
Drug Repositioning for Hand, Foot, and Mouth Disease

 , ,
, ,
Abstract
:1. Introduction
2. Major Outbreaks of HFMD
3. Drug Repositioning for HFMD
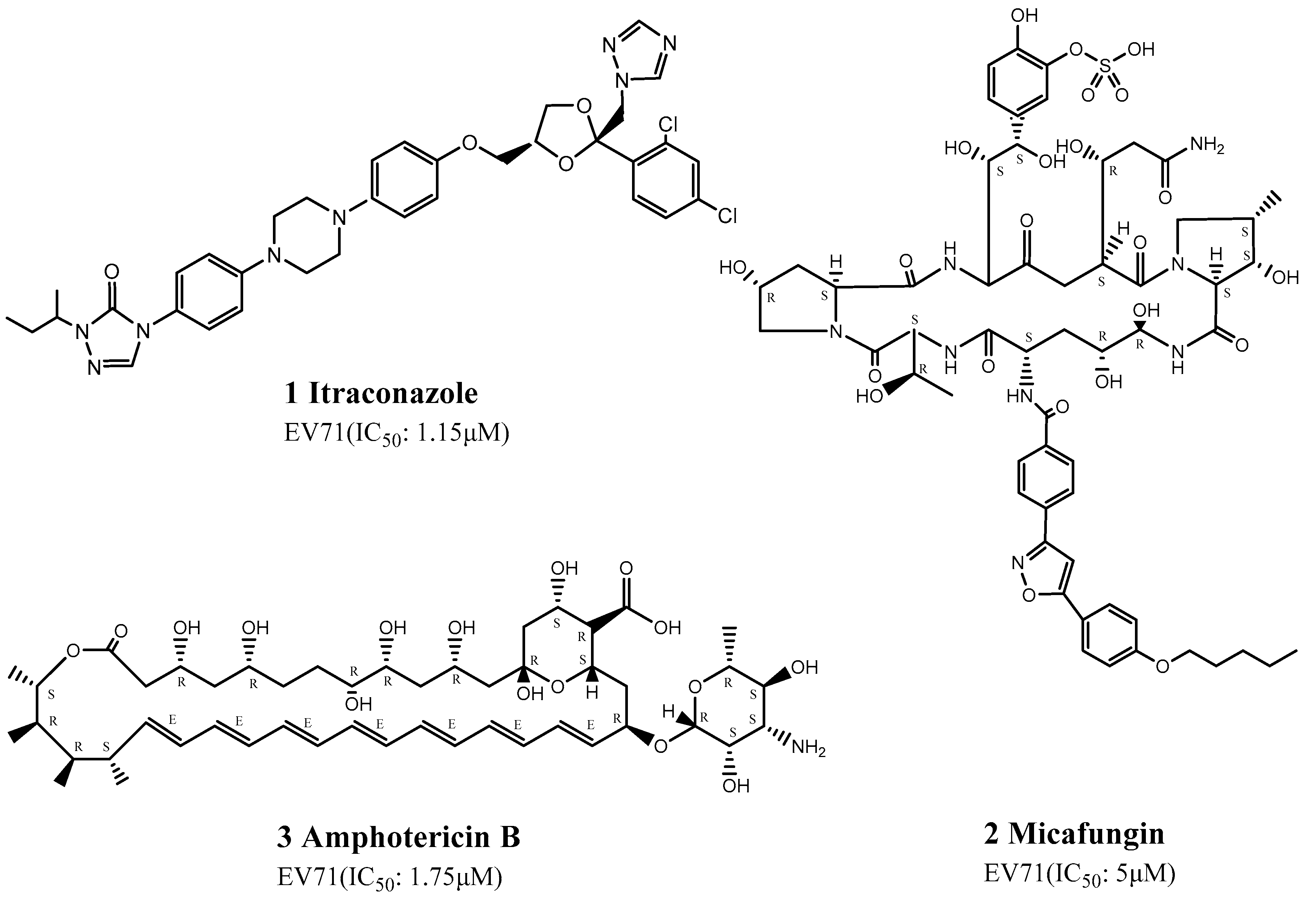
3.1. Repositioning of Antifungal Drugs
3.2. Repositioning of Antibacterial Drugs
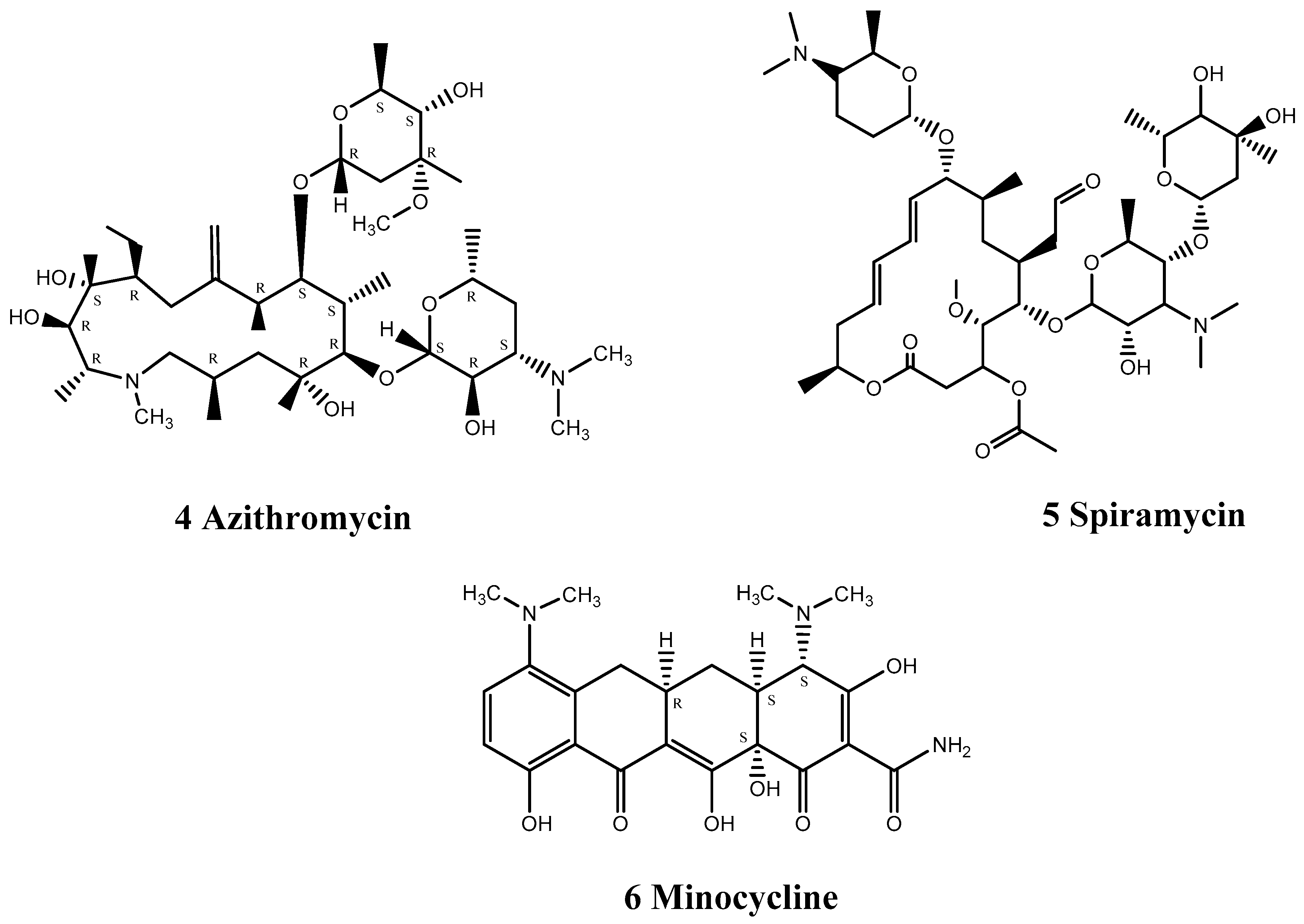
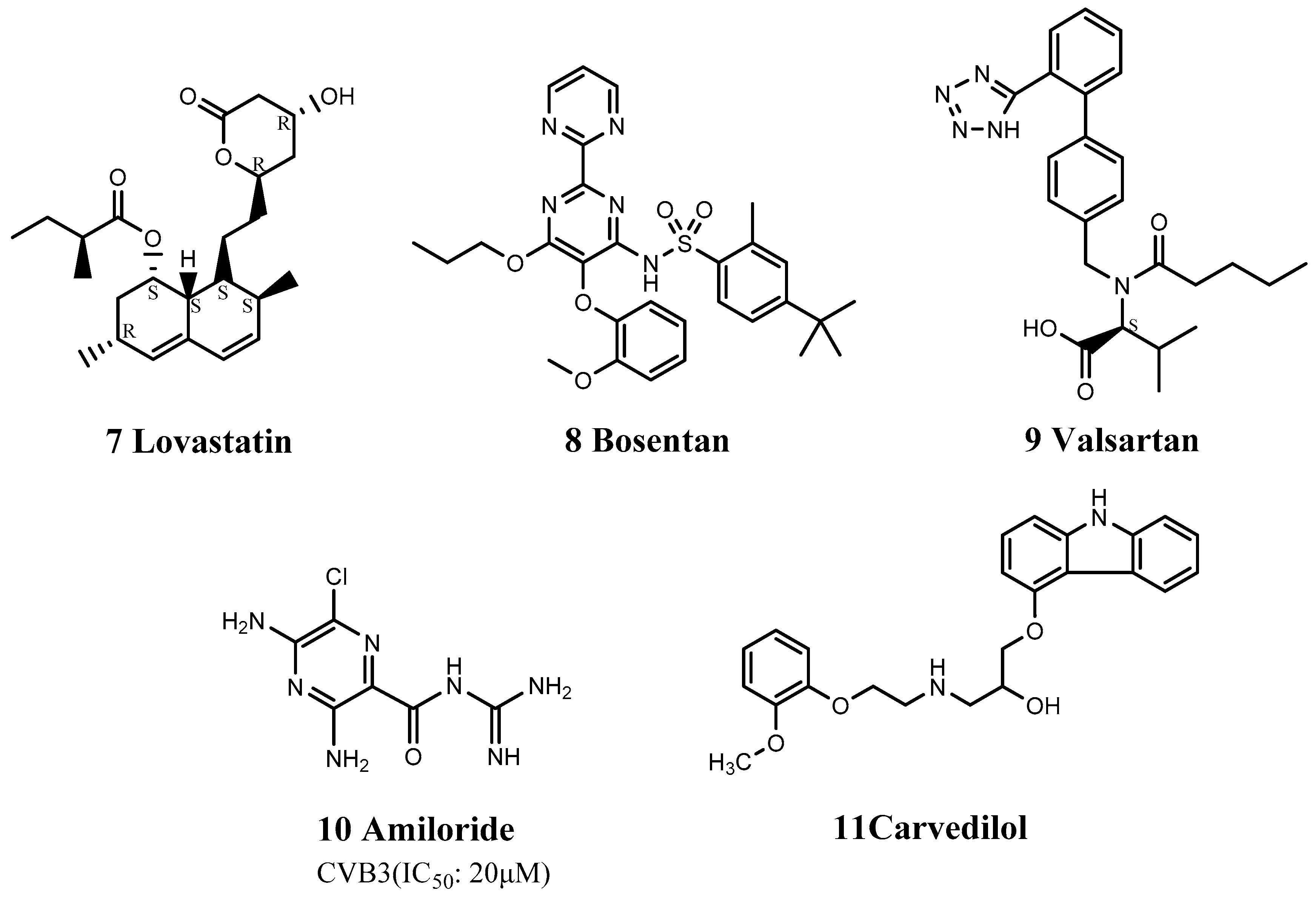
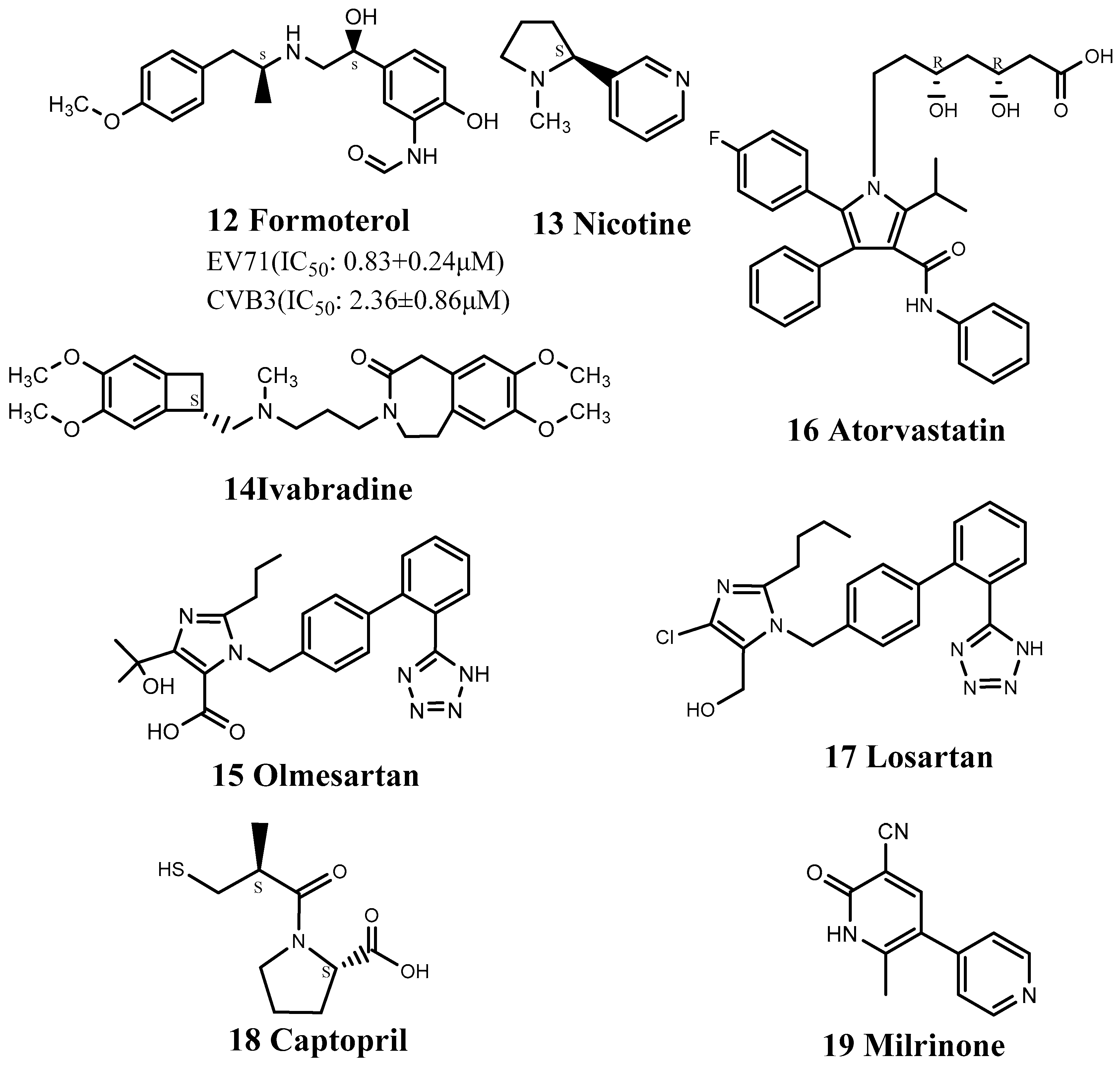
3.3. Repositioning of Cardiovascular Drugs
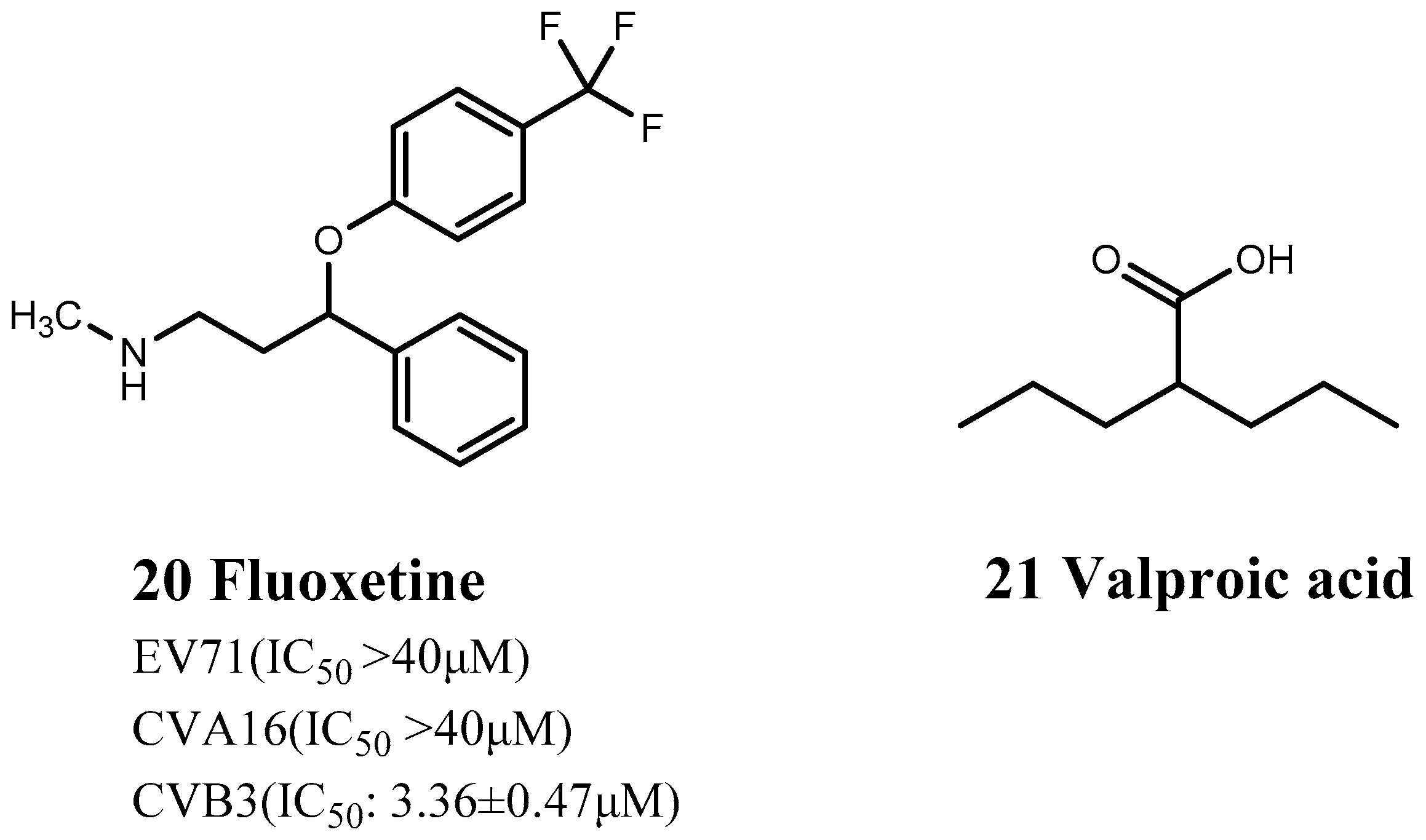
3.4. Repositioning of Nervous System Drugs
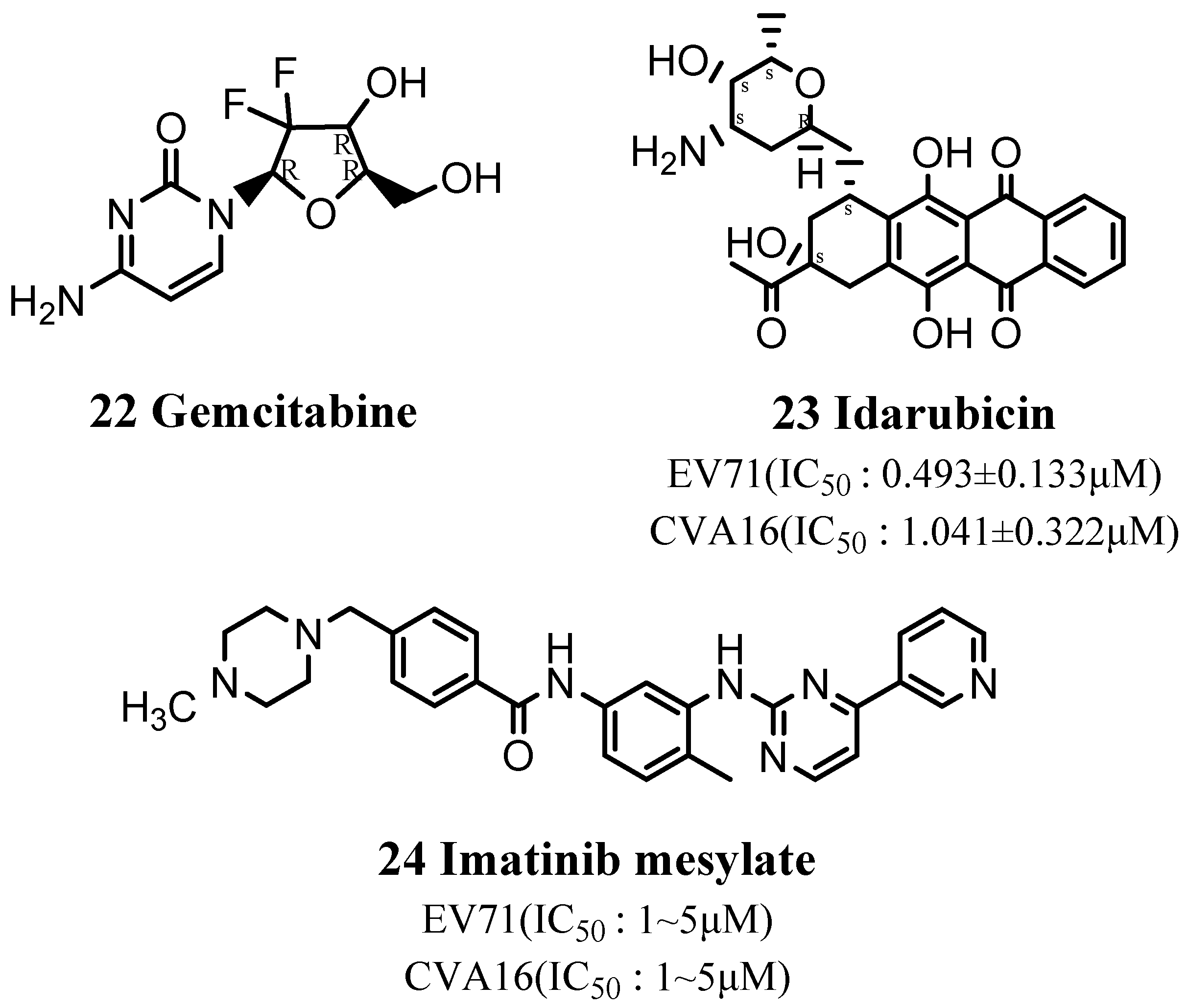
3.5. Repositioning of Anticancer Drugs
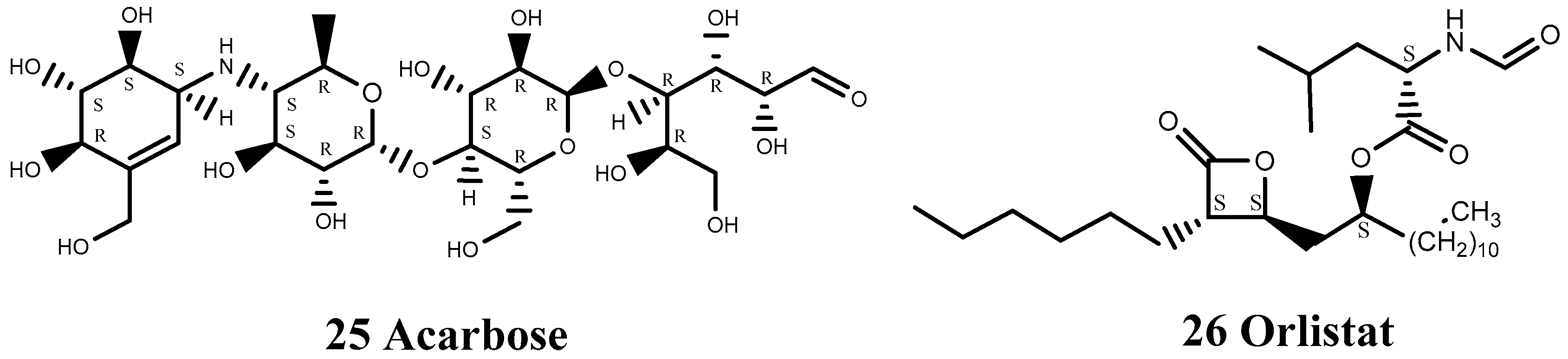
3.6. Repositioning of Antidiabetic and Anti-Obesity Drugs
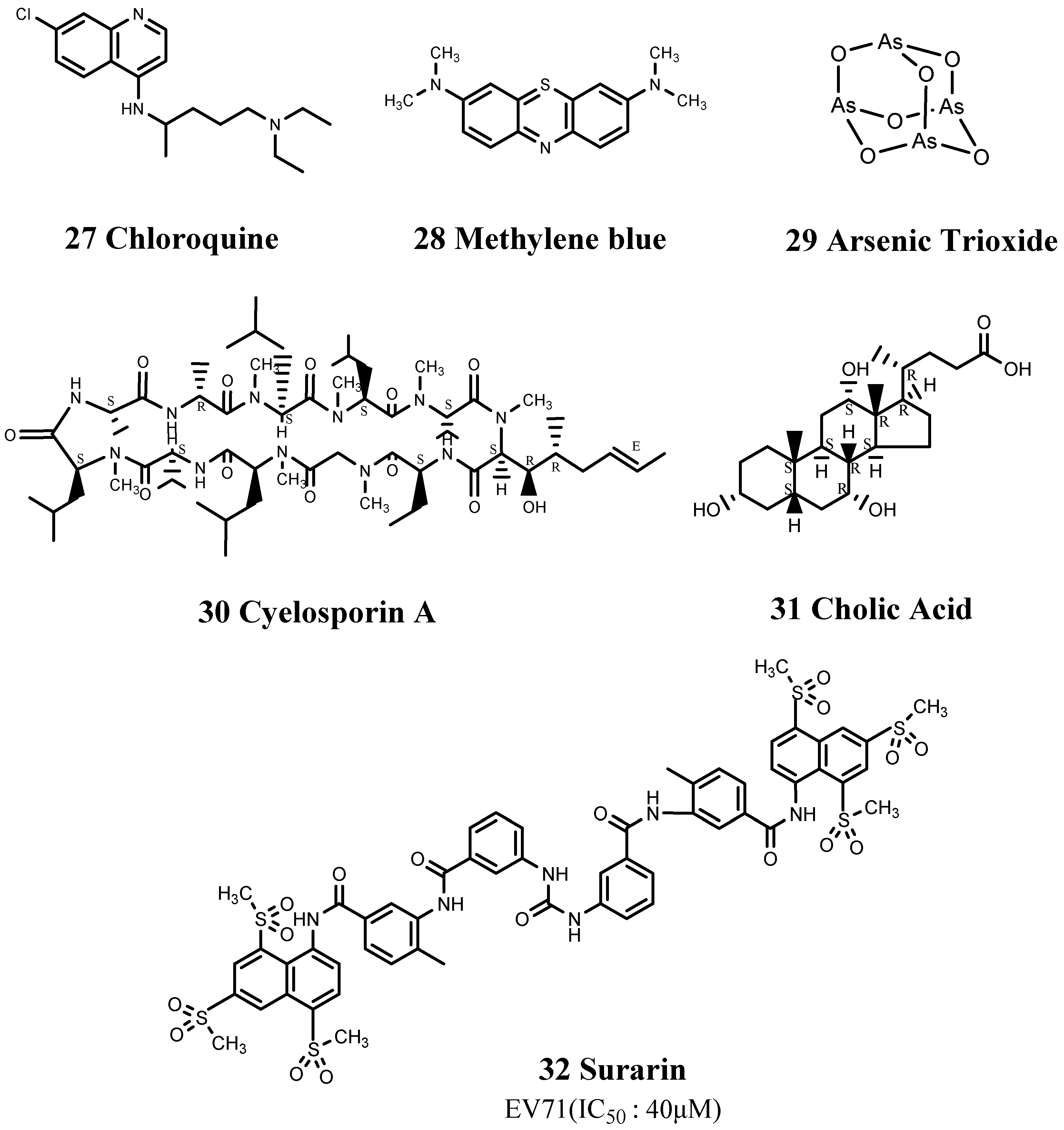
3.7. Repositioning of Other Drugs
4. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Esposito, S.; Principi, N. Hand, foot and mouth disease: Current knowledge on clinical manifestations, epidemiology, aetiology and prevention. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Muehlenbachs, A.; Bhatnagar, J.; Zaki, S.R. Tissue tropism, pathology and pathogenesis of enterovirus infection. J. Pathol. 2015, 235, 217–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimmis, B.D.; Downing, C.; Tyring, S. Hand-foot-and-mouth disease caused by coxsackievirus A6 on the rise. Cutis 2018, 102, 353–356. [Google Scholar]
- Li, X.W.; Ni, X.; Qian, S.Y.; Wang, Q.; Jiang, R.M.; Xu, W.B.; Zhang, Y.C.; Yu, G.J.; Chen, Q.; Shang, Y.X.; et al. Chinese guidelines for the diagnosis and treatment of hand, foot and mouth disease (2018 edition). World J. Pediatr. 2018, 14, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Sahebnasagh, A.; Avan, R.; Saghafi, F.; Mojtahedzadeh, M.; Sadremomtaz, A.; Arasteh, O.; Tanzifi, A.; Faramarzi, F.; Negarandeh, R.; Safdari, M.; et al. Pharmacological treatments of COVID-19. Pharmacol. Rep. 2020, 72, 1446–1478. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Peng, T. Strategy, Progress, and Challenges of Drug Repurposing for Efficient Antiviral Discovery. Front. Pharmacol. 2021, 12, 660710. [Google Scholar] [CrossRef]
- Jourdan, J.-P.; Bureau, R.; Rochais, C.; Dallemagne, P. Drug repositioning: A brief overview. J. Pharm. Pharmacol. 2020, 72, 1145–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.L.; Pan, H.; Liu, P.; Amer, S.; Chan, T.C.; Zhan, J.; Huo, X.; Liu, Y.; Teng, Z.; Wang, L.; et al. Comparative epidemiology and virology of fatal and nonfatal cases of hand, foot and mouth disease in mainland China from 2008 to 2014. Rev. Med. Virol. 2015, 25, 115–128. [Google Scholar] [CrossRef]
- Chan, Y.F.; Wee, K.L.; Chiam, C.W.; Khor, C.S.; Chan, S.Y.; Amalina, W.M.Z.; Sam, I.C. Comparative genetic analysis of VP4, VP1 and 3D gene regions of enterovirus 71 and coxsackievirus A16 circulating in Malaysia between 1997–2008. Trop. Biomed. 2012, 29, 451–466. [Google Scholar]
- Melnick, J.L.; Tagaya, I.; von Magnus, H. Enteroviruses 69, 70, and 71. Intervirology 1974, 4, 369–370. [Google Scholar] [CrossRef]
- Cai, K.; Wang, Y.; Guo, Z.; Yu, H.; Li, H.; Zhang, L.; Xu, S.; Zhang, Q. Clinical characteristics and managements of severe hand, foot and mouth disease caused by enterovirus A71 and coxsackievirus A16 in Shanghai, China. BMC Infect. Dis. 2019, 19, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melnick, J.L.; Schmidt, N.J.; Mirkovic, R.R.; Chumakov, M.P.; Lavrova, I.K.; Voroshilova, M.K. Identification of Bulgarian strain 258 of enterovirus 71. Intervirology 1980, 12, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yeo, A.; Phoon, M.C.; Tan, E.L.; Poh, C.L.; Quak, S.H.; Chow, V.T.K. The largest outbreak of hand; foot and mouth disease in Singapore in 2008: The role of enterovirus 71 and coxsackievirus A strains. Int. J. Infect. Dis. 2010, 14, e1076–e1081. [Google Scholar] [CrossRef] [Green Version]
- Kapusinszky, B.; Szomor, K.N.; Farkas, A.; Takács, M.; Berencsi, G. Detection of non-polio enteroviruses in Hungary 2000–2008 and molecular epidemiology of enterovirus 71, coxsackievirus A16, and echovirus 30. Virus Genes 2010, 40, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-H.; Huang, L.M.; Wong, W.-W.; Wu, T.-Z.; Chiu, T.-F.; Chang, L.-Y. Molecular diagnosis and clinical presentations of enteroviral infections in Taipei during the 2008 epidemic. J. Microbiol. Immunol. Infect. 2011, 44, 178–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortner, B.; Huang, C.-W.; Schmid, D.; Mutz, I.; Wewalka, G.; Allerberger, F.; Yang, J.-Y.; Huemer, H.P. Epidemiology of enterovirus types causing neurological disease in Austria 1999–2007: Detection of clusters of echovirus 30 and enterovirus 71 and analysis of prevalent genotypes. J. Med. Virol. 2009, 81, 317–324. [Google Scholar] [CrossRef]
- Mizuta, K.; Aoki, Y.; Matoba, Y.; Yahagi, K.; Itagaki, T.; Katsushima, F.; Katsushima, Y.; Ito, S.; Hongo, S.; Matsuzaki, Y. Molecular epidemiology of enterovirus 71 strains isolated from children in Yamagata, Japan, between 1990 and 2013. J. Med. Microbiol. 2014, 63 Pt 10, 1356–1362. [Google Scholar] [CrossRef]
- van der Sanden, S.; Koopmans, M.; Uslu, G.; van der Avoort, H. Epidemiology of enterovirus 71 in the Netherlands, 1963 to 2008. J. Clin. Microbiol. 2009, 47, 2826–2833. [Google Scholar] [CrossRef] [Green Version]
- Le, T.V.; Nguyen, V.T.T.; Nguyen, Q.H.; Pham, D.T. Molecular epidemiology analysis of enterovirus 71 strains isolated in Dak Lak, Vietnam, 2011–2016. J. Med. Virol. 2019, 91, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Badran, S.A.; Midgley, S.; Andersen, P.; Böttiger, B. Clinical and virological features of enterovirus 71 infections in Denmark, 2005 to 2008. Scand. J. Infect. Dis. 2011, 43, 642–648. [Google Scholar] [CrossRef]
- Akhmadishina, L.V.; Eremeeva, T.P.; Trotsenko, O.E.; Ivanova, O.E.; Mikhailov, M.I.; Lukashev, A.N. Seroepidemiology and molecular epidemiology of enterovirus 71 in Russia. PLoS ONE 2014, 9, e97404. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.Y.Q.; Gonfrier, G.; Ninove, L.; Zandotti, C.; Dubot-Pérès, A.; de Lamballerie, X.; Charrel, R.N. Screening and detection of human enterovirus 71 infection by a real-time RT-PCR assay in Marseille, France, 2009–2011. Clin. Microbiol. Infect. 2012, 18, E77–E80. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.H.; Lau, C.S.; Cheng, P.K.C.; Ng, A.Y.Y.; Lim, W.W.L. Coxsackievirus B3-associated aseptic meningitis: An emerging infection in Hong Kong. J. Med. Virol. 2011, 83, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Wieczorek, M.; Krzysztoszek, A. Molecular Characterization of Enteroviruses Isolated from Acute Flaccid Paralysis Cases in Poland, 1999–2014. Pol. J. Microbiol. 2017, 65, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laxmivandana, R.; Cherian, S.S.; Yergolkar, P.; Chitambar, S.D. Genomic characterization of coxsackievirus type B3 strains associated with acute flaccid paralysis in south-western India. J. Gen. Virol. 2016, 97, 694–705. [Google Scholar] [CrossRef]
- Tian, H.; Zhang, Y.; Sun, Q.; Zhu, S.; Li, X.; Pan, Z.; Xu, W.; Xu, B. Prevalence of multiple enteroviruses associated with hand, foot, and mouth disease in Shijiazhuang City, Hebei province, China: Outbreaks of coxsackieviruses a10 and b3. PLoS ONE 2014, 9, e84233. [Google Scholar] [CrossRef]
- Han, Z.; Zhang, Y.; Huang, K.; Wang, J.; Tian, H.; Song, Y.; Yang, Q.; Yan, D.; Zhu, S.; Yao, M.; et al. Two Coxsackievirus B3 outbreaks associated with hand, foot, and mouth disease in China and the evolutionary history worldwide. BMC Infect. Dis. 2019, 19, 466. [Google Scholar] [CrossRef] [Green Version]
- Mao, Q.; Wang, Y.; Yao, X.; Bian, L.; Wu, X.; Xu, M.; Liang, Z. Coxsackievirus A16: Epidemiology, diagnosis, and vaccine. Hum. Vaccin Immunother. 2014, 10, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.R.; Doane, F.W.; Rhodes, A.J. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957; isolation of group A Coxsackie virus. Can. Med. Assoc. J. 1958, 79, 615–621. [Google Scholar]
- Alsop, J.; Flewett, T.H.; Foster, J.R. “Hand-foot-and-mouth disease” in Birmingham in 1959. Br. Med. J. 1960, 2, 1708–1711. [Google Scholar] [CrossRef]
- Richardson, H.B.; Leibovitz, A. “Hand, Foot, and Mouth Disease” in Children.; an Epidemic Associated with Coxsakie Virus a-16. J. Pediatr. 1965, 67, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Rabenau, H.F.; Richter, M.; Doerr, H.W. Hand, foot and mouth disease: Seroprevalence of Coxsackie A16 and Enterovirus 71 in Germany. Med. Microbiol. Immunol. 2010, 199, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Gopalkrishna, V.; Patil, P.R.; Patil, G.P.; Chitambar, S.D. Circulation of multiple enterovirus serotypes causing hand, foot and mouth disease in India. J. Med. Microbiol. 2012, 61 Pt 3, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Aswathyraj, S.; Arunkumar, G.; Alidjinou, E.K.; Hober, D. Hand, foot and mouth disease (HFMD): Emerging epidemiology and the need for a vaccine strategy. Med. Microbiol. Immunol. 2016, 205, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Di, B.; Zhang, Y.; Xie, H.; Li, X.; Chen, C.; Ding, P.; He, P.; Wang, D.; Geng, J.; Luo, L.; et al. Circulation of Coxsackievirus A6 in hand-foot-mouth disease in Guangzhou, 2010–2012. Virol. J. 2014, 11, 157. [Google Scholar] [CrossRef] [Green Version]
- Mirand, A.; Henquell, C.; Archimbaud, C.; Ughetto, S.; Antona, D.; Bailly, J.L.; Peigue-Lafeuille, H. Outbreak of hand, foot and mouth disease/herpangina associated with coxsackievirus A6 and A10 infections in 2010, France: A large citywide, prospective observational study. Clin. Microbiol. Infect. 2012, 18, E110–E118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Zhu, R.; Huo, D.; Du, Y.; Yan, Y.; Liang, Z.; Luo, Y.; Yang, Y.; Jia, L.; Chen, L.; et al. An outbreak of Coxsackievirus A6-associated hand, foot, and mouth disease in a kindergarten in Beijing in 2015. BMC Pediatr. 2018, 18, 277. [Google Scholar] [CrossRef]
- Montes, M.; Artieda, J.; Piñeiro, L.D.; Gastesi, M.; Diez-Nieves, I.; Cilla, G. Hand, foot, and mouth disease outbreak and coxsackievirus A6, northern Spain, 2011. Emerg. Infect. Dis. 2013, 19, 676–678. [Google Scholar] [CrossRef]
- Puenpa, J.; Chieochansin, T.; Linsuwanon, P.; Korkong, S.; Thongkomplew, S.; Vichaiwattana, P.; Theamboonlers, A.; Poovorawan, Y. Hand, foot, and mouth disease caused by coxsackievirus A6, Thailand, 2012. Emerg. Infect. Dis. 2013, 19, 641–643. [Google Scholar] [CrossRef] [Green Version]
- Bian, L.; Gao, F.; Mao, Q.; Sun, S.; Wu, X.; Liu, S.; Yang, X.; Liang, Z. Hand, foot, and mouth disease associated with coxsackievirus A10: More serious than it seems. Expert. Rev. Anti Infect. Ther. 2019, 17, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.-Y.; Tyan, Y.-C.; Chen, Y.-S.; Chen, H.-L.; Lu, P.-L.; Chen, Y.-H.; Chen, B.-C.; Huang, T.-S.; Wang, C.-F.; Su, H.-J.; et al. Transmission and Demographic Dynamics of Coxsackievirus B1. PLoS ONE 2015, 10, e0129272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Nonpolio enterovirus and human parechovirus surveillance—United States, 2006–2008. MMWR Morb. Mortal. Wkly. Rep. 2010, 59, 1577–1580. [Google Scholar]
- Kim, H.; Kang, B.; Hwang, S.; Hong, J.; Chung, J.; Kim, S.; Jeong, Y.-S.; Kim, K.; Cheon, D.-S. Molecular characteristics of human coxsackievirus B1 infection in Korea, 2008–2009. J. Med. Virol. 2013, 85, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Bracho, M.A.; González-Candelas, F.; Valero, A.; Córdoba, J.; Salazar, A. Enterovirus co-infections and onychomadesis after hand, foot, and mouth disease, Spain, 2008. Emerg. Infect. Dis. 2011, 17, 2223–2231. [Google Scholar] [CrossRef]
- Ji, H.; Fan, H.; Lu, P.-X.; Zhang, X.-F.; Ai, J.; Shi, C.; Huo, X.; Bao, C.-J.; Shan, J.; Jin, Y. Surveillance for severe hand, foot, and mouth disease from 2009 to 2015 in Jiangsu province: Epidemiology, etiology, and disease burden. BMC Infect. Dis. 2019, 19, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Cássia Compagnoli Carmona, R.; Machado, B.C.; de Sousa, C.A.; Vieira, H.R.; Alves, M.R.M.; de Souza, K.A.F.; de Souza Gregório, D.; Vilanova, B.C.; Timenetsky, M.d.C.S.T. Distribution of species Enterovirus B in patients with central nervous system infections in São Paulo State, Brazil. J. Med. Virol. 2020, 92, 3849–3856. [Google Scholar] [CrossRef] [PubMed]
- Duong, V.; Mey, C.; Eloit, M.; Zhu, H.; Danet, L.; Huang, Z.; Zou, G.; Tarantola, A.; Cheval, J.; Perot, P.; et al. Molecular epidemiology of human enterovirus 71 at the origin of an epidemic of fatal hand, foot and mouth disease cases in Cambodia. Emerg. Microbes. Infect. 2016, 5, e104. [Google Scholar] [CrossRef] [Green Version]
- Upala, P.; Apidechkul, T.; Suttana, W.; Kullawong, N.; Tamornpark, R.; Inta, C. Molecular epidemiology and clinical features of hand, foot and mouth disease in northern Thailand in 2016: A prospective cohort study. BMC Infect. Dis. 2018, 18, 630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, P.-Y.; Lu, P.-L.; Tsai, Y.-L.; Hsi, E.; Yao, C.-Y.; Chen, Y.-H.; Hsu, L.-C.; Wang, S.-Y.; Wu, H.-S.; Lin, Y.-Y.; et al. Spatiotemporal phylogenetic analysis and molecular characterization of coxsackievirus A4. Infect. Genet. Evol. 2011, 11, 1426–1435. [Google Scholar] [CrossRef]
- Li, J.-S.; Dong, X.-G.; Qin, M.; Xie, Z.-P.; Gao, H.-C.; Yang, J.-Y.; Yang, X.-X.; Li, D.-D.; Li, J.; Duan, Z.-J. Outbreak of febrile illness caused by coxsackievirus A4 in a nursery school in Beijing, China. Virol. J. 2015, 12, 92. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Li, C.; Liu, L.; Liu, X.; Shang, S.; Mao, H.; Zhang, Y. Molecular epidemiology of enterovirus from children with herpangina or hand, foot, and mouth disease in Hangzhou, 2016. Arch. Virol. 2019, 164, 2565–2571. [Google Scholar] [CrossRef]
- Wang, H.-Y.; Li, Y.; Xu, A.-Q.; Zhang, Y.; Tao, Z.-X.; Liu, G.-F.; Liu, Y.; Song, L.-Z.; Zhang, L.; Yan, B.-Y.; et al. Identification and phylogenic analysis of Coxsackie-virus B5 during an outbreak of aseptic meningitis in Shandong. Zhonghua Liu Xing Bing Xue Za Zhi 2010, 31, 64–68. [Google Scholar]
- Krumbholz, A.; Egerer, R.; Braun, H.; Schmidtke, M.; Rimek, D.; Kroh, C.; Hennig, B.; Groth, M.; Sauerbrei, A.; Zell, R. Analysis of an echovirus 18 outbreak in Thuringia, Germany: Insights into the molecular epidemiology and evolution of several enterovirus species B members. Med. Microbiol. Immunol. 2016, 205, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Miao, Z.; Lyu, H.; Zhou, J.; Gong, L.; Mao, H.; Sun, Y.; Zhang, Y. Etiology and molecular-epidemiological characteristics of viral meningoencephalitis of Zhejiang province in 2013. Zhonghua Liu Xing Bing Xue Za Zhi 2015, 36, 280–284. [Google Scholar]
- Tsuno, K.; Miyatake, C.; Nishijima, H.; Hotta, C.; Ogawa, T.; Asano, T. Coxsackievirus B5 Aseptic Meningitis in Infants in Chiba Prefecture, Japan, in 2016. J. Nippon Med. Sch. 2018, 85, 187–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, A.; Yu, D.; Zhu, Z.; Meng, L.; Li, H.; Liu, J.; Liu, G.; Mao, N.; Xu, W. An outbreak of aseptic meningitis caused by coxsackievirus A9 in Gansu, the People’s Republic of China. Virol. J. 2010, 7, 72. [Google Scholar] [CrossRef]
- Pabbaraju, K.; Wong, S.; Chan, E.N.Y.; Tellier, R. Genetic characterization of a Coxsackie A9 virus associated with aseptic meningitis in Alberta, Canada in 2010. Virol. J. 2013, 10, 93. [Google Scholar] [CrossRef] [Green Version]
- Smuts, H.; Cronje, S.; Thomas, J.; Brink, D.; Korsman, S.; Hardie, D. Molecular characterization of an outbreak of enterovirus-associated meningitis in Mossel Bay, South Africa, December 2015–January 2016. BMC Infect. Dis. 2018, 18, 709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Q.; Yuan, S.; Zhang, C.; Wang, Y.; Wang, Y.; He, G.; Zhang, S.; Altmeyer, R.; Zou, G. Discovery of itraconazole with broad-spectrum in vitro antienterovirus activity that targets nonstructural protein 3A. Antimicrob. Agents Chemother. 2015, 59, 2654–2665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.; Kang, H.; Kim, D.-E.; Song, J.-H.; Choi, M.; Kang, M.; Lee, K.; Kim, H.S.; Shin, J.S.; Jeong, H.; et al. Antiviral activity of micafungin against enterovirus 71. Virol. J. 2016, 13, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, F.; Zhao, X.; Hu, S.; Li, J.; Yin, L.; Mei, S.; Liu, T.; Wang, Y.; Ren, L.; Cen, S.; et al. Amphotericin B Inhibits Enterovirus 71 Replication by Impeding Viral Entry. Sci. Rep. 2016, 6, 33150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, S.; Meng, X.; Huang, Q.; Lei, N.; Zeng, L.; Jiang, X.; Guo, X. Spiramycin and azithromycin, safe for administration to children, exert antiviral activity against enterovirus A71 in vitro and in vivo. Int. J. Antimicrob. Agents 2019, 53, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-M. Milrinone in Enterovirus 71 Brain Stem Encephalitis. Front. Pharmacol. 2016, 7, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, Y.-T.; Wang, S.-M.; Chen, S.-H. Anti-inflammatory and antiviral effects of minocycline in enterovirus 71 infections. Biomed. Pharmacother. 2019, 118, 109271. [Google Scholar] [CrossRef] [PubMed]
- Werner, B.; Dittmann, S.; Funke, C.; Überla, K.; Piper, C.; Niehaus, K.; Horstkotte, D.; Farr, M. Effect of lovastatin on coxsackievirus B3 infection in human endothelial cells. Inflamm. Res. 2014, 63, 267–276. [Google Scholar] [CrossRef]
- Funke, C.; Farr, M.; Werner, B.; Dittmann, S.; Überla, K.; Piper, C.; Niehaus, K.; Horstkotte, D. Antiviral effect of Bosentan and Valsartan during coxsackievirus B3 infection of human endothelial cells. J. Gen. Virol. 2010, 91 Pt 8, 1959–1970. [Google Scholar] [CrossRef]
- Gazina, E.V.; Smidansky, E.D.; Holien, J.K.; Harrison, D.N.; Cromer, B.A.; Arnold, J.J.; Parker, M.W.; Cameron, C.E.; Petrou, S. Amiloride is a competitive inhibitor of coxsackievirus B3 RNA polymerase. J. Virol. 2011, 85, 10364–10374. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Chen, Y.; Jiang, J.; Zhou, A.; Pan, L.; Chen, Q.; Qian, Y.; Chu, M.; Chen, C. Carvedilol has stronger anti-inflammation and anti-virus effects than metoprolol in murine model with coxsackievirus B3-induced viral myocarditis. Gene 2014, 547, 195–201. [Google Scholar] [CrossRef]
- Gong, X.-Y.; Li, B.-F. Clinical effect of carvedilol in treatment of children with severe hand-foot-mouth disease caused by enterovirus 71 infection. Zhongguo Dang Dai Er Ke Za Zhi 2019, 21, 796–800. [Google Scholar]
- Ulferts, R.; de Boer, S.M.; van der Linden, L.; Bauer, L.; Lyoo, H.R.; Maté, M.J.; Lichière, J.; Canard, B.; Lelieveld, D.; Omta, W.; et al. Screening of a Library of FDA-Approved Drugs Identifies Several Enterovirus Replication Inhibitors That Target Viral Protein 2C. Antimicrob. Agents Chemother. 2016, 60, 2627–2638. [Google Scholar] [CrossRef] [Green Version]
- Li-Sha, G.; Jing-Lin, Z.; Li, L.; Guang-Yi, C.; Xiao-Wei, L.; Yue-Chun, L. Nicotine inhibits the production of proinflammatory cytokines of mice infected with coxsackievirus B3. Life Sci. 2016, 148, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-C.; Luo, Q.; Ge, L.-S.; Chen, Y.-H.; Zhou, N.-D.; Zhang, T.; Guan, X.-Q.; Lin, J.-F. Ivabradine inhibits the production of proinflammatory cytokines and inducible nitric oxide synthase in acute coxsackievirus B3-induced myocarditis. Biochem. Biophys. Res. Commun. 2013, 431, 450–455. [Google Scholar] [CrossRef]
- Zhang, A.; Zhang, H.; Wu, S. Immunomodulation by atorvastatin upregulates expression of gap junction proteins in coxsackievirus B3 (CVB3)-induced myocarditis. Inflamm. Res. 2010, 59, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-Y.; Li, J.-N.; Xia, H.H.-X.; Zhang, S.-L.; Zhong, J.; Wu, Y.-Y.; Miao, S.-K.; Zhou, L.-M. Protective effects of losartan in mice with chronic viral myocarditis induced by coxsackievirus B3. Life Sci. 2013, 92, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-B.; Rao, B.-F.; Chang, J.; Liao, X.-G.; Cao, Y.-D. Effects of captopril on myocardial energy metabolism in mice with viral myocarditis. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2003, 15, 485–488. [Google Scholar] [PubMed]
- Bauer, L.; Manganaro, R.; Zonsics, B.; Strating, J.R.P.M.; El Kazzi, P.; Lorenzo Lopez, M.; Ulferts, R.; van Hoey, C.; Maté, M.J.; Langer, T.; et al. Fluoxetine Inhibits Enterovirus Replication by Targeting the Viral 2C Protein in a Stereospecific Manner. ACS Infect. Dis. 2019, 5, 1609–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, H.; Guo, X. Valproic acid ameliorates coxsackievirus-B3-induced viral myocarditis by modulating Th17/Treg imbalance. Virol. J. 2016, 13, 168. [Google Scholar] [CrossRef]
- Kang, H.; Kim, C.; Kim, D.-e.; Song, J.-H.; Choi, M.; Choi, K.; Kang, M.; Lee, K.; Kim, H.S.; Shin, J.S.; et al. Synergistic antiviral activity of gemcitabine and ribavirin against enteroviruses. Antiviral. Res. 2015, 124, 1–10. [Google Scholar] [CrossRef]
- Hou, H.-Y.; Lu, W.-W.; Wu, K.-Y.; Lin, C.-W.; Kung, S.-H. Idarubicin is a broad-spectrum enterovirus replication inhibitor that selectively targets the virus internal ribosomal entry site. J. Gen. Virol. 2016, 97, 1122–1133. [Google Scholar] [CrossRef] [Green Version]
- Leipner, C.; Grün, K.; Müller, A.; Buchdunger, E.; Borsi, L.; Kosmehl, H.; Berndt, A.; Janik, T.; Uecker, A.; Kiehntopf, M.; et al. Imatinib mesylate attenuates fibrosis in coxsackievirus b3-induced chronic myocarditis. Cardiovasc. Res. 2008, 79, 118–126. [Google Scholar] [CrossRef]
- Feng, Q.; Zhou, H.; Zhang, X.; Liu, X.; Wang, J.; Zhang, C.; Ma, X.; Quan, C.; Zheng, Z. Acarbose, as a potential drug, effectively blocked the dynamic metastasis of EV71 from the intestine to the whole body. Infect. Genet. Evol. 2020, 81, 104210. [Google Scholar] [CrossRef] [PubMed]
- Ammer, E.; Nietzsche, S.; Rien, C.; Kühnl, A.; Mader, T.; Heller, R.; Sauerbrei, A.; Henke, A. The anti-obesity drug orlistat reveals anti-viral activity. Med. Microbiol. Immunol. 2015, 204, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Shang, L.; Xu, M.; Yin, Z. Antiviral drug discovery for the treatment of enterovirus 71 infections. Antiviral. Res. 2013, 97, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Shih, S.-R.; Weng, K.-F.; Stollar, V.; Li, M.-L. Viral protein synthesis is required for Enterovirus 71 to induce apoptosis in human glioblastoma cells. J. Neurovirol. 2008, 14, 53–61. [Google Scholar] [CrossRef]
- Wong, T.-W.; Huang, H.-J.; Wang, Y.-F.; Lee, Y.-P.; Huang, C.-C.; Yu, C.-K. Methylene blue-mediated photodynamic inactivation as a novel disinfectant of enterovirus 71. J. Antimicrob. Chemother. 2010, 65, 2176–2182. [Google Scholar] [CrossRef] [Green Version]
- Molin, Y.; Frisk, P.; Hjelm, E.; Blomberg, J.; Friman, G.; Ilbäck, N.-G. Arsenic trioxide influences viral replication in target organs of coxsackievirus B3-infected mice. Microbes. Infect. 2010, 12, 1027–1034. [Google Scholar] [CrossRef]
- Marton, J.; Albert, D.; Wiltshire, S.A.; Park, R.; Bergen, A.; Qureshi, S.; Malo, D.; Burelle, Y.; Vidal, S.M. Cyclosporine A Treatment Inhibits Abcc6-Dependent Cardiac Necrosis and Calcification following Coxsackievirus B3 Infection in Mice. PLoS ONE 2015, 10, e0138222. [Google Scholar] [CrossRef]
- Han, J.-Y.; Jeong, H.I.; Park, C.-W.; Yoon, J.; Ko, J.; Nam, S.-J.; Lim, B.-K. Cholic Acid Attenuates ER Stress-Induced Cell Death in Coxsackievirus-B3 Infection. J. Microbiol. Biotechnol. 2018, 28, 109–114. [Google Scholar] [CrossRef]
- Ren, P.; Zou, G.; Bailly, B.; Xu, S.; Zeng, M.; Chen, X.; Shen, L.; Zhang, Y.; Guillon, P.; Arenzana-Seisdedos, F.; et al. The approved pediatric drug suramin identified as a clinical candidate for the treatment of EV71 infection-suramin inhibits EV71 infection in vitro and in vivo. Emerg. Microbes. Infect. 2014, 3, e62. [Google Scholar] [CrossRef]
- Wang, Y.; Qing, J.; Sun, Y.; Rao, Z. Suramin inhibits EV71 infection. Antiviral. Res. 2014, 103, 1–6. [Google Scholar] [CrossRef]
- Soumajit, S.; Tamil Selvan, R.P.; Bhanuprakash, V. In vitro antiviral efficacy of pleconaril and ribavirin on foot-and-mouth disease virus replication. Virusdisease 2019, 30, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Niklasson, B.; Klitz, W.; Juntti-Berggren, L.; Berggren, P.O.; Lindquist, L. Effectiveness of Antivirals in a Type 1 Diabetes Model and the Move Toward Human Trials. Viral. Immunol. 2020, 33, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Klitz, W.; Niklasson, B. Extending the Enterovirus Lead: Could a Related Picornavirus be Responsible for Diabetes in Humans? Microorganisms 2020, 8, 1382. [Google Scholar] [CrossRef] [PubMed]
- Niklasson, B.; Lindquist, L.; Klitz, W.; Fredrikson, S.; Morgell, R.; Mohammadi, R.; Netherlands Brain, B.; Karapetyan, Y.; Englund, E. Picornavirus May Be Linked to Parkinson’s Disease through Viral Antigen in Dopamine-Containing Neurons of Substantia Nigra. Microorganisms 2022, 10, 599. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Virus | Asia | Others | ||||||
|---|---|---|---|---|---|---|---|---|
| EV71 | Area | Year | Number Infected | Area | Year | Number Infected | ||
| Malaysia | 1997 | 41 | [9] | California | 1974 | UNKNOWN | [10] | |
| China | 2008–2012 | >7 million | [11] | Bulgarian | 1975 | 700 | [12] | |
| Singapore | 2008 | 29686 | [13] | Hungary | 2000 | UNKNOWN | [14] | |
| Taiwan | 1998 | 1.5 million | [15] | Austria | 2002 | 12 | [16] | |
| Japan | 2010 | 2900 | [17] | Holland | 2007 | 58 | [18] | |
| Vietnam | 2005 | 173 | [19] | Denmark | 2007 | 29 | [20] | |
| Russia | 2013 | UNKNOWN | [21] | Marseille, France | 2009 | 3 | [22] | |
| CVB3 | Hong Kong | 2008 | <100 | [23] | Poland | 1999–2014 | <55 | [24] |
| India | 2009–2010 | 15 | [25] | |||||
| Hebei, China | 2010–2012 | 26 | [26] | |||||
| Shandong, China | 2016 | 42 | [27] | |||||
| CVA16 | Shanghai, China | 2014–2016 | 144 | [28] | Toronto | 1957 | <100 | [29] |
| Birmingham | 1959 | 24 | [30] | |||||
| USA | 1959 | UNKNOWN | [31] | |||||
| Germany | 2006 | <500 | [32] | |||||
| CVA6 | India | 2009–2010 | <89 | [33] | Finland | 2008 | <50 | [34] |
| GZ, China | 2010–2012 | 720 | [35] | France | 2010 | 25 | [36] | |
| BJ, China | 2015 | <56 | [37] | Spain | 2010–2012 | <30 | [38] | |
| Thailand | 2012 | <600 | [39] | |||||
| CVA10 | Japan | 1981–1982 | 18 | [40] | USA | 1950/2016 | UNKNOWN | [40] |
| Tajikistan | 2004 | UNKNOWN | [40] | Germany | 2003 | UNKNOWN | [40] | |
| China | 2004–2008 | >1000 | [40] | France | 2010 | <100 | [40] | |
| Russia | 2004–2013 | UNKNOWN | [40] | Chad | 2006 | UNKNOWN | [40] | |
| Singapore | 2008 | <100 | [40] | Austria | 2007 | UNKNOWN | [40] | |
| Spain | 2008 | UNKNOWN | [40] | |||||
| Central African Republic | 2008 | UNKNOWN | [40] | |||||
| CVB1 | India | 2007 | UNKNOWN | [41] | USA | 2006–2008 | 235 | [42] |
| Korea | 2008 | >104 | [43] | Spain | 2008 | <100 | [44] | |
| Taiwan | 2008–2010 | >22 | [41] | |||||
| CVB2 | Jiangsu, China | 2009 | <111 | [45] | São Paulo State, Brazil | 2004 | <10 | [46] |
| Cambodia | 2012 | <50 | [47] | |||||
| Thailand | 2016 | <20 | [48] | |||||
| CVA4 | Taiwan | 2004–2006 | UNKNOWN | [49] | USA | 1950 | UNKNOWN | [49] |
| BJ, China | 2011 | 21 | [50] | |||||
| Hangzhou, China | 2016 | 3 | [51] | |||||
| CVB5 | Shandong, China | 2005 | >54 | [52] | Thuringia, Germany | 2010 | <7 | [53] |
| Zhejiang, China | 2013 | <92 | [54] | Chiba Prefecture, Japan | 2016 | 3 | [55] | |
| CVA9 | Gansu, China | 2005 | <85 | [56] | Alberta, Canada | 2010 | 174 | [57] |
| Mossel Bay, South Africa | Dec 2015–Jan 2016 | >26 | [58] | |||||
| Classification. | Drug | Company (Action Date) | Previous Use(s) | Repurposed Use(s) | Clinical Phases |
|---|---|---|---|---|---|
| Anti-fungal | Itraconazole (1) | SANDOZ (05/28/2004) | deep fungi infection | a broad-spectrum enterovirus inhibitor | Preclinical |
| Micafungin (2) | FRESENIUS KABI USA (05/17/2019) | candida infection | may target any step in the early viral infection | Preclinical | |
| Amphotericin B (3) | XGEN PHARMS (04/29/1992) | cryptococcus infection | inhibit the production of EV71 | Preclinical | |
| Anti-bacterial | Azithromycin (4) | OAK PHARMS INC (04/27/2007) | respiratory tract infection | reduce the RNA and protein levels of EV-71 | Preclinical |
| Spiramycin (5) | Odan Laboratories Ltd. (12/31/1957) | Respiratory infection | inhibit virus RNA replication | Preclinical | |
| Minocycline (6) | FOAMIX (10/18/2019) | broad-spectrum antibiotic | suppress cytokine productions and viral protein expressions | Preclinical | |
| Cardiovascular System | Lovastatin (7) | COVIS PHARMA BV (06/26/2002) | hypercholesterolemia | reduce CAR mRNA and protein | Preclinical |
| Bosentan (8) | PAR PHARM INC (04/26/2019) | pulmonary hypertension (PAH) | reduce CAR mRNA | Preclinical | |
| Valsartan (9) | LUPIN (03/30/2015) | anti-hypertension | reduce CAR mRNA | Preclinical | |
| Amiloride (10) | PAR PHARM (01/22/1986) | liver cirrhosis, edema, primary aldosteronism | affect RNA elongation | Preclinical | |
| Carvedilol (11) | TEVA (09/05/2007) | heart failure and essential hypertension | alleviate the dysfunction caused by HFMD | Preclinical | |
| Formoterol (12) | NOVARTIS (09/25/2001) | chronic asthma | a panentervirus inhibitor; inhibit CVB3-induced Myocarditis | Preclinical | |
| Nicotine (13) | DR REDDYS LABS SA (11/27/1991) | improve inflammation | improve myocarditis caused by CVB3 | Preclinical | |
| Ivabradine (14) | AMGEN INC (04/15/2015) | heart failure | reduce myocardial damage | Preclinical | |
| Olmesartan (15) | DAIICHI SANKYO (04/25/2002) | antihypertensive | inhibit the synthesis of NO to treat viral myocarditis | Preclinical | |
| Atorvastatin (16) | SANDOZ INC (05/29/2012) | a lipid-lowering drug | reduce myocardial necrosis and treate viral myocarditis | Preclinical | |
| Losartan (17) | MERCK SHARP DOHME (04/14/1995) | antihypertensive | used as immunomodulators to treat viral myocarditis (VMC) | Preclinical | |
| Captopril (18) | MYLAN (02/13/1996) | hypertension and heart failure | reduce myocardial calcification and fibrosis | Preclinical | |
| Milrinone (19) | WEST-WARD PHARMS INT (05/28/2002) | chronic congestive heart failure | Enterovirus 71 Brain Stem Encephalitis | Preclinical | |
| Nervous System | Fluoxetine (20) | APNAR PHARMA LP (08/02/2001) | antidepressant | inhibit CVB3 proliferation | Preclinical |
| Valproic Acid (21) | WOCKHARDT BIO AG (07/01/1986) | epilepsy | improve myocarditis | Preclinical | |
| Anti-cancer | Gemcitabine (22) | HOSPIRA (07/25/2011) | a pyrimidine anti-tumor drug | binds to viral RNA | Preclinical |
| Idarubicin (23) | FRESENIUS KABI USA (08/04/2009) | non-specific anticancer drug | prevent the synthesis of EV71 virus protein and RNA | Preclinical | |
| Imatinib Mesylate (24) | NOVARTIS (04/18/2003) | chronic myeloid leukemia | reduces cardiac fibrosis | Preclinical | |
| Antidiabetic and Anti-obesity | Acarbose (25) | WATSON LABS (05/07/2008) | (non)insulin-dependent diabetes | reduce EV71 intestinal infection | Preclinical |
| Orlistat (26) | CHEPLAPHARM (04/23/1999) | an obesity treatment drug | decrease the replication of different viral pathogens | Preclinical | |
| Others | Chloroquine (27) | SANDOZ (11/30/1995) | malaria | block the uncoating of EV71 and reduce viral RNA synthesis | Preclinical |
| Methylene blue (28) | PROVEPHARM SAS (04/08/2016) | chemical indicator, dye, and drug | destroy EV71’s viral proteins and genome | Preclinical | |
| Arsenic Trioxide (29) | ZYDUS PHARMS (11/13/2018) | one of the oldest poisons | reduce the viral load of CVB3 RNA in the pancreas | Preclinical | |
| Cyclosporin (30) | SUN PHARMA GLOBAL (08/14/2018) | anti-rejection reaction of liver, kidney, and heart transplantation | reduce the degree of myocardial calcification | Preclinical | |
| Cholic Acid (31) | RTRX (03/17/2015) | peroxisomal disorders | reduce the production of the viral capsid protein VP1 | Preclinical | |
| Suramin (32) | BAYER | treat sleeping sickness caused by trypanosomes | Inhibit the proliferation of EV71 and CVA16 | Phase 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, R.; He, J.; Liu, G.; Zhong, J.; Xu, J.; Zheng, K.; Ren, Z.; He, Z.; Zhu, Q. Drug Repositioning for Hand, Foot, and Mouth Disease. Viruses 2023, 15, 75. https://doi.org/10.3390/v15010075
Yan R, He J, Liu G, Zhong J, Xu J, Zheng K, Ren Z, He Z, Zhu Q. Drug Repositioning for Hand, Foot, and Mouth Disease. Viruses. 2023; 15(1):75. https://doi.org/10.3390/v15010075
Chicago/Turabian StyleYan, Ran, Jiahao He, Ge Liu, Jianfeng Zhong, Jiapeng Xu, Kai Zheng, Zhe Ren, Zhendan He, and Qinchang Zhu. 2023. "Drug Repositioning for Hand, Foot, and Mouth Disease" Viruses 15, no. 1: 75. https://doi.org/10.3390/v15010075