
Remdesivir or Nirmatrelvir/Ritonavir Therapy for Omicron SARS-CoV-2 Infection in Hematological Patients and Cell Therapy Recipients
 , , , , , , , , and
on behalf of the Infectious Complications Subcommittee of the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group (GETH-TC)add
Show full author list
, , , , , , , , and
on behalf of the Infectious Complications Subcommittee of the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group (GETH-TC)add
Show full author list
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Inclusion Criteria, Variables of Interest and Clinical and Virological Monitoring
2.3. Definitions
2.4. Endpoints and Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Characteristics of SARS-CoV-2 Infection and Efficacy According to the Type of Antiviral Used
3.3. Univariate and Multivariate Analyses for Mortality
3.4. Cause of Death
3.5. Prolonged Shedding
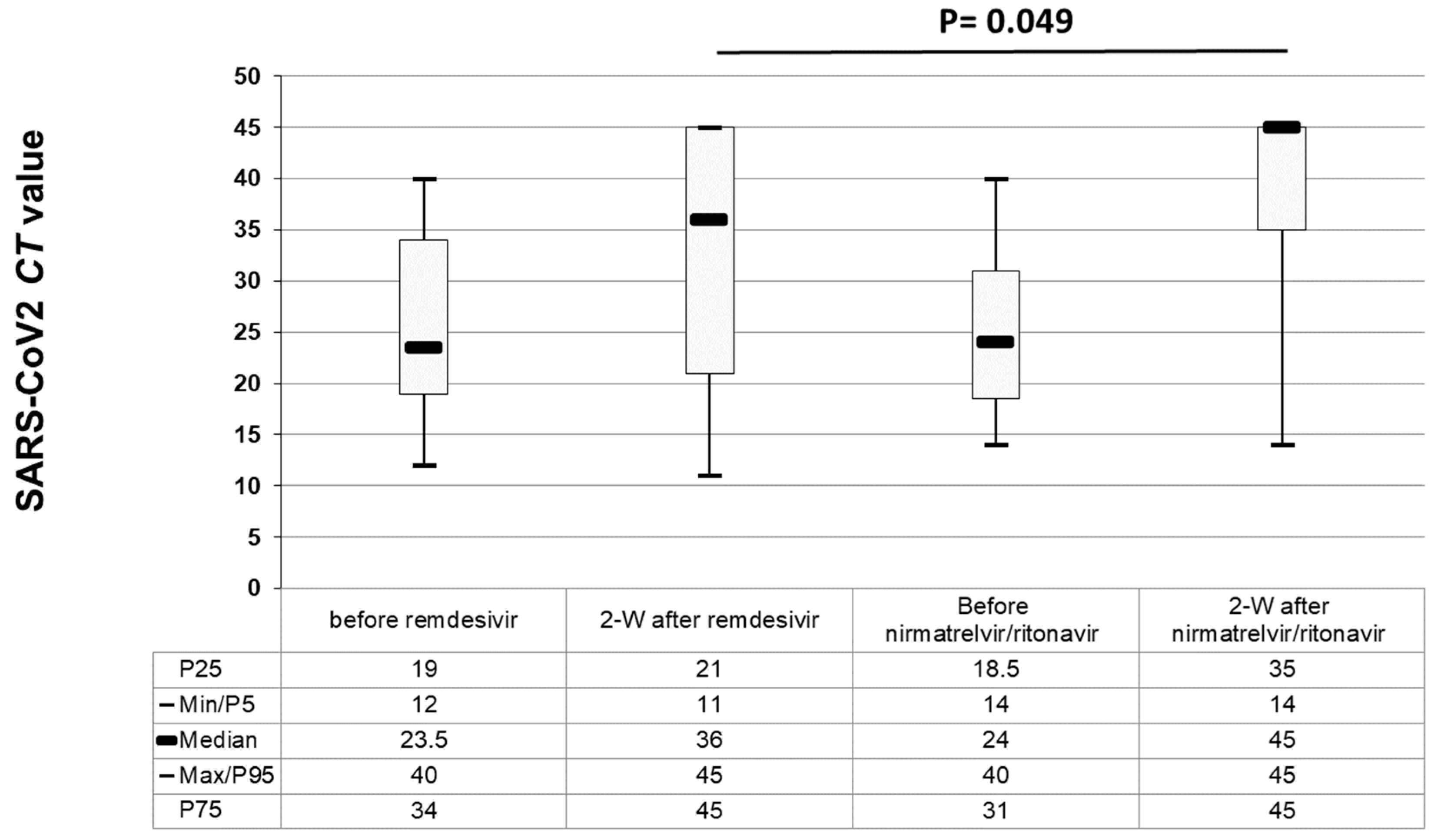
3.6. Antiviral Effect According to the Antiviral Drug
3.7. Tolerability of Antiviral Drugs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langerbeins, P.; Hallek, M. COVID-19 in patients with hematologic malignancy. Blood 2022, 140, 236–252. [Google Scholar]
- Ljungman, P.; de la Camara, R.; Mikulska, M.; Tridello, G.; Aguado, B.; Zahrani, M.A.; Apperley, J.; Berceanu, A.; Bofarull, R.M.; Calbacho, M.; et al. COVID-19 and stem cell transplantation; results from an EBMT and GETH multicenter prospective survey. Leukemia 2021, 35, 2885–2894. [Google Scholar] [CrossRef]
- Piñana, J.L.; Martino, R.; García-García, I.; Parody, R.; Morales, M.D.; Benzo, G.; Gómez-Catalan, I.; Coll, R.; De La Fuente, I.; Luna, A.; et al. Infectious Complications Subcommittee of the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group (GETH). Risk factors and outcome of COVID-19 in patients with hematological malignancies. Exp. Hematol. Oncol. 2020, 9, 21. [Google Scholar] [CrossRef]
- Piñana, J.L.; López-Corral, L.; Martino, R.; Vazquez, L.; Pérez, A.; Martin-Martin, G.; Gago, B.; Sanz-Linares, G.; Sanchez-Salinas, A.; Villalon, L.; et al. Infectious Complications Subcommittee of the Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group (GETH-TC). SARS-CoV-2 vaccine response and rate of infection in patients with hematological disorders. J. Hematol. Oncol. 2022, 15, 54. [Google Scholar] [CrossRef]
- Piñana, J.L.; Martino, R.; Vazquez, L.; López-Corral, L.; Pérez, A.; Chorão, P.; Avendaño-Pita, A.; Pascual, M.-J.; Sánchez-Salinas, A.; Sanz-Linares, G.; et al. Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group (GETH-TC). SARS-CoV-2-reactive antibody waning, booster effect and SARS-CoV-2 infection in hematopoietic stem cell transplant and cell therapy recipients at one year after vaccination. Bone Marrow Transpl. 2023, 58, 567–580. [Google Scholar] [CrossRef]
- Piñana, J.L.; Vazquez, L.; Calabuig, M.; López-Corral, L.; Martin-Martin, G.; Villalon, L.; Sanz-Linares, G.; Conesa-Garcia, V.; Sanchez-Salinas, A.; Gago, B.; et al. Spanish Hematopoietic Stem Cell Transplantation and Cell Therapy Group (GETH-TC). One-year SARS-CoV-2 infection and correlates of protection in fully vaccinated hematological patients. Blood Cancer J. 2023, 13, 8. [Google Scholar] [CrossRef]
- Ljungman, P.; Tridello, G.; Piñana, J.L.; Ciceri, F.; Sengeloev, H.; Kulagin, A.; Mielke, S.; Yegin, Z.A.; Collin, M.; Einardottir, S.; et al. Improved outcomes over time and higher mortality in CMV seropositive allogeneic stem cell transplantation patients with COVID-19; An infectious disease working party study from the European Society for Blood and Marrow Transplantation registry. Front. Immunol. 2023, 14, 1125824. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the treatment of Covid-19–final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Yang, L.; Wang, Z. Bench-to-bedside: Innovation of small molecule anti-SARS-CoV-2 drugs in China. Eur. J. Med. Chem. 2023, 257, 115503. [Google Scholar] [CrossRef]
- Zhang, J.L.; Li, Y.H.; Wang, L.L.; Liu, H.Q.; Lu, S.Y.; Liu, Y.; Li, K.; Liu, B.; Li, S.Y.; Shao, F.M.; et al. Azvudine is a thymus-homing anti-SARS-CoV-2 drug effective in treating COVID-19 patients. Signal. Transduct. Target Ther. 2021, 6, 414. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with Covid-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- Fischer, W.A., 2nd; Eron, J.J., Jr.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. A phase 2a clinical trial of molnupiravir in patients with COVID-19 shows accelerated SARS-CoV-2 RNA clearance and elimination of infectious virus. Sci. Transl. Med. 2022, 14, eabl7430. [Google Scholar] [CrossRef]
- Vangeel, L.; Chiu, W.; De Jonghe, S.; Maes, P.; Slechten, B.; Raymenants, J.; André, E.; Leyssen, P.; Neyts, J.; Jochmans, D. Remdesivir, Molnupiravir and Nirmatrelvir remain active against SARS-CoV-2 Omicron and other variants of concern. Antivir. Res. 2022, 198, 105252. [Google Scholar] [CrossRef] [PubMed]
- Cesaro, S.; Mikulska, M.; Hirsch, H.H.; Styczynski, J.; Meylan, S.; Cordonnier, C.; Navarro, D.; von Lilienfeld-Toal, M.; Mehra, V.; Marchesi, F.; et al. Update of recommendations for the management of COVID-19 in patients with haematological malignancies, haematopoietic cell transplantation and CAR T therapy, from the 2022 European Conference on Infections in Leukaemia (ECIL 9). Leukemia 2023, 37, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Salmanton-García, J.; Marchesi, F.; Gomes da Silva, M.; Farina, F.; Dávila-Valls, J.; Bilgin, Y.M.; Glenthøj, A.; Falces-Romero, I.; Van Doesum, J.; Labrador, J.; et al. EPICOVIDEHA registry. Nirmatrelvir/ritonavir in COVID-19 patients with haematological malignancies: A report from the EPICOVIDEHA registry. EClinicalMedicine 2023, 58, 101939. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Lin, Y.; Wang, X.; Gao, Y.; Ye, S. Paxlovid in patients who are immunocompromised and hospitalised with SARS-CoV-2 infection. Lancet Infect Dis. 2022, 22, 1279. [Google Scholar] [CrossRef] [PubMed]
- Magyari, F.; Pinczés, L.I.; Páyer, E.; Farkas, K.; Ujfalusi, S.; Diószegi, Á.; Sik, M.; Simon, Z.; Nagy, G.; Hevessy, Z.; et al. Early administration of remdesivir plus convalescent plasma therapy is effective to treat COVID-19 pneumonia in B-cell depleted patients with hematological malignancies. Ann. Hematol. 2022, 101, 2337–2345. [Google Scholar] [CrossRef]
- Aiello, T.F.; Puerta-Alcalde, P.; Chumbita, M.; Lopera, C.; Monzó, P.; Cortes, A.; Fernández-Avilés, F.; Suárez-Lledó, M.; Correa, J.; Ortiz-Maldonado, V.; et al. Current outcomes of SARS-CoV-2 Omicron variant infection in high-risk haematological patients treated early with antivirals. J. Antimicrob. Chemother. 2023, 78, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Høeg, T.B.; Duriseti, R.; Prasad, V. Potential “Healthy Vaccinee Bias” in a Study of BNT162b2 Vaccine against Covid-19. N. Engl. J. Med. 2023, 389, 284–285. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Chinn, J.; De Ferrante, M.; Kirby, K.A.; Hohmann, S.F.; Amin, A. Male gender is a predictor of higher mortality in hospitalized adults with COVID-19. PLoS ONE 2021, 16, e0254066. [Google Scholar] [CrossRef]
- Bischof, E.; Wolfe, J.; Klein, S.L. Clinical trials for COVID-19 should include sex as a variable. J. Clin. Investig. 2020, 130, 3350–3352. [Google Scholar] [CrossRef] [PubMed]
- Bienvenu, L.A.; Noonan, J.; Wang, X.; Peter, K. Higher mortality of COVID-19 in males: Sex differences in immune response and cardiovascular comorbidities. Cardiovasc Res. 2020, 116, 2197–2206. [Google Scholar]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [PubMed]
- Yoshida, Y.; Wang, J.; Zu, Y. Sex differences in comorbidities and COVID-19 mortality-Report from the real-world data. Front. Public Health 2022, 10, 881660. [Google Scholar] [CrossRef] [PubMed]
- Søvik, S.; Barrat-Due, A.; Kåsine, T.; Olasveengen, T.; Strand, M.W.; Tveita, A.A.; Berdal, J.E.; Lehre, M.A.; Lorentsen, T.; Heggelund, L.; et al. Corticosteroids and superinfections in COVID-19 patients on invasive mechanical ventilation. J. Infect. 2022, 85, 57–63. [Google Scholar] [CrossRef]
- Patton, M.J.; Orihuela, C.J.; Harrod, K.S.; Bhuiyan, M.A.N.; Dominic, P.; Kevil, C.G.; Fort, D.; Liu, V.X.; Farhat, M.; Koff, J.L.; et al. COVID-19 bacteremic co-infection is a major risk factor for mortality, ICU admission, and mechanical ventilation. Crit. Care 2023, 27, 34. [Google Scholar] [CrossRef]
- Fehér, Á.; Szarvas, Z.; Lehoczki, A.; Fekete, M.; Fazekas-Pongor, V. Co-infections in COVID-19 patients and correlation with mortality rate. Minireview Physiol. Int. 2022, 109, 1–8. [Google Scholar] [CrossRef]
- Piñana, J.L.; Xhaard, A.; Tridello, G.; Passweg, J.; Kozijn, A.; Polverelli, N.; Heras, I.; Perez, A.; Sanz, J.; Berghuis, D.; et al. Seasonal Human Coronavirus Respiratory Tract Infection in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation. J. Infect. Dis. 2021, 223, 1564–1575. [Google Scholar] [CrossRef]
- Piñana, J.L.; Tridelo, G.; Xhaard, A.; Wendel, L.; Montoro, J.; Vazquez, L.; Heras, I.; Ljungman, P.; Mikulska, M.; Salmenniemi, U.; et al. Upper and/or lower respiratory tract infection caused by human metapneumovirus after allogeneic hematopoietic stem cell transplantation. J. Infect. Dis. 2023, jiad268. [Google Scholar] [CrossRef]
- Chartrand, C.; Tremblay, N.; Renaud, C.; Papenburg, J. Diagnostic Accuracy of Rapid Antigen Detection Tests for Respiratory Syncytial Virus Infection: Systematic Review and Meta-analysis. J. Clin. Microbiol. 2015, 53, 3738–3749. [Google Scholar] [CrossRef]
- Seo, S.; Waghmare, A.; Scott, E.M.; Xie, H.; Kuypers, J.M.; Hackman, R.C.; Campbell, A.P.; Choi, S.-M.; Leisenring, W.M.; Jerome, K.R.; et al. Human rhinovirus detection in the lower respiratory tract of hematopoietic cell transplant recipients: Association with mortality. Haematologica 2017, 102, 1120–1130. [Google Scholar] [CrossRef]
- Seo, S.; Xie, H.; Campbell, A.P.; Kuypers, J.M.; Leisenring, W.M.; Englund, J.A.; Boeckh, M. Parainfluenza virus lower respiratory tract disease after hematopoietic cell transplant: Viral detection in the lung predicts outcome. Clin. Infect Dis. 2014, 58, 1357–1368. [Google Scholar] [CrossRef]
- Chemaly, R.F.; Hanmod, S.S.; Rathod, D.B.; Ghantoji, S.S.; Jiang, Y.; Doshi, A.; Vigil, K.; Adachi, J.A.; Khoury, A.M.; Tarrand, J.; et al. The characteristics and outcomes of parainfluenza virus infections in 200 patients with leukemia or recipients of hematopoietic stem cell transplantation. Blood 2012, 119, 2738–2745. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Aiello, T.F.; Salmanton-Garcia, J.; Marchesi, F.; Weinbergerova, B.; Glenthoj, A.; Van Praet, J.; Farina, F.; Davila-Valls, J.; Martín-Pérez, S.; El-Ashwah, S.; et al. Dexamethasone Treatment for COVID-19 is Related with Increased Mortality in Haematological Malignancy Patients: Results from the EPICOVIDEHA Registry. SSRN. Available online: https://ssrn.com/abstract=4473151 (accessed on 8 September 2023). [CrossRef]
- Aydillo, T.; Gonzalez-Reiche, A.S.; Aslam, S.; van de Guchte, A.; Khan, Z.; Obla, A.; Dutta, J.; van Bakel, H.; Aberg, J.; García-Sastre, A.; et al. Shedding of viable SARS-CoV-2 after immunosuppressive therapy for cancer. N. Engl. J. Med. 2020, 383, 2586–2588. [Google Scholar] [CrossRef]
- Avanzato, V.A.; Matson, M.J.; Seifert, S.N.; Pryce, R.; Williamson, B.N.; Anzick, S.L.; Barbian, K.; Judson, S.D.; Fischer, E.R.; Martens, C.; et al. Case study: Prolonged infectious SARS-CoV-2 shedding from an asymptomatic immunocompromised individual with cancer. Cell 2020, 183, 1901–1912.e9. [Google Scholar]
- Liu, Y.; Yan, L.M.; Wan, L.; Xiang, T.X.; Le, A.; Liu, J.M.; Peiris, M.; Poon, L.L.M.; Zhang, W. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect Dis. 2020, 20, 656–657. [Google Scholar] [CrossRef]
- Wu, J.; Li, W.; Shi, X.; Chen, Z.; Jiang, B.; Liu, J.; Wang, D.; Liu, C.; Meng, Y.; Cui, L.; et al. Early antiviral treatment con¬tributes to alleviate the severity and improve the prognosis of patients with novel coronavirus disease (COVID-19). J. Intern. Med. 2020, 288, 128–138. [Google Scholar] [CrossRef]
- McCullough, P.A.; Kelly, R.J.; Ruocco, G.; Lerma, E.; Tumlin, J.; Wheelan, K.R.; Katz, N.; Lepor, N.E.; Vijay, K.; Carter, H.; et al. Pathophysiological basis and rationale for early outpatient treatment of SARS-CoV-2 (COVID-19) infection. Am. J. Med. 2021, 134, 16–22. [Google Scholar] [CrossRef]
- Vassilopoulos, A.; Mylonakis, E. In patients with COVID-19 at risk for severe disease, nirmatrelvir + ritonavir reduced hospitalization or death. Ann. Intern. Med. 2022, 175, JC63. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L.; et al. Treatment of 5 critically ill patients with COVID-19 with convalescent plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Remdesivir Cohort (n = 243) | Nirmatrelvir/Ritonavir Cohort (n = 223) | p Value |
|---|---|---|---|
| Age (years), median (range) | 64 (19–92) | 65 (19–90) | 0.4 |
| • 0–40 years, n (%) | 18 (8) | 19 (9) | 0.28 |
| • 41–60 years, n (%) | 86 (35) | 66 (30) | |
| • 61–70 years, n (%) | 49 (20) | 60 (27) | |
| • >71 years, n (%) | 90 (37) | 78 (35) | |
| Male, n (%) | 150 (62) | 131 (59) | 0.63 |
| Baseline disease, n (%) | 0.34 | ||
| • AML | 41 (17) | 26 (12) | |
| • ALL | 9 (4) | 6 (3) | |
| • MDS | 21 (9) | 13 (6) | |
| • CMPD | 8 (3) | 7 (3) | |
| • B-cell NHL | 78 (32) | 88 (40) | |
| • T-cell NHL | 7 (3) | 2 (1) | |
| • CLL | 20 (8) | 12 (5) | |
| • Plasmatic cell disorder | 38 (16) | 57 (25.5) | |
| • HD | 12 (5) | 11 (5) | |
| • AA or others | 6 (2) | 1 (0.5) | |
| Time from last therapy to COVID-19 | 0.61 | ||
| • <6 months | 182 (75) | 158 (71) | |
| • 6–12 months | 19 (8) | 20 (9) | |
| • >12 months or not treated | 42 (17) | 45 (20) | |
| Anti-CD 20 and time from to COVID-19, n (%) | 74 (31) | 88 (40) | 0.13 |
| • <6 months | 56 (24) | 68 (31) | |
| • 6–12 months | 6 (3) | 3 (1.5) | |
| • >12 months or not treated | 12 (5) | 17 (8) | |
| Cell therapy, n (%) | 94 (39) | 81 (36) | 0.63 |
| - ASCT, n (%) | 36 (15) | 41 (18) | |
| - Allo-SCT donor, n (%) | 46 (19) | 25 (11) | |
| • HLA identical sibling | 21 (9) | 8 (3.6) | |
| • Unrelated Donor | 12 (5) | 9 (4) | |
| • Haplo-identical family donor | 12 (5) | 8 (3.6) | |
| • UCBT | 1 (0.5) | 0 | |
| - CAR-T type, n (%) | 12 (5) | 15 (7) | |
| • Axi-cell | 6 | 6 | |
| • Tisa-cell | 1 | 2 | |
| • Anti-BCMA | 1 | 1 | |
| • ARI-001 (anti-CD19) | 4 | 5 | |
| Corticosteroids at the time of COVID-19, n (%) | 68 (28) | 48 (22) | 0.1 |
| Number of vaccine doses, n (%) | 0.017 | ||
| • 0, n (%) | 22 (9) | 14 (6) | |
| • 1, n (%) | 8 (3) | 8 (4) | |
| • 2, n (%) | 56 (23) | 29 (13) | |
| • 3, n (%) | 87 (36) | 92 (41) | |
| • >3, n (%) | 70 (29) | 80 (36) | |
| Vaccination status ©, n (%) | 0.003 | ||
| • Incomplete | 86 (36) | 51 (23) | |
| • Complete | 157 (64) | 172 (77) | |
| Tixagevimab/cilgavimab pre-exposure prophylaxis n (%) | 4 (1.6) | 8 (3.6) | 0.25 |
| Pulmonary/cardiovascular RF, n (%) | |||
| • Active smoking | 21 (9) | 21 (9) | 0.87 |
| • Arterial hypertension | 105 (43) | 79 (35) | 0.2 |
| • Cardiomyopathy | 49 (20) | 30 (14) | 0.14 |
| • Pulmonary disease | 33 (14) | 15 (7) | 0.05 |
| Overall mortality, n (%) | 50 (21) | 20 (9) | <0.001 |
| Median F/U after COVID-19, days (range) | 119 (3–549) | 136 (5–539) | 0.4 |
| Characteristics | Remdesivir Cohort (n = 243) | Nirmatrelvir/Ritonavir Cohort (n = 223) | p Value |
|---|---|---|---|
| Diagnostic test, n (%) | <0.001 | ||
| • PCR | 218 (90) | 135 (60) | |
| • Antigen-test-based | 25 (10) | 88 (40) | |
| Asymptomatic, n (%) | 2 (1) | 6 (3) | 0.1 |
| Fever, n (%) | 127 (52) | 71 (32) | <0.001 |
| Respiratory symptoms, n (%) | 172 (71) | 107 (48) | <0.001 |
| Pneumonia, n (%) | 97 (40) | 14 (6) | <0.001 |
| COVID-19-related hospital admission, n (%) | 118 (49) | 19 (9) | <0.001 |
| Oxygen support, n (%) | 69 (28) | 5 (2) | <0.001 |
| COVID-19 severity, n (%) | <0.001 | ||
| • Mild | 146 (60) | 209 (94) | |
| • Moderate | 28 (12) | 9 (4) | |
| • Severe | 69 (28) | 5 (2) | |
| Median time from dx to ATV therapy, days (range) | 1 (0–57) | 1 (0–140) | |
| • <5 days, n (%) | 190 (78) | 203 (91) | <0.001 |
| • ≥5 days, n (%) | 53 (22) | 20 (9) | <0.001 |
| Median duration of ATV therapy, days (range) | 5 (1–19) | 5 (2–15) | |
| • <5 days, n (%) | 89 (37) | 4 (2) | <0.001 |
| • 5 days, n (%) | 100 (41) | 204 (91) | <0.001 |
| • >5 days, n (%) | 54 (22) | 15 (7) | <0.001 |
| Co-infection, n (%) | 46 (19) | 9 (4) | <0.001 |
| • Bacterial | 35 (14) | 5 (2) | |
| • viral | 6 (3) | 3 (1.5) | |
| • Fungal | 5 (2) | 1 (0.5) | |
| Other COVID-19 therapies, n (%) | <0.001 | ||
| • Sotrovimab | 43 (19) | 7 (3) | |
| • Tixagevimab/cilgavimab | 4 (2) | 0 | |
| ➢ Median onset after COVID-19, days (range) | 6 (0–129) | 62 (0–104) | <0.001 |
| • Convalescent plasma | 30 (12) | 6 (3) | <0.001 |
| • Corticosteroids as COVID-19 therapy | 79 (32) | 6 (3) | <0.001 |
| ➢ Median onset after COVID-19, days (range) | 2 (-5–46) | 8 (0–79) | <0.001 |
| Laboratory characteristics at the time of SARS-CoV-2 detection | |||
| (A) ANC < 0.5× 109/L, n/evaluable (%) | 18/144 (13) | 10/96 (10) | 0.2 |
| (B) ALC < 0.5× 109/L, n/evaluable (%) | 50/144 (35) | 30/96 (31) | 0.35 |
| • CRP > 8 IU/mL, n/evaluable, %) | 76/142 (53) | 50/90 (55) | 0.6 |
| • Ct value at diagnosis available, n (%) | 142 (58) | 104 (47) | 0.2 |
| • Ct value at diagnostic, median (range) | 20 (0–40) | 21 (9–40) | 0.8 |
| Recovery from COVID-19 at last F/U (n/evaluable, %) | 163/234 (70) | 170/173 (98) | <0.001 |
| • PCR monitoring (n/evaluable, %) | 128/243 (53) | 122/223 (55) | 0.3 |
| • PCR negativity at last F/U, n (%) | 132 (63) | 125 (69) | 0.45 |
| • Median time from diagnosis to negativity, days (range) | 31 (2–209) | 22 (2–237) | <0.001 |
| • Prolonged shedding, n/evaluable (%) | 80/128 (63) | 49/122 (40) | <0.001 |
| • COVID-19-related death, n (%) | 21 (9) | 3 (1.3) | <0.001 |
| Median time from diagnosis to death (range) | 30 (4–111) | 24 (18–77) | 0.2 |
| ICU admission, n (%) | 14 (6) | 1 (0.5) | 0.005 |
| Variables | Log. Regr. COVID-19 Mortality * (n = 21 Out of 243) | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| OR (95% C.I.) % (95%C.I.) | P | OR (95% C.I.) | P | |
| Age (years), | ||||
| • <41 years | 1 | |||
| • 41–60 years | 0.6 (0.06–6.2) | 0.68 | ||
| • 61–70 years | 1.5 (0.15–14.5) | 0.7 | ||
| • >71 years | 2.87 (0.35–23) | 0.3 | ||
| Male, n (%) | 0.41 (0.17–1.06) | 0.069 | 0.35 (0.13–0.96) | 0.042 |
| Baseline disease, n (%) | ns | |||
| • AML | 1 | |||
| • ALL | - | |||
| • MDS | 1.02 (0.12–3.5) | 0.8 | ||
| • CMPD | 1.7 (0.14–21) | 0.65 | ||
| • B-cell NHL | 3.9 (0.83–18) | 0.08 | ||
| • T-cell NHL | 3.2 (0.25–41) | 0.36 | ||
| • CLL | 3.44 (0.52–22) | 0.19 | ||
| • Plasmatic cell disorder | 0.52 (0.04–6.06) | 0.6 | ||
| • HD | - | |||
| • AA or others | - | |||
| Time from last therapy to COVID-19 | ||||
| • <6 months | 1 | |||
| • 6–12 months | 2.08 (0.54–7.9) | 0.28 | ||
| • >12 months or not treated | 0.85 (0.23–3.1) | 0.8 | ||
| Prior anti-CD20 therapy | 3.44 (1.38–8.5) | 0.008 | ns | |
| Time from anti-CD 20 to COVID-19, n (%) | ns | |||
| • No anti-CD20 | 1 | |||
| • <6 months | 2.47 (0.87–6.9) | 0.08 | ||
| • 6–12 months | 17.6 (3.12–100) | 0.001 | ||
| • >12 months or not treated | 3.5 (0.6–18.5) | 0.13 | ||
| Corticosteroids at the time of COVID-19 | 1.03 (0.38–2.7) | 0.9 | ||
| Procedure | ||||
| • Non-SCT | 0.88 (.27–3.2) | 0.8 | ||
| • Allo-SCT | 1 | |||
| • ASCT | 1.2 (0.06–5.6) | 0.8 | ||
| • CAR-T | 1.83 (0.25–13) | 0.54 | ||
| Vaccination status© | ||||
| • Complete | 1 | |||
| • Incomplete | 1.1 (0.45–2.85) | 0.78 | ||
| Pulmonary/cardiovascular risk factors, n (%) | ||||
| • Active smoking | 0.5 (0.06–3.9) | 0.5 | ||
| • Arterial hypertension | 2.8 (1.1–7.2) | 0.032 | ns | |
| • Cardiomyopathy | 3.3 (1.3–8.5) | 0.011 | ns | |
| • Pulmonary disease | 2.8 (1.01–7.8) | 0.05 | ns | |
| Other COVID-19 therapies | ||||
| • Convalescent plasma | 0.33 (0.04–2.5) | 0.29 | ||
| • Monoclonal antibodies | 0.99 (0.31–3.1) | 0.9 | ||
| • Corticosteroids | 11 (3.55–33.8) | <0.0001 | 9.4 (2.9–30.2) | <0.001 |
| Co-infection | 4.59 (1.8–11.6) | 0.001 | 2.8 (1.01–7.7) | 0.047 |
| ATV onset | ||||
| • <5 days | 1 | |||
| • ≥5 days | 1.48 (0.54–4.04) | 0.43 | ||
| Duration of remdesivir | ||||
| • <5 days | 1.13 (0.4–3.1) | 0.8 | ||
| • 5 days | 1 | |||
| • >5 days | 1.17 (0.36–3.78) | 0.78 | ||
| Ct value at diagnosis * | ||||
| • ≥20 | 1 | |||
| • <20 | 1.35 (0.41–4.3) | 0.61 | ||
| CRP > 8 UI/mL * | 1.8 (0.5–5.2) | 0.9 | ||
| ALC < 0.5 × 109/L * | 0.74 (0.13–3.9) | 0.7 | ||
| ANC < 0.5 × 109/L * | 1.1 (0.13–10.2) | 0.9 | ||
| Remdesivir Cohort Ω SARS-CoV-2 Shedding | Nirmatrelvir/Ritonavir Cohort Ω SARS-CoV-2 Shedding | |||||
|---|---|---|---|---|---|---|
| Variable | Median Days (Range) | n | p Value | Median Days (Range) | n | p Value |
| Age | 0.25 | 0.87 | ||||
| • <41 years | 21 (2–32) | 7 | 17 (6–95) | 12 | ||
| • 41–60 years | 30 (2–162) | 55 | 20.5 (2–220) | 40 | ||
| • 61–70 years | 30 (1–208) | 32 | 17.5 (2–132) | 30 | ||
| • >71 years | 25 (2–108) | 34 | 21 (2–167) | 40 | ||
| SARS-CoV-2 infection severity | 0.013 | NT | ||||
| • Mild | 27 (2–162) | 91 | 20 (2–220) | 116 | ||
| • Moderate | 27.5 (3–108) | 16 | 7.5 (2–25) | 4 | ||
| • Severe | 39 (1–208) | 21 | 5 (2–8) | 2 | ||
| Fever | 0.035 | 0.83 | ||||
| • Yes | 32 (1–208) | 61 | 20 (2–122) | 42 | ||
| • No | 23 (2–162) | 67 | 19.5 (2–220) | 80 | ||
| Corticosteroids at infection | 0.82 | 0.13 | ||||
| • Yes | 31 (3–208) | 39 | 14.5 (2–75) | 32 | ||
| • No | 28 (1–162) | 89 | 21 (2–220) | 90 | ||
| Pneumonia | 0.022 | NT | ||||
| • Yes | 34 (1–208) | 37 | 7.5 (2–25) | 6 | ||
| • No | 27 (2–162) | 91 | 20.5 (2–220) | 116 | ||
| Hospital admission | 0.15 | 0.88 | ||||
| • Yes | 30 (1–117) | 69 | 25 (2–52) | 11 | ||
| • No | 24 (2–208) | 59 | 20 (2–220) | 111 | ||
| Oxygen requirement | 0.022 | 0.8 | ||||
| • Yes | 39 (1–208) | 21 | 5 (2–8) | 2 | ||
| • No | 26.5 (2–162) | 106 | 20 (2–220) | 120 | ||
| Monoclonal antibodies | 0.055 | 0.82 | ||||
| • Yes | 35 (7–162) | 26 | 20.5 (2–132) | 11 | ||
| • No | 25 (1–208) | 98 | 20 (2–220) | 111 | ||
| Convalescent plasma | 0.7 | 0.49 | ||||
| • Yes | 30 (4–106) | 24 | 25 (2–59) | 5 | ||
| • No | 28 (1–208) | 104 | 19 (2–220) | 117 | ||
| Corticosteroids for COVID-19 therapy | 0.004 | 0.11 | ||||
| • Yes | 37 (1–208) | 31 | 2 (2–25) | 3 | ||
| • No | 26 (2–117) | 97 | 20 (2–220) | 119 | ||
| Time from last therapy to COVID-19 | 0.49 | 0.87 | ||||
| • <6 months | 29 (1–162) | 104 | 19.5 (2–167) | 90 | ||
| • 6–12 months | 29 (11–62) | 9 | 18.5 (2–122) | 12 | ||
| • >12 months or not treated | 17 (3–208) | 15 | 22.5 (2–220) | 18 | ||
| Anti-CD20 | 0.015 | 0.34 | ||||
| • Yes | 33 (1–162) | 39 | 20 (2–220) | 59 | ||
| • No | 27 (2–208) | 89 | 20 (2–167) | 63 | ||
| Time from anti-CD 20 to COVID-19 | 0.027 | 0.69 | ||||
| • <6 months | 34 (1–162) | 32 | 20 (6–132) | 49 | ||
| • 6–12 months | 67.5 (62–73) | 2 | 32 (2–63) | 2 | ||
| • >12 months | 29 (7–63) | 5 | 16 (2–220) | 8 | ||
| • Not treated | 27 (2–208) | 89 | 20 (2–167) | 63 | ||
| B-cell NHL/CLL vs. others | 0.005 | 0.61 | ||||
| • Yes | 33 (1–162) | 49 | 19.5 (2–220) | 64 | ||
| • No | 25 (2–208) | 79 | 20.5 (2–167) | 58 | ||
| Ct value at diagnosis * | 0.001 | 0.82 | ||||
| • ≥20 | 19 (2–108) | 49 | 19 (2–90) | 28 | ||
| • <20 | 38 (1–208) | 47 | 21 (5–95) | 34 | ||
| ATV onset from the first positive PCR | 0.008 | 0.6 | ||||
| • <5 days | 27.5 (2–208) | 100 | 20 (2–167) | 110 | ||
| • ≥5 days | 31 (1–162) | 28 | 20.5 (2–220) | 12 | ||
| Duration of ATV | 0.001 | 0.83 | ||||
| • <5 days | 19 (2–89) | 42 | 21 (20–21) | 2 | ||
| • 5 days | 33 (1–208) | 52 | 19 (2–220) | 108 | ||
| • >5 days | 31.5 (4–108) | 34 | 24 (4–132) | 12 | ||
| Co-infections | 0.34 | 0.63 | ||||
| • Yes | 34 (2–208) | 17 | 38 (13–63) | 2 | ||
| • No | 27 (1–162) | 111 | 20 (2–220) | 120 | ||
| ANC < 0.5 × 109/L | 0.4 | 0.25 | ||||
| • Yes | 38 (2–108) | 11 | 14 (6–51) | 5 | ||
| • No | 30 (1–117) | 77 | 24 (2–122) | 49 | ||
| ALC < 0.5 × 109/L | 0.1 | 0.81 | ||||
| • Yes | 35 (2–117) | 36 | 20.5 (2–122) | 18 | ||
| • No | 27 (1–90) | 52 | 23 (2–95) | 36 | ||
| Vaccination status | 0.039 | 0.28 | ||||
| • Complete | 31 (1–208) | 82 | 20 (2–220) | 93 | ||
| • Incomplete | 24.5 (2–90) | 46 | 18 (2–167) | 29 | ||
| Characteristics | Remdesivir (n = 194) | Nirmatrelvir/Ritonavir (n = 223) | p Value |
|---|---|---|---|
| Risk of drug–drug interactions, n (%) | 0.001 | ||
| • Baseline treatment modification | 1 (0.5) | 5 (2.2) | |
| • ATV dose modification | 1 (0.5) | 9 (4) | |
| • Early ATV interruption | 27 (14) | 38 (17) | |
| • Treatment completed | 165 (68) | 120 (54) | |
| Adverse events ≥ grade 3, n (%) | 1 (0.5) | 3 (1.3) | 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piñana, J.L.; Heras, I.; Aiello, T.F.; García-Cadenas, I.; Vazquez, L.; Lopez-Jimenez, J.; Chorão, P.; Aroca, C.; García-Vidal, C.; Arroyo, I.; et al. Remdesivir or Nirmatrelvir/Ritonavir Therapy for Omicron SARS-CoV-2 Infection in Hematological Patients and Cell Therapy Recipients. Viruses 2023, 15, 2066. https://doi.org/10.3390/v15102066
Piñana JL, Heras I, Aiello TF, García-Cadenas I, Vazquez L, Lopez-Jimenez J, Chorão P, Aroca C, García-Vidal C, Arroyo I, et al. Remdesivir or Nirmatrelvir/Ritonavir Therapy for Omicron SARS-CoV-2 Infection in Hematological Patients and Cell Therapy Recipients. Viruses. 2023; 15(10):2066. https://doi.org/10.3390/v15102066
Chicago/Turabian StylePiñana, José Luis, Inmaculada Heras, Tommaso Francesco Aiello, Irene García-Cadenas, Lourdes Vazquez, Javier Lopez-Jimenez, Pedro Chorão, Cristina Aroca, Carolina García-Vidal, Ignacio Arroyo, and et al. 2023. "Remdesivir or Nirmatrelvir/Ritonavir Therapy for Omicron SARS-CoV-2 Infection in Hematological Patients and Cell Therapy Recipients" Viruses 15, no. 10: 2066. https://doi.org/10.3390/v15102066