
Reduced Neutralization Efficacy against Omicron Variant after Third Boost of BNT162b2 Vaccine among Liver Transplant Recipients
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Serology Assay
2.1.1. Antibody Detection Testing
2.1.2. T-Cell Response Testing
2.1.3. Viral Isolation of the Wild-Type, Delta and Omicron Variants and SARS-CoV-2 Micro-Neutralization Assay
2.1.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison of Immune Response between Liver Transplant Recipients and Immunocompetent Controls
3.3. Predictors of a Humoral Immune Response to THIRD BNT162b2 Vaccine Dose among LT Recipients
3.4. T-Cell Immunity to the Third Dose of the BNT162b2 Vaccine
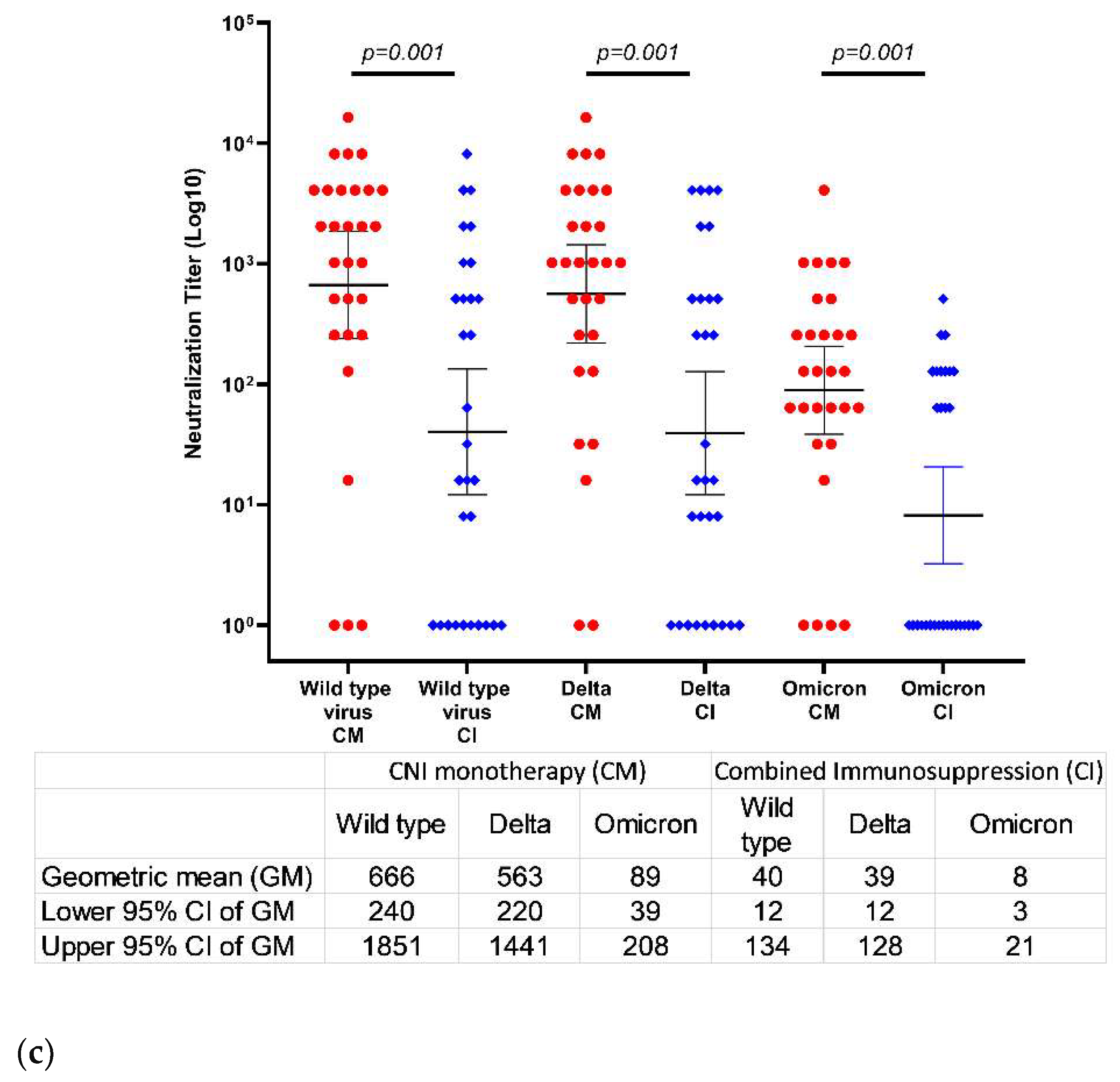
3.5. Neutralization of Wild-Type, Delta, and Omicron Variants 22 Days after the Third Vaccine Dose
3.6. Breakthrough Infection after the Third Vaccine Dose
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 vaccine in a nationwide mass vaccination setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID symptom study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning immune humoral response to BNT162b2 COVID-19 vaccine over 6 months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning immunity after the BNT162b2 vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef]
- Bajema, K.L.; Dahl, R.M.; Evener, S.L.; Prill, M.M.; Rodriguez-Barradas, M.C.; Marconi, V.C.; Beenhouwer, D.O.; Holodniy, M.; Lucero-Obusan, C.; Brown, S.T.; et al. Comparative effectiveness and antibody responses to Moderna and Pfizer-BioNTech COVID-19 vaccines among hospitalized veterans—Five Veterans Affairs Medical Centers, United States, February 1–September 30, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1700–1705. [Google Scholar] [CrossRef]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 vaccination neutralization of SARS-CoV-2 omicron infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef]
- Shen, C.; Risk, M.; Schiopu, E.; Hayek, S.S.; Xie, T.; Holevinski, L.; Akin, C.; Freed, G.; Zhao, L. Efficacy of COVID-19 vaccines in patients taking immunosuppressants. Ann. Rheum. Dis. 2022, 81, 875–880. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transplant. 2021, 21, 2719–2726. [Google Scholar] [CrossRef] [PubMed]
- Peled, Y.; Ram, E.; Lavee, J.; Sternik, L.; Segev, A.; Wieder-Finesod, A.; Mandelboim, M.; Indenbaum, V.; Levy, I.; Raanani, E.; et al. BNT162b2 vaccination in heart transplant recipients: Clinical experience and antibody response. J. Heart Lung Transplant. 2021, 40, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Davidov, Y.; Tsaraf, K.; Cohen-Ezra, O.; Likhter, M.; Ben Yakov, G.; Levy, I.; Levin, E.G.; Lustig, Y.; Mor, O.; Rahav, G.; et al. Immunogenicity and adverse effect of two dose BNT162b2 mRNA vaccine among liver transplant recipients. Liver Transplant. 2022, 28, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Lustig, Y.; Cohen, C.; Rahav, G.; Asraf, K.; Amit, S.; Jaber, H.; Nemet, I.; et al. Early immunogenicity and safety of the third dose of BNT162b2 messenger RNA coronavirus disease 2019 vaccine among adults older than 60 years: Real-world experience. J. Infect. Dis. 2022, 225, 785–792. [Google Scholar] [CrossRef]
- Davidov, Y.; Indenbaum, V.; Tsaraf, K.; Cohen-Ezra, O.; Likhter, M.; Yakov, G.B.; Halperin, R.; Levy, I.; Mor, O.; Agmon-Levin, N.; et al. A third dose of the BNT162b2 mRNA vaccine significantly improves immune responses among liver transplant recipients. J. Hepatol. 2022, 77, 702–709. [Google Scholar] [CrossRef]
- Cele, S.; Jackson, L.; Khoury, D.S.; Khan, K.; Moyo-Gwete, T.; Tegally, H.; San, J.E.; Cromer, D.; Scheepers, C.; Amoako, D.G.; et al. Omicron extensively but incompletely escapes Pfizer BNT162b2 neutralization. Nature 2022, 602, 654–656. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484.e15. [Google Scholar] [CrossRef]
- SARS-CoV-2 Variants in Analyzed Sequences, Israel. Available online: https://covariants.org/per-country (accessed on 1 January 2023).
- Glatman-Freedman, A.; Bromberg, M.; Hershkovitz, Y.; Sefty, H.; Kaufman, Z.; Dichtiar, R.; Keinan-Boker, L. Effectiveness of BNT162b2 vaccine booster against SARS-CoV-2 infection and breakthrough complications, Israel. Emerg. Infect. Dis. 2022, 28, 948–956. [Google Scholar] [CrossRef]
- Wang, C.; Liu, B.; Zhang, S.; Huang, N.; Zhao, T.; Lu, Q.B.; Cui, F. Differences in incidence and fatality of COVID-19 by SARS-CoV-2 Omicron variant versus Delta variant in relation to vaccine coverage: A world-wide review. J. Med. Virol. 2023, 95, e28118. [Google Scholar] [CrossRef]
- Rössler, A.; Riepler, L.; Bante, D.; von Laer, D.; Kimpel, J. SARS-CoV-2 Omicron Variant neutralization in serum from vaccinated and convalescent persons. N. Engl. J. Med. 2022, 386, 698–700. [Google Scholar] [CrossRef]
- Planas, D.; Saunders, N.; Maes, P.; Guivel-Benhassine, F.; Planchais, C.; Buchrieser, J.; Bolland, W.H.; Porrot, F.; Staropoli, I.; Lemoine, F.; et al. Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature 2021, 602, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Al Jurdi, A.; Gassen, R.B.; Borges, T.J.; Lape, I.T.; Morena, L.; Efe, O.; Solhjou, Z.; El Fekih, R.; Deban, C.; Bohan, B.; et al. Suboptimal antibody response against SARS-CoV-2 Omicron variant after third dose of mRNA vaccine in kidney transplant recipients. Kidney Int. 2022, 101, 1282–1286. [Google Scholar] [CrossRef]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: A prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Nemet, I.; Kliker, L.; Zuckerman, N.; Yishai, R.; Alroy-Preis, S.; Mendelson, E. Neutralizing response against variants after SARS-CoV-2 infection and one dose of BNT162b2. N. Engl. J. Med. 2021, 384, 2453–2454. [Google Scholar] [CrossRef] [PubMed]
- Peled, Y.; Ram, E.; Lavee, J.; Segev, A.; Matezki, S.; Wieder-Finesod, A.; Halperin, R.; Mandelboim, M.; Indenbaum, V.; Levy, I.; et al. Third dose of the BNT162b2 vaccine in heart transplant recipients: Immunogenicity and clinical experience. J. Heart Lung Transplant. 2022, 41, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Kantauskaite, M.; Müller, L.; Kolb, T.; Fischer, S.; Hillebrandt, J.; Ivens, K.; Andree, M.; Luedde, T.; Orth, H.M.; Adams, O.; et al. Intensity of mycophenolate mofetil treatment is associated with an impaired immune response to SARS-CoV-2 vaccination in kidney transplant recipients. Am. J. Transplant. 2022, 22, 634–639. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a fourth dose of COVID-19 mRNA vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. Bivalent Omicron-containing booster vaccine against COVID-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef]
- Britton, A.; Embi, P.J.; Levy, M.E.; Gaglani, M.; DeSilva, M.B.; Dixon, B.E.; Dascomb, K.; Patel, P.; Schrader, K.E.; Klein, N.O.; et al. Effectiveness of COVID-19 mRNA vaccines against COVID-19-associated hospitalizations among immunocompromised adults during SARS-CoV-2 Omicron predominance-VISION network, 10 States, December 2021–August 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Weber, Z.A.; Natarajan, K.; Klein, N.P.; Kharbanda, A.B.; Stenehjem, E.; Embi, P.J.; Reese, S.E.; Naleway, A.L.; Grannis, S.J.; et al. Early estimates of bivalent mRNA vaccine effectiveness in preventing COVID-19-associated emergency department or urgent care encounters and hospitalizations among immunocompetent adults-VISION network, nine states, September–November 2022. MMWR Morb. Mortal. Wkly Rep. 2022, 71, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Peretz, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Yaron, S.; Hammerman, A.; Bilenko, N.; Netzer, D. Effectiveness of the bivalent mRNA vaccine in preventing severe COVID-19 outcomes: An observational cohort study. Lancet 2023. preprint. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | First Test | Second Test | ||||
|---|---|---|---|---|---|---|
| LT N = 59 | HCW N = 20 | p Value | LT N = 59 | HCW N = 67 | p Value | |
| Age (years) | 66 (54–70) | 63 (51–67) | 0.2 | 66 (54–70) | 63 (49–66) | 0.06 |
| Male, n (%) | 35 (59.3) | 8 (40) | 0.1 | 35 (59.3) | 37 (55.2) | 0.6 |
| Time from third dose of the vaccine to serology testing, (days) | 22 (21–28) | 33 (28–35) | 0.004 | 133 (131–138) | 133 (129–138) | 0.9 |
| Positive IgG-RBD, n (%) § | 48 (81.4) | 20 (100) | 0.03 | 45 (76.3) | 67 (100) | <0.0001 |
| SARS-CoV-2 IgG titers, GMT (CI 95%), BAU/mL | 483 (225–1038) | 3297 (2373–4681) | 0.01 | 205 (97–433) | 844 (663–1074) | 0.03 |
| SARS-CoV-2 neutralizing antibodies, GMT (CI 95%) | 653 (238–1795) | 6420 (4173–9879) | 0.004 | 459 (201–1049) | 745 (385–1440) | 0.8 |
| Characteristics | Total LT Cohort N = 59 | Non-Responders § N = 11 (18.6%) | Responders § N = 48 (81.4%) | p Value |
|---|---|---|---|---|
| Age, years | 66 (54–70) | 66 (61–75) | 64 (53–70) | 0.2 |
| Male | 35 (59.3) | 7 (63.6) | 28 (58.3) | 0.7 |
| Indication for LT | 0.3 | |||
| Hepatitis C | 13 (22) | 4 (36.4) | 9 (18.8) | |
| NASH | 15 (25.4) | 4 (36.4) | 11 (22.9) | |
| Hepatitis B | 4 (6.8) | 0 | 4 (8.3) | |
| PSC | 4 (6.8) | 0 | 4 (8.3) | |
| PBC | 4 (6.8) | 1 (9.1) | 3 (6.3) | |
| Other ¶ | 19 (32.2) | 2 (18.2) | 17 (35.4) | |
| Age at transplantation, years | 53 (42–63) | 60 (54–65) | 51 (41–62) | 0.02 |
| Time since liver transplantation, years | 7 (4–16) | 6 (1–10) | 9 (4–19) | 0.07 |
| Comorbidities | ||||
| Diabetes mellitus | 25 (43.1) | 7 (63.6) | 18 (38.3) | 0.1 |
| Hypertension | 31 (53.4) | 8 (72.7) | 23 (48.9) | 0.1 |
| Dyslipidemia | 31 (53.4) | 8 (72.7) | 23 (48.9) | 0.1 |
| Chronic kidney disease | 35 (59.3) | 9 (81.8) | 15 (31.3) | 0.003 |
| BMI, kg/m2 | 26 (22–28) | 26 (23–27) | 26 (22–28) | 0.8 |
| WBC, K/microL | 5.6 (4.1–6.3) | 4.7 (3.9–5.8) | 5.8 (4.7–7.1) | 0.03 |
| Hemoglobin, g/dL | 13.1 (11.7–14.5) | 10.4 (9–11.7) | 13.5 (12.8–14.6) | 0.003 |
| Platelets, K/microL | 164 (125–197) | 168 (130–241) | 163 (124–188) | 0.4 |
| Creatinine, mg/dL | 1.0 (0.8–1.3) | 1.4 (1.2–2) | 1 (0.8–1.2) | 0.002 |
| ALT, IU/L | 20 (15–26) | 12 (7–18) | 21 (16–31) | 0.003 |
| ALP, IU/L | 95 (74–128) | 85 (72–106) | 99 (77–130) | 0.3 |
| Bilirubin, mg/dL | 0.6 (0.5–0.9) | 0.5 (0.4–0.7) | 0.6 (0.6–0.9) | 0.07 |
| Tacrolimus dose, mg/ trough level, μg/L | 2.5 (1.5–4.0)/5.2 (4.1–6.3) | 2 (1.5–4)/3 (2.9–5.4) | 3 (1.5–4)/5.3 (4.5–6.6) | 0.03/0.5 |
| Prednisone, n (%)/dose, mg | 8 (13.6)/10 (5–10) | 2 (18.2)/5 (5–10) | 6 (12.5)/10 (5–10) | 0.6/0.4 |
| MMF, n (%)/dose mg | 16 (27.1)/875 (500–1000) | 6 (54.5)/625 (500–1000) | 10 (20.8)/1000 (500–1000) | 0.03/0.4 |
| Everolimus, n (%)/dose mg/trough level, ng/ml | 9 (15.3)/2 (1.5–2.5)/2.9 (2.1–3.8) | 3 (27.3)/4.2 (1.2–5.6)/2.5 (1.5–2.5) | 6 (12.5)/2.8 (2.1–3.1)/1.8 (1.5–2.0) | 0.2/0.4/0.6 |
| Double ‡/triple ‡‡ immunosuppression | 28 (47.5)/2 (3.4) | 10 (90.9)/0 | 18 (37.5)/2 (4.2) | 0.003 |
| Characteristics | Maintained Immune Response * N = 45 (76.3%) | No Maintained Immune Response * N = 14 (23.7%) | Univariate | Multivariate § | ||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |||
| Age at transplantation, years | 51 (41–62) | 59 (55–65) | 0.004 | 0.9 (0.8–0.99) | 0.02 | |
| Time since liver transplantation, years | 9 (5–19) | 6 (1–10) | 0.04 | 1.1 (0.9–1.2) | 0.08 | |
| Chronic kidney disease | 15 (33.3) | 9 (64.3) | 3.6 (1.0–13) | 0.04 | 2.1 (0.5–9.3) | 0.3 |
| WBC, K/microL | 5.7 (4.7–7) | 4.8 (3.9–6.2) | 0.09 | 1.1 (0.8–1.6) | 0.6 | |
| Hemoglobin, g/dL | 13.6 (12.8–14.7) | 11.1 (9.9–12.4) | 0.003 | 1.5 (1.1–2.2) | 0.03 | |
| Hemoglobin > 12 g/dL | 39 (86.7) | 4 (28.6) | 16.2 (3.8–69) | <0.0001 | 13 (2.4–68) | 0.003 |
| Creatinine, mg/dL | 1.0 (0.8–1.2) | 1.3 (1.1–1.9) | 0.01 | 0.9 (0.5–1.5) | 0.7 | |
| ALT, IU/L | 21 (16–31) | 12.5 (8–18) | 0.0001 | 1.2 (1.0–1.3) | 0.02 | |
| ALT > 15.5 IU/mL | 36 (80) | 4 (28.6) | 10 (2.5–39) | <0.0001 | 8.6 (1.8–40) | 0.007 |
| CNI monotherapy | 27 (60) | 2 (14.3) | 0.1 (0.02–0.6) | 0.003 | 7.4 (1.4–40.2) | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davidov, Y.; Indenbaum, V.; Mandelboim, M.; Asraf, K.; Gonen, T.; Tsaraf, K.; Cohen-Ezra, O.; Likhter, M.; Nemet, I.; Kliker, L.; et al. Reduced Neutralization Efficacy against Omicron Variant after Third Boost of BNT162b2 Vaccine among Liver Transplant Recipients. Viruses 2023, 15, 253. https://doi.org/10.3390/v15010253
Davidov Y, Indenbaum V, Mandelboim M, Asraf K, Gonen T, Tsaraf K, Cohen-Ezra O, Likhter M, Nemet I, Kliker L, et al. Reduced Neutralization Efficacy against Omicron Variant after Third Boost of BNT162b2 Vaccine among Liver Transplant Recipients. Viruses. 2023; 15(1):253. https://doi.org/10.3390/v15010253
Chicago/Turabian StyleDavidov, Yana, Victoria Indenbaum, Michal Mandelboim, Keren Asraf, Tal Gonen, Keren Tsaraf, Oranit Cohen-Ezra, Mariya Likhter, Ital Nemet, Limor Kliker, and et al. 2023. "Reduced Neutralization Efficacy against Omicron Variant after Third Boost of BNT162b2 Vaccine among Liver Transplant Recipients" Viruses 15, no. 1: 253. https://doi.org/10.3390/v15010253