 (95.53) | 1292 (27.17) | 3251 (68.36) | ||
| Not related * | 213 | 35 | 187 | ||
| Headache | |||||
| Yes | 1782 (37.33) | 663 (13.89) | 1119 (23.44) | 1.900 (1.673–2.158) | <0.0001 |
| No | 2991 (62.67) | 711 (14.90) | 2280 (47.77) | ||
| Not related * | 205 | 26 | 179 | ||
| Abdominal pain | |||||
| Yes | 27 (0.57) | 8 (0.17) | 19 (0.40) | 1.050 (0.485–2.325) | 0.9084 |
| No | 4716 (99.43) | 1350 (28.46) | 3366 (70.97) | ||
| Not related * | 235 | 42 | 193 | ||
| Rhinorrhea | |||||
| Yes | 1494 (31.33) | 509 (10.67) | 985 (20.65) | 1.453 (1.282–1.658) | <0.0001 |
| No | 3275 (68.67) | 859 (18.01) | 2416 (50.66) | ||
| Not related * | 209 | 32 | 177 | ||
| Body ache | |||||
| Yes | 230 (4.84) | 107 (2.25) | 123 (2.59) | 2.264 (1.739–2.962) | <0.0001 |
| No | 4518 (95.16) | 1254 (26.41) | 3264 (68.74) | ||
| Not related * | 230 | 39 | 191 | ||
| Loss of taste | |||||
| Yes | 297 (6.26) | 197 (4.15) | 100 (2.11) | 5.574 (4.334–7.186) | <0.0001 |
| No | 4446 (93.74) | 1161 (24.48) | 3285 (69.26) | ||
| Not related * | 235 | 42 | 493 | ||
| Loss of smell | |||||
| Yes | 302 (6.36) | 208 (4.38) | 94 (1.98) | 6.327 (4.899–8.144) | <0.0001 |
| No | 4442 (93.63) | 1151 (24.26) | 3291 (69.37) | ||
| Not related * | 234 | 41 | 193 | ||
| Other | |||||
| Yes | 440 (8.84) | 145 (2.91) | 295 (5.93) | 1.286 (1.040–1.587) | 0.0182 |
| No | 4538 (91.16) | 1255 (25.21) | 3283 (68.95) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Silva, M.F.; dos Santos, U.R.; Ferreira, F.B.; Albuquerque, G.R.; Mariano, A.P.M.; Fehlberg, H.F.; Santos de Santana, Í.T.; dos Santos, P.R.; Santos, L.C.; Silva de Jesus, L.L.; et al. SARS-CoV-2 Infection in Cities from the Southern Region of Bahia State, Brazil: Analysis of Variables Associated in Both Individual and Community Level. Viruses 2023, 15, 1583. https://doi.org/10.3390/v15071583
da Silva MF, dos Santos UR, Ferreira FB, Albuquerque GR, Mariano APM, Fehlberg HF, Santos de Santana ÍT, dos Santos PR, Santos LC, Silva de Jesus LL, et al. SARS-CoV-2 Infection in Cities from the Southern Region of Bahia State, Brazil: Analysis of Variables Associated in Both Individual and Community Level. Viruses. 2023; 15(7):1583. https://doi.org/10.3390/v15071583
Chicago/Turabian Styleda Silva, Murillo Ferreira, Uener Ribeiro dos Santos, Fabrício Barbosa Ferreira, George Rego Albuquerque, Ana Paula Melo Mariano, Hllytchaikra Ferraz Fehlberg, Íris Terezinha Santos de Santana, Pérola Rodrigues dos Santos, Luciano Cardoso Santos, Laine Lopes Silva de Jesus, and et al. 2023. "SARS-CoV-2 Infection in Cities from the Southern Region of Bahia State, Brazil: Analysis of Variables Associated in Both Individual and Community Level" Viruses 15, no. 7: 1583. https://doi.org/10.3390/v15071583