
Hepatitis E Virus Seroprevalence and Associated Risk Factors in Pregnant Women Attending Antenatal Consultations in Senegal

 , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
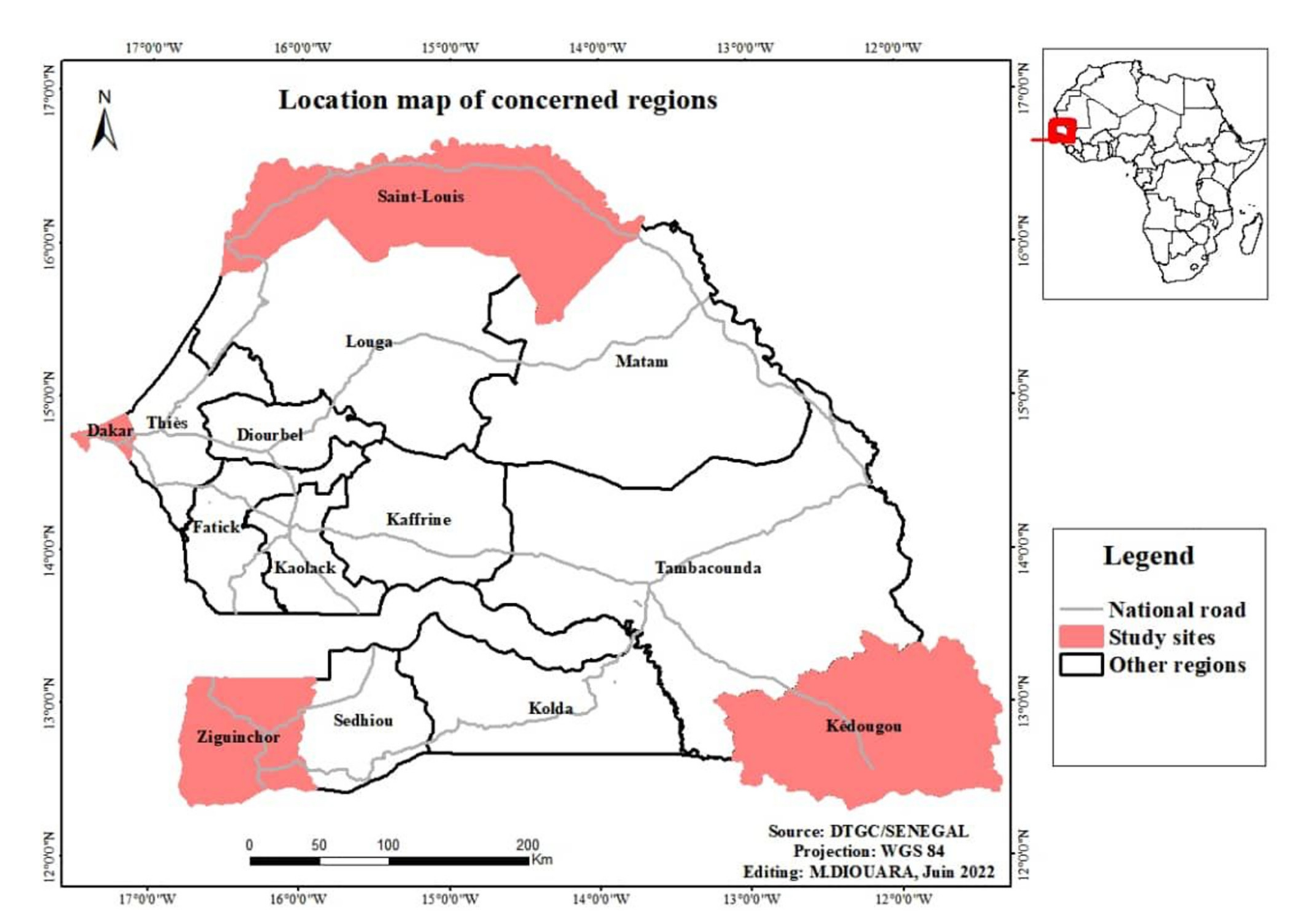
2.1. Study Sites, Sampling and Data Collection
2.2. Anti-HEV Antibody Detection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bradley, D.W. Hepatitis E virus: A brief review of the biology, molecular virology, and immunology of a novel virus. J. Hepatol. 1995, 22 (Suppl. 1), 140–145. [Google Scholar] [PubMed]
- Sridhar, S.; Teng, J.L.L.; Chiu, T.H.; Lau, S.K.P.; Woo, P.C.Y. Hepatitis E Virus Genotypes and Evolution: Emergence of Camel Hepatitis E Variants. Int. J. Mol. Sci. 2017, 18, 869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes, G.R.; Purdy, M.A.; Kim, J.P.; Luk, K.C.; Young, L.M.; Fry, K.E.; Bradley, D. Isolation of a cDNA from the virus responsible for enterically transmitted non-A, non-B hepatitis. Science 1990, 247, 1335–1339. [Google Scholar] [CrossRef]
- Lu, L.; Li, C.; Hagedorn, C.H. Phylogenetic analysis of global hepatitis E virus sequences: Genetic diversity, subtypes and zoonosis. Rev. Med. Virol. 2006, 16, 5–36. [Google Scholar] [CrossRef]
- Purdy, M.A.; Khudyakov, Y.E. The molecular epidemiology of hepatitis E virus infection. Virus Res. 2011, 161, 31–39. [Google Scholar] [CrossRef] [PubMed]
- International Committee on Taxonomy of Viruses (ICTV). Available online: https://ictv.global/taxonomy/ (accessed on 8 July 2022).
- Smith, D.B.; Purdy, M.A.; Simmonds, P. Genetic variability and the classification of hepatitis E virus. J. Virol. 2013, 87, 4161–4169. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.B.; Simmonds, P.; Izopet, J.; Oliveira-Filho, E.F.; Ulrich, R.G.; Johne, R.; Koeing, M.; Jameel, S.; Harrison, T.; Meng, X.; et al. Proposed reference sequences for hepatitis E virus subtypes. J. Gen. Virol. 2016, 97, 537–542. [Google Scholar] [CrossRef]
- Rein, D.B.; Stevens, G.A.; Theaker, J.; Wittenborn, J.S.; Wiersma, S.T. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology 2012, 55, 988–997. [Google Scholar] [CrossRef]
- Guthmann, J.P.; Klovstad, H.; Boccia, D.; Hamid, N.; Pinoges, L.; Nizou, J.Y.; Tatay, M.; Diaz, F.; Moren, A.; Grais, R.; et al. A large outbreak of hepatitis E among a displaced population in Darfur, Sudan, 2004: The role of water treatment methods. Clin. Infect. Dis. 2006, 42, 1685–1691. [Google Scholar] [CrossRef] [Green Version]
- Gurley, E.S.; Halder, A.K.; Streatfield, P.K.; Sazzad, H.M.; Huda, T.M.; Hossain, M.J.; Luby, S. Estimating the burden of maternal and neonatal deaths associated with jaundice in Bangladesh: Possible role of hepatitis E infection. Am. J. Public Health 2012, 102, 2248–2254. [Google Scholar] [CrossRef]
- Sharma, S.; Kumar, A.; Kar, P.; Agarwal, S.; Ramji, S.; Husain, S.A.; Sharma, P. Risk factors for vertical transmission of hepatitis E virus infection. J. Viral Hepat. 2017, 24, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Khuroo, M.S.; Kamili, S.; Jameel, S. Vertical transmission of hepatitis E virus. Lancet 1995, 345, 1025–1026. [Google Scholar] [CrossRef]
- Patra, S.; Kumar, A.; Trivedi, S.S.; Puri, M.; Sarin, S.K. Maternal and fetal outcomes in pregnant women with acute hepatitis E virus infection. Ann. Intern. Med. 2007, 147, 28–33. [Google Scholar] [CrossRef]
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N.S.; Ijaz, S.; Izopet, J.; Dalton, H. Hepatitis, E. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef]
- Riveiro-Barciela, M.; Minguez, B.; Girones, R.; Rodriguez-Frias, F.; Quer, J.; Buti, M. Phylogenetic demonstration of hepatitis E infection transmitted by pork meat ingestion. J. Clin. Gastroenterol. 2015, 49, 165–168. [Google Scholar] [CrossRef]
- Renou, C.; Roque-Afonso, A.M.; Pavio, N. Foodborne transmission of hepatitis E virus from raw pork liver sausage, France. Emerg. Infect. Dis. 2014, 20, 1945–1947. [Google Scholar] [CrossRef] [Green Version]
- Namsai, A.; Louisirirotchanakul, S.; Wongchinda, N.; Siripanyaphinyo, U.; Virulhakul, P.; Puthavathana, P.; Gannarong, M.; Ittapong, R. Surveillance of hepatitis A and E viruses contamination in shellfish in Thailand. Lett. Appl. Microbiol. 2011, 53, 608–613. [Google Scholar] [CrossRef]
- Crossan, C.; Baker, P.J.; Craft, J.; Takeuchi, Y.; Dalton, H.R.; Scobie, L. Hepatitis E virus genotype 3 in shellfish, United Kingdom. Emerg. Infect. Dis. 2012, 18, 2085–2087. [Google Scholar] [CrossRef]
- Dalton, H.R.; Bendall, R.; Ijaz, S.; Banks, M. Hepatitis E: An emerging infection in developed countries. Lancet Infect. Dis. 2008, 8, 698–709. [Google Scholar] [CrossRef]
- Sridhar, S.; Yip, C.C.; Lo, K.H.; Wu, S.; Situ, J.; Chew, N.F.; Leung, K.; Chan, H.; Wong, S.; Leung, A.; et al. Hepatitis E virus species C infection in humans, Hong Kong. Clin. Infect. Dis. 2021, ciab919. [Google Scholar] [CrossRef]
- Rivero-Juarez, A.; Frias, M.; Perez, A.B.; Pineda, J.A.; Reina, G.; Fuentes-Lopez, A.; Freyre-Carrillo, C.; Ramirez-Arellano, E.; Alados, J.; Rivero, A. Orthohepevirus C infection as an emerging cause of acute hepatitis in Spain: First report in Europe. J. Hepatol. 2022, 77, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Andonov, A.; Robbins, M.; Borlang, J.; Cao, J.; Hatchette, T.; Stueck, A.; Deschambault, Y.; Murnaghan, K.; Varga, J.; Johnson, L. Rat Hepatitis E Virus Linked to Severe Acute Hepatitis in an Immunocompetent Patient. J. Infect. Dis. 2019, 220, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Brassard, J.; Gagne, M.J.; Genereux, M.; Cote, C. Detection of human food-borne and zoonotic viruses on irrigated, field-grown strawberries. Appl. Environ. Microbiol. 2012, 78, 3763–3766. [Google Scholar] [CrossRef] [Green Version]
- Nieuwenhuijse, D.F.; Koopmans, M.P. Metagenomic Sequencing for Surveillance of Food- and Waterborne Viral Diseases. Front. Microbiol. 2017, 8, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pariente, A.; Renou, C. Epidemiology of hepatitis E: A (re) emerging disease? Presse Med. 2015, 44, 333–338. [Google Scholar] [CrossRef]
- Desai, A.N.; Mohareb, A.M.; Elkarsany, M.M.; Desalegn, H.; Madoff, L.C.; Lassmann, B. Viral Hepatitis E Outbreaks in Refugees and Internally Displaced Populations, sub-Saharan Africa, 2010–2020. Emerg. Infect. Dis. 2022, 28, 1074–1076. [Google Scholar] [CrossRef]
- Aggarwal, R. The Global Prevalence of Hepatitis E Virus Infection and Susceptibility: A Systematic Review; World Health Organization: Geneva, Switzerland, 2010; Available online: http://apps.who.int/iris/bitstream/handle/10665/70513/WHO_IVB_10.14_eng.pdf?sequence=1 (accessed on 4 August 2022).
- Aggarwal, R. Hepatitis E: Historical, contemporary and future perspectives. J. Gastroenterol. Hepatol. 2011, 26 (Suppl. 1), 72–82. [Google Scholar] [CrossRef]
- Chiaruzzi, M.; Zawadzki, E.; Nguyen-Khac, P.; Duhaut, G.; Choukroun, J.L.; Schmit, J.L.; Marolleau, J.P.; Slama, M.; Brochot, E.; Schmit, J.; et al. L’hépatite E: Une Infection Émergente à ne pas Méconnaître, Notamment chez L’immunodéprimé. Étude Transversale Monocentrique. 75ème Congrès Français de Médecine Interne—Brest, 14, 15 et 16 juin 2017/La Revue de Médecine Interne 38S (2017) A49–A109. 2017. Available online: https://www.em-consulte.com/es/article/1122707/article/l-hepatite-e%C2%A0-une-infection-emergente-a-ne-pas-mec (accessed on 4 August 2022).
- Lhomme, S.; Abravanel, F.; Dubois, M.; Sandres-Saune, K.; Mansuy, J.M.; Rostaing, L.; Kamar, N.; Izopet, J. Characterization of the polyproline region of the hepatitis E virus in immunocompromised patients. J. Virol. 2014, 88, 12017–12025. [Google Scholar] [CrossRef] [Green Version]
- Caron, M.; Bouscaillou, J.; Kazanji, M. Acute risk for hepatitis E virus infection among HIV-1-positive pregnant women in central Africa. Virol. J. 2012, 9, 254. [Google Scholar] [CrossRef] [Green Version]
- Amougou Atsama, M.; Atangana, P.J.A.; Noah, D.; Moundipa, P.F.; Pineau, P.; Njouom, R. Hepatitis E virus infection as a promoting factor for hepatocellular carcinoma in Cameroon: Preliminary Observations. Int. J. Infect. Dis. 2017, 64, 4–8. [Google Scholar] [CrossRef] [Green Version]
- Obiri-Yeboah, D.; Asante Awuku, Y.; Adu, J.; Pappoe, F.; Obboh, E.; Nsiah, P.; Amoako-Sakyi, D.; Simpore, J. Sero-prevalence and risk factors for hepatitis E virus infection among pregnant women in the Cape Coast Metropolis, Ghana. PLoS ONE 2018, 13, e0191685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Hepatitis E—Key Facts. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-e (accessed on 4 August 2022).
- Kim, J.H.; Nelson, K.E.; Panzner, U.; Kasture, Y.; Labrique, A.B.; Wierzba, T.F. A systematic review of the epidemiology of hepatitis E virus in Africa. BMC Infect. Dis. 2014, 14, 308. [Google Scholar] [CrossRef] [PubMed]
- Rayis, D.A.; Jumaa, A.M.; Gasim, G.I.; Karsany, M.S.; Adam, I. An outbreak of hepatitis E and high maternal mortality at Port Sudan, Eastern Sudan. Pathog. Glob. Health. 2013, 107, 66–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OMS. Hépatite E—Niger Bulletin D߰information sur les Flambées Épidémiques. 2017. Available online: http://www.who.int/csr/don/05-may-2017-hepatitis-e-niger/fr/ (accessed on 27 July 2018).
- OMS. Hépatite E—Tchad. Bulletin D߰information sur les Flambées Épidémiques. 2017. Available online: http://www.who.int/csr/don/24-january-2017-hepatitis-e-chad/fr/ (accessed on 27 July 2018).
- Teshale, E.H.; Grytdal, S.P.; Howard, C.; Barry, V.; Kamili, S.; Drobeniuc, J.; Hill, V.; Okware, S.; Hu, D.; Holmberg, S. Evidence of person-to-person transmission of hepatitis E virus during a large outbreak in Northern Uganda. Clin. Infect. Dis. 2010, 50, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- De Paschale, M.; Ceriani, C.; Romano, L.; Cerulli, T.; Cagnin, D.; Cavallari, S.; Ndayake, J.; Zaongo, D.; Diombo, K.; Priuli, G. Epidemiology of hepatitis E virus infection during pregnancy in Benin. Trop. Med. Int. Health 2016, 21, 108–113. [Google Scholar] [CrossRef] [Green Version]
- Traore, K.A.; Rouamba, H.; Nebie, Y.; Sanou, M.; Traore, A.S.; Barro, N.; Roques, P. Seroprevalence of fecal-oral transmitted hepatitis A and E virus antibodies in Burkina Faso. PLoS ONE 2012, 7, e48125. [Google Scholar] [CrossRef]
- Stoszek, S.K.; Abdel-Hamid, M.; Saleh, D.A.; El Kafrawy, S.; Narooz, S.; Hawash, Y.; Shebl, F.; Daly, M.; Said, A.; Kassem, E.; et al. High prevalence of hepatitis E antibodies in pregnant Egyptian women. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 95–101. [Google Scholar] [CrossRef]
- Ola, S.O.; Odaibo, G.N.; Olaleye, O.D.; Ayoola, E.A. Hepatitis B and E viral infections among Nigerian healthcare workers. Afr. J. Med. Sci. 2012, 41, 387–391. [Google Scholar]
- Sadio, B. Study of Seroprevalence in an Epidemic Context of the Hepatitis E Virus in the Region of Kédougou. Master߰s Thesis, Faculté de Médecine, de Pharmacie et d߰Odontologie de l߰Université Cheikh Anta DIOP, Dakar, Sénégal, 2016. Available online: http://bibnum.ucad.sn/viewer.php?c=mmoires&d=memm%5f2016%5f0193 (accessed on 4 August 2022).
- ANSD. Enquête Démographique et de Santé Continue (EDS-Continue 2018); ANSD, ICF: Rockville, MA, USA, 2018. [Google Scholar]
- ANSD. Enquête Continue sur la Prestation des Services de Soins de Santé (ECPSS) du Sénégal 2014; ANSD, ICF International: Calverton, MA, USA, 2015; pp. 1–256. [Google Scholar]
- Bagulo, H.; Majekodunmi, A.O.; Welburn, S.C. Hepatitis E in Sub Saharan Africa—A significant emerging disease. One Health 2021, 11, 100186. [Google Scholar] [CrossRef]
- Al Absi, E.S.; Al-Sadeq, D.W.; Khalili, M.; Younes, N.; Al-Dewik, N.; Abdelghany, S.K.; Abouzid, S.; Al Thani, A.; Yassine, H.; Coyle, P.; et al. The prevalence of HEV among non-A-C hepatitis in Qatar and efficiency of serological markers for the diagnosis of hepatitis E. BMC Gastroenterol. 2021, 21, 266. [Google Scholar] [CrossRef]
- Ifeorah, I.M.; Faleye, T.O.C.; Bakarey, A.S.; Adewumi, M.O.; Akere, A.; Omoruyi, E.C.; Ogunwale, A.; Adeniji, J. Acute Hepatitis E Virus Infection in Two Geographical Regions of Nigeria. J. Pathog. 2017, 2017, 4067108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adjei, A.A.; Tettey, Y.; Aviyase, J.T.; Adu-Gyamfi, C.; Obed, S.; Mingle, J.A.; Ayeh-Kumi, P.; Adiku, T. Hepatitis E virus infection is highly prevalent among pregnant women in Accra, Ghana. Virol. J. 2009, 6, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niguse, S.; Hailekiros, H.; Buruh, G.; Dejene, T.; Berhe, N.; Asmelash, T. Seroprevalence and risk factors of Hepatitis E virus infection among pregnant women attending antenatal care in health facilities of Tigray, Northern Ethiopia. J. Med. Virol. 2018, 90, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Dimeglio, C.; Kania, D.; Mantono, J.M.; Kagone, T.; Zida, S.; Tassembedo, S.; Dicko, A.; Tinto, B.; Yaro, S.; Hien, H.; et al. Hepatitis E Virus Infections among Patients with Acute Febrile Jaundice in Burkina Faso. Viruses 2019, 11, 554. [Google Scholar] [CrossRef] [Green Version]
- Coursaget, P.; Leboulleux, D.; Gharbi, Y.; Enogat, N.; Ndao, M.A.; Coll-Seck, A.M.; Kastally, R. Etiology of acute sporadic hepatitis in adults in Senegal and Tunisia. Scand. J. Infect. Dis. 1995, 27, 9–11. [Google Scholar] [CrossRef]
- Crato, M.; Michel, P.; Rodier, G.R.; Ka, M.; Hugard, L.; Diouf, G. Viral markers of acute hepatitis: A, B, C, D, and E in Dakar. October 92–October 93. Dakar Med. 1993, 38, 183–185. [Google Scholar]
- Diallo, A.S.; Faye, B.; Leguenno, B.; Pillot, J. Biological diagnosis of hepatitis e. Completion of a test for detection of infected patients. Dakar Med. 1992, 37, 95–102. [Google Scholar]
- Cevrioglu, A.S.; Altindis, M.; Tanir, H.M.; Aksoy, F. Investigation of the incidence of hepatitis E virus among pregnant women in Turkey. J. Obstet. Gynaecol. Res. 2004, 30, 48–52. [Google Scholar] [CrossRef]
- Hannachi, N.; Hidar, S.; Harrabi, I.; Mhalla, S.; Marzouk, M.; Ghzel, H.; Ghannem, H.; Khairi, H.; Boukadida, J. Seroprevalence and risk factors of hepatitis E among pregnant women in central Tunisia. Pathol. Biol. 2011, 59, e115–e118. [Google Scholar] [CrossRef]
- Amanya, G.; Kizito, S.; Nabukenya, I.; Kalyango, J.; Atuheire, C.; Nansumba, H.; Abowye, S.; Opio, D.; Kibuuka, E.; Karamagi, C. Risk factors, person, place and time characteristics associated with Hepatitis E Virus outbreak in Napak District, Uganda. BMC Infect Dis. 2017, 17, 451. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Study Sites | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Saint-Louis (n = 400) | Dakar (n = 166) | Kédougou (n = 397) | Ziguinchor (n = 264) | All Sites (n = 1227) | ||||||
| Frequency (%) | Median | Frequency (%) | Median | Frequency (%) | Median | Frequency (%) | Median | Frequency (%) | Median | |
| Range of age | ||||||||||
| 18–23 | 112 (28) | 20 | 49 (29.5) | 21 | 256 (64.5) | 19 | 111 (42) | 20 | 528 (43) | 20 |
| 24–29 | 136 (34) | 26 | 44 (26.5) | 27 | 90 (22.7) | 26 | 87 (33) | 26 | 357 (29.1) | 26 |
| 30–35 | 101 (25.3) | 32 | 48 (28.9) | 32.5 | 29 (7.3) | 30 | 45 (17) | 32 | 223 (18.2) | 32 |
| 36 and above | 51 (12.8) | 36 | 25 (15.1) | 37 | 22 (5.5) | 38 | 21 (8) | 39 | 119 (9.7) | 38 |
| Educational level | ||||||||||
| None | 62 (15.5) | . | 25 (15.1) | . | 233 (58.7) | . | 69 (26.1) | . | 389 (31.7) | . |
| Primary | 170 (42.5) | . | 46 (27.7) | . | 82 (20.7) | . | 77 (29.2) | . | 375 (30.6) | . |
| Secondary | 122 (30.5) | . | 52 (31.3) | . | 75 (18.9) | . | 104 (39.4) | . | 353 (28.8) | . |
| Higher | 46 (11.5) | . | 43 (25.9) | . | 7 (1.8) | . | 14 (5.3) | . | 110 (9) | . |
| Marital status | ||||||||||
| unspecified | 11 (2.8) | . | 0 (0) | . | 16 (4.0) | . | 4 (1.5) | . | 31 (2.5) | . |
| Single | 8 (2) | . | 6 (3.6) | . | 12 (3) | . | 39 (14.8) | . | 65 (5.2) | . |
| Married | 381 (95.3) | . | 160 (96.4) | . | 369 (93) | . | 220 (83.3) | . | 1130 (92) | . |
| Divorced or widowed | 0 (0) | . | 0 (0) | . | 0 (0) | . | 1 (0.4) | . | 1 (0.08) | . |
| Regular income (paid work) | ||||||||||
| unspecified | 6 (1.5) | . | 1 (0.6) | . | 36 (9.1) | . | 4 (1.5) | . | 47 (3.8) | . |
| Yes | 47 (11.8) | . | 76 (45.8) | . | 63 (15.9) | . | 43 (16.3) | . | 229 (18.7) | . |
| No | 347 (86.8) | . | 89 (53.6) | . | 298 (75.1) | . | 217 (82.2) | . | 951 (77.5) | . |
| Access to safe water supply services | ||||||||||
| unspecified | 2 (0.5) | . | 0 (0) | . | 24 (6) | . | 5 (1.9) | . | 31 (2.5) | . |
| Occasionally | 0 (0) | . | 0 (0) | . | 0 (0) | . | 10 (3.8) | . | 10 (0.8) | . |
| Yes | 387 (96.8) | . | 166 (100) | . | 311 (78.3) | . | 98 (37.1) | . | 962 (78.4) | . |
| No | 11 (2.8) | . | 0 (0) | . | 62 (15.6) | . | 151 (57.2) | . | 224 (18.3) | . |
| Access to sanitation services | ||||||||||
| unspecified | 1 (0.3) | . | 0 (0) | . | 12 (3) | . | 5 (1.9) | . | 18 (1.5) | . |
| Occasionally | 0 (0) | . | 0 (0) | . | 0 (0) | . | 5 (1.9) | . | 5 (0.4) | . |
| Yes | 388 (97) | . | 166 (100) | . | 363 (91.4) | . | 141 (53.4) | . | 1058 (86.2) | . |
| No | 11 (2.8) | . | 0 (0) | . | 22 (5.5) | . | 113 (42.8) | . | 146 (11.9) | . |
| Disinfection of food products that are not wrapped and handled by hand (examples: Vegetables. fruits. etc.) | ||||||||||
| unspecified | 1 (0.3) | . | 0 (0) | . | 28 (7.1) | . | 3 (1.1) | . | 32 (2.6) | . |
| Occasionally | 59 (14.8) | . | 0 (0) | . | 0 (0) | . | 1 (0.4) | . | 60 (4.9) | . |
| Yes | 285 (71.3) | . | 166 (100) | . | 348 (87.7) | . | 182 (68.9) | . | 981 (79.9) | . |
| 55 (13.8) | . | 0 | . | 21 (5.3) | . | 78 (29.5) | . | 154 (12.5) | . | |
| Systematic hand washing | ||||||||||
| unspecified | 0 (0) | . | 0 (0) | . | 16 (4) | . | 4 (1.5) | . | 20 (1.6) | . |
| Occasionally | 0 (0) | . | 0 (0) | . | 0 (0) | . | 6 (2.3) | . | 6 (0.5) | . |
| Yes | 392 (98) | . | 166 (100) | . | 350 (88.2) | . | 206 (78) | . | 1114 (90.8) | . |
| No | 8 (2) | . | 0 (0) | . | 31 (7.8) | . | 48 (18.2) | . | 87 (7.1) | . |
| HEV markers seroprevalance | ||||||||||
| HEV IgM Positive | 2 (0.5) | . | 0 (0) | . | 4 (1) | . | 0 (0) | . | 6 (0.5) | . |
| HEV IgG Positive | 42 (10.5) | . | 7 (4.2) | . | 38 (9.6) | . | 4 (1.5) | . | 91 (7.4) | . |
| IgM HEV | IgG HEV | |||
|---|---|---|---|---|
| [Age Groups] (%) | n (%) | p-Value | n (%) | p-Value |
| [18,19,20,21,22,23], n = 528 (43) | 1 (0.18) | 0.0372 | 28 (5.30) | 0.0048 |
| [24,25,26,27,28,29], n = 357 (29.1) | 2 (0.56) | 26 (7.28) | ||
| [30,31,32,33,34,35], n = 223 (18.2) | 2 (0.89) | 19 (8.52) | ||
| ≥36 years, n = 119 (9.7) | 1 (0.84) | 18 (15.12) | ||
| Total (n = 1227) | 6 (0.48) | 91 (7.41) | ||
| Location (Frequency) | ||||
| Saint-Louis (n = 400) | 2 (0.50) | 0.3293 | 42 (10.50) | 0.0133 |
| Dakar (n = 166) | 0 (0.00) | 7 (4.21) | ||
| Ziguinchor (n = 264) | 0 (0.00) | 4 (1.51) | ||
| Kédougou (n = 397) | 4 (1.00) | 38 (9.57) | ||
| Total (n = 1227) | 6 (0.48) | 91 (7.41) | ||
| IgM HEV | IgG HEV | ||||||
|---|---|---|---|---|---|---|---|
| Educational Level | Frequency (%) | n | Prevalence | p-Value | n | Prevalence | p-Value |
| None | 389 (31.7) | 4 | 1.03 | 0.4655 | 32 | 8.23 | 0.4017 |
| Primary | 375 (30.6) | 1 | 0.27 | 30 | 8 | ||
| Secondary | 353 (28.8) | 1 | 0.28 | 25 | 7.08 | ||
| Higher | 110 (9) | 0 | 0 | 4 | 3.64 | ||
| Marital status | |||||||
| unspecified | 31 (2.5) | 0 | 0 | 0.9999 | 2 | 6.45 | < 0.0001 |
| Single | 65 (5.2) | 0 | 0 | 7 | 10.77 | ||
| Maried | 1130 (92) | 6 | 0.53 | 82 | 7.26 | ||
| Divorced or widowed | 1 (0.08) | 0 | 0 | 0 | 0 | ||
| Regular income (paid work) | |||||||
| unspecified | 47 (3.8) | 0 | 0 | 1 | 1 | 2.13 | 0.0043 |
| Yes | 229 (18.7) | 1 | 0.44 | 12 | 5.24 | ||
| No | 951 (77.5) | 5 | 0.53 | 78 | 8.2 | ||
| Access to the potable water supply service | |||||||
| unspecified | 31 (2.5) | 1 | 3.23 | 0.1958 | 2 | 6.45 | 0.4001 |
| Occasionally | 10 (0.8) | 0 | 0 | 0 | 0 | ||
| Yes | 962 (78.4) | 4 | 0.42 | 78 | 8.11 | ||
| No | 224 (18.3) | 1 | 0.45 | 11 | 4.91 | ||
| Access to sanitation services (Adequate toilets, appropriate wastewater disposal system) | |||||||
| unspecified | 18 (1.5) | 0 | 0 | 1 | 2 | 11.11 | 0.0006 |
| Occasionally | 5 (0.4) | 0 | 0 | 0 | 0 | ||
| Yes | 1058 (86.2) | 6 | 0.57 | 87 | 8.22 | ||
| No | 146 (11.9) | 0 | 0 | 2 | 1.37 | ||
| Disinfection of food products that are not wrapped and hand-handled (examples: Vegetables, fruits, etc.) | |||||||
| unspecified | 32 (2.6) | 0 | 0 | 1 | 2 | 6.25 | 0.5984 |
| Occasionally | 60 (4.9) | 0 | 0 | 6 | 10 | ||
| Yes | 981 (79.9) | 6 | 0.61 | 75 | 7.65 | ||
| No | 154 (12.5) | 0 | 0 | 8 | 5.19 | ||
| Systematic hand washing | |||||||
| unspecified | 20 (1.6) | 0 | 0 | 0.4406 | 2 | 10 | 0.1950 |
| Occasionally | 6 (0.5) | 0 | 0 | 0 | 0 | ||
| Yes | 1114 (90.8) | 5 | 0.45 | 87 | 7.81 | ||
| No | 87 (7.1) | 1 | 1.15 | 2 | 2.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diouara, A.A.M.; Lo, S.; Nguer, C.M.; Senghor, A.; Diop Ndiaye, H.; Manga, N.M.; Danfakha, F.; Diallo, S.; Faye Dieme, M.E.; Thiam, O.; et al. Hepatitis E Virus Seroprevalence and Associated Risk Factors in Pregnant Women Attending Antenatal Consultations in Senegal. Viruses 2022, 14, 1742. https://doi.org/10.3390/v14081742
Diouara AAM, Lo S, Nguer CM, Senghor A, Diop Ndiaye H, Manga NM, Danfakha F, Diallo S, Faye Dieme ME, Thiam O, et al. Hepatitis E Virus Seroprevalence and Associated Risk Factors in Pregnant Women Attending Antenatal Consultations in Senegal. Viruses. 2022; 14(8):1742. https://doi.org/10.3390/v14081742
Chicago/Turabian StyleDiouara, Abou Abdallah Malick, Seynabou Lo, Cheikh Momar Nguer, Assane Senghor, Halimatou Diop Ndiaye, Noël Magloire Manga, Fodé Danfakha, Sidy Diallo, Marie Edouard Faye Dieme, Ousmane Thiam, and et al. 2022. "Hepatitis E Virus Seroprevalence and Associated Risk Factors in Pregnant Women Attending Antenatal Consultations in Senegal" Viruses 14, no. 8: 1742. https://doi.org/10.3390/v14081742