

SARS-CoV-2 Antibody Response and Sustainability after a Third Dose of BNT162b2 in Healthcare Workers at Health Promotion Centers
 ,
,
Abstract
:1. Introductions
2. Materials and Methods
2.1. Study Design and Participants
2.2. Receptor-Binding Domain (RBD) IgG Measurement for Anti-SARS-CoV-2 Spike Protein
2.3. Statistical Analyses
3. Results
3.1. Characteristics of the Study Participants
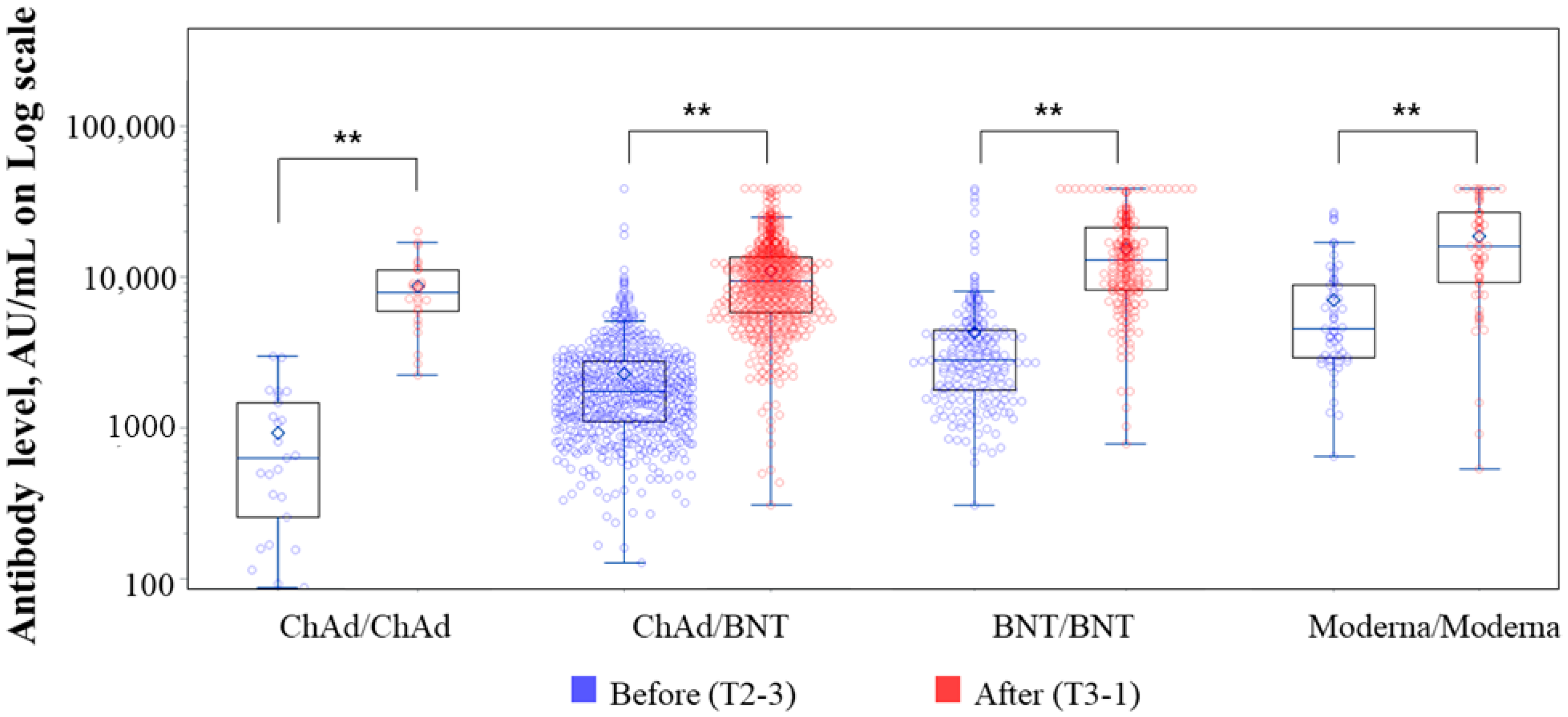
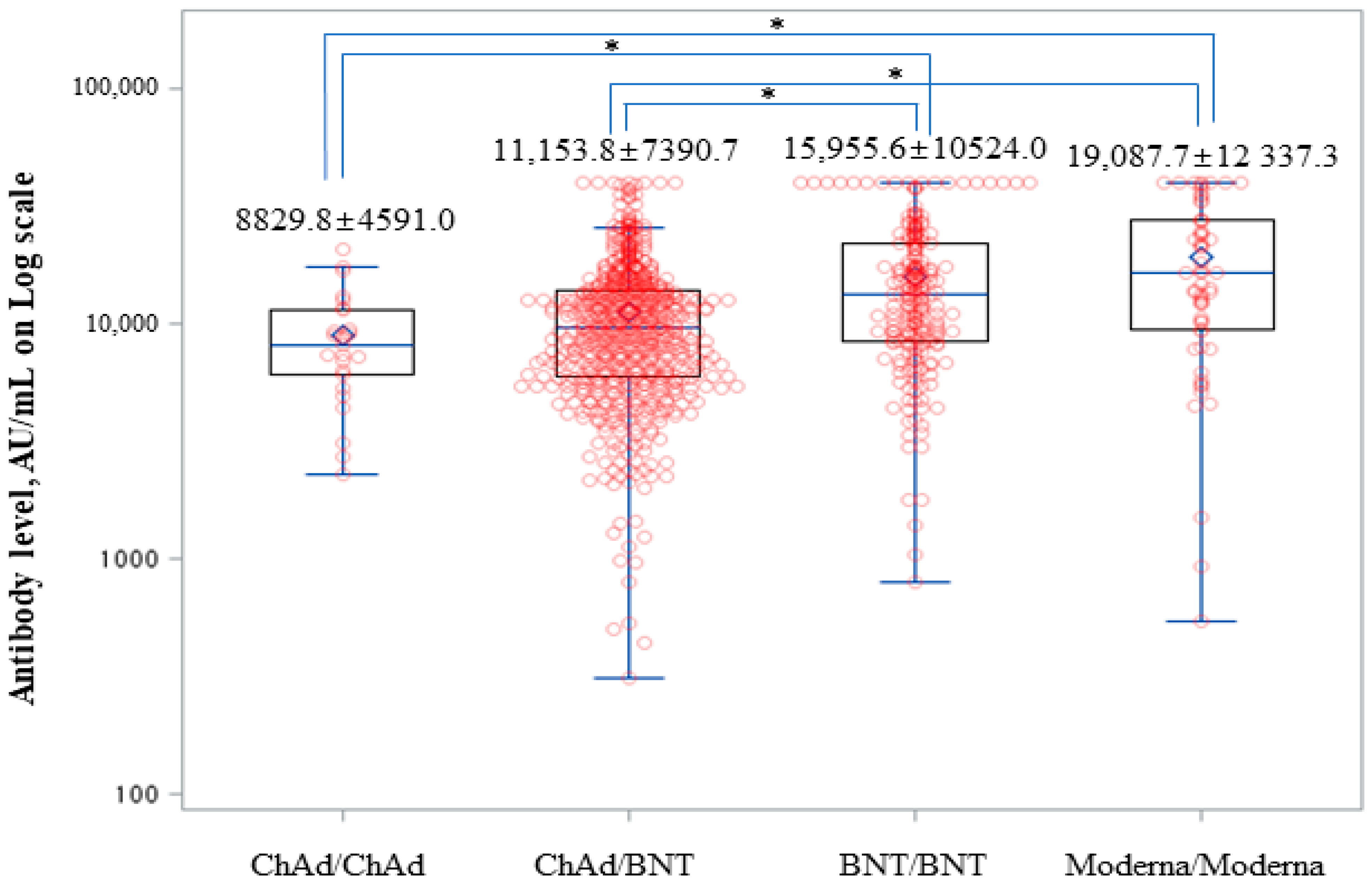
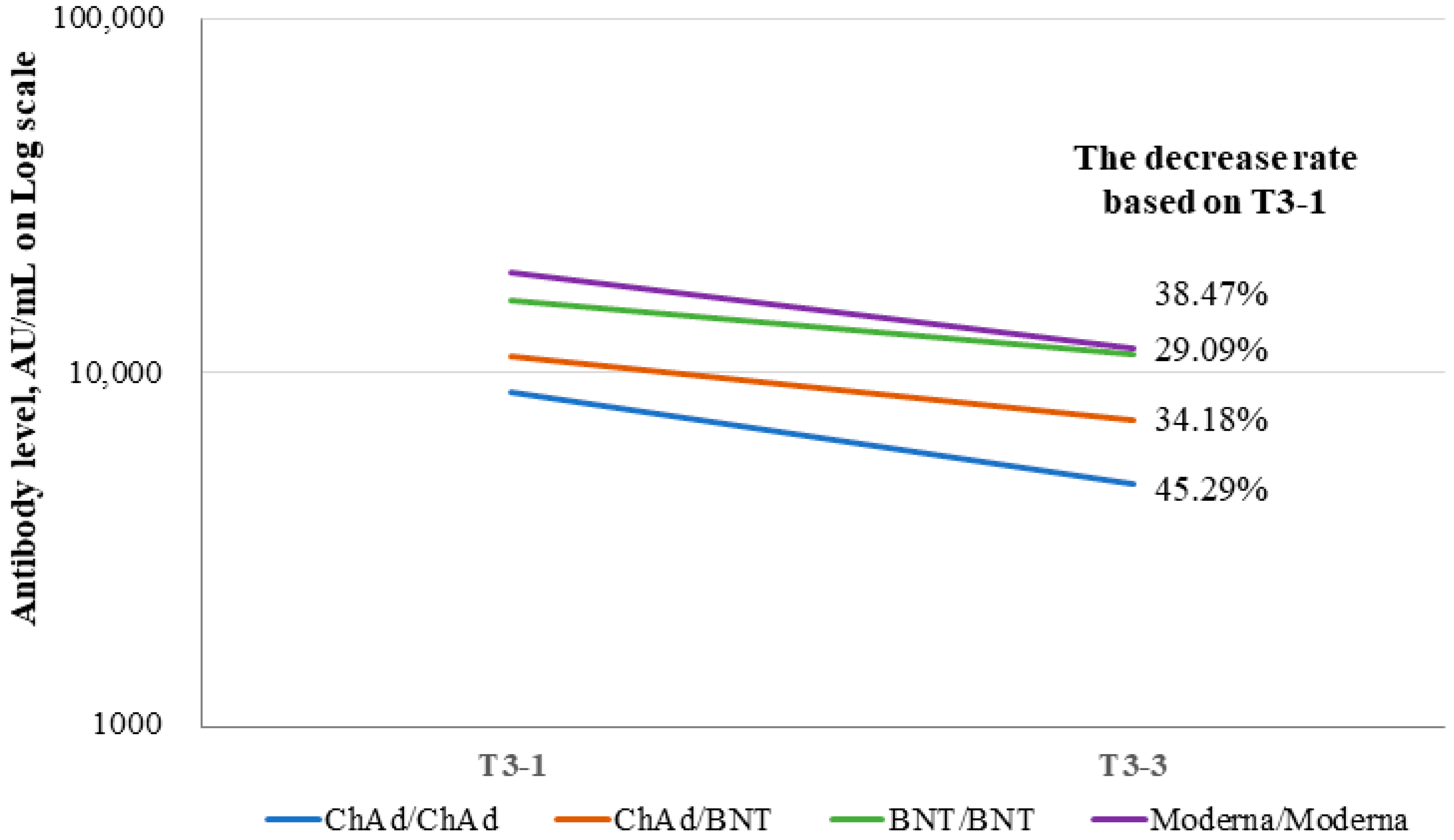
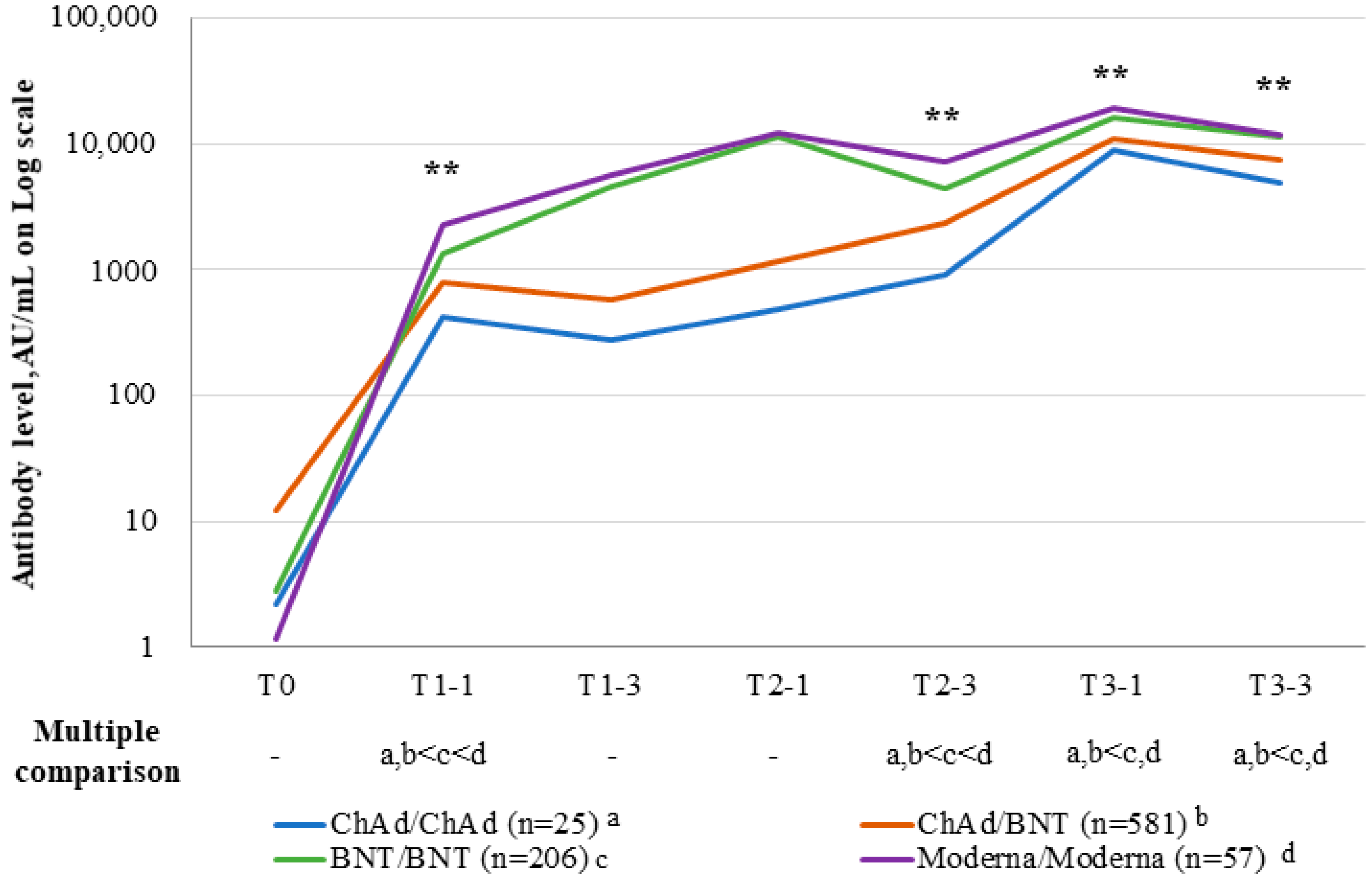
3.2. Antibody Levels and Their Sustainability after the Third Dose
3.3. Factors Associated with Anti-SARS-CoV-2 S-RBD IgG Levels at T3-1
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control. Epidemiological Update. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-omicron-data-16-december (accessed on 31 January 2023).
- Stedman, E. What Are the Symptoms of Omicron and Has Anyone Died from It? Available online: https://www.goodto.com/wellbeing/health/symptoms-omicron-variant-anyone-died-639120 (accessed on 31 January 2023).
- Fowlkes, A.; Gaglani, M.; Groover, K.; Thiese, M.S.; Tyner, H.; Ellingson, K. HEROES-RECOVER Cohorts. Effectiveness of COVID-19 vaccines in preventing SARS-CoV-2 infection among frontline workers before and during B.1.617.2 (delta) variant-eight U.S. locations, December 2020-August 2021. MMWR 2021, 70, 1167–1169. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.M.; Vostok, J.; Johnson, H.; Burns, M.; Gharpure, R.; Sami, S.; Sabo, R.T.; Hall, N.; Foreman, A.; Schubert, P.L.; et al. Outbreak of SARS-CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings-Barnstable County, Massachusetts, July 2021. MMWR 2021, 70, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- WHO. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 31 January 2023).
- Garcia-Beltran, W.F.; St Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef]
- Gruell, H.; Vanshylla, K.; Tober-Lau, P.; Hillus, D.; Schommers, P.; Lehmann, C.; Kurth, F.; Sander, L.E.; Klein, F. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. Nat. Med. 2022, 28, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of protection against mild and severe disease by Covid-19 vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection of BNT162b2 vaccine booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Figueroa Muñiz, M.J.; Wise, J.K.; Adhikari, N.; Ferolito, B.R.; Kurgansky, K.E.; Gagnon, D.R.; Cho, K.; et al. Comparative effectiveness of third doses of mRNA-based COVID-19 vaccines in US veterans. Nat. Microbiol. 2023, 8, 55–63. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Cromer, D.; Steain, M.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Kent, S.J.; Triccas, J.A.; Khoury, D.S.; Davenport, M.P. Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: A meta-analysis. Lancet Microbe. 2021, 3, e52–e61. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of heterologous ChAdOx1 nCoV-19 and mRNA prime-boost vaccination against symptomatic Covid-19 infection in Sweden: A nationwide cohort study. Lancet Reg. Health. Eur. 2021, 11, 100249. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Klemis, V.; Schub, D.; Mihm, J.; Hielscher, F.; Marx, S.; Abu-Omar, A.; Ziegler, L.; Guckelmus, C.; Urschel, R.; et al. Immunogenicity and reactogenicity of heterologous ChAdOx1 nCoV-19/mRNA vaccination. Nat. Med. 2021, 27, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Frenck, R.W.; Walsh, E.E., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 neutralization with BNT162b2 vaccine dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.; Koch, M.; Wu, K.; Chu, L.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.; Oestreicher, J.; Colpitts, T.; et al. Safety and immunogenicity of SARS-CoV-2 variant mRNA vaccine boosters in healthy adults: An interim analysis. Nat. Med. 2021, 27, 2025–2031. [Google Scholar] [CrossRef]
- Nah, E.H.; Cho, S.; Park, H.; Kim, S.; Noh, D.; Kwon, E.; Cho, H.I. Antibody response after two doses of homologous or heterologous SARS-CoV-2 vaccines in healthcare workers at health promotion centers: A prospective observational study. J. Med. Virol. 2022, 94, 4719–4726. [Google Scholar] [CrossRef]
- Kristiansen, P.A.; Page, M.; Bernasconi, V.; Mattiuzzo, G.; Dull, P.; Makar, K.; Plotkin, S.; Knezevic, I. WHO International Standard for anti-SARS-CoV-2 immunoglobulin. Lancet 2021, 397, 1347–1348. [Google Scholar] [CrossRef]
- Abbott. Architect System Operation Manual: SARS-CoV-2 IgG II Quant. Available online: www.corelaboratory.abbott (accessed on 31 January 2023).
- Clinical, Laboratory Standard Institute. Evaluation of the Linearity of Quantitative Measurement Procedures: A Statistical Approach; Approved Guideline, CLSI Document EP06-A; Clinical and Laboratory Standard Institute: Wayne, PA, USA, 2003. [Google Scholar]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and heterologous Covid-19 booster vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Pavord, S.; Scully, M.; Hunt, B.J.; Lester, W.; Bagot, C.; Craven, B.; Rampotas, A.; Ambler, G.; Makris, M. Clinical features of vaccine-induced immune thrombocytopenia and thrombosis. N. Engl. J. Med. 2021, 385, 1680–1689. [Google Scholar] [CrossRef] [PubMed]
- Moderbacher, C.R.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-specific adaptive immunity to SARS-CoV-2 in acute COVID-19 and associations with age and disease severity. Cell 2020, 183, 996–1012.e19. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; Hsiao, S.H.; Fang, T.C.; Lin, Y.C.; Wang, J.C.; Hung, C.S.; Chen, T.H.; Sue, Y.M. SARS-CoV2 antibody response after a third dose of heterologous ChAdOx1 nCoV-19 and Moderna vaccine in chronic dialysis patients. J. Infect. 2022, 84, e98–e100. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Vaccines | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ChAd/ChAd | ChAd/BNT | BNT/BNT | Moderna/Moderna | p | ||||||
| N | (%) | N | (%) | N | (%) | N | (%) | |||
| Total (N = 869) | 25 | 581 | 206 | 57 | ||||||
| Sex | ||||||||||
| Male | 13 | (52) | 209 | (36) | 48 | (23.3) | 16 | (28.1) | 0.001 | |
| Female | 12 | (48) | 372 | (64) | 158 | (76.7) | 41 | (71.9) | ||
| Age, years | ||||||||||
| ≤29 | 0 | - | 2 | (0.3) | 89 | (43.2) | 7 | (12.3) | <0.001 | |
| 30–39 | 4 | (16) | 199 | (34.3) | 69 | (33.5) | 23 | (40.4) | ||
| 40–49 | 2 | (8) | 230 | (39.6) | 35 | (17) | 15 | (26.3) | ||
| 50–59 | 18 | (72) | 128 | (22) | 11 | (5.3) | 12 | (21.1) | ||
| 60–69 | 1 | (4) | 18 | (3.1) | 0 | - | 0 | - | ||
| ≥70 | 0 | - | 4 | (0.7) | 2 | (1) | 0 | - | ||
| Mean ± SD | 50.9 | ±9.2 a | 43.9 | ±8.6 b | 33.9 | ±9.1 c | 40.2 | ±9.4 d | <0.001 † | |
| Interval between second and third doses, months (mean ± SD) | 4.4 | ±0.7 a | 5.0 | ±0.8 b | 4.5 | ±1.1 c | 4 | ±0.9 d | <0.001 ‡ | |
| Working in patient-facing healthcare | ||||||||||
| No | 8 | (32) | 83 | (14.3) | 46 | (22.3) | 7 | (12.3) | 0.007 | |
| Yes | 17 | (68) | 498 | (85.7) | 160 | (77.7) | 50 | (87.7) | ||
| 1 Month after the Third Vaccination | ||||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | |||||||
| Coef. | (SE) | Exp (Coef.) | p-Value | Coef. | (SE) | Exp (Coef.) | p-Value | |
| Sex, ref: female | −0.129 | (0.053) | 0.88 | 0.016 | −0.087 | (0.052) | 0.92 | 0.098 |
| Age | −0.004 | (0.003) | - | 0.100 | 0.004 | (0.003) | - | 0.187 |
| Vaccine type, ref: ChAd/ChAd | ||||||||
| ChAd/BNT | 0.159 | (0.147) | 1.17 | 0.279 | 0.16 | (0.149) | 1.17 | 0.283 |
| BNT/BNT | 0.497 | (0.152) | 1.64 | 0.001 | 0.536 | (0.16) | 1.71 | 0.001 |
| Moderna/Moderna | 0.609 | (0.172) | 1.84 | <0.001 | 0.645 | (0.176) | 1.91 | <0.001 |
| Working in patient facing healthcare role, ref. no | −0.046 | (0.067) | 0.96 | 0.496 | −0.019 | (0.068) | 0.98 | 0.783 |
| Interval between the second and third doses, (months) | −0.031 | (0.027) | - | 0.250 | 0.027 | (0.028) | - | 0.342 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nah, E.-H.; Cho, S.; Park, H.; Kim, S.; Noh, D.; Kwon, E.; Cho, H.-I. SARS-CoV-2 Antibody Response and Sustainability after a Third Dose of BNT162b2 in Healthcare Workers at Health Promotion Centers. Viruses 2023, 15, 751. https://doi.org/10.3390/v15030751
Nah E-H, Cho S, Park H, Kim S, Noh D, Kwon E, Cho H-I. SARS-CoV-2 Antibody Response and Sustainability after a Third Dose of BNT162b2 in Healthcare Workers at Health Promotion Centers. Viruses. 2023; 15(3):751. https://doi.org/10.3390/v15030751
Chicago/Turabian StyleNah, Eun-Hee, Seon Cho, Hyeran Park, Suyoung Kim, Dongwon Noh, Eunjoo Kwon, and Han-Ik Cho. 2023. "SARS-CoV-2 Antibody Response and Sustainability after a Third Dose of BNT162b2 in Healthcare Workers at Health Promotion Centers" Viruses 15, no. 3: 751. https://doi.org/10.3390/v15030751