
Remdesivir Use in the Real-World Setting: An Overview of Available Evidence
 , ,
, ,
Abstract
:1. Introduction
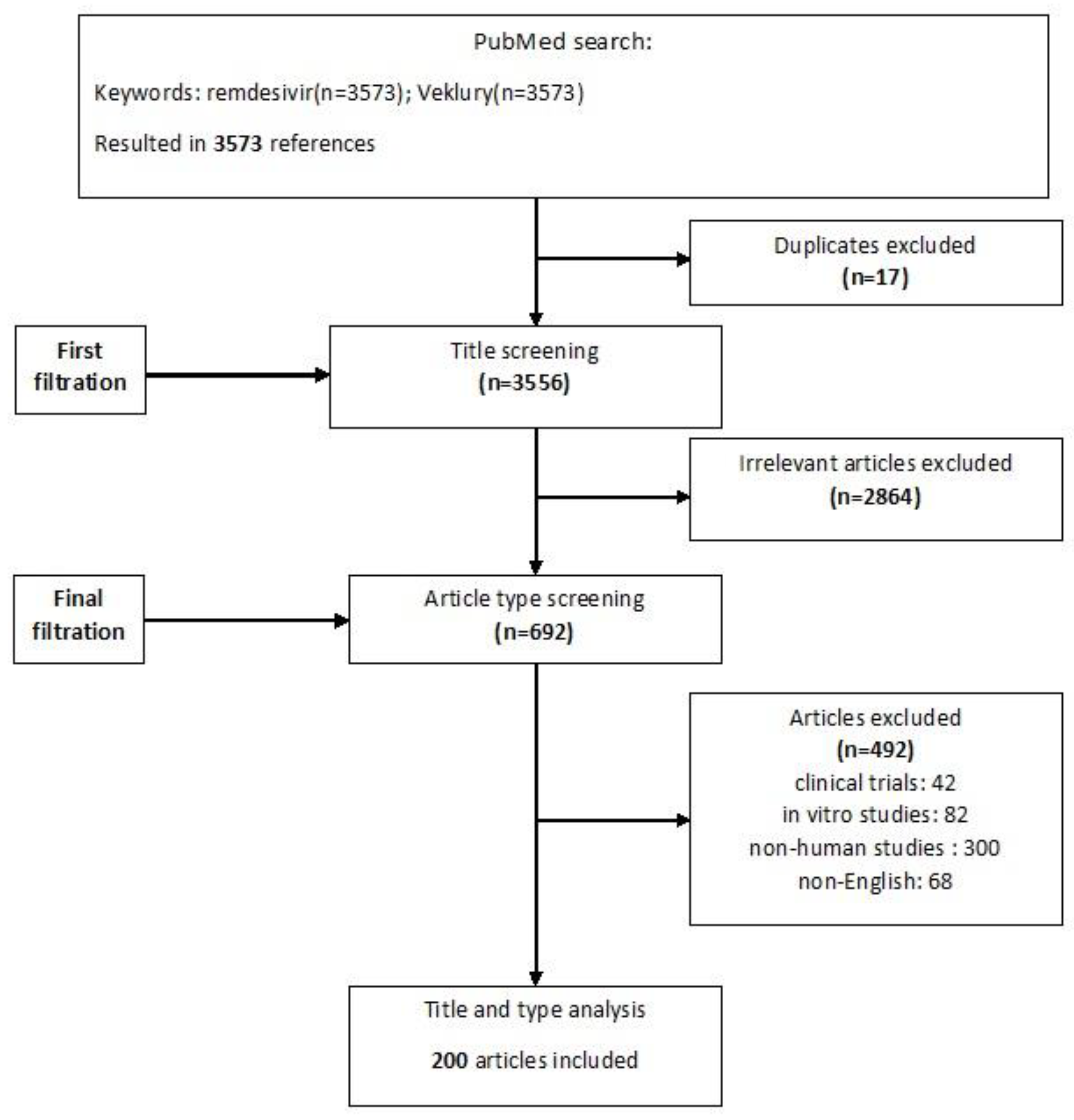
2. Materials and Methods
3. Remdesivir Outcomes
3.1. Clinical Improvement and Increased Chance of Recovery
3.2. Reduced Disease Progression
3.3. Reduced Mortality: Treatment Comparison
3.4. Benefits of Early Treatment
3.5. Reduced Post Hospitalization Outcomes
4. Remdesivir in Combination with Other Agents
5. Special Populations
6. Resistance/Mutations
7. Limitations
8. Expert Opinion and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yang, L. Broad-spectrum prodrugs with anti-SARS-CoV-2 activities: Strategies, benefits, and challenges. J. Med. Virol. 2022, 94, 1373–1390. [Google Scholar] [CrossRef] [PubMed]
- Frediansyah, A.; Nainu, F.; Dhama, K.; Mudatsir, M.; Harapan, H. Remdesivir and its antiviral activity against COVID-19: A systematic review. Clin. Epidemiol. Glob. Health 2021, 9, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Aleem, A.; Kothadia, J.P. Remdesivir. In StatPearls; StatPearls Publishing LLC: Tampa, FL, USA, 2023. [Google Scholar]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.X.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Ho, Y.F.; Hu, F.C.; Lee, P.I. The Advantages and Challenges of Using Real-World Data for Patient Care. Clin. Transl. Sci. 2020, 13, 4–7. [Google Scholar] [CrossRef]
- Liang, C.; Tian, L.; Liu, Y.; Hui, N.; Qiao, G.; Li, H.; Shi, Z.; Tang, Y.; Zhang, D.; Xie, X.; et al. A promising antiviral candidate drug for the COVID-19 pandemic: A mini-review of remdesivir. Eur. J. Med. Chem. 2020, 201, 112527. [Google Scholar] [CrossRef]
- Yang, L.; Wang, Z. Natural Products, Alone or in Combination with FDA-Approved Drugs, to Treat COVID-19 and Lung Cancer. Biomedicines 2021, 9, 689. [Google Scholar] [CrossRef]
- Tchesnokov, E.P.; Gordon, C.J.; Woolner, E.; Kocinkova, D.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; Gotte, M. Template-dependent inhibition of coronavirus RNA-dependent RNA polymerase by remdesivir reveals a second mechanism of action. J. Biol. Chem. 2020, 295, 16156–16165. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Zeger, S.L.; Bandeen-Roche, K.; Wang, M.C.; Alexander, G.C.; Gupta, A.; Bollinger, R.; Xu, Y. Comparison of Time to Clinical Improvement With vs. Without Remdesivir Treatment in Hospitalized Patients With COVID-19. JAMA Netw. Open 2021, 4, e213071. [Google Scholar] [CrossRef]
- Olender, S.A.; Walunas, T.L.; Martinez, E.; Perez, K.K.; Castagna, A.; Wang, S.; Kurbegov, D.; Goyal, P.; Ripamonti, D.; Balani, B.; et al. Remdesivir Versus Standard-of-Care for Severe Coronavirus Disease 2019 Infection: An Analysis of 28-Day Mortality. Open Forum Infect. Dis. 2021, 8, ofab278. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Betz, J.; Caleb Alexander, G.; Andersen, K.M.; Joseph, C.S.; Mehta, H.B.; Korwek, K.; Sands, K.E.; et al. Real-World Effectiveness of Remdesivir in Adults Hospitalized With Coronavirus Disease 2019 (COVID-19): A Retrospective, Multicenter Comparative Effectiveness Study. Clin. Infect. Dis. 2022, 75, e516–e524. [Google Scholar] [CrossRef] [PubMed]
- Lapadula, G.; Bernasconi, D.P.; Bellani, G.; Soria, A.; Rona, R.; Bombino, M.; Avalli, L.; Rondelli, E.; Cortinovis, B.; Colombo, E.; et al. Remdesivir Use in Patients Requiring Mechanical Ventilation due to COVID-19. Open Forum Infect. Dis. 2020, 7, ofaa481. [Google Scholar] [CrossRef] [PubMed]
- Petrakis, V.; Rapti, V.; Akinosoglou, K.; Bonelis, C.; Athanasiou, K.; Dimakopoulou, V.; Syrigos, N.K.; Spernovasilis, N.; Trypsianis, G.; Marangos, M.; et al. Greek Remdesivir Cohort (GREC) Study: Effectiveness of Antiviral Drug Remdesivir in Hospitalized Patients with COVID-19 Pneumonia. Microorganisms 2022, 10, 1949. [Google Scholar] [CrossRef]
- Joo, E.J.; Ko, J.H.; Kim, S.E.; Kang, S.J.; Baek, J.H.; Heo, E.Y.; Shi, H.J.; Eom, J.S.; Choe, P.G.; Bae, S.; et al. Clinical and Virologic Effectiveness of Remdesivir Treatment for Severe Coronavirus Disease 2019 (COVID-19) in Korea: A Nationwide Multicenter Retrospective Cohort Study. J. Korean Med. Sci. 2021, 36, e83. [Google Scholar] [CrossRef] [PubMed]
- Benfield, T.; Bodilsen, J.; Brieghel, C.; Harboe, Z.B.; Helleberg, M.; Holm, C.; Israelsen, S.B.; Jensen, J.; Jensen, T.; Johansen, I.S.; et al. Improved Survival Among Hospitalized Patients With Coronavirus Disease 2019 (COVID-19) Treated With Remdesivir and Dexamethasone. A Nationwide Population-Based Cohort Study. Clin. Infect. Dis. 2021, 73, 2031–2036. [Google Scholar] [CrossRef] [PubMed]
- Fintzi, J.; Bonnett, T.; Sweeney, D.A.; Huprikar, N.A.; Ganesan, A.; Frank, M.G.; McLellan, S.L.F.; Dodd, L.E.; Tebas, P.; Mehta, A.K. Deconstructing the Treatment Effect of Remdesivir in the Adaptive Coronavirus Disease 2019 (COVID-19) Treatment Trial-1: Implications for Critical Care Resource Utilization. Clin. Infect. Dis. 2022, 74, 2209–2217. [Google Scholar] [CrossRef] [PubMed]
- Chokkalingam, A.P.; Hayden, J.; Goldman, J.D.; Li, H.; Asubonteng, J.; Mozaffari, E.; Bush, C.; Wang, J.R.; Kong, A.; Osinusi, A.O.; et al. Association of Remdesivir Treatment With Mortality Among Hospitalized Adults With COVID-19 in the United States. JAMA Netw. Open 2022, 5, e2244505. [Google Scholar] [CrossRef]
- Mozaffari, E.; Chandak, A.; Zhang, Z.; Liang, S.; Thrun, M.; Gottlieb, R.L.; Kuritzkes, D.R.; Sax, P.E.; Wohl, D.A.; Casciano, R.; et al. Remdesivir Treatment in Hospitalized Patients With Coronavirus Disease 2019 (COVID-19): A Comparative Analysis of In-hospital All-cause Mortality in a Large Multicenter Observational Cohort. Clin. Infect. Dis. 2022, 75, e450–e458. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Remdesivir and three other drugs for hospitalised patients with COVID-19: Final results of the WHO Solidarity randomised trial and updated meta-analyses. Lancet 2022, 399, 1941–1953. [Google Scholar] [CrossRef]
- Amstutz, A.; Speich, B.; Mentré, F.; Rueegg, C.S.; Belhadi, D.; Assoumou, L.; Costagliola, D.; Olsen, I.C.; Briel, M. Remdesivir in Hospitalized COVID-19 Patients: Individual Patient Data Meta-Analysis. In Proceedings of the 2023 Conference on Retroviruses and Opportunistic Infections, Seattle, WA, USA, 19–22 February 2023. [Google Scholar]
- Mozaffari, E.; Chandak, A.; Kalil, A.C.; Chima-Melton, C.; Chiang, M.; Lee, E.Y.; Gupta, R.; Wang, C.Y.; Gottlieb, R. Immunocompromised patients hospitalized for COVID-19 in the United States: Evolving patient characteristics and clinical outcomes across emerging variants. In Proceedings of the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Mozaffari, E.; Chandak, A.; Gottlieb, R.L.; Chima-Melton, C.; Read, S.; Dau, L.; Thrun, M.; Gupta, R.; Berry, M.; Hollemeersch, S.; et al. Remdesivir is associated with decreased mortality in hospitalised COVID-19 patients requiring high-flow oxygen in the United States. In Proceedings of the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Tiseo, G.; Barbieri, C.; Galfo, V.; Occhineri, S.; Matucci, T.; Almerigogna, F.; Kalo, J.; Sponga, P.; Cesaretti, M.; Marchetti, G.; et al. Efficacy and Safety of Nirmatrelvir/Ritonavir, Molnupiravir, and Remdesivir in a Real-World Cohort of Outpatients with COVID-19 at High Risk of Progression: The PISA Outpatient Clinic Experience. Infect. Dis. Ther. 2023, 12, 257–271. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Alonso, R.; Camon, A.M.; Cardozo, C.; Albiach, L.; Agüero, D.; Marcos, M.A.; Ambrosioni, J.; Bodro, M.; Chumbita, M.; et al. Impact of remdesivir according to the pre-admission symptom duration in patients with COVID-19. J. Antimicrob. Chemother. 2021, 76, 3296–3302. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, V.; Voarino, M.; Tonelli, M.; Galli, L.; Poli, A.; Bruzzesi, E.; Racca, S.; Clementi, N.; Oltolini, C.; Tresoldi, M.; et al. Impact of Remdesivir on SARS-CoV-2 Clearance in a Real-Life Setting: A Matched-Cohort Study. Drug Des. Devel. Ther. 2022, 16, 3645–3654. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Lau, K.T.K.; Au, I.C.H.; Xiong, X.; Lau, E.H.Y.; Cowling, B.J. Clinical Improvement, Outcomes, Antiviral Activity, and Costs Associated With Early Treatment With Remdesivir for Patients With Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2022, 74, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Aye, T.T.; Myat, K.; Tun, H.P.; Thiha, P.; Han, T.M.; Win, Y.Y.; Han, A.M.M. Early initiation of remdesivir and its effect on oxygen desaturation: A clinical review study among high-risk COVID-19 patients in Myanmar. J. Fam. Med. Prim. Care 2022, 11, 4644–4649. [Google Scholar] [CrossRef] [PubMed]
- Paranjape, N.; Husain, M.; Priestley, J.; Koonjah, Y.; Watts, C.; Havlik, J. Early Use of Remdesivir in Patients Hospitalized With COVID-19 Improves Clinical Outcomes: A Retrospective Observational Study. Infect. Dis. Clin. Pract. 2021, 29, e282–e286. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos, P.; Petrakis, V.; Trypsianis, G.; Papazoglou, D. Early 3-day course of remdesivir in vaccinated outpatients with SARS-CoV-2 infection. A success story. J. Chemother. 2022, 34, 550–553. [Google Scholar] [CrossRef]
- Piccicacco, N.; Zeitler, K.; Ing, A.; Montero, J.; Faughn, J.; Silbert, S.; Kim, K. Real-world effectiveness of early remdesivir and sotrovimab in the highest-risk COVID-19 outpatients during the Omicron surge. J. Antimicrob. Chemother. 2022, 77, 2693–2700. [Google Scholar] [CrossRef]
- Biscarini, S.; Villa, S.; Genovese, C.; Tomasello, M.; Tonizzo, A.; Fava, M.; Iannotti, N.; Bolis, M.; Mariani, B.; Valzano, A.G.; et al. Safety Profile and Outcomes of Early COVID-19 Treatments in Immunocompromised Patients: A Single-Centre Cohort Study. Biomedicines 2022, 10, 2002. [Google Scholar] [CrossRef]
- Meini, S.; Bracalente, I.; Bontempo, G.; Longo, B.; De Martino, M.; Tascini, C. Early 3-day course of remdesivir to prevent progression to severe Covid-19 in high-risk patients with hospital-acquired SARS-CoV-2 infection: Preliminary results from two Italian outbreaks. New Microbiol. 2022, 45, 304–307. [Google Scholar]
- Rajme-Lopez, S.; Martinez-Guerra, B.A.; Zalapa-Soto, J.; Roman-Montes, C.M.; Tamez-Torres, K.M.; Gonzalez-Lara, M.F.; Hernandez-Gilosul, T.; Kershenobich-Stalnikowitz, D.; Sifuentes-Osornio, J.; Ponce-de-Leon, A.; et al. Early Outpatient Treatment With Remdesivir in Patients at High Risk for Severe COVID-19: A Prospective Cohort Study. Open Forum Infect. Dis. 2022, 9, ofac502. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, E.; Liang, S.; Stewart, H.M.; Thrun, M.; Hodgkins, P.; Haubrich, R. 459. COVID-19 Hospitalization and 30-Day Readmission: A Cohort Study of U.S. Hospitals. Open Forum Infect. Dis. 2021, 8, S332. [Google Scholar] [CrossRef]
- Finn, A.; Jindal, A.; Andrea, S.B.; Selvaraj, V.; Dapaah-Afriyie, K. Association of Treatment with Remdesivir and 30-day Hospital Readmissions in Patients Hospitalized with COVID-19. Am. J. Med. Sci. 2022, 363, 403–410. [Google Scholar] [CrossRef]
- Gupta, R.S.; Berry, M.; Abdelghany, M.; Chokkalingam, A. Remdesivir Reduced the Hazard of Hospital Readmission in People With COVID-19 Admitted to the ICU While Delta and Omicron Were the Predominant Circulating Variants. In Proceedings of the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Boglione, L.; Meli, G.; Poletti, F.; Rostagno, R.; Moglia, R.; Cantone, M.; Esposito, M.; Scianguetta, C.; Domenicale, B.; Di Pasquale, F.; et al. Risk factors and incidence of long-COVID syndrome in hospitalized patients: Does remdesivir have a protective effect? QJM 2022, 114, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Nevalainen, O.P.O.; Horstia, S.; Laakkonen, S.; Rutanen, J.; Mustonen, J.M.J.; Kalliala, I.E.J.; Ansakorpi, H.; Kreivi, H.R.; Kuutti, P.; Paajanen, J.; et al. Effect of remdesivir post hospitalization for COVID-19 infection from the randomized SOLIDARITY Finland trial. Nat. Commun. 2022, 13, 6152. [Google Scholar] [CrossRef] [PubMed]
- Marrone, A.; Nevola, R.; Sellitto, A.; Cozzolino, D.; Romano, C.; Cuomo, G.; Aprea, C.; Schwartzbaum, M.X.P.; Ricozzi, C.; Imbriani, S.; et al. Remdesivir Plus Dexamethasone Versus Dexamethasone Alone for the Treatment of Coronavirus Disease 2019 (COVID-19) Patients Requiring Supplemental O2 Therapy: A Prospective Controlled Nonrandomized Study. Clin. Infect. Dis. 2022, 75, e403–e409. [Google Scholar] [CrossRef] [PubMed]
- Hanafusa, M.; Nawa, N.; Goto, Y.; Kawahara, T.; Miyamae, S.; Ueki, Y.; Nosaka, N.; Wakabayashi, K.; Tohda, S.; Tateishi, U.; et al. Effectiveness of remdesivir with corticosteroids for COVID-19 patients in intensive care unit: A hospital-based observational study. J. Med. Virol. 2023, 95, e28168. [Google Scholar] [CrossRef] [PubMed]
- Pilgram, L.; Appel, K.S.; Ruethrich, M.M.; Koll, C.E.M.; Vehreschild, M.; de Miranda, S.M.N.; Hower, M.; Hellwig, K.; Hanses, F.; Wille, K.; et al. Use and effectiveness of remdesivir for the treatment of patients with covid-19 using data from the Lean European Open Survey on SARS-CoV-2 infected patients (LEOSS): A multicentre cohort study. Infection 2023, in press. [Google Scholar] [CrossRef]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Grundmann, A.; Wu, C.H.; Hardwick, M.; Baillie, J.K.; Openshaw, P.J.M.; Semple, M.G.; Böhning, D.; Pett, S.; Michael, B.D.; Thomas, R.H.; et al. Fewer COVID-19 Neurological Complications with Dexamethasone and Remdesivir. Ann. Neurol. 2023, 93, 88–102. [Google Scholar] [CrossRef] [PubMed]
- Kojima, Y.; Nakakubo, S.; Kamada, K.; Yamashita, Y.; Takei, N.; Nakamura, J.; Matsumoto, M.; Horii, H.; Sato, K.; Shima, H.; et al. Combination therapy with remdesivir and immunomodulators improves respiratory status in COVID-19: A retrospective study. J. Med. Virol. 2022, 94, 5702–5712. [Google Scholar] [CrossRef]
- Padilla, S.; Polotskaya, K.; Fernández, M.; Gonzalo-Jiménez, N.; de la Rica, A.; García, J.A.; García-Abellán, J.; Mascarell, P.; Gutiérrez, F.; Masiá, M. Survival benefit of remdesivir in hospitalized COVID-19 patients with high SARS-CoV-2 viral loads and low-grade systemic inflammation. J. Antimicrob. Chemother. 2022, 77, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Simmons, W.; Karmarkar, E.N.; Yoke, L.H.; Braimah, A.B.; Orozco, J.J.; Ghiuzeli, C.M.; Barnhill, S.; Sack, C.L.; Benditt, J.O.; et al. Successful Treatment of Prolonged, Severe Coronavirus Disease 2019 Lower Respiratory Tract Disease in a B cell Acute Lymphoblastic Leukemia Patient With an Extended Course of Remdesivir and Nirmatrelvir/Ritonavir. Clin. Infect. Dis. 2022, 76, 926–929. [Google Scholar] [CrossRef] [PubMed]
- Dioverti, M.V.; Gaston, D.C.; Morris, C.P.; Huff, C.A.; Jain, T.; Jones, R.; Anders, V.; Lederman, H.; Saunders, J.; Mostafa, H.H.; et al. Combination Therapy With Casirivimab/Imdevimab and Remdesivir for Protracted SARS-CoV-2 Infection in B-cell-Depleted Patients. Open Forum Infect. Dis. 2022, 9, ofac064. [Google Scholar] [CrossRef]
- Rajakumar, I.; Isaac, D.L.; Fine, N.M.; Clarke, B.; Ward, L.P.; Malott, R.J.; Pabbaraju, K.; Gill, K.; Berenger, B.M.; Lin, Y.-C.; et al. Extensive environmental contamination and prolonged severe acute respiratory coronavirus-2 (SARS CoV-2) viability in immunosuppressed recent heart transplant recipients with clinical and virologic benefit with remdesivir. Infect. Control Hosp. Epidemiol. 2022, 43, 817–819. [Google Scholar] [CrossRef] [PubMed]
- Baldi, F.; Dentone, C.; Mikulska, M.; Fenoglio, D.; Mirabella, M.; Magne, F.; Portunato, F.; Altosole, T.; Sepulcri, C.; Giacobbe, D.R.; et al. Case report: Sotrovimab, remdesivir and nirmatrelvir/ritonavir combination as salvage treatment option in two immunocompromised patients hospitalized for COVID-19. Front. Med. 2022, 9, 1062450. [Google Scholar] [CrossRef] [PubMed]
- Trottier, C.A.; Wong, B.; Kohli, R.; Boomsma, C.; Magro, F.; Kher, S.; Anderlind, C.; Golan, Y. Dual Antiviral Therapy for Persistent Coronavirus Disease 2019 and Associated Organizing Pneumonia in an Immunocompromised Host. Clin. Infect. Dis. 2023, 76, 923–925. [Google Scholar] [CrossRef] [PubMed]
- Buckland, M.S.; Galloway, J.B.; Fhogartaigh, C.N.; Meredith, L.; Provine, N.M.; Bloor, S.; Ogbe, A.; Zelek, W.M.; Smielewska, A.; Yakovleva, A.; et al. Treatment of COVID-19 with remdesivir in the absence of humoral immunity: A case report. Nat. Commun. 2020, 11, 6385. [Google Scholar] [CrossRef] [PubMed]
- Helleberg, M.; Niemann, C.U.; Moestrup, K.S.; Kirk, O.; Lebech, A.-M.; Lane, C.; Lundgren, J. Persistent COVID-19 in an Immunocompromised Patient Temporarily Responsive to Two Courses of Remdesivir Therapy. J. Infect. Dis. 2020, 222, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.A.; Chen, T.Y.; Choi, H.; Hwang, M.; Navarathna, D.; Hao, L.; Gale, M., Jr.; Camus, G.; Ramirez, H.E.; Jinadatha, C. Extended Remdesivir Infusion for Persistent Coronavirus Disease 2019 Infection. Open Forum Infect. Dis. 2022, 9, ofac382. [Google Scholar] [CrossRef]
- Camprubí, D.; Gaya, A.; Marcos, M.A.; Martí-Soler, H.; Soriano, A.; Mosquera, M.D.M.; Oliver, A.; Santos, M.; Muñoz, J.; García-Vidal, C. Persistent replication of SARS-CoV-2 in a severely immunocompromised patient treated with several courses of remdesivir. Int. J. Infect. Dis. 2021, 104, 379–381. [Google Scholar] [CrossRef]
- Fesu, D.; Bohacs, A.; Hidvegi, E.; Matics, Z.; Polivka, L.; Horvath, P.; Czaller, I.; Sutto, Z.; Eszes, N.; Vincze, K.; et al. Remdesivir in Solid Organ Recipients for COVID-19 Pneumonia. Transplant. Proc. 2022, 54, 2567–2569. [Google Scholar] [CrossRef] [PubMed]
- Colaneri, M.; Amarasinghe, N.; Rezzonico, L.; Pieri, T.C.; Segalini, E.; Sambo, M.; Roda, S.; Meloni, F.; Gregorini, M.; Rampino, T.; et al. Early remdesivir to prevent severe COVID-19 in recipients of solid organ transplant: A real-life study from Northern Italy. Int. J. Infect. Dis. 2022, 121, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Lafont, E.; Pere, H.; Lebeaux, D.; Cheminet, G.; Thervet, E.; Guillemain, R.; Flahault, A. Targeted SARS-CoV-2 treatment is associated with decreased mortality in immunocompromised patients with COVID-19. J. Antimicrob. Chemother. 2022, 77, 2688–2692. [Google Scholar] [CrossRef] [PubMed]
- Shields, A.M.; Anantharachagan, A.; Arumugakani, G.; Baker, K.; Bahal, S.; Baxendale, H.; Bermingham, W.; Bhole, M.; Boules, E.; Bright, P.; et al. Outcomes following SARS-CoV-2 infection in patients with primary and secondary immunodeficiency in the UK. Clin. Exp. Immunol. 2022, 209, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Park, S.D.; Jeon, Y.; Chung, Y.K.; Kwon, J.W.; Jeon, Y.H.; Jung, H.Y.; Park, S.H.; Kim, C.D.; Kim, Y.L.; et al. Clinical Effectiveness and Safety of Remdesivir in Hemodialysis Patients with COVID-19. Kidney Int. Rep. 2022, 7, 2522–2525. [Google Scholar] [CrossRef]
- Ackley, T.W.; McManus, D.; Topal, J.E.; Cicali, B.; Shah, S. A Valid Warning or Clinical Lore: An Evaluation of Safety Outcomes of Remdesivir in Patients with Impaired Renal Function from a Multicenter Matched Cohort. Antimicrob. Agents Chemother. 2021, 65, e02290-20. [Google Scholar] [CrossRef]
- Thakare, S.; Gandhi, C.; Modi, T.; Bose, S.; Deb, S.; Saxena, N.; Katyal, A.; Patil, A.; Patil, S.; Pajai, A.; et al. Safety of Remdesivir in Patients With Acute Kidney Injury or CKD. Kidney Int. Rep. 2021, 6, 206–210. [Google Scholar] [CrossRef]
- Kikuchi, K.; Nangaku, M.; Ryuzaki, M.; Yamakawa, T.; Yoshihiro, O.; Hanafusa, N.; Sakai, K.; Kanno, Y.; Ando, R.; Shinoda, T.; et al. Survival and predictive factors in dialysis patients with COVID-19 in Japan: A nationwide cohort study. Ren. Replace. Ther. 2021, 7, 59. [Google Scholar] [CrossRef]
- Pettit, N.N.; Pisano, J.; Nguyen, C.T.; Lew, A.K.; Hazra, A.; Sherer, R.; Mullane, K.M. Remdesivir Use in the Setting of Severe Renal Impairment: A Theoretical Concern or Real Risk? Clin. Infect. Dis. 2021, 73, e3990–e3995. [Google Scholar] [CrossRef]
- Aiswarya, D.; Arumugam, V.; Dineshkumar, T.; Gopalakrishnan, N.; Lamech, T.M.; Nithya, G.; Sastry, B.; Vathsalyan, P.; Dhanapriya, J.; Sakthirajan, R. Use of Remdesivir in Patients With COVID-19 on Hemodialysis: A Study of Safety and Tolerance. Kidney Int. Rep. 2021, 6, 586–593. [Google Scholar] [CrossRef]
- Elec, F.; Magnusson, J.; Elec, A.; Muntean, A.; Antal, O.; Moisoiu, T.; Cismaru, C.; Lupse, M.; Oltean, M. COVID-19 and kidney transplantation: The impact of remdesivir on renal function and outcome-a retrospective cohort study. Int. J. Infect. Dis. 2022, 118, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Butt, B.; Hussain, T.; Jarrar, M.; Khalid, K.; Albaker, W.; Ambreen, A.; Waheed, Y. Efficacy and Safety of Remdesivir in COVID-19 Positive Dialysis Patients. Antibiotics 2022, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Estiverne, C.; Strohbehn, I.A.; Mithani, Z.; Hirsch, J.S.; Wanchoo, R.; Goyal, P.G.; Lee Dryden-Peterson, S.; Pearson, J.C.; Kubiak, D.W.; Letourneau, A.R.; et al. Remdesivir in Patients With Estimated GFR <30 ml/min per 1.73 m(2) or on Renal Replacement Therapy. Kidney Int. Rep. 2021, 6, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Stancampiano, F.; Jhawar, N.; Alsafi, W.; Valery, J.; Harris, D.M.; Kempaiah, P.; Shah, S.; Heckman, M.G.; Siddiqui, H.; Libertin, C.R. Use of remdesivir for COVID-19 pneumonia in patients with advanced kidney disease: A retrospective multicenter study. Clin. Infect. Pract. 2022, 16, 100207. [Google Scholar] [CrossRef]
- Burwick, R.M.; Yawetz, S.; Stephenson, K.E.; Collier, A.-R.Y.; Sen, P.; Blackburn, B.G.; Kojic, E.M.; Hirshberg, A.; Suarez, J.F.; Sobieszczyk, M.E.; et al. Compassionate Use of Remdesivir in Pregnant Women With Severe Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 73, e3996–e4004. [Google Scholar] [CrossRef]
- Eid, J.; Abdelwahab, M.; Colburn, N.; Day, S.; Cackovic, M.; Rood, K.M.; Costantine, M.M. Early Administration of Remdesivir and Intensive Care Unit Admission in Hospitalized Pregnant Individuals With Coronavirus Disease 2019 (COVID-19). Obs. Gynecol. 2022, 139, 619–621. [Google Scholar] [CrossRef]
- Nasrallah, S.; Nguyen, A.Q.; Hitchings, L.; Wang, J.Q.; Hamade, S.; Maxwell, G.L.; Khoury, A.; Gomez, L.M. Pharmacological treatment in pregnant women with moderate symptoms of coronavirus disease 2019 (COVID-19) pneumonia. J. Matern. Fetal Neonatal Med. 2022, 35, 5970–5977. [Google Scholar] [CrossRef]
- Brooks, K.M.; Pinilla, M.; Stek, A.M.; Shapiro, D.E.; Barr, E.; Febo, I.L.; Paul, M.E.; Deville, J.G.; George, K.; Knowles, K.; et al. Pharmacokinetics of Tenofovir Alafenamide With Boosted Protease Inhibitors in Pregnant and Postpartum Women Living With HIV: Results From IMPAACT P1026s. J. Acquir. Immune Defic. Syndr. 2022, 90, 343–350. [Google Scholar] [CrossRef]
- Ahmed, A.; Rojo, P.; Agwu, A.; Kimberlin, D.; Deville, J.; Mendez-Echevarria, A.; Sue, P.K.; Galli, I.; Humeniuk, R.; Juneja, K.; et al. Remdesivir in the treatment of children 28 days to < 18 years of age hospitalised with COVID-19 in the CARAVAN study. Thorax 2022, 77, A172–A173. [Google Scholar]
- Goldman, D.L.; Aldrich, M.L.; Hagmann, S.H.F.; Bamford, A.; Camacho-Gonzalez, A.; Lapadula, G.; Lee, P.; Bonfanti, P.; Carter, C.C.; Zhao, Y.; et al. Compassionate Use of Remdesivir in Children With Severe COVID-19. Pediatrics 2021, 147, e2020047803. [Google Scholar] [CrossRef]
- Umemura, T.; Nishikawa, K.; Mutoh, Y.; Sasano, H.; Kozaki, K.; Yamada, T.; Ichihara, T. Usage experience of remdesivir for SARS-CoV-2 infection in a patient with chronic cirrhosis of Child–Pugh class C. J. Antimicrob. Chemother. 2021, 76, 1947–1948. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Rincon, J.M.; Lopez-Carmona, M.D.; Cobos-Palacios, L.; Lopez-Sampalo, A.; Rubio-Rivas, M.; Martin-Escalante, M.D.; de-Cossio-Tejido, S.; Taboada-Martinez, M.L.; Muino-Miguez, A.; Areses-Manrique, M.; et al. Remdesivir in Very Old Patients (>/=80 Years) Hospitalized with COVID-19: Real World Data from the SEMI-COVID-19 Registry. J. Clin. Med. 2022, 11, 3769. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Au, I.C.H.; Cheng, W.Y.; Man, K.K.C.; Lau, K.T.K.; Mak, L.Y.; Lui, S.L.; Chung, M.S.H.; Xiong, X.; Lau, E.H.Y.; et al. Remdesivir use and risks of acute kidney injury and acute liver injury among patients hospitalised with COVID-19: A self-controlled case series study. Aliment. Pharmacol. Ther. 2022, 56, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.C.; Marks, K.; Bruno, R.; Montejano, R.; Spinner, C.; Galli, M.; Ahn, M.Y.; Nahass, R.; et al. Impact of baseline alanine aminotransferase levels on the safety and efficacy of remdesivir in severe COVID-19 patients. Hepatology 2020, 72 (Suppl. 1), 279A. Available online: https://pesquisa.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/resource/pt/covidwho-986086 (accessed on 29 April 2023).
- Akinosoglou, K.; Schinas, G.; Rigopoulos, E.A.; Polyzou, E.; Tzouvelekis, A.; Adonakis, G.; Gogos, C. COVID-19 Pharmacotherapy in Pregnancy: A Literature Review of Current Therapeutic Choices. Viruses 2023, 15, 787. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.R.; Goldman, J.D.; Tuttle, K.R.; Teixeira, J.P.; Koullias, Y.; Llewellyn, J.; Zhao, Y.; Huang, H.; Hyland, R.H.; Osinusi, A.; et al. The REDPINE Study: Efficacy and Safety of Remdesivir in People With Moderately and Severely Reduced Kidney Function Hospitalised for COVID-19 Pneumonia. In Proceedings of the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Liu, X.I.; Dallmann, A.; Brooks, K.; Best, B.M.; Clarke, D.F.; Mirochnick, M.; van den Anker, J.N.; Capparelli, E.V.; Momper, J.D. Physiologically-based pharmacokinetic modeling of remdesivir and its metabolites in pregnant women with COVID-19. CPT Pharmacomet. Syst. Pharm. 2023, 12, 148–153. [Google Scholar] [CrossRef]
- Choi, B.; Choudhary, M.C.; Regan, J.; Sparks, J.A.; Padera, R.F.; Qiu, X.; Solomon, I.H.; Kuo, H.H.; Boucau, J.; Bowman, K.; et al. Persistence and Evolution of SARS-CoV-2 in an Immunocompromised Host. N. Engl. J. Med. 2020, 383, 2291–2293. [Google Scholar] [CrossRef]
- Mozaffari, E.C.A.; Chima-Melton, C.; Kalill, A.; Read, S.; Der-Torossian, C.; Dau, L.; Gupta, R.; Berry, M.; Gottlieb, R.L. Remdesivir is associated with lower mortality in cancer patients hospitalized for COVID-19 across emerging variants. In Proceedings of the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Lee, E.Y.; Goldman, J.D.; Berry, M.; Brown, G.; Abdelghany, M.; Chokkalingam, A. Remdesivir Reduces Readmission in Immunocompromised Adult Patients Hospitalised with COVID-19. In Proceedings of the European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Copenhagen, Denmark, 15–18 April 2023. [Google Scholar]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Parcha, V.; Booker, K.S.; Kalra, R.; Kuranz, S.; Berra, L.; Arora, G.; Arora, P. A retrospective cohort study of 12,306 pediatric COVID-19 patients in the United States. Sci. Rep. 2021, 11, 10231. [Google Scholar] [CrossRef]
- Gordon, C.J.; Tchesnokov, E.P.; Woolner, E.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; Götte, M. Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency. J. Biol. Chem. 2020, 295, 6785–6797. [Google Scholar] [CrossRef]
- Agostini Maria, L.; Andres Erica, L.; Sims Amy, C.; Graham Rachel, L.; Sheahan Timothy, P.; Lu, X.; Smith Everett, C.; Case James, B.; Feng Joy, Y.; Jordan, R.; et al. Coronavirus Susceptibility to the Antiviral Remdesivir (GS-5734) Is Mediated by the Viral Polymerase and the Proofreading Exoribonuclease. mBio 2018, 9, e00221-18. [Google Scholar] [CrossRef]
- Stevens, L.J.; Pruijssers, A.J.; Lee, H.W.; Gordon, C.J.; Tchesnokov, E.P.; Gribble, J.; George, A.S.; Hughes, T.M.; Lu, X.; Li, J.; et al. Mutations in the SARS-CoV-2 RNA-dependent RNA polymerase confer resistance to remdesivir by distinct mechanisms. Sci. Transl. Med. 2022, 14, eabo0718. [Google Scholar] [CrossRef] [PubMed]
- Focosi, D.; Maggi, F.; McConnell, S.; Casadevall, A. Very low levels of remdesivir resistance in SARS-COV-2 genomes after 18 months of massive usage during the COVID19 pandemic: A GISAID exploratory analysis. Antivir. Res. 2022, 198, 105247. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, S.; Klein, J.; Robertson, A.J.; Peña-Hernández, M.A.; Lin, M.J.; Roychoudhury, P.; Lu, P.; Fournier, J.; Ferguson, D.; Mohamed Bakhash, S.A.K.; et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. Nat. Commun. 2022, 13, 1547. [Google Scholar] [CrossRef] [PubMed]
- Martinot, M.; Jary, A.; Fafi-Kremer, S.; Leducq, V.; Delagreverie, H.; Garnier, M.; Pacanowski, J.; Mékinian, A.; Pirenne, F.; Tiberghien, P.; et al. Emerging RNA-Dependent RNA Polymerase Mutation in a Remdesivir-Treated B-cell Immunodeficient Patient With Protracted Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 73, e1762–e1765. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, L. Tissue distributions of antiviral drugs affect their capabilities of reducing viral loads in COVID-19 treatment. Eur. J. Pharmacol. 2020, 889, 173634. [Google Scholar] [CrossRef]
- Boshier, F.A.; Pang, J.; Penner, J.; Parker, M.; Alders, N.; Bamford, A.; Grandjean, L.; Grunewald, S.; Hatcher, J.; Best, T. Evolution of viral variants in remdesivir-treated and untreated SARS-CoV-2-infected pediatrics patients. J. Med. Virol. 2022, 94, 161–172. [Google Scholar] [CrossRef]
- Heyer, A.; Günther, T.; Robitaille, A.; Lütgehetmann, M.; Addo, M.M.; Jarczak, D.; Kluge, S.; Aepfelbacher, M.; Schulze zur Wiesch, J.; Fischer, N.; et al. Remdesivir-induced emergence of SARS-CoV2 variants in patients with prolonged infection. Cell Rep. Med. 2022, 3, 100735. [Google Scholar] [CrossRef]
- Hogan, J.I.; Duerr, R.; Dimartino, D.; Marier, C.; Hochman, S.; Mehta, S.; Wang, G.; Heguy, A. Remdesivir resistance in transplant recipients with persistent COVID-19. Clin. Infect. Dis. 2023, 76, 342–345. [Google Scholar] [CrossRef]
- Frost, M.T.; Jimenez-Solem, E.; Ankarfeldt, M.Z.; Nyeland, M.E.; Andreasen, A.H.; Petersen, T.S. The Adaptive COVID-19 Treatment Trial-1 (ACTT-1) in a real-world population: A comparative observational study. Crit. Care 2020, 24, 677. [Google Scholar] [CrossRef]
- Zamani, S.; Alizadeh, M.; Shahrestanaki, E.; Mohammadpoor Nami, S.; Qorbani, M.; Aalikhani, M.; Hassani Gelsefid, S.; Mohammadian Khonsari, N. Prognostic comparison of COVID-19 outpatients and inpatients treated with Remdesivr: A retrospective cohort study. PLoS ONE 2022, 17, e0277413. [Google Scholar] [CrossRef]
- Pereta, I.; Morancho, A.; Lopez, N.; Ibanez, B.; Salas, C.; Moreno, L.; Castells, E.; Barta, A.; Cubedo, M.; Coloma, E.; et al. Hospital at home treatment with remdesivir for patients with COVID-19: Real-life experience. Int. J. Infect. Dis. 2023, 127, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Checkmahomed, L.; Carbonneau, J.; Du Pont, V.; Riola, N.C.; Perry, J.K.; Li, J.; Paré, B.; Simpson, S.M.; Smith, M.A.; Porter, D.P.; et al. In Vitro Selection of Remdesivir-Resistant SARS-CoV-2 Demonstrates High Barrier to Resistance. Antimicrob. Agents Chemother. 2022, 66, e0019822. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, L.L.H.; Li, J.; Martin, R.; Han, D.; Xu, S.; Camus, G.; Perry, J.K.; Hyland, R.; Porter, D.P. Remdesivir Resistance Analyses From The Pinetree Study In Outpatients With COVID-19. In Proceedings of the 2023 Conference on Retroviruses and Opportunistic Infections, Seattle, WA, USA, 19–22 February 2023. [Google Scholar]
- Wang, Z.; Yang, L.; Song, X.Q. Oral GS-441524 derivatives: Next-generation inhibitors of SARS-CoV-2 RNA-dependent RNA polymerase. Front. Immunol. 2022, 13, 1015355. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Country of Origin | Population Characteristics | Number of Patients | Therapeutic Care | Endpoints |
|---|---|---|---|---|---|
| Immunocompromised individuals | |||||
| Ford, E. S., et al. (2022). Successful treatment of prolonged, severe COVID-19 lower respiratory tract disease in a B-cell ALL patient with an extended course of remdesivir and nirmatrelvir/ritonavir. Clin Infect Dis. [48] https://doi.org/10.1093/cid/ciac868 | USA | 40-year-old man B-cell acute lymphoblastic leukemia with complete remission Under chemotherapy Prophylaxis with Casirivimab and Imdevimab prolonged, persistent, and severe lower respiratory tract COVID-19 | 1 | Multiple therapies tried 10 days IV remdesivir, dexamethasone, and nirmatrelvir/ritonavir 20 days nirmatrelvir/ritonavir | Virus remained detectable by BAL, and oxygen requirement returned after 10 days of nirmatrelvir/ritonavir in combination with remdesivir Sustained improvement and clinical cure: 20 days of nirmatrelvir/ritonavir |
| Dioverti, M. V., et al. (2022). Combination Therapy With Casirivimab/Imdevimab and Remdesivir for Protracted SARS-CoV-2 Infection in B-cell-Depleted Patients. Open forum infectious diseases, 9(6), ofac064. [49] https://doi.org/10.1093/ofid/ofac064 | USA | B-cell-depleted patients | 3 | Patient 1: Casirivimab/Imdevimab on day 70 Remdesivir on days 75–79 Patient 2: Casirivimab/Imdevimab on day 111 Remdesivir on days 115–119 Patient 3: Casirivimab/Imdevimab on day 47 Remdesivir on days 46–50 | Patient 1: SARS-CoV-2 test negative on day 84 Resolution of cough by 2 weeks Normalization of chest CT by 4 weeks Leukopenia/ neutropenia normalized by 2 weeks Clinically well 10 months after treatment Patient 2: Negative test on day 146 Clinically well 10 months after treatment Patient 3: Negative test on day 64 Clinically well 8 months after treatment |
| Rajakumar, I., et al. (2022). Extensive environmental contamination and prolonged severe acute respiratory coronavirus-2 (SARS CoV-2) viability in immunosuppressed recent heart transplant recipients with clinical and virologic benefit with remdesivir. Infection Control & Hospital Epidemiology, 43(6), 817–819. [50] https://doi.org/10.1017/ice.2021.89 | UK | Immunosuppressed recent heart transplant recipients with benefit with remdesivir | 2 | Case 1: 10 day course of remdesivir on day 23 Case 2: 5 day course of remdesivir on day 16 | Case 1: clinical condition and chest radiograph improved by day 44 Case 2: Clinical recovery and discharge on day 23 |
| Baldi, F., et al. (2023). Case report: Sotrovimab, remdesivir and nirmatrelvir/ritonavir combination as salvage treatment option in two immunocompromised patients hospitalized for COVID-19. Frontiers in medicine, 9, 1062450. [51] https://doi.org/10.3389/fmed.2022.1062450 | Italy | Immunocompromised individuals treated with rituximab in need of hospitalization for COVID-19 | 2 Case1: non-Hodgkin lymphoma Case 2: granulomatosis with polyangiitis | A single infusion of IV sotrovimab 500 mg, a 7-day course of IV remdesivir (200 mg of loading dose, 100 mg of maintenance dose) plus 5 days of oral nirmatrelvir/ritonavir 300 mg/100 mg q12h. Case 1: On day 7: initiation of treatment plus IV corticosteroids Case 2: On day 6: initiation of treatment | Case 1: clinical improvement on day 9, no need for oxygen supplementation by day 13. Discharged on day 17 Case 2: clinical improvement on day 11, no need for oxygen supplementation by day 12. Discharged on day 14 |
| Trottier, C. A., et al. (2023). Dual Antiviral Therapy for Persistent Coronavirus Disease 2019 and Associated Organizing Pneumonia in an Immunocompromised Host. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 76(5), 923–925. [52] https://doi.org/10.1093/cid/ciac847 | USA | Immunocompromised patient with chronic lymphocytic leukemia with persistent COVID-19 | 1 | First admission: 10 days of remdesivir plus iv corticosteroids. Second admission: received bebtelovimab Third admission: IV corticosteroids with remdesivir and nirmatrelvir/ritonavir for 20 days | First admission: Clinical improvement, relapse in one month. Readmitted two months later Second admission: Clinical improvement, relapse in one month and readmission Third admission: Clinical improvement by day 3 By day 9, discharged No relapse and no adverse events two months later. |
| Buckland, M. S., et al. (2020). Treatment of COVID-19 with remdesivir in the absence of humoral immunity: a case report. Nature communications, 11(1), 6385. [53] https://doi.org/10.1038/s41467-020-19761-2 | UK | Patient with genetic antibody deficiency X-linked agammaglobulinemia (XLA) with persistent COVID-19 | 1 | 10 days of remdesivir on day 34 Readmitted on day 54 10 more days of remdesivir on day 61 | First admission: Fever, dyspnea improved by 36 h Nausea, vomiting ceased Oxygen saturation raised CRP decreased Rise in lymphocyte count Improved CT findings Discharged on day 43 Second admission: Similar results Discharged on day 73 |
| Helleberg, M., et al. (2020). Persistent COVID-19 in an Immunocompromised Patient Temporarily Responsive to Two Courses of Remdesivir Therapy. The Journal of infectious diseases, 222(7), 1103–1107. [54] https://doi.org/10.1093/infdis/jiaa446 | Denmark | Immunocompromised patient due to treatment for chronic lymphocytic leukemia with persistent COVID-19 with high fever and severe pneumonia | 1 | Two 10-day courses of remdesivir (200 mg first dose and 100 mg per day after) On day 24 and day 45 | First treatment course (days 26–35): On day 26: Fever abated General condition improved Discharged on day 35 Relapsed and readmitted on day 36 Second treatment course (days 45–54) Afebrile on day 46 Discharged on day 54 with negative nasal swab On day 55: Fever recurred Readmitted with positive test On day 58, the patient received convalescent plasma Discharged on day 65 |
| Biscarini, S., et al. (2022). Safety Profile and Outcomes of Early COVID-19 Treatments in Immunocompromised Patients: A Single-Centre Cohort Study. Biomedicines, 10(8), 2002. [32] https://doi.org/10.3390/biomedicines10082002 | Italy | Non-hospitalized people who received early treatment with remdesivir or monoclonal antibodies | 143 106/143 (74.1%) immunocompromised (41 solid organ transplant recipients, 6 hematopoietic stem cell transplant recipients) 37/143 not immunocompromised | 23 treated with remdesivir 122 treated with monoclonal antibodies 2 treated with both | There were no statistically significant differences between the two groups in AEs (23/143 or 16.1%) Mean duration of symptoms after treatment onset: 2.5 days (IQR: 1.0–6.0) molecular swab positivity: 10 days (IQR: 6–16) Clinical outcome: hospital or ICU admission: 5/143 (3.5%) mortality: 1/143 (0.7%) |
| Martinez, M. A., et al. (2022). Extended Remdesivir Infusion for Persistent Coronavirus Disease 2019 Infection. Open Forum Infectious Diseases, 9(8), ofac382. [55] https://doi.org/10.1093/ofid/ofac382 | USA | Immunocompromised patient with granulomatosis with polyangiitis and secondary hypogammaglobulinemia treated with multiple immunocompromising agents | 1 | First admission: remdesivir IV for 5 days plus corticosteroids IV for 10 days Second admission on day 18: Convalescent plasma Third admission on day 52: Only antibiotic therapy Fourth admission on day 75: remdesivir and IV corticosteroids on day 94 for 10 days Fifth admission on day 110: convalescent plasma and remdesivir for 30 days | After 30 days of remdesivir treatment on the fifth admission, the patient was discharged on day 142. At 12-month follow-up: No major adverse events reported No relapse at 12-month follow-up |
| Camprubí, D., et al. (2021). Persistent replication of SARS-CoV-2 in a severely immunocompromised patient treated with several courses of remdesivir. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases, 104, 379–381. [56] https://doi.org/10.1016/j.ijid.2020.12.050 | Spain | Severely immunocompromised patient in treatment for stage IV-A follicular lymphoma | 1 | 200 mg first dose and 100 mg per day for 8 days On day 28, a single dose of remdesivir was accidentally administered 10-day course of remdesivir at second admission | First treatment course (days 28–36): Discharged on day 36 Relapsed and readmitted on day 39 Afebrile 1 day after the accidental remdesivir admission Second treatment course: Rapid clinical improvement Fever resolved Short courses of remdesivir might be insufficient for treating high-risk populations |
| Fesu, D., et al. (2022). Remdesivir in Solid Organ Recipients for COVID-19 Pneumonia. Transplantation proceedings, 54(9), 2567–2569. [57] https://doi.org/10.1016/j.transproceed.2022.10.043 | Hungary | Solid organ transplant recipients Mean age 53.2 ± 12.7 Control group: non-transplanted patients who received remdesivir (RDV group) and standard of care (SOC group) | 25 transplant recipients (lung: 19; kidney: 3; liver: 2; heart: 1) | 15/25 treated with remdesivir (RDV-TX group) 10/25 received standard of care treatment (SOC-TX) | Safety and efficacy of remdesivir was assessed: worse clinical score was noted in RDV patients compared with RDV-TX transfer to ICU was worse in RDV-TX group compared to RDV 60-day survival was worse in RDV-TX group compared to RDV All 60-day fatalities were among the lung transplant recipients (6/19) No AEs were noted related to remdesivir therapy Remdesivir use was safe in solid organ transplant recipients; however, outcome was significantly worse compared to the non-transplanted individuals |
| Colaneri, M., et al. (2022). Early remdesivir to prevent severe COVID-19 in recipients of solid organ transplant: a real-life study from Northern Italy. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases, 121, 157–160. [58] https://doi.org/10.1016/j.ijid.2022.05.001 | Italy | Outpatient solid organ transplant recipients who received and did not receive pre-emptive remdesivir were evaluated | 24 7/24 (29.1%) treated with pre-emptive remdesivir | 3-day course of remdesivir to prevent hospitalization. | Remdesivir prevented hospitalization at day 28 after the positive test: Hospitalization or COVID-19 worsening: remdesivir group 0/7 vs. non-remdesivir group 9/17 (1/9 ICU admission) (aHR 0.05; CI [0.00–0.65], p-value = 0.01) Time to negative SARS-CoV-2 RT-PCR swab test result was shortened No differences between the two groups was found (p-value = 0.86). |
| Lafont, E., et al. (2022). Targeted SARS-CoV-2 treatment is associated with decreased mortality in immunocompromised patients with COVID-19. The Journal of antimicrobial chemotherapy, 77(10), 2688–2692. [59] https://doi.org/10.1093/jac/dkac253 | France | Immunocompromised patients with COVID-19 | 67 | 10 did not receive targeted treatment 22 remdesivir 16 sotrovimab 13 tixagevimab/cilgavimab 1 Casirivimab/Imdevimab | Mortality after targeted treatment vs. no targeted treatment and safety of use: Mortality: Significantly lower in treatment patients [n = 0 (0%) vs. n = 2 (20%); p = 0.034] Safety: No severe adverse events were reported among treated patients Targeted COVID-19 treatment is safe and efficient and could be proposed in high-risk immunocompromised patients. |
| Shields, A. M., et al. (2022). Outcomes following SARS-CoV-2 infection in patients with primary and secondary immunodeficiency in the UK. Clinical and experimental immunology, 209(3), 247–258. [60] https://doi.org/10.1093/cei/uxac008 | UK | Patients with primary (PID) and secondary immunodeficiency (SID) and COVID-19 | 310 | 33 received targeted treatment 26/33 received remdesivir | Mortality rate 55/310 (17.7%) CVID: Infection fatality rate (IFR): 17/93 (18.3%) PID: IFR: 26/159 (16.3%) SID: IFR: 25/92 (27.2%) |
| Patients with impaired renal function | |||||
| Lim, J. H., et al. (2022). “Clinical Effectiveness and Safety of Remdesivir in Hemodialysis Patients with COVID-19.” Kidney Int Rep 7(11): 2522–2525. [61] https://www.ncbi.nlm.nih.gov/pubmed/36105653 | South Korea | Mean age: 68.5 ± 12.8 years 66.1% male hospitalized patients with COVID-19 who are on hemodialysis | 118 in total 44 received remdesivir 74 did not receive remdesivir | Remdesivir at half the standard dose Loading dose 100 mg Maintenance dose was 50 mg for the next 2 to 4 days | The remdesivir group had a tendency of more severe disease (p = 0.058) The NEWS on the day of hospitalization was significantly higher in the remdesivir group (p = 0.026) Mortality: 1/44 [2.3%] vs. 5/74 [6.8%] (p = 0.284) The composite outcome of mortality, use of a high-flow nasal cannula, and transfer to the intensive care unit occurred less frequently in the remdesivir group (1 [2.3%] vs. 10 [13.5%], p = 0.042) Disease severity aggravation rate was lower in the remdesivir group (3 [6.8%] vs. 15 [20.3%], p = 0.049) |
| Ackley, T. W., et al. (2021). A Valid Warning or Clinical Lore: an Evaluation of Safety Outcomes of Remdesivir in Patients with Impaired Renal Function from a Multicenter Matched Cohort. Antimicrobial agents and chemotherapy, 65(2), e02290-20. [62] https://doi.org/10.1128/AAC.02290-20 | USA | Hospitalized patients with SARS-CoV-2 with impaired renal function Group 1: patients with an estimated creatinine clearance (eCrCl) of <30 mL/min (median, 80 years [64 to 89]) Group 2: eCrCl of ≥30 mL/min (median, 62 years [54 to 74]) | 359 in total 347 included N (Group 1) = 40 N (Group 2) = 307 | Days of remdesivir: Group 1: median 5 [IQR 4–5] Group 2: median 5 [IQR 5–5] | No significant difference in the frequency of end of treatment AKI (5% versus 2.3%; p = 0.283) or early discontinuation due to abnormal liver function tests (LFTs) (0% versus 3.9%; p = 0.374) Mortality rate was higher in group 1 (50% versus 16.2%; p < 0.001) |
| Thakare, S., et al. (2021). Safety of Remdesivir in Patients With Acute Kidney Injury or CKD. Kidney international reports, 6(1), 206–210. [63] https://doi.org/10.1016/j.ekir.2020.10.005 | India | Patients With acute kidney injury or CKD | 157 in total, 46 received remdesivir, 8/46 were kidney transplant recipients | Remdesivir was administered as a total dose of 600 mg (200 mg on day 1, followed by 100 mg/day) 2 patients received 1200 mg because satisfactory clinical improvement was not observed | AST/ALT levels: baseline test abnormalities in 14/46 (30.4%) 12/14 improved by the end of the therapy Stable test results in 28/46 (60.9%) 3/46 (6.5%) newly occurring test abnormalities during therapy Clinical outcomes: 14/46 (30.4%) died 24/46 (52.2%) recovered 8/46 (17.3%) still admitted No renal function abnormalities attributable to the drug were observed |
| Kikuchi, K., et al. (2021). Survival and predictive factors in dialysis patients with COVID-19 in Japan: a nationwide cohort study. Renal replacement therapy, 7(1), 59. [64] https://doi.org/10.1186/s41100-021-00378-0 | Japan | Patients on dialysis with COVID-19 | 1948 in total 1010 included 392 analyzed for the efficacy of remdesivir | 98/392 received remdesivir 294/392 did not receive remdesivir | Mortality risk: increased with age (p < 0.001). significantly higher in patients with peripheral arterial disease (HR: 1.49, 95% CI: 1.05–2.10) significantly lower in patients who were treated with remdesivir (HR: 0.60, 95% CI: 0.37–0.98) increased with increase in BMI, increased with increase in CRP, decreased with increase in albumin. Length of stay: 20.9 ± 13.2 days in the remdesivir group, 16.2 ± 8.1 days in the other group (Difference: 4.7 days, 95% CI: 2.2–7.4, p < 0.001). Clinical outcomes 699/1010 (69.2%) recovered 311/1010 (30.8%) died |
| Pettit, N. N., et al. (2021). Remdesivir Use in the Setting of Severe Renal Impairment: A Theoretical Concern or Real Risk?. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 73(11), e3990–e3995. [65] https://doi.org/10.1093/cid/ciaa1851 | USA | Hospitalized patients (median age: 50) and patients with severe renal impairment (SRI, creatinine clearance < 30 mL/min or requiring renal replacement therapy) (median age: 74) | 137 in total 135 included N(SRI) = 20 | 5-day course of remdesivir | Safety assessment of remdesivir in patients with SRI: The incidence of possible AEs was 30% among those with SRI vs. 11% without (p = 0.06). Liver function test (LFT) elevations occurred in 10% vs. 4% (p = 0.28) Serum creatinine (SCr) elevations in 27% vs. 6% (p = 0.02) Mortality and length of stay were consistent with historical controls. The use of remdesivir in this small series of patients with SRI appeared to be relatively safe |
| Aiswarya, D., et al. (2021). Use of Remdesivir in Patients With COVID-19 on Hemodialysis: A Study of Safety and Tolerance. Kidney international reports, 6(3), 586–593. [66] https://doi.org/10.1016/j.ekir.2020.12.003 | India | Dialysis-dependent patients with COVID-19 Mean age 50.1 ± 12.2 years | 48 38 men 10 women | 100 mg of remdesivir 4 h before dialysis Max. of 6 doses | Before and after treatment comparison: Liver function: No events of significant alterations CRP: significant decline was noted (p = 0.001) O2 requirements: 68.6% improved Length of stay: shortened by mean 5.5 days (p = 0.001) |
| Elec, F., et al. (2022). COVID-19 and kidney transplantation: the impact of remdesivir on renal function and outcome—a retrospective cohort study. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases, 118, 247–253. [67] https://doi.org/10.1016/j.ijid.2022.03.015 | Romania | Kidney transplant recipients | 165 | 200 mg of remdesivir on day 1 followed by 100 mg for 2 to 10 days 5-day course for 38/165 Standard of care for 127/165 | Impact of remdesivir on: Overall mortality: no difference (18% vs. 23%, p > 0.05) ICU mortality: significant reduction (39% vs. 83%, p < 0.05) Incidence of AKI: no difference (50% vs. 43%, p > 0.05) Discharge eGFR values: significant improvement (57 ± 23 vs. 44 ± 22, p < 0.05) |
| Butt B, et al. Efficacy and Safety of Remdesivir in COVID-19 Positive Dialysis Patients. Antibiotics. 2022; 11(2):156. [68] https://doi.org/10.3390/antibiotics11020156 | Pakistan Saudi Arabia | Patients in dialysis with COVID-19 | 83 51/83 received remdesivir within 2 days of symptom onset 32/83 received remdesivir more than 2 days after symptom onset | 100 mg of remdesivir before hemodialysis | Mortality rate: Remdesivir did not reduce the overall mortality (76/83 or 91.5% survived while 7/83 or 8.4% died) Serum CRP (p = 0.028) and total leucocyte count (p = 0.013) increased 30-day mortality Compared remdesivir administration within 2 days versus after more than 2 days: Length of hospitalization was lower (p = 0.03) in the first group Nasal swabs were negative earlier (p = 0.001) in the first group Adverse events: No major AEs observed |
| Estiverne, C., et al. (2021). Remdesivir in Patients With Estimated GFR < 30 mL/min per 1.73 m2 or on Renal Replacement Therapy. Kidney international reports, 6(3), 835–838. [69] https://doi.org/10.1016/j.ekir.2020.11.025 | USA | COVID-19 positive patients with eGFR < 30 mL/min or on renal replacement therapy Median age 63 (IQR 55–76) | 18 13 with low eGFR 5/13 AKI 8/13 stable chronic kidney disease 5 received renal replacement therapy 11 already in ICU 9 already in need of mechanical ventilation | 200 mg first dose and then 100 mg per day | AEs after remdesivir treatment: Changes in ALT: 2 patients developed >5 times ALT levels not attributed to remdesivir Changes in serum creatinine: 8/13 improved creatinine levels 5/13 worsened creatinine levels (in 1 case attributed to remdesivir Overall mortality: 8/18 on day 28 All non-ICU patients survived |
| Stancampiano, F., et al. (2022). Use of remdesivir for COVID-19 pneumonia in patients with advanced kidney disease: A retrospective multicenter study. Clinical infection in practice, 16, 100207. [70] https://doi.org/10.1016/j.clinpr.2022.100207 | USA | Patients with advanced kidney disease (eGFR < 30) Median age 72 (21–100) | 444 114 (25.7%) with stage 3 CKD 229 with stage 4 CKD (51.6%) 101 with stage 5 CKD (22.7%) | 200 mg first dose and 100 mg per day for 5 days total | Clinical outcomes: ICU admissions: 146/444 (32.9%) Deaths 103/444 (23.2%) Patients in need of dialysis during treatment: 120/444 (27%) AEs did not differ between stage groups (p = 0.12) Stage 3 CKD: 20.9% Stage 4 CKD: 30.2% Stage 5 CKD: 32.3% Suggests that the use of remdesivir is safe in patients with severe CKD |
| Pregnant women | |||||
| Burwick, R. M., et al. (2021). Compassionate Use of Remdesivir in Pregnant Women With Severe Coronavirus Disease 2019. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 73(11), e3996–e4004. [71] https://doi.org/10.1093/cid/ciaa1466 | USA | Pregnant women with severe COVID-19 (saturation ≤ 94%) | 86 19/86 delivered before the initiation of remdesivir (postpartum group) 67/86 in pregnant group | 200 mg of remdesivir on day 1 followed by 100 mg for 2 to 10 days | Invasive ventilation required: 40% of pregnant women 95% of postpartum women At 28-day follow-up, oxygen requirement decreased in 96% of pregnant women 89% of postpartum Among women on mechanical ventilation: Pregnant group 93% extubated 93% recovered 90% discharged Postpartum group 89% extubated 89% recovered 84% discharged There was 1 maternal death attributed to neonatal disease There were no neonatal deaths recorded There was low incidence of serious AEs (16%) |
| Eid, J., et al. (2022). Early Administration of Remdesivir and Intensive Care Unit Admission in Hospitalized Pregnant Individuals With Coronavirus Disease 2019 (COVID-19). Obstetrics and gynecology, 139(4), 619–621. [72] https://doi.org/10.1097/AOG.0000000000004734 | USA | Hospitalized pregnant women with COVID-19 All of them unvaccinated | 41 Divided into groups by day of initiation of remdesivir Early group (<7 days after the onset of symptoms) N = 24 Late group (≥7 days after the onset of symptoms) N = 17 | Early group: mean duration of therapy: 3 days (1–6 days) Late group: mean duration of therapy: 9 days (7–14 days) | Comparison between early and late groups showed Lower ICU admission rate: 21% vs. 59% (OR: 0.18 [95% CI: 0.04–0.72]) Lower length of hospital stay: 5 [IQR 4–5.75] vs. 11 [IQR 4.5–15.5] p < 0.01 Decreased progression to critical disease: 12% vs. 4% (OR: 0.20 [95% CI: 0.51–0.87]) |
| Nasrallah, S., et al. (2022). Pharmacological treatment in pregnant women with moderate symptoms of coronavirus disease 2019 (COVID-19) pneumonia. The journal of maternal-fetal & neonatal medicine: the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 35(25), 5970–5977. [73] https://doi.org/10.1080/14767058.2021.1903426 | USA | Pregnant women hospitalized with moderate COVID-19 | 748 in total 35 included 17 received remdesivir within 48 h of hospitalization (15/17 with moderate symptoms, 2/17 with critical COVID-19) 7 received remdesivir >48 h of hospitalization 11 did not receive remdesivir | 5-day course of remdesivir, antibiotics and/or glucocorticoids | Clinical recovery on day 7 17/17 recovered 7/7 required supplemental oxygen 3/11 recovered Clinical recovery significance between groups: p < 0.001 |
| Brooks, K. M., et al. IMPAACT 2032: remdesivir pk & safety in pregnant and non-pregnant women with COVID-19. Topics in Antiviral Medicine; 30(1 SUPPL):267, 2022. [74] https://pesquisa.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/resource/en/covidwho-1880041 | USA | Pregnant and non-pregnant women with COVID-19 | 18 in total 10 pregnant (3/10 discontinued early) | 200 mg of remdesivir on day 1 followed by 100 mg for 5 to 10 days | Preliminary results were comparable between pregnant and non-pregnant women, but no formal statistical comparisons were made. |
| Pediatric population | |||||
| Ahmed, A., et al. (2022). P168 Remdesivir in the treatment of children 28 days to <18 years of age hospitalised with COVID-19 in the CARAVAN study. Thorax, 77 (Suppl 1), A172–A173. [75] https://doi.org/10.1136/thorax-2022-BTSabstracts.302 | USA | Hospitalized children with PCR-confirmed COVID-19 | 53 76% in need of supplemental oxygen (23% invasive ventilation) | 10-day course of IV remdesivir 200 mg on day 1 and 100 mg daily subsequently for children ≥40 kg 5 mg/kg on day 1 and 2.5 mg/kg daily subsequently for children weighing 3 to <40 kg | Clinical outcomes from day 1 to 10 or until discharge and 30-day follow-up On day 10: 75% clinical improvement 60% were discharged By day 30: 85% clinical improvement 83% were discharged A total of 3 deaths documented The incidence of severe adverse events was 21% (none was drug related) |
| Goldman, D. L., et al. (2021). Compassionate Use of Remdesivir in Children With Severe COVID-19. Pediatrics, 147(5), e2020047803. [76] https://doi.org/10.1542/peds.2020-047803 | USA | Hospitalized COVID-19 patients under 18 years old | 77 | 10-day course of IV remdesivir 200 mg on day 1 and 100 mg daily subsequently for children ≥40 kg 5 mg/kg on day 1 and 2.5 mg/kg daily subsequently for children <40 kg | At baseline: 90% required oxygen supplementation 51% required invasive ventilation By 28-day follow-up: 88% had decreased oxygen supplementation needs 83% recovered 73% were discharged Among those in need of invasive ventilation: 90% were extubated 80% recovered 67% were discharged A total of 4 deaths documented There was a low incidence of serious adverse events (16%) |
| Various populations | |||||
| Umemura T., et al. Usage experience of remdesivir for SARS-CoV-2 infection in a patient with chronic cirrhosis of Child–Pugh class C, Journal of Antimicrobial Chemotherapy, Volume 76, Issue 7, July 2021, Pages 1947–1948, [77] https://doi.org/10.1093/jac/dkab076 | Japan | Patient with chronic cirrhosis of Child-Pugh class C | 1 | 200 mg first dose and 100 mg per day for 5 days + dexamethasone | On day 4: Fever resolved Respiratory rate normalized On day 12: Oxygen saturation normalized Discharged on day 20 No change found in liver function up to day 39 |
| Ramos-Rincon, J. M., et al. On Behalf Of The Semi-COVID-Network (2022). Remdesivir in Very Old Patients (≥80 Years) Hospitalized with COVID-19: Real World Data from the SEMI-COVID-19 Registry. Journal of clinical medicine, 11(13), 3769. [78] https://doi.org/10.3390/jcm11133769 | Spain | Patients ≥ 80 years old with COVID-19 | 4431 admitted 1312 (30.3%) included (≥80 years old) | 140/1312 (10.7%) treated with remdesivir 18/140 treated for 3 days 107/140 treated for 4–5 days 11/140 treated for >5 days | Mortality and 30-day all-cause mortality were lower in remdesivir group vs. control group (p < 0.001): Mortality was lower in remdesivir group (OR: 0.45 [95% CI: 0.29–0.69]) 30-day all-cause mortality was lower in remdesivir group (adjusted OR: 0.40 [95% CI: 0.22–0.61]) |
| Wong, C. K. H., et al. (2022). Remdesivir use and risks of acute kidney injury and acute liver injury among patients hospitalised with COVID-19: a self-controlled case series study. Alimentary pharmacology & therapeutics, 56(1), 121–130. [79] https://doi.org/10.1111/apt.16894 | China | Patients hospitalized with COVID-19 | 10.412 in total 860 included | 200 mg of remdesivir on day 1 followed by 100 mg for 4 days or until discharge | Risk of ALI, AKI associated with remdesivir: ALI: 334/860 (38.8%) AKI: 137/860 (15.9%) No significantly higher risk with remdesivir use: In the first 2 days: ALI: IRR = 1.261 [95% CI: 0.915–1.737] AKI: IRR = 1.261 [95% CI: 0.899–1.789] Between days 2 and 5: ALI: IRR = 1.087 [95% CI: 0.793–1.489] AKI: IRR = 1.152 [95% CI: 0.821–1.616] |
| Goldman, J. D., et al. Impact of baseline alanine aminotransferase levels on the safety and efficacy of remdesivir in severe COVID-19 patients. Hepatology; 72(1 SUPPL):279A, 2020. [80] https://pesquisa.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/resource/pt/covidwho-986086 | USA | Patients with severe COVID-19 | 397 215 had elevated baseline ALT at initiation of treatment | 5- or 10-day course of treatment with remdesivir | AEs and clinical outcomes after treatment: Incidence of serious AEs was similar between groups Hepatobiliary AEs were higher in the high ALT group: 8.8% vs. 3.3% (p = 0.068) Symptom duration was longer in the high ALT group (p < 0.001) Time to clinical recovery, clinical improvement, and death were similar between groups In severe COVID-19 patients, adverse events and clinical outcomes after RDV initiation were similar among patients with baseline normal ALT and those with elevated ALT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akinosoglou, K.; Rigopoulos, E.A.; Schinas, G.; Kaiafa, G.; Polyzou, E.; Tsoupra, S.; Tzouvelekis, A.; Gogos, C.; Savopoulos, C. Remdesivir Use in the Real-World Setting: An Overview of Available Evidence. Viruses 2023, 15, 1167. https://doi.org/10.3390/v15051167
Akinosoglou K, Rigopoulos EA, Schinas G, Kaiafa G, Polyzou E, Tsoupra S, Tzouvelekis A, Gogos C, Savopoulos C. Remdesivir Use in the Real-World Setting: An Overview of Available Evidence. Viruses. 2023; 15(5):1167. https://doi.org/10.3390/v15051167
Chicago/Turabian StyleAkinosoglou, Karolina, Emmanouil Angelos Rigopoulos, Georgios Schinas, Georgia Kaiafa, Eleni Polyzou, Stamatia Tsoupra, Argyrios Tzouvelekis, Charalambos Gogos, and Christos Savopoulos. 2023. "Remdesivir Use in the Real-World Setting: An Overview of Available Evidence" Viruses 15, no. 5: 1167. https://doi.org/10.3390/v15051167