
Explainable COVID-19 Detection Based on Chest X-rays Using an End-to-End RegNet Architecture
 , ,
, ,
Abstract
:1. Introduction
2. Related Work
- 1.
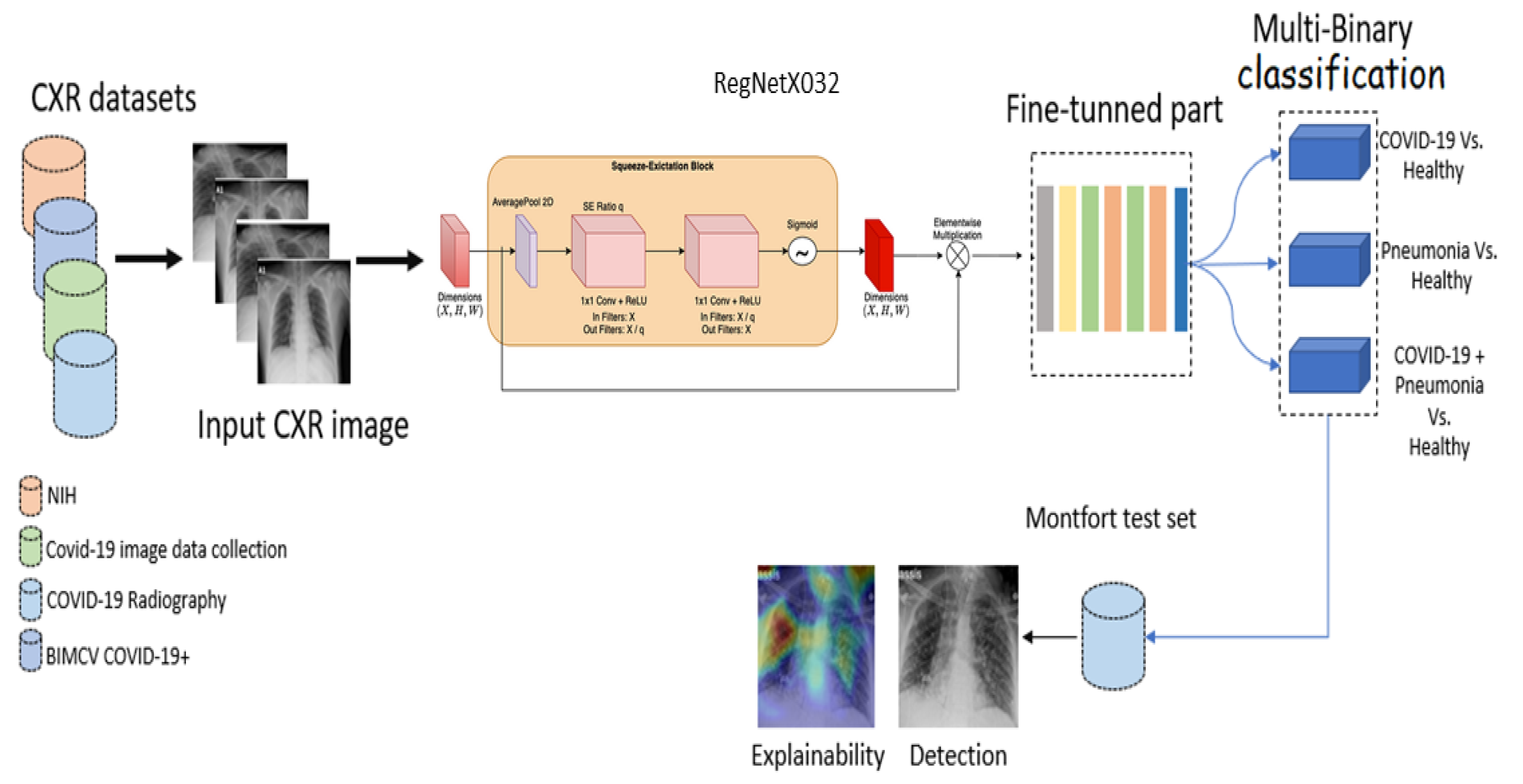
- A state-of-the-art pre-trained CNN model called RegNetX032 was fine-tuned for multi-binary classification (COVID-19 vs. normal, COVID-19 + pneumonia vs. normal, and pneumonia vs. normal. Such a model has not yet been proposed in a medical imaging classification study. Our study investigated the performance of this fine-tuned RegNet model for COVID-19 detection.
- 2.
- We used various datasets, which differed in terms of resolution quality, to validate the performance of the model and its degree of generalization.
- 3.
- We tested the performance and the degree of generalization of the model using a private dataset.
- 4.
- An explainability model was integrated to localize the signs of the disease and provide decision support.The paper is structured as follows: Section 1 introduces the COVID-19 pandemic, and Section 2 presents related work. Section 3 discusses the methods and presents the proposed deep learning model and the datasets used in this study. Section 4 presents the experimental results. Section 5 describes the model’s explainability. Section 6 discusses the model’s limitations. Section 7 presents a discussion and conclusions.
3. Methods
3.1. Deep Learning Model
3.2. Deriving the RegNet Model from Network Design Spaces
3.3. The RegNet Design Space
3.4. Patients and Datasets
3.4.1. NIH Dataset
3.4.2. COVID-19 Image Data Collection
3.4.3. COVID-19 Radiography
3.4.4. BIMCV COVID19+
3.4.5. Montfort Dataset
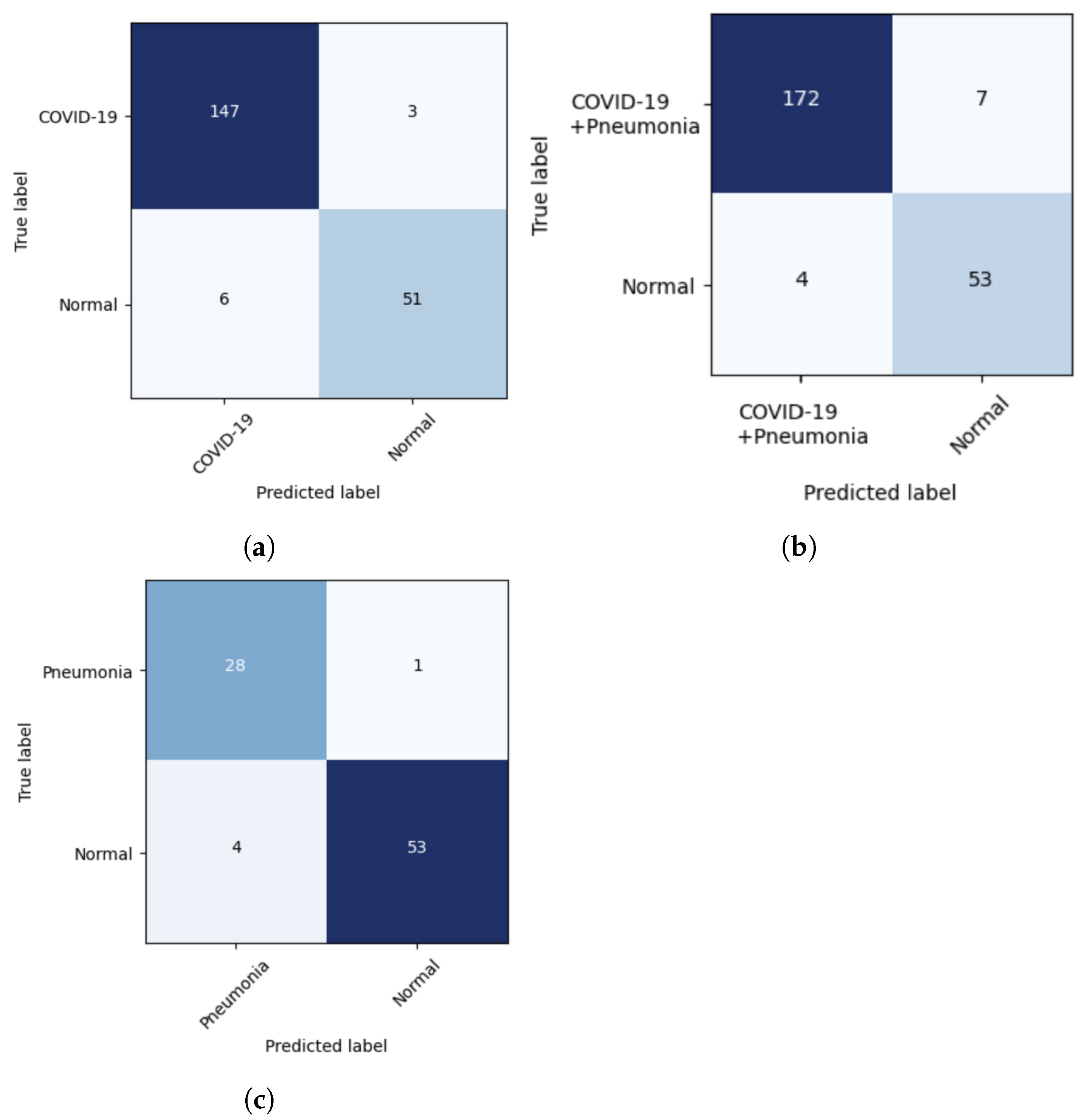
4. Results
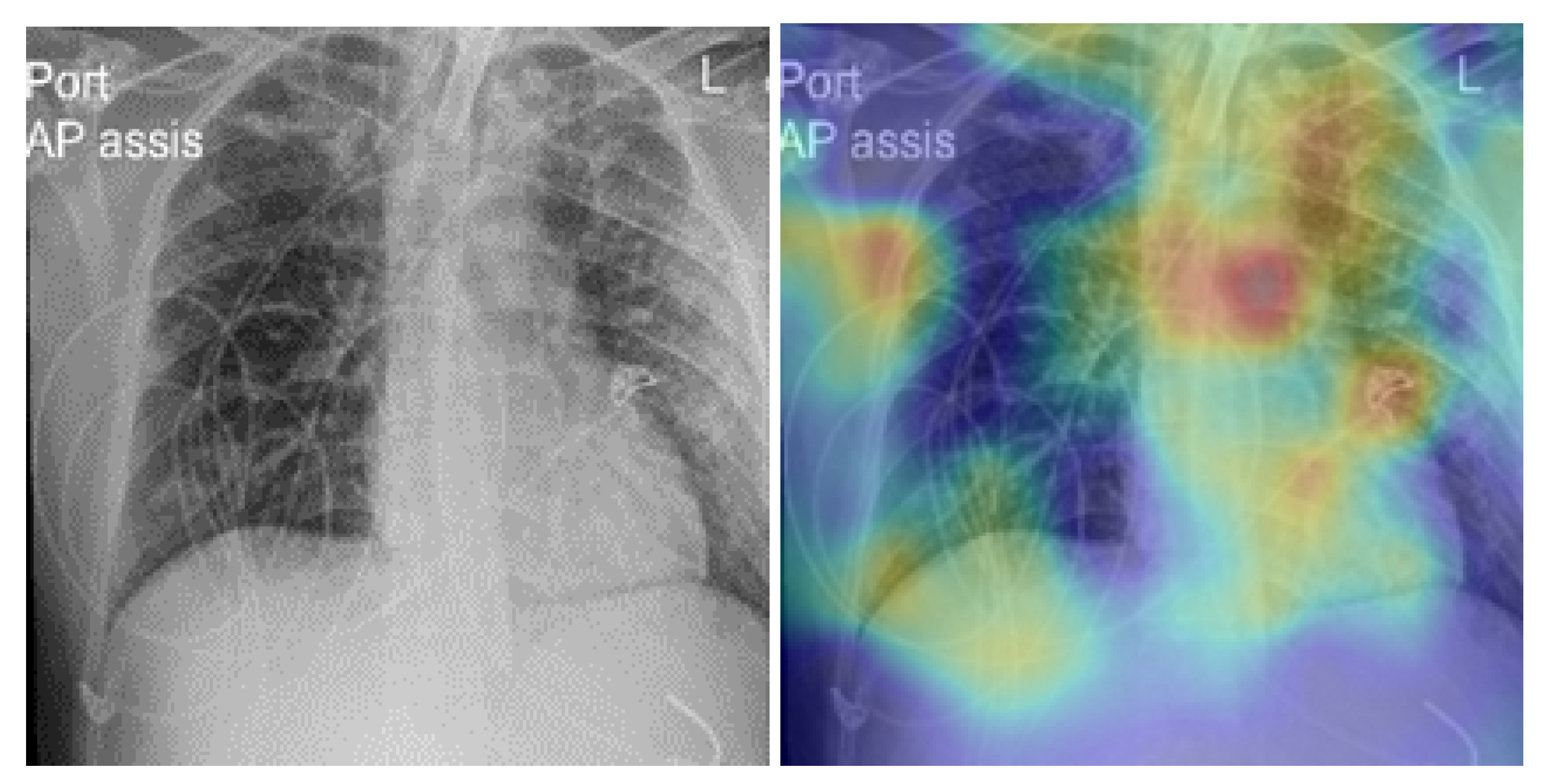
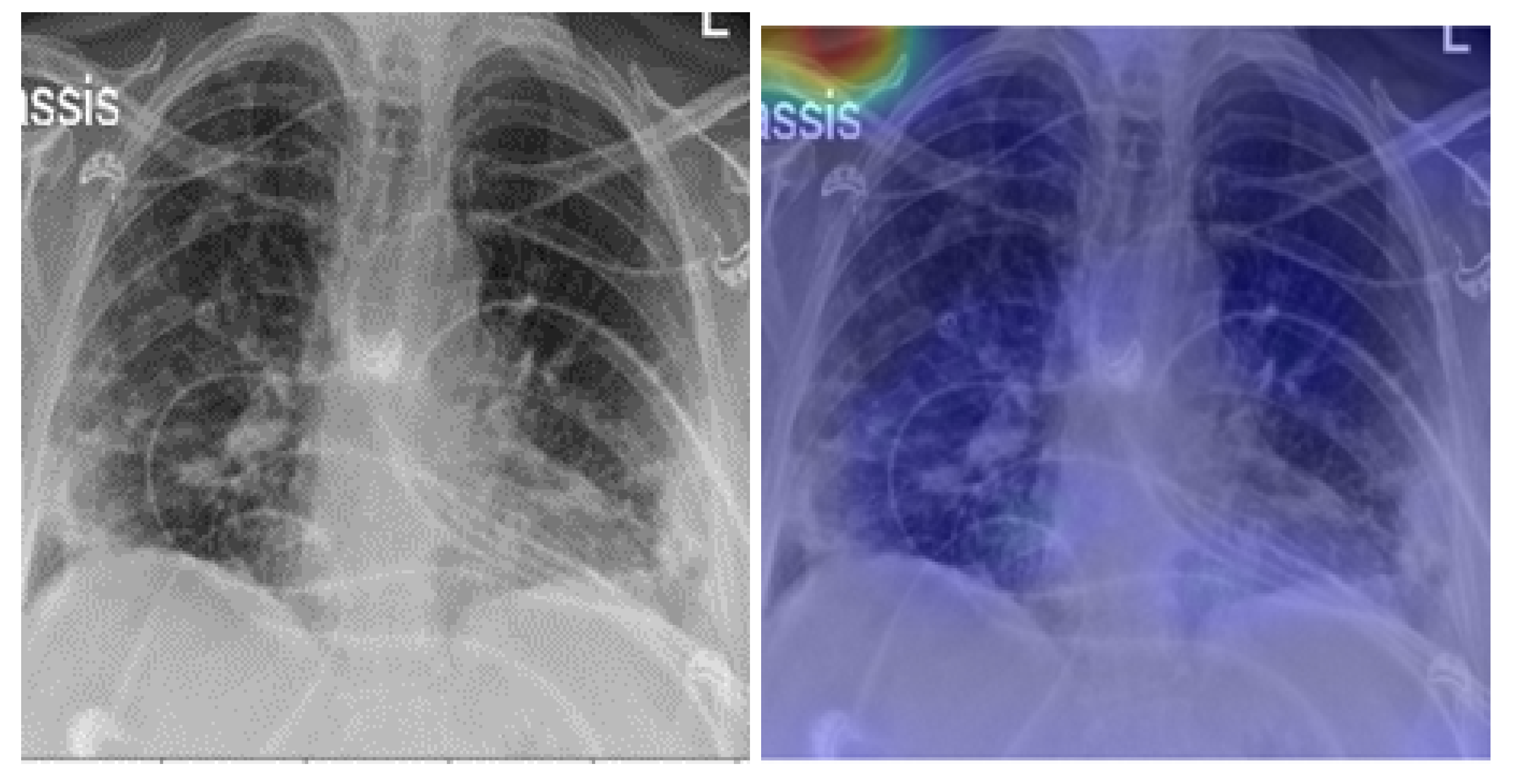
5. Model Explainability
6. Model Limitations
7. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 April 2023).
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Yao, D.; Shi, Y.; Song, Z. Computer-aided detection in chest radiography based on artificial intelligence: A survey. Biomed. Eng. Online 2018, 17, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodwick, G.S.; Keats, T.E.; Dorst, J.P. The coding of roentgen images for computer analysis as applied to lung cancer. Radiology 1963, 81, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Zakirov, A.; Kuleev, R.; Timoshenko, A.; Vladimirov, A. Advanced approaches to computer-aided detection of thoracic diseases on chest X-rays. Appl. Math. Sci. 2015, 9, 4361–4369. [Google Scholar] [CrossRef]
- Yadessa, A.G.; Salau, A.O. Low cost sensor based hand washing solution for COVID-19 prevention. In Proceedings of the International Conference on Innovation and Intelligence for Informatics, Computing, and Technologies (3ICT), Zallaq, Bahrain, 29–30 September 2021; pp. 93–97. [Google Scholar]
- Natnael, T.; Alemnew, Y.; Berihun, G.; Abebe, M.; Andualem, A.; Ademe, S.; Tegegne, B.; Adane, M. Facemask wearing to prevent COVID-19 transmission and associated factors among taxi drivers in Dessie City and Kombolcha Town, Ethiopia. PLoS ONE 2021, 16, e0247954. [Google Scholar] [CrossRef]
- Carvalho, K.; Vicente, J.P.; Jakovljevic, M.; Teixeira, J.P.R. Analysis and forecasting incidence, intensive care unit admissions, and projected mortality attributable to COVID-19 in Portugal, the UK, Germany, Italy, and France: Predictions for 4 weeks ahead. Bioengineering 2021, 8, 84. [Google Scholar] [CrossRef]
- Reshetnikov, V.; Mitrokhin, O.; Shepetovskaya, N.; Belova, E.; Jakovljevic, M. Organizational measures aiming to combat COVID-19 in the Russian Federation: The first experience. Expert Rev. Pharmacoeconomics Outcomes Res. 2020, 20, 571–576. [Google Scholar] [CrossRef]
- Grima, S.; Rupeika-Apoga, R.; Kizilkaya, M.; Romānova, I.; Dalli Gonzi, R.; Jakovljevic, M. A proactive approach to identify the exposure risk to COVID-19: Validation of the pandemic risk exposure measurement (PREM) model using real-world data. Risk Manag. Healthc. Policy 2021, 14, 4775–4787. [Google Scholar] [CrossRef]
- Chetoui, M.; Akhloufi, M.A. Explainable vision transformers and radiomics for COVID-19 detection in chest X-rays. J. Clin. Med. 2022, 11, 3013. [Google Scholar] [CrossRef]
- Akinyelu, A.A.; Blignaut, P. COVID-19 diagnosis using deep learning neural networks applied to CT images. Front. Artif. Intell. 2022, 5, 919672. [Google Scholar] [CrossRef]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning transferable architectures for scalable image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 8697–8710. [Google Scholar]
- Mondal, M.R.H.; Bharati, S.; Podder, P. CO-IRv2: Optimized InceptionResNetV2 for COVID-19 detection from chest CT images. PLoS ONE 2021, 16, e0259179. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Khalil, M.I.; Rehman, S.U.; Alhajlah, M.; Mahmood, A.; Karamat, T.; Haneef, M.; Alhajlah, A. Deep-COVID: Detection and Analysis of COVID-19 Outcomes Using Deep Learning. Electronics 2022, 11, 3836. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning—PMLR, Boca Raton, FL, USA, 16–19 December 2019; pp. 6105–6114. [Google Scholar]
- Hasan, M.K.; Alam, M.A.; Dahal, L.; Roy, S.; Wahid, S.R.; Elahi, M.T.E.; Martí, R.; Khanal, B. Challenges of deep learning methods for COVID-19 detection using public datasets. Informatics Med. Unlocked 2022, 30, 100945. [Google Scholar] [CrossRef]
- Abdul Gafoor, S.; Sampathila, N.; K S, S. Deep learning model for detection of COVID-19 utilizing the chest X-ray images. Cogent Eng. 2022, 9, 2079221. [Google Scholar] [CrossRef]
- Sahlol, A.T.; Yousri, D.; Ewees, A.A.; Al-Qaness, M.A.; Damasevicius, R.; Elaziz, M.A. COVID-19 image classification using deep features and fractional-order marine predators algorithm. Sci. Rep. 2020, 10, 15364. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. Chexnet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Cohen, J.P.; Morrison, P.; Dao, L.; Roth, K.; Duong, T.Q.; Ghassemi, M. COVID-19 Image Data Collection: Prospective Predictions Are the Future. arXiv 2020, arXiv:2006.11988. [Google Scholar] [CrossRef]
- Chowdhury, M.E.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Mahbub, Z.B.; Islam, K.R.; Khan, M.S.; Iqbal, A.; Al Emadi, N.; et al. Can AI help in screening viral and COVID-19 pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]
- Kumar, S.; Shastri, S.; Mahajan, S.; Singh, K.; Gupta, S.; Rani, R.; Mohan, N.; Mansotra, V. LiteCovidNet: A lightweight deep neural network model for detection of COVID-19 using X-ray images. Int. J. Imaging Syst. Technol. 2022, 32, 1464–1480. [Google Scholar] [CrossRef]
- Muhammad, W.; Bhutto, Z.; Shah, S.A.R.; Shah, J.; Shaikh, M.H.; Hussain, A.; Thaheem, I.; Ali, S. Deep transfer learning CNN based approach for COVID-19 detection. Int. J. Adv. Appl. Sci. 2022, 9, 44–52. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Ayalew, A.M.; Salau, A.O.; Abeje, B.T.; Enyew, B. Detection and classification of COVID-19 disease from X-ray images using convolutional neural networks and histogram of oriented gradients. Biomed. Signal Process. Control 2022, 74, 103530. [Google Scholar] [CrossRef]
- Ghose, P.; Alavi, M.; Tabassum, M.; Uddin, M.A.; Biswas, M.; Mahbub, K.; Gaur, L.; Mallik, S.; Zhao, Z. Detecting COVID-19 infection status from chest X-ray and CT scan via single transfer learning-driven approach. Front. Genet. 2022, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Indumathi, N.; Shanmuga Eswari, M.; Salau, A.O.; Ramalakshmi, R.; Revathy, R. Prediction of COVID-19 outbreak with current substantiation using machine learning algorithms. In Intelligent Interactive Multimedia Systems for E-Healthcare Applications; Springer: Berlin/Heidelberg, Germany, 2022; pp. 171–190. [Google Scholar]
- Salau, A.O. Detection of corona virus disease using a novel machine learning approach. In Proceedings of the International Conference on Decision Aid Sciences and Application (DASA), Sakheer, Bahrain, 7–8 December 2021; pp. 587–590. [Google Scholar]
- Frimpong, S.A.; Salau, A.; Quansah, A.; Hanson, I.; Abubakar, R.; Yeboah, V. Innovative IoT-Based Wristlet for Early COVID-19 Detection and Monitoring Among Students. Math. Model. Eng. Probl. 2022, 9, 1557–1564. [Google Scholar] [CrossRef]
- Liu, S.; Cai, T.; Tang, X.; Zhang, Y.; Wang, C. COVID-19 diagnosis via chest X-ray image classification based on multiscale class residual attention. Comput. Biol. Med. 2022, 149, 106065. [Google Scholar] [CrossRef]
- Chouat, I.; Echtioui, A.; Khemakhem, R.; Zouch, W.; Ghorbel, M.; Hamida, A.B. COVID-19 detection in CT and CXR images using deep learning models. Biogerontology 2022, 23, 65–84. [Google Scholar] [CrossRef]
- Deriba, F.G.; Salau, A.O.; Tefera, B.T.; Demilie, W.B. Artificial Intelligence Assisted Decision Making in Predicting COVID-19 Patient’s Path. J. Pharm. Negat. Results 2023, 14, 1250–1255. [Google Scholar]
- Wubineh, B.Z.; Salau, A.O.; Braide, S.L. Knowledge Based Expert System for Diagnosis of COVID-19. J. Pharm. Negat. Results 2023, 14, 1242–1249. [Google Scholar]
- Italiana, C.R. COVID-19 Database. 2020. Available online: https://sirm.org/COVID-19/ (accessed on 1 April 2023).
- Radosavovic, I.; Kosaraju, R.P.; Girshick, R.; He, K.; Dollár, P. Designing network design spaces. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020; pp. 10428–10436. [Google Scholar]
- imageNet. Large Scale Visual Recognition Challenge (ILSVRC). 2012. Available online: http://image-net.org/challenges/LSVRC/ (accessed on 1 April 2023).
- Sandler, M.; Howard, A.G.; Zhu, M.; Zhmoginov, A.; Chen, L. Inverted Residuals and Linear Bottlenecks: Mobile Networks for Classification, Detection and Segmentation. arXiv 2018, arXiv:1801.04381. [Google Scholar]
- Tan, M.; Le, Q.V. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. arXiv 2019, arXiv:1905.11946. [Google Scholar]
- Malhotra, A.; Mittal, S.; Majumdar, P.; Chhabra, S.; Thakral, K.; Vatsa, M.; Singh, R.; Chaudhury, S.; Pudrod, A.; Agrawal, A. Multi-task driven explainable diagnosis of COVID-19 using chest X-ray images. Pattern Recognit. 2022, 122, 108243. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T. COVID-19 Radiography Database. 2020. Available online: https://www.kaggle.com/tawsifurrahman/covid19-radiography-database (accessed on 1 April 2023).
- BIMCV Valencia Region; Pertusa, A.; de la Iglesia Vaya, M. BIMCV-COVID19+; OSF: Frankfurt, Germany, 2020. [Google Scholar] [CrossRef]
- Chollet, F. Keras. 2015. Available online: https://keras.io (accessed on 1 April 2023).
- NVIDIA. 2080 Ti. 2018. Available online: https://www.nvidia.com/en-us/geforce/graphics-cards/rtx-2080 (accessed on 1 April 2023).
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Chetoui, M.; Akhloufi, M.A. Deep Efficient Neural Networks for Explainable COVID-19 Detection on CXR Images. In Advances and Trends in Artificial Intelligence—Artificial Intelligence Practices, Proceedings of the 34th International Conference on Industrial, Engineering and Other Applications of Applied Intelligent Systems, IEA/AIE 2021, Kuala Lumpur, Malaysia, 26–29 July 2021; Springer: Berlin/Heidelberg, Germany, 2021; pp. 329–340. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario 1 | Scenario 2 | Scenario 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ACC | SN | SP | ACC | SN | SP | ACC | SN | SP | |
| Val (merged sets) | 98.6% | 98.0% | 96.0% | 97.3% | 97.0% | 96.0% | 95.0% | 95.0% | 95.0% |
| Test (Montfort) | 96.0% | 98.0% | 90.0% | 95.3% | 96.0% | 93.0% | 96.4% | 97.0% | 93.0% |
| Study | Method | ACC | AUC | SN | SP | COVID-19 Images | Explainibility |
|---|---|---|---|---|---|---|---|
| [30] | CNN and HOG | 99.6% | - | - | - | 3000 with data augmentation | No |
| [31] | CNN | 99.5% | 99.2% | 99.5% | 99.5% | 1626 | No |
| [32] | SVM | 98.5% | - | 88% | 87.2% | 250 | No |
| [35] | CNN | 97.71% | - | 96.76% | 96.56% | 3338 | Yes |
| [36] | 4 CNN | 98.0% | - | - | - | 500 | No |
| [17] | CNN | 97.0% | - | - | - | 217 | No |
| [26] | CNN | 94.5% | - | - | - | 203 | No |
| Our model | CNN | 98.6% 96.0% | 98.0% 99.1% | 98.0% 98.0% | 96.0% 96.0% | 4148 150 | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chetoui, M.; Akhloufi, M.A.; Bouattane, E.M.; Abdulnour, J.; Roux, S.; Bernard, C.D. Explainable COVID-19 Detection Based on Chest X-rays Using an End-to-End RegNet Architecture. Viruses 2023, 15, 1327. https://doi.org/10.3390/v15061327
Chetoui M, Akhloufi MA, Bouattane EM, Abdulnour J, Roux S, Bernard CD. Explainable COVID-19 Detection Based on Chest X-rays Using an End-to-End RegNet Architecture. Viruses. 2023; 15(6):1327. https://doi.org/10.3390/v15061327
Chicago/Turabian StyleChetoui, Mohamed, Moulay A. Akhloufi, El Mostafa Bouattane, Joseph Abdulnour, Stephane Roux, and Chantal D’Aoust Bernard. 2023. "Explainable COVID-19 Detection Based on Chest X-rays Using an End-to-End RegNet Architecture" Viruses 15, no. 6: 1327. https://doi.org/10.3390/v15061327