
A Novel and Simplified Score for Determining Treatment Eligibility for Patients with Chronic Hepatitis B
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Standard International Guidelines and Thai Guideline
- HBeAg-positive or -negative patients with HBV DNA > 2000 IU/mL, ALT > upper limit normal (ULN), and/or at least moderate liver necroinflammation or fibrosis;
- Patients with HBV DNA > 20,000 IU/mL and ALT > 2 × ULN, regardless of the degree of fibrosis;
- Patients with cirrhosis and detectable HBV DNA.
- Patients with high HBV DNA levels (>20,000 IU/mL if HBeAg-positive and >2000 IU/mL if HBeAg-negative) and elevated ALT levels >2 × ULN;
- Patient with cirrhosis with HBV DNA > 2000 IU/mL.
- Patients with high HBV DNA levels (>20,000 IU/mL if HBeAg-positive and >2000 IU/mL if HBeAg-negative) and persistently elevated ALT levels > 2 × ULN (at least 1 month between observations);
- Patients with high HBV DNA levels (>20,000 IU/mL if HBeAg-positive and >2000 IU/mL if HBeAg-negative) and a biopsy showing moderate-to-severe inflammation or significant fibrosis;
- Patients with decompensated cirrhosis and detectable HBV DNA;
- Patients with compensated cirrhosis and HBV DNA > 2000 IU/mL, even if their ALT levels are normal.
- Patients with high HBV DNA levels (>2000 IU/mL, regardless of their HBeAg status) and persistently elevated ALT levels > 2 × ULN (with at least 3 months between observations);
- Patients with high HBV DNA levels (>2000 IU/mL, regardless of their HBeAg status) and liver fibrosis ≥ F2 from LSM (defined as LSM ≥ 7.0 kPa) or biopsy shows moderate-to-severe inflammation or significant fibrosis;
- Patients with cirrhotic and detectable HBV DNA.
2.4. Simplified Criteria and Scoring Systems
2.4.1. WHO Simplified Criteria
2.4.2. TREAT-B
2.4.3. REACH-B
2.5. Rationale for Selecting Scoring System Parameters
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Participant Characteristics
3.2. Development of the HePAA Scoring System
- HBeAg status (“0” for negative; “1” for positive)
- platelet count (“0” for ≥150 × 109/L; “1” for <150 × 109/L)
- ALT (“0” for <30 IU/L; “1” for 30–39 IU/L; “2” for 40–49 IU/L; “3” for ≥50 IU/L)
- albumin (“0” for ≥4 g/dL; “1” for <4 g/dL)
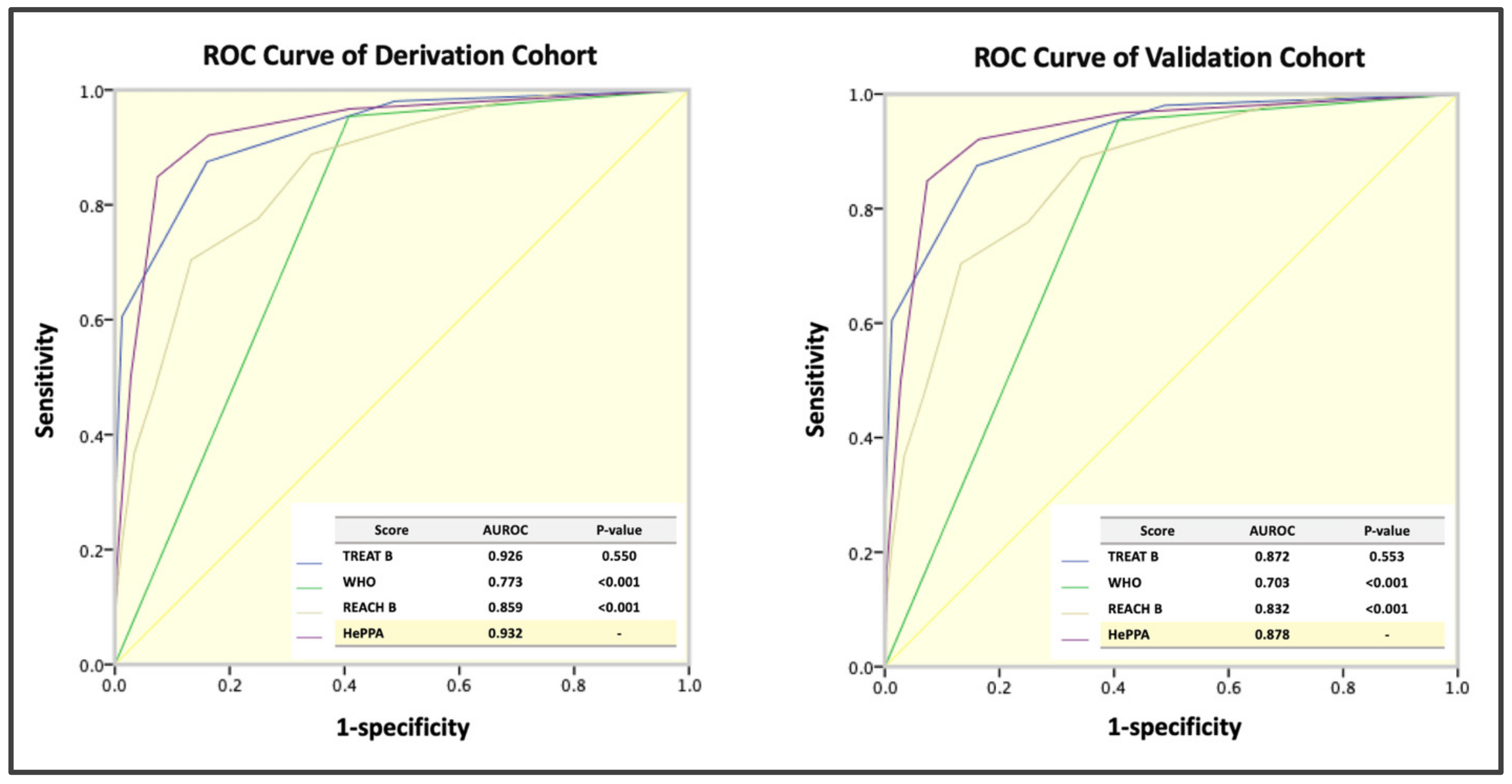
3.3. Performance of the HePAA Scoring System and Optimal Cutoff Selection
3.4. Validation and Comparison with Other Systems
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar] [CrossRef] [PubMed]
- Hutin, Y.; Nasrullah, M.; Easterbrook, P.; Nguimfack, B.D.; Burrone, E.; Averhoff, F.; Bulterys, M. Access to Treatment for Hepatitis B Virus Infection—Worldwide, 2016. Am. J. Transplant. 2018, 67, 773–777. [Google Scholar]
- WHO. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- WHO. Global Hepatitis Report 2017. Available online: http://apps.who.int/iris/handle/10665/255016 (accessed on 14 March 2022).
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EASL. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- THASL. Thailand Practice Guideline for Management of Chronic Hepatitis B and C 2015. Available online: https://thasl.org/wp-content/uploads/2019/09/25.Thailand-guideline-for-management-of-CHB-and-CHC-2015.pdf (accessed on 14 March 2022).
- WHO. Guidelines for the Prevention, Care and Treatment of Persons with Chronic Hepatitis B Infection. Available online: http://whoint/hiv/pub/hepatitis/hepatitis-b-guidelines/en/ (accessed on 31 March 2022).
- Shimakawa, Y.; Njie, R.; Ndow, G.; Vray, M.; Mbaye, P.S.; Bonnard, P.; Sombié, R.; Nana, J.; Leroy, V.; Bottero, J.; et al. Development of a simple score based on HBeAg and ALT for selecting patients for HBV treatment in Africa. J. Hepatol. 2018, 69, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Howell, J.; Anderson, D.; Bloom, S.; Lubel, J.; Kemp, W.; Williams, J.; Bell, S.; Croagh, C.; Demediuk, B.; Desmond, P.; et al. Validation of the TREAT-B score for hepatitis B treatment eligibility in a large Asian cohort: TREAT-B improves with age. J. Hepatol. 2020, 73, 1282–1284. [Google Scholar] [CrossRef]
- Yoshida, K.; Post, G.; Shimakawa, Y.; Thursz, M.; Brown, A.; Ingiliz, P.; Lemoine, M. Clinical utility of TREAT-B score in African and non-African HBV-infected patients living in Europe. J. Hepatol. 2019, 70, 1295–1297. [Google Scholar] [CrossRef] [Green Version]
- Shimakawa, Y.; Boucheron, P.; Luong Nguyen, L.B.; Lemoine, M.; Sombié, R. Performance of two simplified HBV treatment criteria (TREAT-B score and WHO guidelines) in Burkina Faso, West Africa. J. Hepatol. 2019, 71, 842–844. [Google Scholar] [CrossRef] [Green Version]
- Johannessen, A.; Aberra, H.; Desalegn, H.; Gordien, E.; Berhe, N. A novel score to select patients for treatment in chronic hepatitis B: Results from a large Ethiopian cohort. J. Hepatol. 2019, 71, 840–841. [Google Scholar] [CrossRef] [Green Version]
- Vinikoor, M.J.; Sinkala, E.; Kanunga, A.; Muchimba, M.; Zanolini, A.; Saag, M.; Pry, J.; Nsokolo, B.; Chisenga, T.; Kelly, P. Eligibility for hepatitis B antiviral therapy among adults in the general population in Zambia. PLoS ONE 2020, 15, e0227041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu Hai, V.; Shimakawa, Y.; Kim, J.; Do Ngoc, H.; Le Minh, Q.; Laureillard, D.; Lemoine, M. Assessment and Simplification of Treatment Eligibility Among Patients With Chronic Hepatitis B Infection in Vietnam. Clin. Infect. Dis. 2021, 73, e1072–e1077. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Lemoine, M. Reply to: “Validation of the TREAT-B score for hepatitis B treatment eligibility in a large Asian cohort: TREAT-B improves with age”. J. Hepatol. 2020, 73, 1284–1285. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Lemoine, M.; Njai, H.F.; Bottomley, C.; Ndow, G.; Goldin, R.D.; Jatta, A.; Jeng-Barry, A.; Wegmuller, R.; Moore, S.E.; et al. Natural history of chronic HBV infection in West Africa: A longitudinal population-based study from The Gambia. Gut 2016, 65, 2007–2016. [Google Scholar] [CrossRef]
- Chang, M.H. Natural history and clinical management of chronic hepatitis B virus infection in children. Hepatol. Int. 2008, 2 (Suppl. S1), 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.I.; Yuen, M.F.; Chan, H.L.; Han, K.H.; Chen, P.J.; Kim, D.Y.; Ahn, S.H.; Chen, C.J.; Wong, V.W.; Seto, W.K. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): Development and validation of a predictive score. Lancet Oncol. 2011, 12, 568–574. [Google Scholar] [CrossRef]
- Wong, V.W.; Chan, S.L.; Mo, F.; Chan, T.C.; Loong, H.H.; Wong, G.L.; Lui, Y.Y.; Chan, A.T.; Sung, J.J.; Yeo, W.; et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. J. Clin. Oncol. 2010, 28, 1660–1665. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.L.; Chan, H.L.; Wong, C.K.; Leung, C.; Chan, C.Y.; Ho, P.P.; Chung, V.C.; Chan, Z.C.; Tse, Y.K.; Chim, A.M.; et al. Liver stiffness-based optimization of hepatocellular carcinoma risk score in patients with chronic hepatitis B. J. Hepatol. 2014, 60, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino, R.B. Presentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef]
- Nahm, F.S. Receiver operating characteristic curve: Overview and practical use for clinicians. Korean J. Anesthesiol. 2022, 75, 25–36. [Google Scholar] [CrossRef]
- Shreffler, J.; Huecker, M.R. Diagnostic Testing Accuracy: Sensitivity, Specificity, Predictive Values and Likelihood Ratios. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Papatheodoridis, G.; Dalekos, G.; Sypsa, V.; Yurdaydin, C.; Buti, M.; Goulis, J.; Calleja, J.L.; Chi, H.; Manolakopoulos, S.; Mangia, G.; et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J. Hepatol. 2016, 64, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, Y.D.; Lee, M.; Jun, B.G.; Kim, T.S.; Suk, K.T.; Kang, S.H.; Kim, M.Y.; Cheon, G.J.; Kim, D.J.; et al. Modified PAGE-B score predicts the risk of hepatocellular carcinoma in Asians with chronic hepatitis B on antiviral therapy. J. Hepatol. 2018, 69, 1066–1073. [Google Scholar] [CrossRef]
- Sharma, S.A.; Kowgier, M.; Hansen, B.E.; Brouwer, W.P.; Maan, R.; Wong, D.; Shah, H.; Khalili, K.; Yim, C.; Heathcote, E.J.; et al. Toronto HCC risk index: A validated scoring system to predict 10-year risk of HCC in patients with cirrhosis. J. Hepatol. 2017, 68, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Kao, J.H. Global perspective on the natural history of chronic hepatitis B: Role of hepatitis B virus genotypes A to J. Semin. Liver Dis. 2013, 33, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Cooksley, W.G. Do we need to determine viral genotype in treating chronic hepatitis B? J. Viral. Hepat. 2010, 17, 601–610. [Google Scholar] [CrossRef]
- Evans, A.A.; O’Connell, A.P.; Pugh, J.C.; Mason, W.S.; Shen, F.M.; Chen, G.C.; Lin, W.Y.; Dia, A.; M’Boup, S.; Dramé, B.; et al. Geographic variation in viral load among hepatitis B carriers with differing risks of hepatocellular carcinoma. Cancer Epidemiol. Biomark. Prev. 1998, 7, 559–565. [Google Scholar]
- Fung, J.; Seto, W.K.; Lai, C.L.; Yuen, J.; Wong, D.K.; Yuen, M.F. Profiles of HBV DNA in a large population of Chinese patients with chronic hepatitis B: Implications for antiviral therapy. J. Hepatol. 2011, 54, 195–200. [Google Scholar] [CrossRef]


{kind=link}
| Derivation Cohort (n = 602) | Validation Cohort (n = 420) | p-Value ** | |
|---|---|---|---|
| Age (years) | 51.10 ± 13.825 | 43.24 ± 11.97 | <0.001 |
| Male sex, n (%) | 279 (46.3%) | 227 (54.0%) | 0.010 |
| BMI (kg/m2) | 23.39 ± 3.87 | 23.56 ± 3.68 | 0.480 |
| HBV DNA <2000, n (%) 2000–20,000, n (%) >20,000, n (%) | 283 (47%) 88 (14.6%) 231 (38.4%) | 174 (41.4%) 67 (16.0%) 179 (42.6%) | 0.697 |
| HBeAg positive, n (%) | 88 (14.6%) | 58 (13.8%) | 0.697 |
| Liver fibrosis by LSM, n (%) F0–1 (LSM < 7.9) F2–3 (LSM 7.9–9.4) F4 (LSM > 9.4) | 334 (83.5%) 22 (5.5%) 44 (11%) | 297 (83.9%) 21 (5.9%) 36 (10.2%) | 0.911 |
| AST (IU/L), median (IQR) | 25.0 (20.0, 40.0) | 26.0 (20.0, 36.0) | 0.589 |
| ALT (IU/L), median (IQR) | 25.0 (17.0, 47.0) | 30.0 (20.0, 50.0) | <0.001 |
| Albumin (g/L), mean ± SD | 4.26 ± 0.47 | 4.48 ± 0.52 | <0.001 |
| TB (IU/L), median (IQR) | 0.50 (0.40, 0.70) | 0.8 (0.1, 1.0) | <0.001 |
| Platelet (109/L), median (IQR) | 242 (201, 279) | 231 (199, 270) | 0.018 |
| APRI, median (IQR) | 0.269 (0.192, 0.453) | 0.390 (0.270, 0.560) | <0.001 |
| FIB−4, median (IQR) | 1112 (0.789, 1.594) | 1146 (0.642, 1.219) | <0.001 |
| Eligible for EASL treatment criteria, n (%) | 165 (27.5%) | 92 (21.9%) | 0.042 |
| Eligible for AASLD treatment criteria, n (%) | 170 (28.2%) | 94 (22.4%) | 0.032 |
| Eligible for APASL treatment criteria, n (%) | 162 (27.2%) | 94 (22.4%) | 0.079 |
| Eligible for THASL treatment criteria, n (%) | 171 (28.4%) | 94 (22.4%) | 0.028 |
| Variables | Not Eligible for Treatment (n = 602) | Eligible for Treatment by EASL Guidelines (n = 172) | p-Value | Final Model Selected by Forward Stepwise Regression | |
|---|---|---|---|---|---|
| β Regression Coefficient | p-Value | ||||
| Age, mean ± SD (years) | 50.98 ± 13.62 | 51.47 ± 14.39 | 0.695 | ||
| BMI, mean ± SD (kg/m2) | 23.37 ± 3.92 | 23.42 ± 3.78 | 0.901 | ||
| Male sex, n (%) | 178 (40.70) | 101 (61.20) | <0.01 | ||
| HBeAg, n (%) | 29 (6.60) | 59 (35.8) | <0.01 | 0.899 | 0.036 |
| AST, median (P25, P75) (IU/L) | 22 (19, 27) | 58 (42, 87) | <0.01 | ||
| ALT, median (P25, P75) (IU/L) | 20 (15, 28) | 80 (47, 123) | <0.01 | 0.097 | <0.01 |
| Albumin, mean ± SD (g/L) | 4.34 ± 0.41 | 4.11 ± 0.55 | 0.015 | −0.838 | 0.025 |
| TB median (P25, P75) (IU/L) | 0.48 (0.37, 0.64) | 0.64 (0.46, 0.90) | <0.01 | ||
| Platelet < 150 × 109/L, n (%) | 7 (1.6%) | 24 (14.5%) | <0.01 | 2.405 | <0.01 |
| Predictors | Categories | β Regression Coefficient | Adjusted with Constant ** | Points |
|---|---|---|---|---|
| HBeAg | Negative | 0 | 0 | 0 |
| Positive | 1095 | 4.568 | 1 | |
| Platelet (109/L) | <1,500,000 | 2.2561 | 5.928 | 1 |
| ≥1,500,000 | 0 | 0 | 0 | |
| ALT (IU/L) | <30 | 0 | 0 | 0 |
| 30–39 | 1558 | 5093 | 1 | |
| 40–49 | 3143 | 6754 | 2 | |
| ≥50 | 4757 | 8361 | 3 | |
| Albumin (g/L) | <4 | 0.436 | 4236 | 1 |
| ≥4 | 0 | 0 | 0 |
| TREAT-B (≥2) | Simplified WHO Criteria | REACH-B (≥6) | HePAA (≥2) | HePAA (≥3) | |
|---|---|---|---|---|---|
| AUROC | 0.926 (0.901–0.950) | 0.773 (0.742–0.805) | 0.859 (0.825–0.893) | 0.932 (0.907–0.957) | |
| p-Value ** | 0.550 | <0.001 | <0.001 | N/A | |
| Sensitivity (%) | 86.7 (80.5–91.5) | 94.5 (89.9–97.5) | 98.2 (94.8–99.6) | 92.1 (86.6–95.9) | 84.9 (78.2–90.2) |
| Specificity (%) | 86.3 (82.7–89.4) | 62.0 (57.3–66.6) | 37.5 (33.0–42.3) | 83.6 (79.2–87.5) | 92.6 (89.2–95.2) |
| Positive Predictive Value (%) | 70.4 (63.7–76.6) | 48.4 (42.9–54.1) | 37.2 (32.7–42.0) | 72.5 (65.7–78.7) | 84.3 (84.3–77.6) |
| Negative Predictive Value (%) | 94.5 (91.8–96.5) | 96.8 (94.0–98.5) | 98.2 (94.8–99.6) | 95.8 (92.7–97.8) | 92.9 (89.5–95.4) |
| Positive Likelihood Ratio | 6.31 (4.95–8.04) | 2.49 (2.20–2.82) | 1.57 (1.46–1.70) | 5.63 (4.38–7.23) | 11.46 (7.75–16.94) |
| Negative Likelihood Ratio | 0.15 (0.10–0.23) | 0.09 (0.05–0.17) | 0.05 (0.02–0.15) | 0.09 (0.05–0.16) | 0.16 (0.11–0.24) |
| TREAT-B (≥2) | Simplified WHO Criteria | REACH-B (≥6) | HePAA (≥2) | HePAA (≥3) | |
|---|---|---|---|---|---|
| AUROC | 0.872 (0.833–0.910) | 0.703 (0.668–0.737) | 0.832 (0.789–0.875) | 0.878 (0.843–0.913) | |
| p-Value ** | 0.553 | <0.001 | <0.001 | N/A | |
| Sensitivity (%) | 84.8 (75.8–91.4) | 95.7 (89.2–98.8) | 93.5 (86.3–97.6) | 97.8 (92.3–99.7) | 87.9 (79.4–93.8) |
| Specificity (%) | 72.0 (66.8–76.7) | 55.2 (49.6–60.7) | 36.0 (30.8–41.4) | 56.9 (51.3–62.3) | 73.7 (68.6–78.4) |
| Positive Predictive Value (%) | 45.9 (38.2–53.7) | 37.5 (34.5–40.5) | 29.1 (23.9–34.6) | 38.7 (35.7–41.8) | 31.5 (27.4–35.9) |
| Negative Predictive Value (%) | 94.4 (90.8–96.9) | 97.8 (94.5–99.2) | 95.2 (89.8–98.2) | 98.9 (95.9–99.7) | 97.8 (96.2–98.7) |
| Positive Likelihood Ratio | 3.02 (2.49–3.67) | 2.13 (1.88−2.43) | 1.46 (1.32–1.61) | 2.27 (2.00–2.58) | 3.34 (2.75–4.07) |
| Negative Likelihood Ratio | 0.21 (0.13–0.34) | 0.08 (0.03–0.21) | 0.18 (0.08–0.40) | 0.04 (0.01–0.15) | 0.16 (0.09–0.29) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geeratragool, T.; Tangkijvanich, P.; Nimanong, S.; Chainuvati, S.; Charatcharoenwitthaya, P.; Tanwandee, T.; Chotiyaputta, W. A Novel and Simplified Score for Determining Treatment Eligibility for Patients with Chronic Hepatitis B. Viruses 2023, 15, 724. https://doi.org/10.3390/v15030724
Geeratragool T, Tangkijvanich P, Nimanong S, Chainuvati S, Charatcharoenwitthaya P, Tanwandee T, Chotiyaputta W. A Novel and Simplified Score for Determining Treatment Eligibility for Patients with Chronic Hepatitis B. Viruses. 2023; 15(3):724. https://doi.org/10.3390/v15030724
Chicago/Turabian StyleGeeratragool, Tanawat, Pisit Tangkijvanich, Supot Nimanong, Siwaporn Chainuvati, Phunchai Charatcharoenwitthaya, Tawesak Tanwandee, and Watcharasak Chotiyaputta. 2023. "A Novel and Simplified Score for Determining Treatment Eligibility for Patients with Chronic Hepatitis B" Viruses 15, no. 3: 724. https://doi.org/10.3390/v15030724