
Efficacy of Remdesivir and Neutralizing Monoclonal Antibodies in Monotherapy or Combination Therapy in Reducing the Risk of Disease Progression in Elderly or Immunocompromised Hosts Hospitalized for COVID-19: A Single Center Retrospective Study
 , ,
, ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Patient Population
2.2. Treatment Exposure
2.3. Study Outcomes
2.4. Other Definitions
- Asymptomatic or presymptomatic infection: individuals who test positive for SARS-CoV-2 using a virologic test (i.e., a nucleic acid amplification test [NAAT] or an antigen test) but have no symptoms consistent with COVID-19;
- Mild illness: individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, or loss of taste and smell) but do not have shortness of breath, dyspnea, or abnormal chest imaging;
- Moderate illness: individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have an oxygen saturation measured by pulse oximetry (SpO2) ≥ 94% in room air at sea level;
- Severe illness: individuals who have SpO2 < 94% in room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mm Hg, a respiratory rate >30 breaths/min, or lung infiltrates >50%;
- Critical illness: individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.
2.5. Statistical Analysis
3. Results
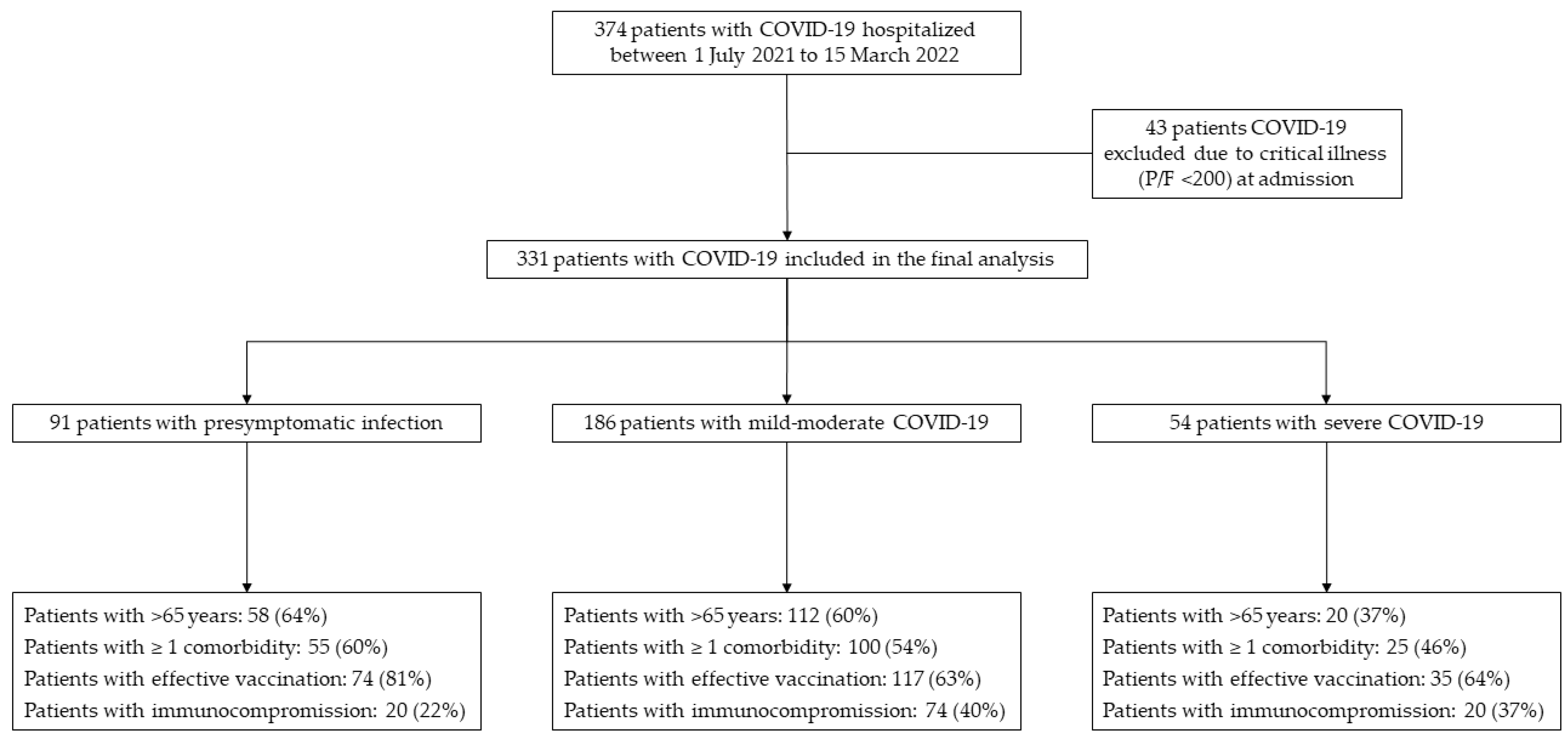
3.1. Study Population and Outcome Distribution
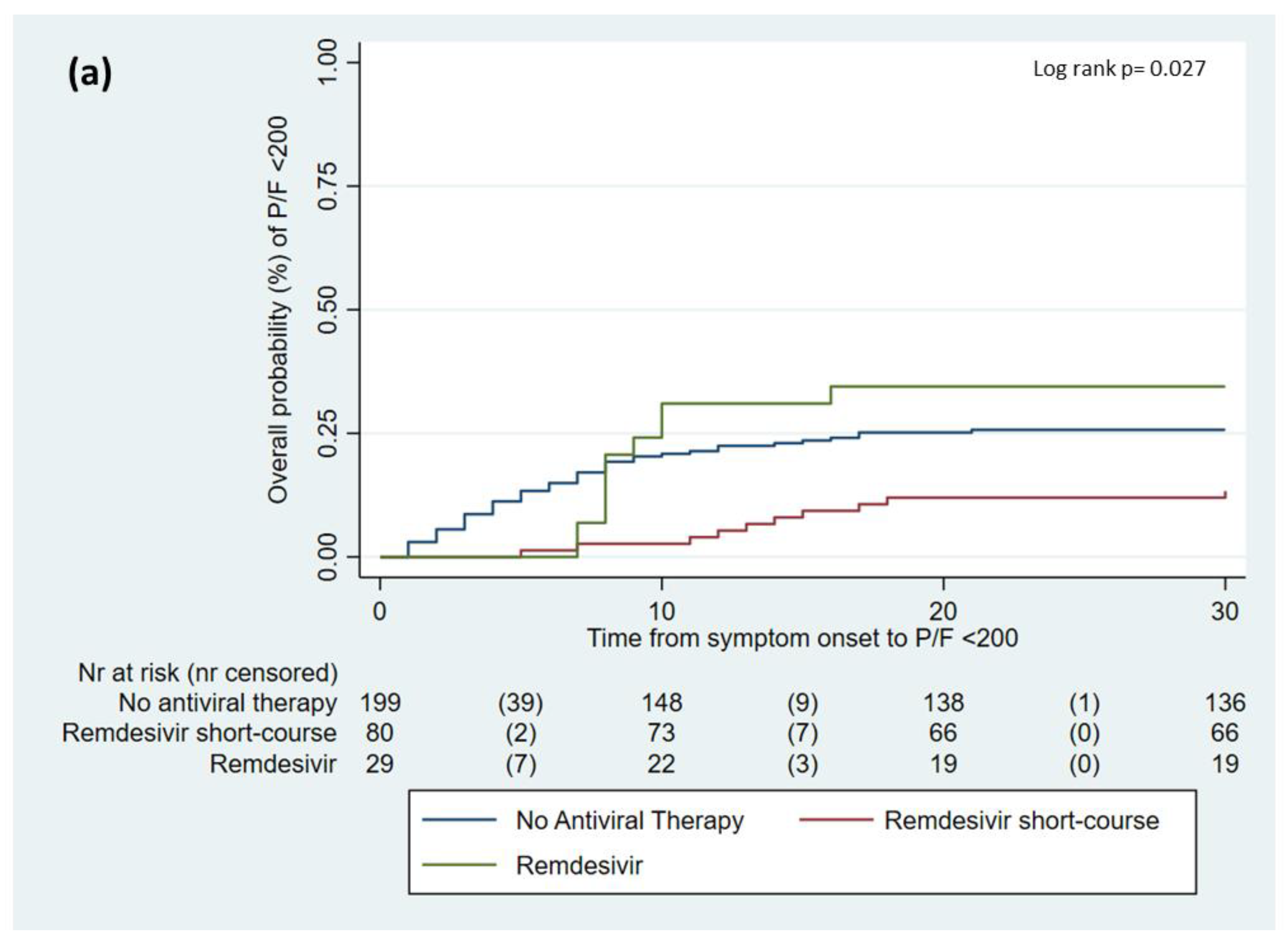
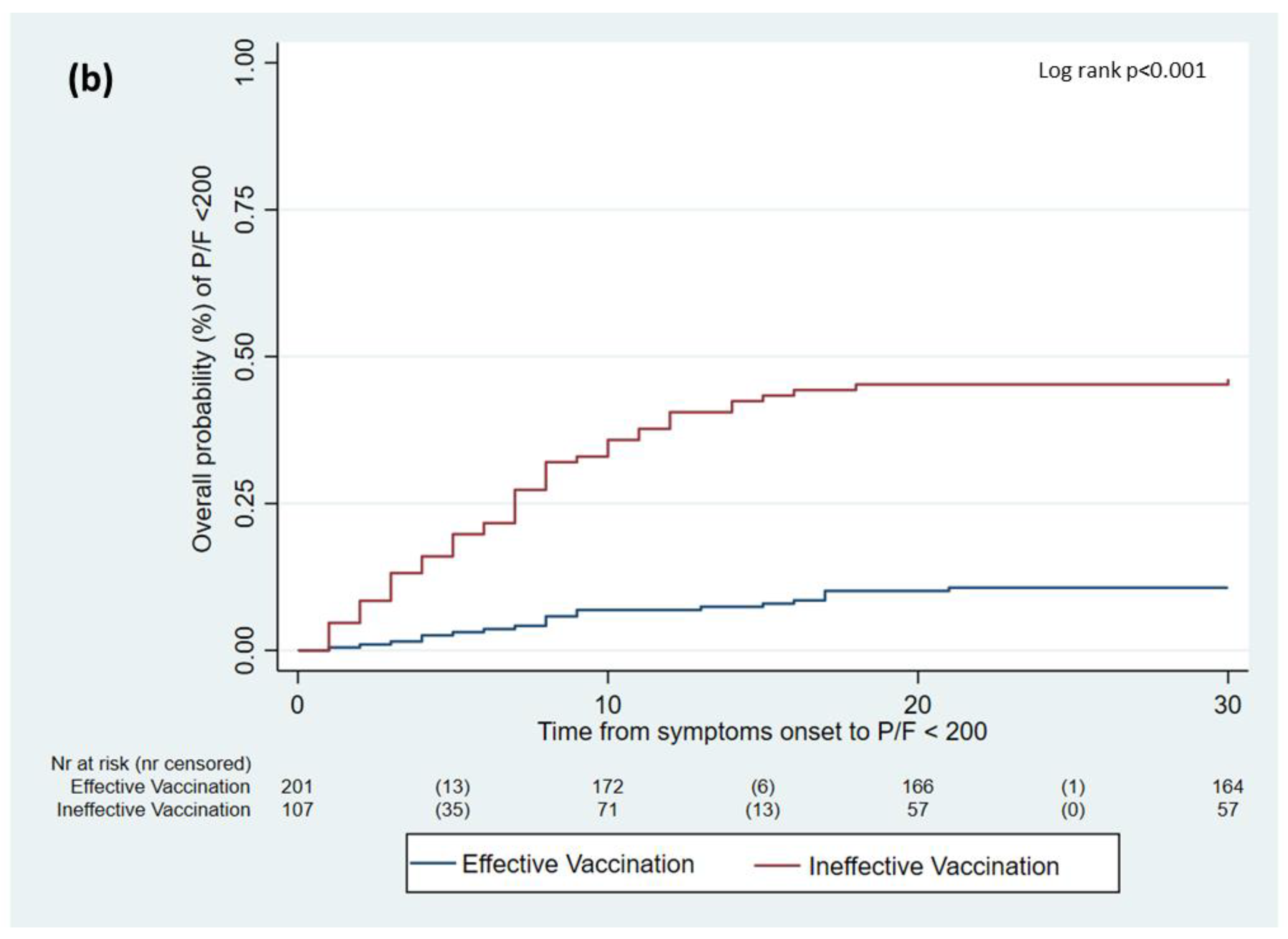
3.2. Predictors of COVID-19 Disease Progression in the Overall Population
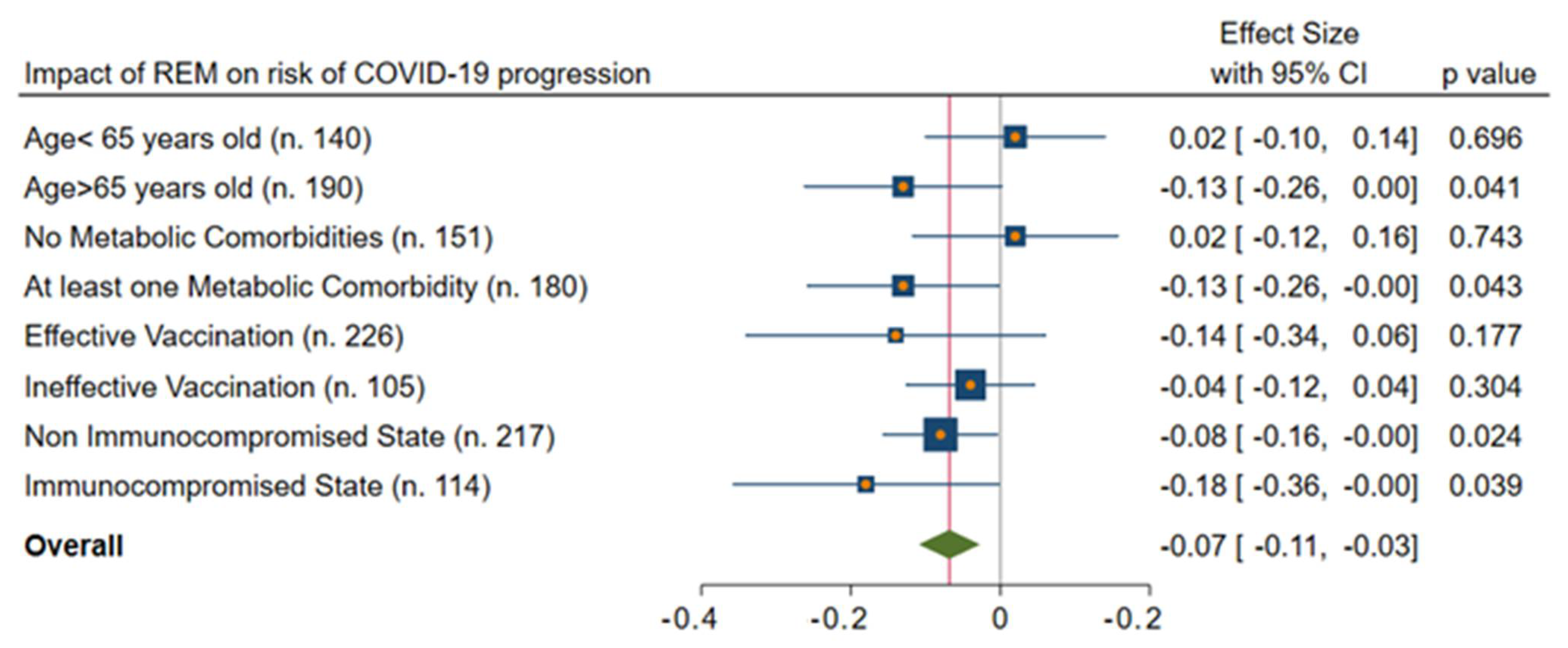
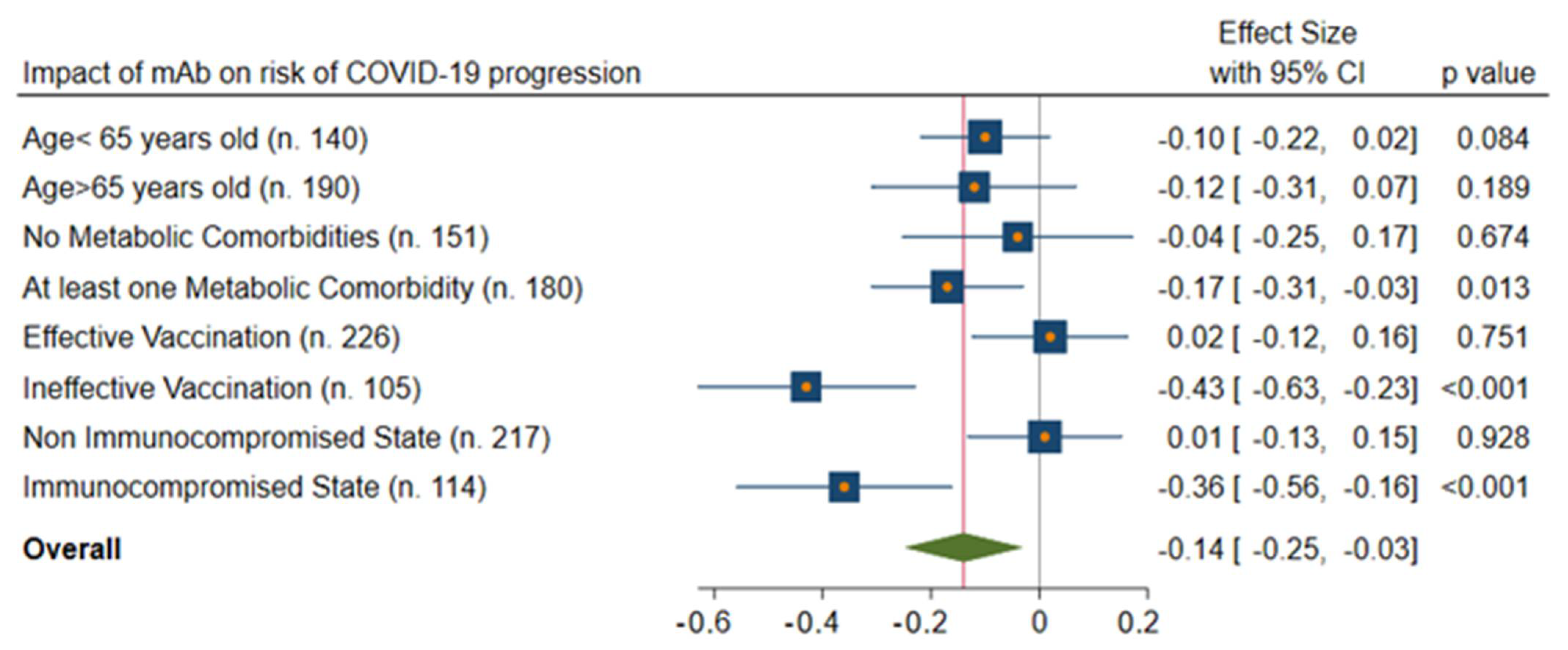
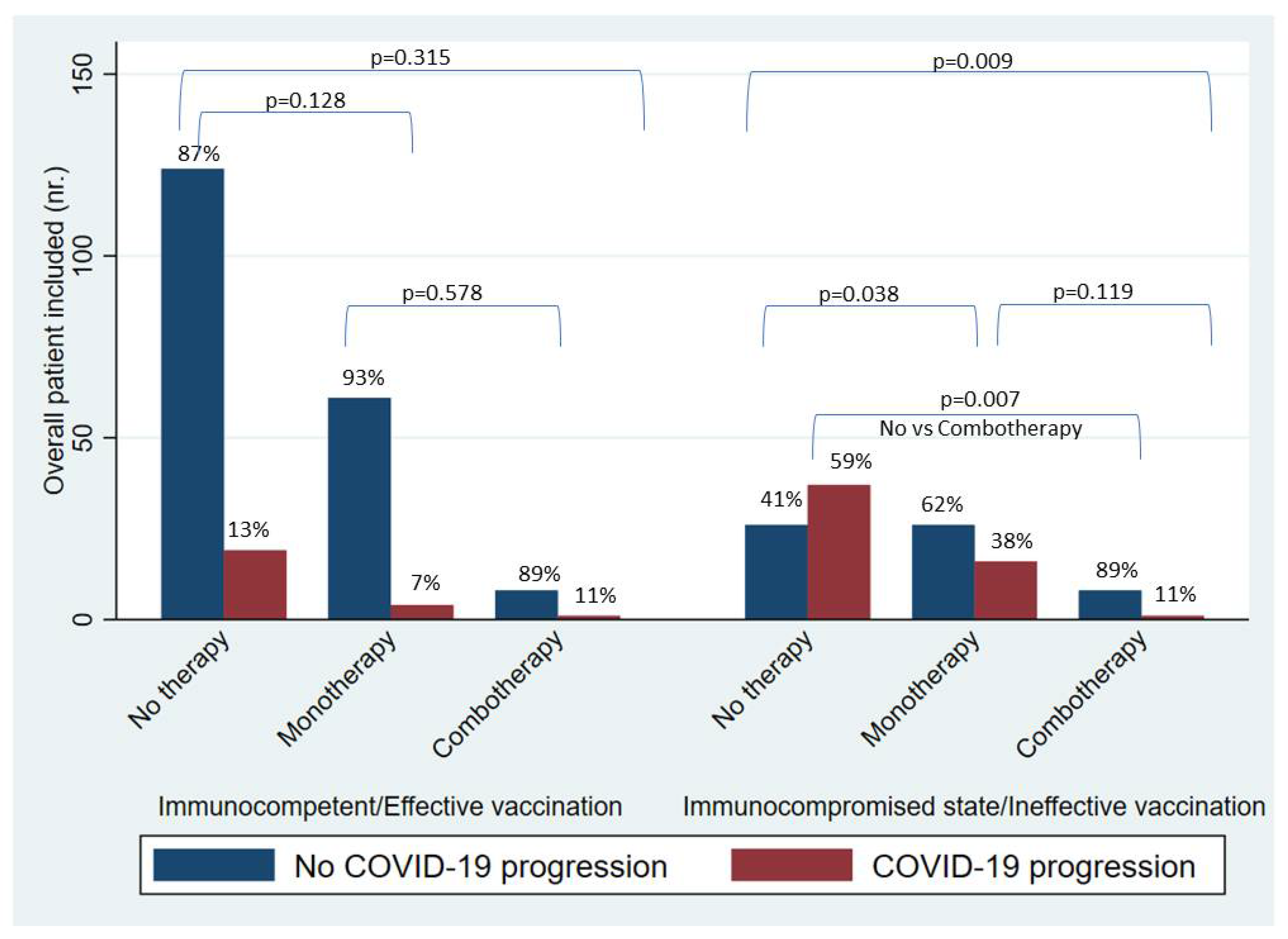
3.3. Impact of Mono- or Combo-Therapy on Risk of COVID-19 Progression According to Immunological Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Goletti, D.; Cantini, F. Baricitinib Therapy in COVID-19 Pneumonia—An Unmet Need Fulfilled. N. Engl. J. Med. 2021, 384, 867–869. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yang, L. Chinese herbal medicine: Fighting SARS-CoV-2 infection on all fronts. J. Ethnopharmacol. 2021, 270, 113869. [Google Scholar] [CrossRef] [PubMed]
- Bharadwaj, S.; El-Kafrawy, S.A.; Alandijany, T.A.; Bajrai, L.H.; Shah, A.A.; Dubey, A.; Sahoo, A.K.; Yadava, U.; Kamal, M.A.; Azhar, E.I.; et al. Structure-Based Identification of Natural Products as SARS-CoV-2 Mpro Antagonist from Echinacea angustifolia Using Computational Approaches. Viruses 2021, 13, 305. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Chamlagain, R.; Shah, S.; Sharma Paudel, B.; Dhital, R.; Kandel, B. Efficacy and Safety of Sarilumab in COVID-19: A Systematic Review. Interdiscip. Perspect. Infect. Dis. 2021, 2021, 8903435. [Google Scholar] [CrossRef]
- Balena, F.; Bavaro, D.F.; Fabrizio, C.; Bottalico, I.F.; Calamo, A.; Santoro, C.R.; Brindicci, G.; Bruno, G.; Mastroianni, A.; Greco, S.; et al. Tocilizumab and corticosteroids for COVID-19 treatment in elderly patients. J. Gerontol. Geriatr. 2020, 68, 197–203. Available online: http://www.jgerontology-geriatrics.com/article/view/283 (accessed on 9 August 2022). [CrossRef]
- Patel, T.K.; Patel, P.B.; Barvaliya, M.; Saurabh, M.K.; Bhalla, H.L.; Khosla, P.P. Efficacy and safety of lopinavir-ritonavir in COVID-19: A systematic review of randomized controlled trials. J. Infect. Public Health 2021, 14, 740–748. [Google Scholar] [CrossRef]
- Bansal, P.; Goyal, A.; Cusick, A.; Lahan, S., 4th; Dhaliwal, H.S.; Bhyan, P.; Bhattad, P.B.; Aslam, F.; Ranka, S.; Dalia, T.; et al. Hydroxychloroquine: A comprehensive review and its controversial role in coronavirus disease 2019. Ann. Med. 2021, 53, 117–134. [Google Scholar] [CrossRef]
- Ozer, M.; Goksu, S.Y.; Conception, R.; Ulker, E.; Balderas, R.M.; Mahdi, M.; Manning, Z.; To, K.; Effendi, M.; Anandakrishnan, R.; et al. Effectiveness and safety of Ivermectin in COVID-19 patients: A prospective study at a safety-net hospital. J. Med. Virol. 2022, 94, 1473–1480. [Google Scholar] [CrossRef]
- Milam, A.N.; Doan, D.T.; Childress, D.T.; Durham, S.H. Evaluation of Monoclonal Antibodies in Preventing Hospitalizations, Emergency Department Visits, and Mortality in High-Risk COVID-19 Patients. J. Pharm. Technol. 2022, 38, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Komagamine, J.; Yabuki, T.; Yoshihara, S.; Tanaka, N. The effect of casirivimab with imdevimab on disease progression in nonsevere COVID-19 patients in a single hospital in Japan. J. Gen. Fam. Med. 2021, 23, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Admninstration. Facts Sheet for Healthcare Providers: Emergency Use Authorization for Paxlovid. 2021. Available online: https://www.fda.gov/media/155050/download (accessed on 11 January 2023).
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19) Treatment Guidelines [Internet]; National Institutes of Health (US): Bethesda, MD, USA, 21 April 2021–30 September; 2022.
- Veklury: EPAR–Medicine Overview, EMA 666777/2022. Available online: https://www.ema.europa.eu/en/documents/overview/veklury-epar-medicine-overview_en.pdf (accessed on 12 January 2023).
- Wada, D.; Nakamori, Y.; Maruyama, S.; Shimazu, H.; Saito, F.; Yoshiya, K.; Kuwagata, Y. Novel treatment combining antiviral and neutralizing antibody-based therapies with monitoring of spike-specific antibody and viral load for immunocompromised patients with persistent COVID-19 infection. Exp. Hematol. Oncol. 2022, 11, 53. [Google Scholar] [CrossRef]
- Helleberg, M.; Niemann, C.U.; Moestrup, K.S.; Kirk, O.; Lebech, A.M.; Lane, C.; Lundgren, J. Persistent COVID-19 in an Immunocompromised Patient Temporarily Responsive to Two Courses of Remdesivir Therapy. J. Infect. Dis. 2020, 222, 1103–1107. [Google Scholar] [CrossRef]
- Gandhi, S.; Klein, J.; Robertson, A.J.; Peña-Hernández, M.A.; Lin, M.J.; Roychoudhury, P.; Lu, P.; Fournier, J.; Ferguson, D.; Mohamed Bakhash, S.A.K.; et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. Nat. Commun. 2022, 13, 1547. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, L.; Song, X.Q. Oral GS-441524 derivatives: Next-generation inhibitors of SARS-CoV-2 RNA-dependent RNA polymerase. Front. Immunol. 2022, 13, 1015355. [Google Scholar] [CrossRef]
- Gidari, A.; Sabbatini, S.; Schiaroli, E.; Bastianelli, S.; Pierucci, S.; Busti, C.; Comez, L.; Libera, V.; Macchiarulo, A.; Paciaroni, A.; et al. The Combination of Molnupiravir with Nirmatrelvir or GC376 Has a Synergic Role in the Inhibition of SARS-CoV-2 Replication In Vitro. Microorganisms 2022, 10, 1475. [Google Scholar] [CrossRef] [PubMed]
- Brookhart, M.A.; Schneeweiss, S.; Rothman, K.J.; Glynn, R.J.; Avorn, J.; Stürmer, T. Variable selection for propensity score models. Am. J. Epidemiol. 2006, 163, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 21 April 2023).
- Zazzara, M.B.; Bellieni, A.; Calvani, R.; Coelho-Junior, H.J.; Picca, A.; Marzetti, E. Inflammaging at the Time of COVID-19. Clin. Geriatr. Med. 2022, 38, 473–481. [Google Scholar] [CrossRef]
- Damanti, S.; Ramirez, G.A.; Bozzolo, E.P.; Da Prat, V.; Di Lucca, G.; Di Terlizzi, G.; Marinosci, A.; Scotti, R.; Strada, S.; Scarpellini, P.; et al. Frailty as a predictor of mortality in COVID-19 patients receiving CPAP for respiratory insufficiency. Aging Clin. Exp. Res. 2022, 34, 945–949. [Google Scholar] [CrossRef]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; Busca, A.; Corradini, P.; Hoenigl, M.; Klimko, N.; Koehler, P.; Pagliuca, A.; Passamonti, F.; et al. COVID-19 infection in adult patients with hematological malignancies: A European Hematology Association Survey (EPICOVIDEHA). J. Hematol. Oncol. 2021, 14, 168. [Google Scholar] [CrossRef]
- Martinez, M.A.; Chen, T.Y.; Choi, H.; Hwang, M.; Navarathna, D.; Hao, L.; Gale, M., Jr.; Camus, G.; Ramirez, H.E.; Jinadatha, C. Extended Remdesivir Infusion for Persistent Coronavirus Disease 2019 Infection. Open Forum Infect. Dis. 2022, 9, ofac382. [Google Scholar] [CrossRef]
- Ford, E.S.; Simmons, W.; Karmarkar, E.N.; Yoke, L.H.; Braimah, A.B.; Orozco, J.J.; Ghiuzeli, C.M.; Barnhill, S.; Sack, C.L.; Benditt, J.O.; et al. Successful treatment of prolonged, severe COVID-19 lower respiratory tract disease in a B-cell ALL patient with an extended course of remdesivir and nirmatrelvir/ritonavir. Clin. Infect. Dis. 2023, 76, 926–929. [Google Scholar] [CrossRef]
- Takashita, E.; Kinoshita, N.; Yamayoshi, S.; Sakai-Tagawa, Y.; Fujisaki, S.; Ito, M.; Iwatsuki-Horimoto, K.; Halfmann, P.; Watanabe, S.; Maeda, K.; et al. Efficacy of Antiviral Agents against the SARS-CoV-2 Omicron Subvariant BA.2. N. Engl. J. Med. 2022, 386, 1475–1477. [Google Scholar] [CrossRef]
- Cox, M.; Peacock, T.P.; Harvey, W.T.; Hughes, J.; Wright, D.W.; COVID-19 Genomics UK (COG-UK) Consortium; Willett, B.J.; Thomson, E.; Gupta, R.K.; Peacock, S.J.; et al. SARS-CoV-2 variant evasion of monoclonal antibodies based on in vitro studies. Nature reviews. Microbiology 2023, 21, 112–124. [Google Scholar] [CrossRef]
- Falcone, M.; Suardi, L.R.; Tiseo, G.; Barbieri, C.; Giusti, L.; Galfo, V.; Forniti, A.; Caroselli, C.; Della Sala, L.; Tempini, S.; et al. Early Use of Remdesivir and Risk of Disease Progression in Hospitalized Patients with Mild to Moderate COVID-19. Clin. Ther. 2022, 44, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Hussain Alsayed, H.A.; Saheb Sharif-Askari, F.; Saheb Sharif-Askari, N.; Hussain, A.A.S.; Hamid, Q.; Halwani, R. Early administration of remdesivir to COVID-19 patients associates with higher recovery rate and lower need for ICU admission: A retrospective cohort study. PLoS ONE 2021, 16, e0258643. [Google Scholar] [CrossRef] [PubMed]
- Paranjape, N.; Husain, M.; Priestley, J.; Koonjah, Y.; Watts, C.; Havlik, J. Early Use of Remdesivir in Patients Hospitalized With COVID-19 Improves Clinical Outcomes: A Retrospective Observational Study. Infect. Dis. Clin. Pract. 2021, 29, e282–e286. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Wakita, H.; Ishihara, T.; Okazaki, H.; Ito, A.; Iwata, M.; Sonoda, S.; Doi, Y. Short-course remdesivir for healthcare-associated COVID-19: Case series from a non-acute care hospital. J. Infect. Chemother. 2023, 29, 95–97. [Google Scholar] [CrossRef]
- ACTIV-3–Therapeutics for Inpatients with COVID-19 (TICO) Study Group. Tixagevimab-cilgavimab for treatment of patients hospitalised with COVID-19: A randomised, double-blind, phase 3 trial. Lancet Respir. Med. 2022, 10, 972–984. [Google Scholar] [CrossRef]
- Yang, L.; Wang, Z. Natural Products, Alone or in Combination with FDA-Approved Drugs, to Treat COVID-19 and Lung Cancer. Biomedicines 2021, 9, 689. [Google Scholar] [CrossRef]
- ACTIV-3/TICO Bamlanivimab Study Group; Lundgren, J.D.; Grund, B.; Barkauskas, C.E.; Holland, T.L.; Gottlieb, R.L.; Sandkovsky, U.; Brown, S.M.; Knowlton, K.U.; Self, W.H.; et al. Responses to a Neutralizing Monoclonal Antibody for Hospitalized Patients With COVID-19 According to Baseline Antibody and Antigen Levels: A Randomized Controlled Trial. Ann. Intern. Med. 2022, 175, 234–243. [Google Scholar] [CrossRef]
- ACTIV-3/Therapeutics for Inpatients with COVID-19 (TICO) Study Group. Efficacy and safety of two neutralising monoclonal antibody therapies, sotrovimab and BRII-196 plus BRII-198, for adults hospitalised with COVID-19 (TICO): A randomised controlled trial. Lancet Infect. Dis. 2022, 22, 622–635. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Shafran, N.; Shafran, I.; Ben-Zvi, H.; Sofer, S.; Sheena, L.; Krause, I.; Shlomai, A.; Goldberg, E.; Sklan, E.H. Secondary bacterial infection in COVID-19 patients is a stronger predictor for death compared to influenza patients. Sci. Rep. 2021, 11, 12703. [Google Scholar] [CrossRef]
- Bavaro, D.F.; Belati, A.; Diella, L.; Poli, M.A.; Calamo, A.; De Candia, G.; Altamura, M.; Spadavecchia, F.A.; Brindicci, G.; De Gennaro, N.; et al. Prompt and Appropriate Antimicrobial Therapy Improves Outcomes of NDM-Producing and KPC-Producing Klebsiella pneumoniae Bloodstream Infections in Patients Hospitalized for COVID-19: A Comparative Retrospective Case-Series. Antibiotics 2022, 11, 1519. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Suardi, L.R.; Tiseo, G.; Galfo, V.; Occhineri, S.; Verdenelli, S.; Ceccarelli, G.; Poli, M.; Merli, M.; Bavaro, D.; et al. Superinfections caused by carbapenem-resistant Enterobacterales in hospitalized patients with COVID-19: A multicentre observational study from Italy (CREVID Study). JAC-Antimicrob. Resist. 2022, 4, dlac064. [Google Scholar] [CrossRef]
- Falcone, M.; Tiseo, G.; Giordano, C.; Leonildi, A.; Menichini, M.; Vecchione, A.; Pistello, M.; Guarracino, F.; Ghiadoni, L.; Forfori, F.; et al. Predictors of hospital-acquired bacterial and fungal superinfections in COVID-19: A prospective observational study. J. Antimicrob. Chemother. 2021, 76, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Simon, M.S.; Satlin, M.J. Bacterial Coinfections in Coronavirus Disease 2019. Trends Microbiol. 2021, 29, 930–941. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, COVID-19 Portal. Available online: https://www.covid19dataportal.it/highlights/highlight47/ (accessed on 15 February 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with Asymptomatic or Mild to Moderate SARS-CoV-2 Infection with no Need for Oxygen Therapy | Patients with Severe SARS-CoV-2 Infection and Respiratory Failure (P/F < 300) | Critical SARS-CoV-2 Infection Requiring High Flow Oxygen Therapy/Non-Invasive Ventilation |
|---|---|---|
| Antiviral Therapy | Antiviral Therapy | Antiviral Therapy |
| Remdesivir 3-day short course | Remdesivir 5-day course | None |
| Inclusion criteria: | ||
| Solid tumor/ hematologic neoplasia | ||
| Chronic kidney failure | ||
| Diabetes | ||
| BMI > 30 | ||
| Severe cardiovascular disease | Inclusion criteria: | |
| Chronic liver impairment | Radiological pneumonia signs | |
| Any condition of immunosuppression | Symptom onset <10 days (even >10 days in immunocompromised) | |
| Monoclonal Antibodies | Monoclonal Antibodies | Monoclonal Antibodies |
| Inclusion criteria: | None | None |
| Ineffective vaccination and severe kidney/liver impairment that contraindicated remdesivir | ||
| OTHER THERAPIES | OTHER THERAPIES | OTHER THERAPIES |
| Low molecular weight heparin for 14 days or until discharge | Low molecular weight heparin for 14 days or until discharge | Low molecular weight heparin for 14 days or until discharge |
| PLUS | PLUS | |
| Dexamethasone for 10 days | Dexamethasone for 10 days | |
| Immunocompromised state or multiple risk factors in subjects with ineffective vaccination | Immunocompromised state or multiple risk factors in subjects with ineffective vaccination | Immunocompromised state or multiple risk factors in subjects with ineffective vaccination |
| Remdesivir + mAbs | Remdesivir + mAbs | No Antiviral/mAbs |
| Overall (n. 331) | No Disease Progression (n. 253) | Disease Progression (n. 78) | p-Value | |
|---|---|---|---|---|
| Age (y), median (q1–q3) | 71 (51–80) | 66 (48–79) | 75 (65–84) | 0.005 |
| Male sex, n (%) | 173 (52) | 138 (55) | 35 (45) | 0.135 |
| Metabolic comorbidities, n (%) | ||||
| Cardiovascular diseases | 32 (10) | 22 (9) | 10 (13) | 0.281 |
| Diabetes | 70 (21) | 49 (19) | 21 (27) | 0.153 |
| Chronic lung diseases * | 50 (15) | 40 (16) | 10 (13) | 0.519 |
| Chronic kidney failure | 28 (8) | 18 (7) | 10 (13) | 0.113 |
| Chronic liver diseases | 14 (4) | 10 (4) | 4 (5) | 0.652 |
| Obesity | 48 (14) | 36 (14) | 12 (15) | 0.800 |
| Immunosuppressive state, n (%) | ||||
| Autoimmune disease | 14 (4) | 11 (4) | 3 (4) | 0.847 |
| Any solid cancer | 62 (19) | 49 (19) | 13 (17) | 0.593 |
| Hematologic neoplasia | 23 (7) | 18 (7) | 6 (7) | 0.768 |
| Solid organ transplant recipient | 15 (5) | 10 (4) | 5 (6) | 0.316 |
| Vaccination status, n (%) | ||||
| No or one dose of anti-SARS-CoV2 vaccine ** | 80 (24) | 45 (18) | 35 (45) | <0.001 |
| Two doses of anti-SARS-CoV2 vaccine | 25 (8) | 8 (3) | 17 (22) | |
| Three doses of anti-SARS-CoV2 vaccine | 226 (68) | 200 (79) | 26 (33) | |
| Median (q1–q3) months since last dose of vaccine | 3 (2–5) | 3 (3–5) | 2 (2–4) | 0.145 |
| Symptoms at hospitalization, n (%) | ||||
| Asymptomatic | 91 (27) | 82 (32) | 9 (12) | <0.001 |
| Fever and organ symptoms | 113 (34) | 93 (37) | 20 (26) | 0.070 |
| Pneumonia and hypoxia | 30 (9) | 12 (5) | 18 (23) | <0.001 |
| Other symptoms | 97 (30) | 64 (26) | 31 (39) | 0.020 |
| COVID-19 disease severity on admission, n (%) | ||||
| Presymptomatic infection | 91 (27) | 82 (32) | 9 (12) | |
| Mild–moderate illness | 186 (56) | 128 (51) | 58 (74) | <0.001 |
| Severe illness | 54 (17) | 43 (17) | 11 (14) | |
| Laboratory features at admission, median (q1–q3) | ||||
| Leucocytes, cell/uL | 6310 (4680–9030) | 6240 (4770–8810) | 7270 (4540–9600) | 0.357 |
| Lymphocytes, cell/uL | 1089 (677–1560) | 1114 (695–1630) | 916 (650–1218) | 0.069 |
| Platelets, cell/uL | 196 (149–258) | 197 (149–255) | 196 (143–269) | 0.783 |
| C-reactive protein mg/L | 62 (13.3–112) | 53.9 (11.5–97.1) | 131 (72.9–178) | <0.001 |
| Treatment included in standard of care, n (%) | ||||
| Corticosteroids | 185 (56) | 119 (47) | 66 (85) | <0.001 |
| Low molecular weight heparin/other anticoagulants | 244 (74) | 175 (69) | 69 (88) | 0.001 |
| Treated with monoclonal antibody, n (%) | 37 (11) | 33 (13) | 4 (5) | 0.052 |
| Treated with remdesivir, n (%) | ||||
| No antivirals | 211 (63) | 155 (62) | 56 (72) | 0.011 |
| Short-course remdesivir | 88 (27) | 77 (30) | 11 (14) | |
| remdesivir | 32 (10) | 21 (8) | 11 (14) | |
| Combination therapy (REM plus mAbs), n (%) | 18 (5) | 16 (6) | 2 (3) | 0.108 |
| Complications during hospitalization, n (%) | ||||
| Heart failure | 25 (8) | 16 (6) | 9 (12) | 0.128 |
| Kidney failure | 22 (7) | 16 (6) | 6 (8) | 0.678 |
| Secondary severe infection | 33 (10) | 17 (7) | 16 (21) | <0.001 |
| All-cause in-hospital mortality, n (%) | 47 (14) | 19 (7) | 28 (36) | <0.001 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | aHR | 95% CI | p-Value | |
| Age (per 1 year increase) | 1.02 | 1.00–1.03 | 0.001 | 1.04 | 1.01–1.06 | <0.001 |
| Male sex | 0.79 | 0.43–1.27 | 0.334 | 0.71 | 0.37–1.37 | 0.319 |
| At least one comorbidity | 1.57 | 0.93–2.65 | 0.088 | 0.93 | 0.45–1.93 | 0.866 |
| Cardiovascular diseases | 1.15 | 0.72–1.86 | 0.543 | \ | ||
| Diabetes | 1.51 | 0.89–2.56 | 0.124 | \ | ||
| Chronic lung diseases | 0.69 | 0.33–1.44 | 0.325 | \ | ||
| Chronic kidney failure | 1.46 | 0.66–3.19 | 0.340 | \ | ||
| Obesity (BMI > 30) | 1.07 | 0.56–2.04 | 0.835 | \ | ||
| Any solid cancer | 0.75 | 0.39–1.43 | 0.390 | \ | ||
| Hematologic cancer | 1.20 | 0.52–2.77 | 0.666 | 3.62 | 1.00–13.05 | 0.049 |
| Vaccination status | ||||||
| No or one dose of anti-SARS-CoV2 vaccine | 1 | 1 | ||||
| Two doses of anti-SARS-CoV2 vaccine | 2.73 | 1.05–7.05 | 0.038 | 2.26 | 0.70–7.24 | 0.169 |
| Three doses of anti-SARS-CoV2 vaccine | 0.16 | 0.09–0.30 | <0.001 | 0.11 | 0.05–0.24 | <0.001 |
| COVID-19 disease severity on admission | ||||||
| Presymptomatic infection | 1 | 1 | ||||
| Mild–moderate illness | 4.12 | 1.94–8.78 | <0.001 | 4.70 | 1.86–11.83 | 0.001 |
| Severe illness | 2.33 | 0.89–6.05 | 0.082 | 3.35 | 1.11–10.12 | 0.032 |
| Complications during hospitalization | ||||||
| Heart failure | 1.63 | 0.74–3.58 | 0.216 | \ | ||
| Kidney failure | 1.22 | 0.49–3.05 | 0.658 | \ | ||
| Secondary severe infection | 3.31 | 1.86–5.87 | <0.001 | 3.36 | 1.30–8.63 | 0.012 |
| Monoclonal antibody | 0.43 | 0.15–1.18 | 0.104 | \ | ||
| Antiviral therapy | ||||||
| No antiviral | 1 | 1 | ||||
| Short-course remdesivir | 0.44 | 0.22–0.88 | 0.021 | 0.20 | 0.08–0.49 | <0.001 |
| Remdesivir | 1.29 | 0.65–2.56 | 0.454 | 0.75 | 0.27–2.04 | 0.578 |
| Treatment strategy | ||||||
| No therapy | 1 | \ | ||||
| Monotherapy (antiviral or mAb) | 0.65 | 0.38–1.12 | 0.127 | \ | ||
| Combination therapy (antiviral plus mAb) | 0.42 | 0.10–1.74 | 0.236 | \ |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | aHR | 95% CI | p-Value | |
| Age (per 1 year increase) | 1.02 | 1.00–1.03 | 0.006 | 1.04 | 1.01–1.07 | 0.006 |
| Male sex | 0.69 | 0.39–1.23 | 0.213 | 0.37 | 0.14–1.00 | 0.050 |
| At least one comorbidity | 1.92 | 0.90–4.05 | 0.087 | 0.97 | 0.32–2.97 | 0.970 |
| Cardiovascular diseases | 1.23 | 0.68–2.20 | 0.479 | |||
| Diabetes | 2.31 | 1.20–4.44 | 0.012 | |||
| Chronic lung diseases | 1.32 | 0.41–4.27 | 0.634 | |||
| Chronic kidney failure | 1.37 | 0.54–3.46 | 0.500 | |||
| Obesity (BMI > 30) | 0.63 | 0.27–1.49 | 0.300 | |||
| Any solid cancer | 0.67 | 0.31–1.43 | 0.307 | |||
| Hematologic cancer | 0.66 | 0.26–1.67 | 0.387 | 1.29 | 0.27–6.11 | 0.747 |
| COVID-19 disease severity on admission | ||||||
| Presymptomatic infection | 1 | 1 | ||||
| Mild–moderate illness | 5.88 | 1.78–19.28 | 0.004 | 13.09 | 2.82–60.77 | 0.001 |
| Severe illness | 1.71 | 0.40–7.33 | 0.468 | 5.93 | 0.89–39.54 | 0.066 |
| Complications during hospitalization | ||||||
| Heart failure | 1.87 | 0.67–5.23 | 0.229 | |||
| Kidney failure | 1.37 | 0.33–5.64 | 0.662 | |||
| Secondary severe infection | 2.78 | 1.34–5.76 | 0.006 | 1.91 | 0.41–8.76 | 0.402 |
| Monoclonal antibody | 0.19 | 0.04–0.80 | 0.024 | \ | ||
| Antiviral therapy | ||||||
| No antiviral | 1 | \ | ||||
| Antiviral therapy with remdesivir | 0.51 | 0.28–0.91 | 0.025 | \ | ||
| Treatment strategy | ||||||
| No therapy | 1 | 1 | ||||
| Monotherapy (antiviral or mAb) | 0.47 | 0.25–0.87 | 0.018 | 0.23 | 0.08–0.65 | 0.006 |
| Combination therapy (antiviral plus mAb) | 0.13 | 0.19–1.02 | 0.053 | 0.06 | 0.02–0.77 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bavaro, D.F.; Diella, L.; Belati, A.; Metrangolo, G.; De Santis, L.; Spada, V.; Camporeale, M.; Dargenio, A.; Brindicci, G.; Balena, F.; et al. Efficacy of Remdesivir and Neutralizing Monoclonal Antibodies in Monotherapy or Combination Therapy in Reducing the Risk of Disease Progression in Elderly or Immunocompromised Hosts Hospitalized for COVID-19: A Single Center Retrospective Study. Viruses 2023, 15, 1199. https://doi.org/10.3390/v15051199
Bavaro DF, Diella L, Belati A, Metrangolo G, De Santis L, Spada V, Camporeale M, Dargenio A, Brindicci G, Balena F, et al. Efficacy of Remdesivir and Neutralizing Monoclonal Antibodies in Monotherapy or Combination Therapy in Reducing the Risk of Disease Progression in Elderly or Immunocompromised Hosts Hospitalized for COVID-19: A Single Center Retrospective Study. Viruses. 2023; 15(5):1199. https://doi.org/10.3390/v15051199
Chicago/Turabian StyleBavaro, Davide Fiore, Lucia Diella, Alessandra Belati, Giuliana Metrangolo, Laura De Santis, Vito Spada, Michele Camporeale, Angelo Dargenio, Gaetano Brindicci, Flavia Balena, and et al. 2023. "Efficacy of Remdesivir and Neutralizing Monoclonal Antibodies in Monotherapy or Combination Therapy in Reducing the Risk of Disease Progression in Elderly or Immunocompromised Hosts Hospitalized for COVID-19: A Single Center Retrospective Study" Viruses 15, no. 5: 1199. https://doi.org/10.3390/v15051199