
Differences in HCV Seroprevalence, Clinical Features, and Treatment Outcomes between Female and Male Incarcerated Population: Results from a Matched Cohort Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Inclusion Criteria and Matching Parameters
2.2. Sample Size and Statistical Analysis
2.3. Outcomes
2.4. Treatments
2.5. Ethical Issues
3. Results
3.1. Study Population
3.2. HCV Seroprevalence and Active Infections
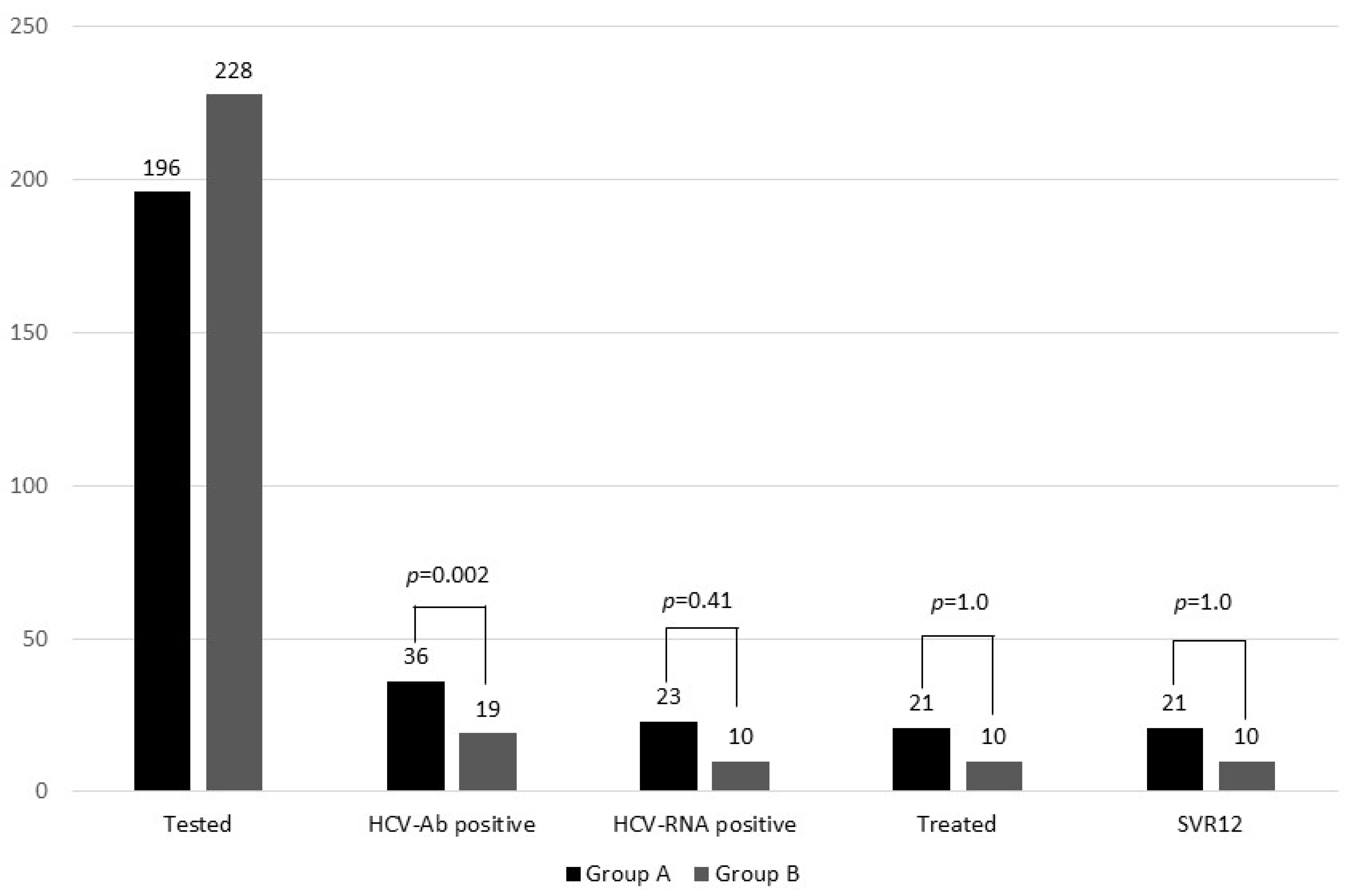
3.3. HCV Treatment Cascade of Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dhiman, R.K.; Premkumar, M. Hepatitis C Virus Elimination by 2030: Conquering Mount Improbable. Clin. Liver Dis. 2020, 16, 254. [Google Scholar] [CrossRef]
- Westbrook, R.H.; Dusheiko, G. Natural History of Hepatitis C. J. Hepatol. 2014, 61, S58–S68. [Google Scholar] [CrossRef]
- Larney, S.; Kopinski, H.; Beckwith, C.G.; Zaller, N.D.; Jarlais, D.D.; Hagan, H.; Rich, J.D.; van den Bergh, B.J.; Degenhardt, L. Incidence and Prevalence of Hepatitis C in Prisons and Other Closed Settings: Results of a Systematic Review and Meta-Analysis. Hepatology 2013, 58, 1215–1224. [Google Scholar] [CrossRef]
- Rich, J.D.; Allen, S.A.; Williams, B.A. Responding to Hepatitis C through the Criminal Justice System. N. Engl. J. Med. 2014, 370, 1871–1874. [Google Scholar] [CrossRef]
- Radley, A.; Robinson, E.; Aspinall, E.J.; Angus, K.; Tan, L.; Dillon, J.F. A Systematic Review and Meta-Analysis of Community and Primary-Care-Based Hepatitis C Testing and Treatment Services That Employ Direct Acting Antiviral Drug Treatments. BMC Health Serv. Res. 2019, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Marino, A.; Zafarana, G.; Ceccarelli, M.; Cosentino, F.; Moscatt, V.; Bruno, G.; Bruno, R.; Benanti, F.; Cacopardo, B.; Celesia, B.M. Immunological and Clinical Impact of DAA-Mediated HCV Eradication in a Cohort of HIV/HCV Coinfected Patients: Monocentric Italian Experience. Diagnostics 2021, 11, 2336. [Google Scholar] [CrossRef] [PubMed]
- Sapena, V.; Enea, M.; Torres, F.; Celsa, C.; Rios, J.; Rizzo, G.E.M.; Nahon, P.; Mariño, Z.; Tateishi, R.; Minami, T.; et al. Hepatocellular Carcinoma Recurrence after Direct-Acting Antiviral Therapy: An Individual Patient Data Meta-Analysis. Gut 2022, 71, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Strazzulla, A.; Iemmolo, R.M.R.; Carbone, E.; Postorino, M.C.; Mazzitelli, M.; De Santis, M.; Di Benedetto, F.; Cristiani, C.M.; Costa, C.; Pisani, V.; et al. The Risk of Hepatocellular Carcinoma After Directly Acting Antivirals for Hepatitis C Virus Treatment in Liver Transplanted Patients: Is It Real? Hepat Mon. 2016, 16, 11. [Google Scholar] [CrossRef]
- He, N.; Feng, G.; Hao, S.; Xu, M.; Liu, J.; Kong, F.; Ren, Z.; Dou, W.; Yao, C.; Liang, T.; et al. The Impact of Direct-Acting Antivirals on Quality of Life in Patients with Hepatitis C Virus Infection: A Meta-Analysis. Ann. Hepatol. 2022, 27, 100705. [Google Scholar] [CrossRef] [PubMed]
- Mazzitelli, M.; Torti, C.; Sabatino, J.; D’Ascoli, G.L.; Costa, C.; Pisani, V.; Raffetti, E.; De Rosa, S.; Strazzulla, A.; Focà, A.; et al. Evaluation of Cardiac Function by Global Longitudinal Strain before and after Treatment with Sofosbuvir-Based Regimens in HCV Infected Patients. BMC Infect Dis. 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Odolini, S.; Pollastri, E.; Volpi, S.; Cappa, V.; Spinetti, A.; Zaltron, S.; Nasta, P.; Compostella, S.; Carriero, C.; Zuglian, G.; et al. Improvement of Patients Reported Outcomes and Neurocognitive Perfor-Mances after Direct-Acting Antivirals: A Longitudinal Study. Infect. Dis. Trop. Med. 2021, 7, e7330. [Google Scholar] [CrossRef]
- Marascio, N.; Quirino, A.; Barreca, G.S.; Galati, L.; Costa, C.; Pisani, V.; Mazzitelli, M.; Matera, G.; Liberto, M.C.; Focà, A.; et al. Discussion on Critical Points for a Tailored Therapy to Cure Hepatitis C Virus Infection. Clin. Mol. Hepatol. 2019, 25, 30–36. [Google Scholar] [CrossRef]
- Stockman, L.J.; Greer, J.; Holzmacher, R.; Dittmann, B.; Hoftiezer, S.A.; Alsum, L.E.; Prieve, A.; Westergaard, R.P.; Guilfoyle, S.M.; Vergeront, J.M. Performance of Risk-Based and Birth-Cohort Strategies for Identifying Hepatitis C Virus Infection Among People Entering Prison, Wisconsin, 2014. Public Health Rep. 2016, 131, 544. [Google Scholar] [CrossRef] [PubMed]
- Fazel, S.; Yoon, I.A.; Hayes, A.J. Substance Use Disorders in Prisoners: An Updated Systematic Review and Meta-Regression Analysis in Recently Incarcerated Men and Women. Addiction 2017, 112, 1725–1739. [Google Scholar] [CrossRef]
- Şahin, Ö.; Kaygusuz, S.; Tuna, A.; Gül, S.; Kaçmaz, B. Genotype Distribution, Intravenous Drug Use Rates and Direct-Acting Antiviral Treatment Results in Prisoner Hepatitis C Patients. Infect. Dis. Trop. Med. 2023, 9, e1120. [Google Scholar] [CrossRef]
- Hofstraat, S.; Falla, A.; Veldhuijzen, I.; Hahné, S.; Benthem, B.H.B.V.; Tavoschi, L. Europäisches Zentrum für die Prävention und die Kontrolle von Krankheiten. In Systematic Review on Hepatitis B and C Prevalence in the EU/EEA; European Centre for Disease Prevention and Control: Stockholm, Sweden; ISBN 978-92-9193-982-4.
- Ministero Della Giustizia|Statistiche. Available online: https://www.giustizia.it/giustizia/it/mg_1_14.page# (accessed on 28 September 2023).
- Masarone, M.; Caruso, R.; Aglitti, A.; Izzo, C.; De Matteis, G.; Attianese, M.R.; Pagano, A.M.; Persico, M. Hepatitis C Virus Infection in Jail: Difficult-to-Reach, Not to-Treat. Results of a Point-of-Care Screening and Treatment Program. Dig. Liver Dis. 2020, 52, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Fiore, V.; De Matteis, G.; Ranieri, R.; Saderi, L.; Pontali, E.; Muredda, A.; Ialungo, A.M.; Caruso, R.; Madeddu, G.; Sotgiu, G.; et al. HCV Testing and Treatment Initiation in an Italian Prison Setting: A Step-by-Step Model to Micro-Eliminate Hepatitis C. Int J. Drug Policy 2021, 90, 103055. [Google Scholar] [CrossRef]
- Fiore, V.; Rastrelli, E.; Madeddu, G.; Ranieri, R.; De Vito, A.; Giuliani, R.; Di Mizio, G.; Bolcato, M.; De Matteis, G.; Ialungo, A.M.; et al. HCV Spread among Female Incarcerated Population and Treatment Pathways to Viral Elimination in Italian Prison Settings: Clinical Perspectives and Medico Legal Aspects. BMC Infect Dis. 2022, 22, 601. [Google Scholar] [CrossRef] [PubMed]
- WHO Elimination of Hepatitis by 2030. Available online: https://www.who.int/health-topics/hepatitis/elimination-of-hepatitis-by-2030#tab=tab_1 (accessed on 28 September 2023).
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a Simple Noninvasive Index to Predict Significant Fibrosis in Patients with HIV/HCV Coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Associazione Italiana Per Lo Studio Del Fegato Documento Di Indirizzo Dell’Associazione Italiana per Lo Studio Del Fegato per l’uso Razionale Dei Farmaci Anti-HCV Disponibili in Italia. 2020, Volume 20. Available online: https://www.webaisf.org/documento-hcv-2020/ (accessed on 28 September 2023).
- Puga, M.A.M.; Bandeira, L.M.; Pompilio, M.A.; Croda, J.; De Rezende, G.R.; Dorisbor, L.F.P.; Tanaka, T.S.O.; Cesar, G.A.; Teles, S.A.; Simionatto, S.; et al. Prevalence and Incidence of HCV Infection among Prisoners in Central Brazil. PLoS ONE 2017, 12, e0169195. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Gawad, M.; Nour, M.; El-Raey, F.; Nagdy, H.; Almansoury, Y.; El-Kassas, M. Gender Differences in Prevalence of Hepatitis C Virus Infection in Egypt: A Systematic Review and Meta-Analysis. Sci. Rep. 2023, 13, 2499. [Google Scholar] [CrossRef] [PubMed]
- Busschots, D.; Kremer, C.; Bielen, R.; Koc, Ö.M.; Heyens, L.; Nevens, F.; Hens, N.; Robaeys, G. Hepatitis C Prevalence in Incarcerated Settings between 2013–2021: A Systematic Review and Meta-Analysis. BMC Public Health 2022, 22, 2159. [Google Scholar] [CrossRef] [PubMed]
- Fiore, V.; De Matteis, G.; Pontali, E.; De Vito, A.; Panese, S.; Geremia, N.; Maida, I.; Artioli, S.; Starnini, G.; Madeddu, G.; et al. Quick Diagnosis, Staging, and Treatment of HCV Infection among People Living in Prison: Opinion Expert Panel. Front. Public Health 2022, 10, 926414. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Results | p-Value | |
|---|---|---|---|
| Group A (n = 196) | Group B (n = 228) | ||
| Age, mean ± SD | 44 ± 10.5 | 41 ± 10.6 | 0.33 * |
| Italian nationality, n (%) | 127 (64.8) | 162 (71.1%) | 0.17 ** |
| PWID, n (%) | 38 (19.5) | 57 (25) | 0.16 ** |
| On OST | 14/38 (36.8) | 33/57 (57.9) | 0.44 ** |
| PLWH (n, %) | 5 (2.6) | 3 (1.3) | 0.35 ** |
| HBV, n (%) | |||
| HBsAg positive | 3 (1.5) | 7 (3) | |
| Anti-HBsAg positive | 95 (48.5) | 111 (48.7) | 0.36 *** |
| Vaccined | 8/95 (8.4) | 13/111 (11.7) | 0.96 ** |
| Past infection | 87/95 (91.6) | 98 (88.2) | 0.43 ** |
| OBI | 9 (4.6) | - | 0.77 ** |
| HCV-Ab positive, n (%) | 36 (18.4) | 19 (8.3) | 0.002 ** |
| HCV RNA positive | 23/36 (63.8) | 10/19 (52.6) | 0.41 ** |
| Variable | Results | p-Value | |
|---|---|---|---|
| Group A (n = 23) | Group B (n = 10) | ||
| HCV RNA, median (Q1-3) | 566,000 (41,200–1,700,000) | 481,381 (128,060–1,020,362.3) | 0.89 * |
| HCV genotype, n (%) 1a 1b 2 3a 4 | 4 (17.4) 2 (8.7) 1 (4.4) 13 (56.5) 3 (13) | 1 (10) 1 (10) - 7 (70) 1 (10) | 1.0 ** 1.0 ** 1.0 ** 0.26 ** 1.0 ** |
| FIB-4 value, n (%) Low (<1.45) Intermediate (1.45–3.25) High (>3.25) | 18 (78.3) 3 (13) 2 (8.7) | 6 (60) 2 (20) 2 (20) | 0.4 ** 0.63 ** 0.57 ** |
| HBV co-infection | 2 (8.7) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiore, V.; De Vito, A.; Rastrelli, E.; Manca, V.; De Matteis, G.; Ranieri, R.; Pontali, E.; Geremia, N.; Panese, S.; Starnini, G.; et al. Differences in HCV Seroprevalence, Clinical Features, and Treatment Outcomes between Female and Male Incarcerated Population: Results from a Matched Cohort Study. Viruses 2023, 15, 2414. https://doi.org/10.3390/v15122414
Fiore V, De Vito A, Rastrelli E, Manca V, De Matteis G, Ranieri R, Pontali E, Geremia N, Panese S, Starnini G, et al. Differences in HCV Seroprevalence, Clinical Features, and Treatment Outcomes between Female and Male Incarcerated Population: Results from a Matched Cohort Study. Viruses. 2023; 15(12):2414. https://doi.org/10.3390/v15122414
Chicago/Turabian StyleFiore, Vito, Andrea De Vito, Elena Rastrelli, Valentina Manca, Giuseppe De Matteis, Roberto Ranieri, Emanuele Pontali, Nicholas Geremia, Sandro Panese, Giulio Starnini, and et al. 2023. "Differences in HCV Seroprevalence, Clinical Features, and Treatment Outcomes between Female and Male Incarcerated Population: Results from a Matched Cohort Study" Viruses 15, no. 12: 2414. https://doi.org/10.3390/v15122414