
SARS-CoV-2 Specific Immune Response and Inflammatory Profile in Advanced HIV-Infected Persons during a COVID-19 Outbreak

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
Definitions
2.2. Statistical Analyses
2.3. Laboratory Tests
3. Results
3.1. Characteristics of the Study Population
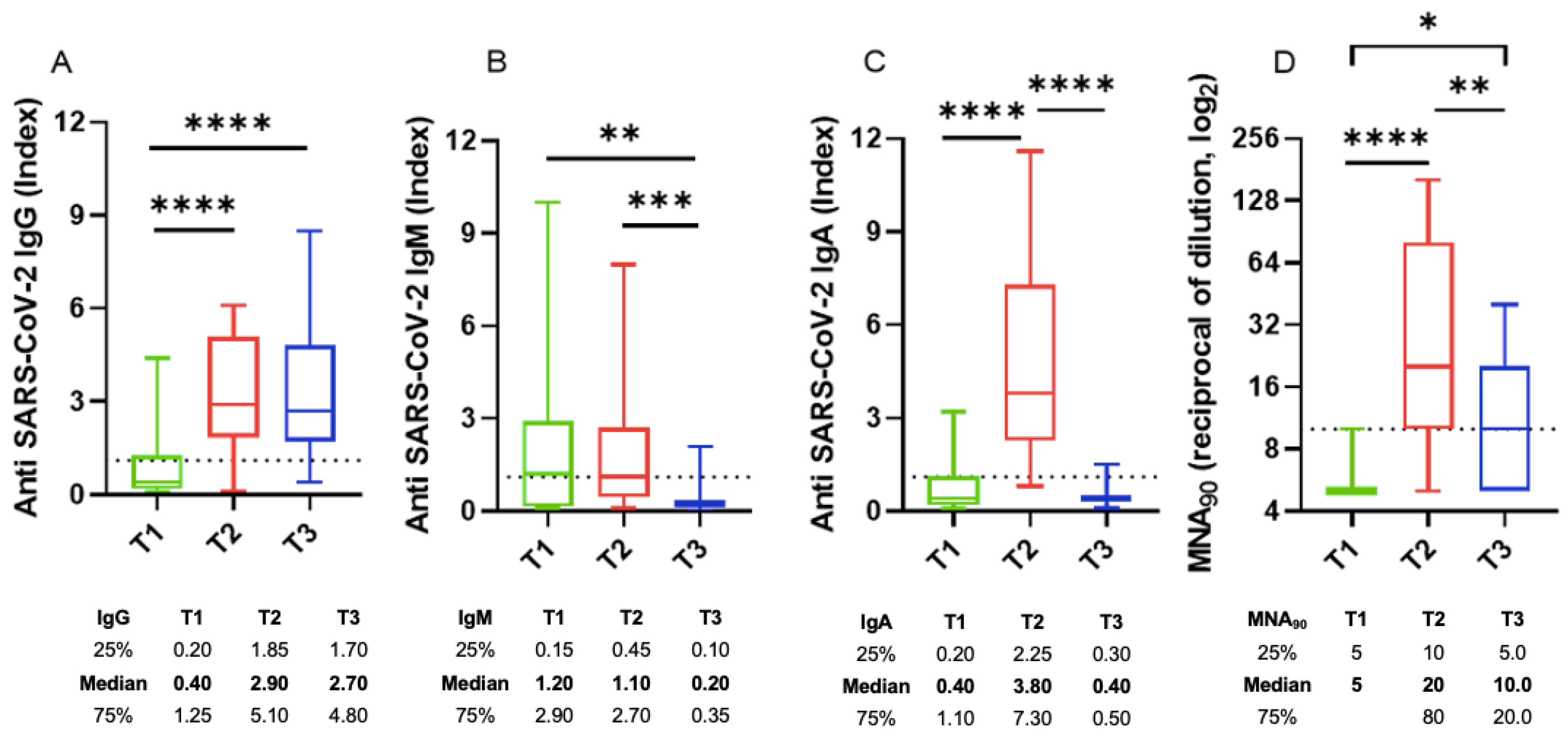
SARS-CoV-2 Specific Immune Response
3.2. Comparisons of the Characteristics of the Three Groups Included in the Analysis
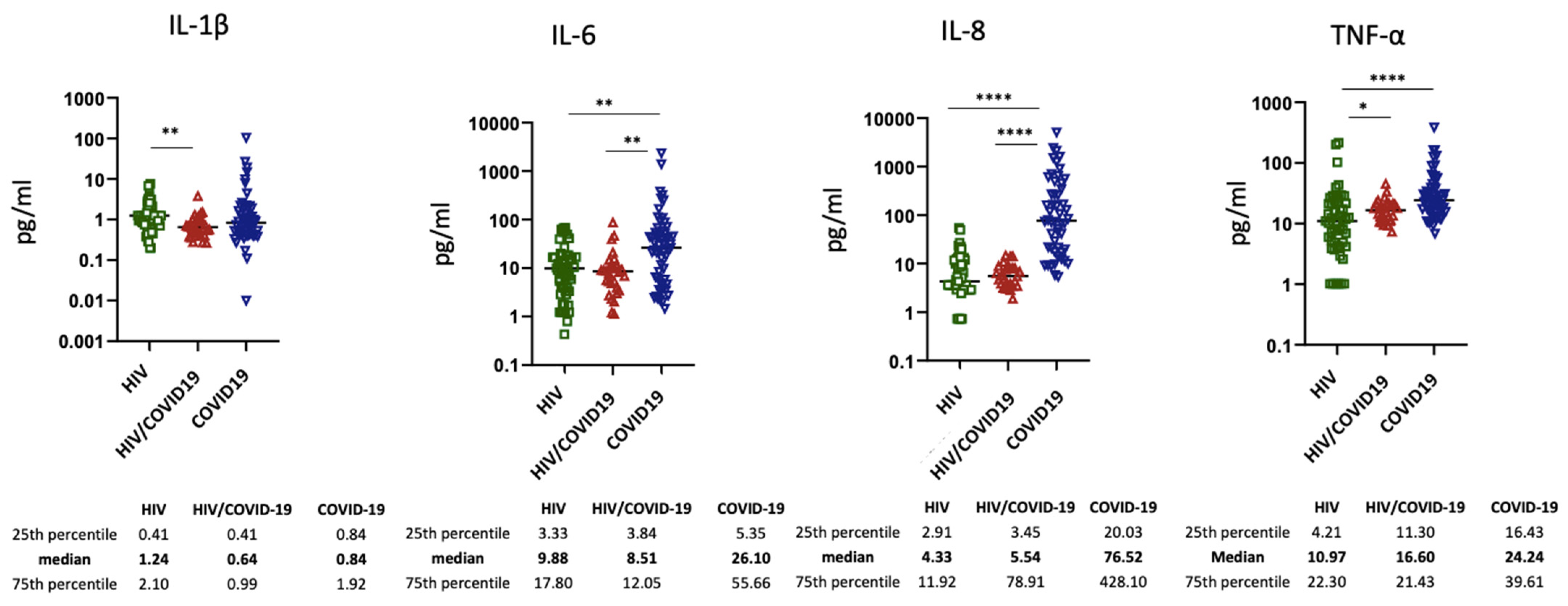
3.3. Inflammatory Biomarkers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blanco, J.L.; Ambrosioni, J.; Garcia, F.; Martínez, E.; Soriano, A.; Mallolas, J.; Miro, J.M.; COVID-19 in HIV Investigators. COVID-19 in patients with HIV: Clinical case series. Lancet HIV 2020, 7, e314–e316. [Google Scholar] [CrossRef]
- Härter, G.; Spinner, C.D.; Roider, J.; Bickel, M.; Krznaric, I.; Grunwald, S.; Schabaz, F.; Gillor, D.; Postel, N.; Mueller, M.C.; et al. COVID-19 in people living with human immunodeficiency virus: A case series of 33 patients. Infection 2020, 48, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Ming, F.; Dong, Y.; Zhang, Q.; Zhang, X.; Mo, P.; Feng, Y.; Liang, K. A Survey for COVID-19 among HIV/AIDS Patients in Two Districts of Wuhan, China (3/4/2020). Available online: https://ssrn.com/abstract=3550029 (accessed on 1 June 2021). [CrossRef]
- Karmen-Tuohy, S.; Carlucci, P.M.; Zervou, F.N.; Zacharioudakis, I.M.; Rebick, G.; Klein, E.; Reich, J.; Jones, S.; Rahimian, J. Outcomes among HIV-Positive Patients Hospitalized with COVID-19. J. Acquir. Immune Defic Syndr. 2020, 85, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Gervasoni, C.; Meraviglia, P.; Riva, A.; Giacomelli, A.; Oreni, L.; Minisci, D.; Atzori, C.; Ridolfo, A.; Cattaneo, D. Clinical Features and Outcomes of Patients With Human Immunodeficiency Virus With COVID-19. Clin. Infect. Dis. 2020, 71, 2276–2278. [Google Scholar] [CrossRef] [PubMed]
- Shalev, N.; Scherer, M.; Lasota, E.D.; Antoniou, P.; Yin, M.T.; Zucker, J.; Sobieszczyk, M.E. Clinical Characteristics and Outcomes in People Living with Human Immunodeficiency Virus Hospitalized for Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2294–2297. [Google Scholar] [CrossRef] [PubMed]
- Vizcarra, P.; Pérez-Elías, M.J.; Quereda, C.; Moreno, A.; Vivancos, M.J.; Dronda, F.; Casado, J.L.; COVID-19 ID Team. Description of COVID-19 in HIV-infected individuals: A single-centre, prospective cohort. Lancet HIV 2020, 7, e554–e564. [Google Scholar] [CrossRef]
- Cabello, A.; Zamarro, B.; Nistal, S.; Victor, V.; Hernández, J.; Prieto-Pérez, L.; Carrillo, I.; Álvarez, B.; Fernández-Roblas, R.; Hernández-Segurado, M.; et al. COVID-19 in people living with HIV: A multicenter case-series study. Int. J. Infect. Dis. 2021, 102, 310–315. [Google Scholar] [CrossRef]
- Inciarte, A.; Gonzalez-Cordon, A.; Rojas, J.; Torres, B.; De Lazzari, E.; De La Mora, L.; Martinez-Rebollar, M.; Laguno, M.; Callau, P.; Gonzalez-Navarro, A.; et al. Clinical characteristics, risk factors, and incidence of symptomatic coronavirus disease 2019 in a large cohort of adults living with HIV: A single-center, prospective observational study. AIDS 2020, 34, 1775–1780. [Google Scholar] [CrossRef]
- Charre, C.; Icard, V.; Pradat, P.; Brochier, C.; Lina, B.; Chidiac, C.; Cotte, L. Coronavirus disease 2019 attack rate in HIV-infected patients and in preexposure prophylaxis users. AIDS 2020, 34, 1765–1770. [Google Scholar] [CrossRef]
- Cooper, T.J.; Woodward, B.L.; Alom, S.; Harky, A. Coronavirus disease 2019 (COVID-19) outcomes in HIV/AIDS patients: A systematic review. HIV Med. 2020, 21, 567–577. [Google Scholar] [CrossRef]
- Sigel, K.; Swartz, T.; Golden, E.; Paranjpe, I.; Somani, S.; Richter, F.; De Freitas, J.K.; Miotto, R.; Zhao, S.; Polak, P.; et al. Coronavirus 2019 and People Living With Human Immunodeficiency Virus: Outcomes for Hospitalized Patients in New York City. Clin. Infect. Dis. 2020, 71, 2933–2938. [Google Scholar] [CrossRef]
- Brown, L.B.; Spinelli, M.A.; Gandhi, M. The interplay between HIV and COVID-19: Summary of the data and responses to date. Curr. Opin. HIV AIDS 2021, 16, 63–73. [Google Scholar] [CrossRef]
- Boulle, A.; Davies, M.A.; Hussey, H.; Ismail, M.; Morden, E.; Vundle, Z.; Zweigenthal, V.; Mahomed, H.; Paleker, M.; Pienaar, D.; et al. Risk factors for COVID-19 death in a population cohort study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2020, 29, ciaa1198. [Google Scholar]
- Geretti, A.M.; Stockdale, A.J.; Kelly, S.H.; Cevik, M.; Collins, S.; Waters, L.; Villa, G.; Docherty, A.; Harrison, E.M.; Turtle, L.; et al. Outcomes of COVID-19 related hospitalization among people with HIV in the ISARIC WHO Clinical Characterization Protocol (UK): A prospective observational study. Clin. Infect. Dis. 2020, 23, ciaa1605. [Google Scholar]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; Morton, C.E.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2021, 8, e24–e32. [Google Scholar] [CrossRef]
- Tesoriero, J.M.; Swain, C.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. Elevated COVID-19 outcomes among persons living with diagnosed HIV infection in New York State: Results from a population-level match of HIV, COVID-19, and hospitalization databases. JAMA Netw Open. 2021, 4, e2037069. [Google Scholar] [CrossRef]
- Mondi, A.; Cimini, E.; Colavita, F.; Cicalini, S.; Pinnetti, C.; Matusali, G.; Casetti, R.; Maeurer, M.; Vergori, A.; Mazzotta, V.; et al. COVID-19 in people living with HIV: Clinical implications of dynamics of the immune response to SARS-CoV-2. J. Med. Virol. 2021, 93, 1796–1804. [Google Scholar] [CrossRef]
- HIV/AIDS Program. WHO Case Definitions of HIV for Surveillance and Revised Clinical Staging and Immunological Classification of HIV-Related Disease in Adults and Children. 2007. Available online: https://www.who.int/hiv/pub/guidelines/HIVstaging150307.pdf (accessed on 1 June 2021).
- NIH COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 1 June 2021).
- Matusali, G.; Colavita, F.; Lapa, D.; Meschi, S.; Bordi, L.; Piselli, P.; Gagliardini, R.; Corpolongo, A.; Nicastri, E.; Antinori, A.; et al. SARS-CoV-2 Serum Neutralization Assay: A Traditional Tool for a Brand-New Virus. Viruses 2021, 13, 655. [Google Scholar] [CrossRef]
- Childs, K.; Post, F.A.; Norcross, C.; Ottaway, Z.; Hamlyn, E.; Quinn, K.; Juniper, T.; Taylor, C. Hospitalized Patients With COVID-19 and Human Immunodeficiency Virus: A Case Series. Clin. Infect. Dis. 2020, 71, 2021–2022. [Google Scholar] [CrossRef]
- Etienne, N.; Karmochkine, M.; Slama, L.; Pavie, J.; Batisse, D.; Usubillaga, R.; Letembet, V.-A.; Brazille, P.; Canouï, E.; Slama, D.; et al. HIV infection and COVID-19: Risk factors for severe disease. AIDS 2020, 34, 1771–1774. [Google Scholar] [CrossRef]
- Hoffmann, C.; Casado, J.L.; Härter, G.; Vizcarra, P.; Moreno, A.; Cattaneo, D.; Meraviglia, P.; Spinner, C.D.; Schabaz, F.; Grunwald, S.; et al. Immune-deficiency is a risk factor for severe COVID-19 in people living with HIV. HIV Med. 2021, 22, 372–378. [Google Scholar] [CrossRef]
- Zheng, H.Y.; Zhang, M.; Yang, C.X.; Zhang, N.; Wang, X.C.; Yang, X.P.; Dong, X.-Q.; Zheng, Y.-T. Elevated exhaustion levels and reduced functional diversity of T cells in peripheral blood may predict severe progression in COVID-19 patients. Cell Mol. Immunol. 2020, 17, 541–543. [Google Scholar] [CrossRef]
- Alrubayyi, A.; Gea-Mallorquí, E.; Touizer, E.; Hameiri-Bowen, D.; Kopycinski, J.; Charlton, B.; Fisher-Pearson, N.; Muir, L.; Rosa, A.; Roustan, C.; et al. Characterization of humoral and SARS-CoV-2 specific T cell responses in people living with HIV. bioRxiv 2021, rs.3.rs-309746, Update in Nat. Commun. 2021, 12, 5839. [Google Scholar] [CrossRef]
- Lederman, M.M.; Funderburg, N.T.; Sekaly, R.P.; Klatt, N.R.; Hunt, P.W. Residual immune dysregulation syndrome in treated HIV infection. Adv. Immunol. 2013, 119, 51–83. [Google Scholar]
- Levy, I.; Finesod, A.W.; Litchevsky, V.; Biber, A.; Indenbaum, V.; Olmer, L.; Huppert, A.; Mor, O.; Goldstein, M.; Levin, E.G.; et al. Immunogenicity and Safety of the BNT162b2 mRNA COVID-19 Vaccine in People Living with HIV-1. Available online: https://ssrn.com/abstract=3829650 (accessed on 1 June 2021). [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Correction to: Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 1294–1297. [Google Scholar] [CrossRef] [Green Version]
- Ho, H.E.; Peluso, M.J.; Margus, C.; Matias Lopes, J.P.; He, C.; Gaisa, M.M.; Osorio, G.; Aberg, J.A.; Mullen, M.P. Clinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People With Human Immunodeficiency Virus. J. Infect. Dis. 2021, 223, 403–408. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘cytokine storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef]
- Kuller, L.L.; Tracy, R.R.; Belloso, W.W.; De Wit, S.; Drummond, F.F.; Lane, C.H.; Ledergerber, B.; Lundgren, J.; Neuhaus, J.J.; Nixon, D.D.; et al. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. 2008, 5, e203. [Google Scholar] [CrossRef]
- Isernia, V.; Julia, Z.; Le Gac, S.; Bachelard, A.; Landman, R.; Lariven, S.; Joly, V.; Deconinck, L.; Rioux, C.; Lescure, X.; et al. SARS-CoV2 infection in 30 HIV-infected patients followed-up in a French University Hospital. Int. J. Infect. Dis. 2020, 101, 49–51. [Google Scholar] [CrossRef]
- Sharov, K.S. HIV/SARS-CoV-2 co-infection: T cell profile, cytokine dynamics and role of exhausted lymphocytes. Int. J. Infect. Dis. 2021, 102, 163–169. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| General Characteristics | HIV Positive COVID-19 | HIV Positive No COVID-19 | p-Value # | COVID-19 No HIV | p-Value * |
|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | |||
| n = 30 | n = 52 | n = 58 | |||
| Gender, n (%) | |||||
| M | 23 (76.7) | 44 (84.6) | 0.332 | 42 (72.4) | 0.667 |
| Age, years, median (IQR) | 57 (53–62) | 49 (43–53) | <0.001 | 58 (42–71) | 0.817 |
| Mode of transmission of HIV, n (%) | |||||
| Unprotected sex | 18 (60.0) | 24 (46.2) | 0.069 | ||
| IVDUs | 12 (40.0) | 20 (38.5) | |||
| Unknown | - | 8 (15.4) | |||
| Years of HIV infection, median (IQR) | 18 (15–29) | 16 (9–20) | 0.026 | ||
| Nadir of CD4 count, cell/mmc, median (IQR) | 57 (23–100) | 92 (52–149) | 0.046 | ||
| CD4 count at test, cell/mmc, median (IQR) | 348 (186–565) | 316 (180–525) | 0.597 | ||
| CD8 count at test, cell/mmc, median (IQR) | 756 (563–1124) | 600 (384–917) | 0.064 | ||
| Antiretroviral treatment, n(%) | 30 (100) | 52(100) | |||
| At least 1 comorbidity, n (%) | 25 (83.3) | 38 (65.5) | 0.079 | ||
| COVID-19 symptoms, n (%) | 9 (30.0) | 54 (93.1) | <0.001 | ||
| COVID-19 pneumonia, n (%) | 6 (30) | 50 (86.2) | <0.001 | ||
| SpO2 at COVID-19 diagnosis/hospital admission, median (IQR) | 96 (96–96) | 96 (95–98) | 0.542 | ||
| Death with COVID-19, n (%) | 3 (10.0) | 9 (15.5) | 0.475 | ||
| Time to viral clearance, days, median (IQR) | 18 (16–25) | 17 (10–25) | 0.137 | ||
| Steroid treatment, n (%) | 6 (20.0) | 30 (51.7) | 0.004 | ||
| Remdesivir, n (%) | 4 (13.3) | 5 (8.6) | 0.489 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vergori, A.; Boschini, A.; Notari, S.; Lorenzini, P.; Castilletti, C.; Colavita, F.; Matusali, G.; Tartaglia, E.; Gagliardini, R.; Boschi, A.; et al. SARS-CoV-2 Specific Immune Response and Inflammatory Profile in Advanced HIV-Infected Persons during a COVID-19 Outbreak. Viruses 2022, 14, 1575. https://doi.org/10.3390/v14071575
Vergori A, Boschini A, Notari S, Lorenzini P, Castilletti C, Colavita F, Matusali G, Tartaglia E, Gagliardini R, Boschi A, et al. SARS-CoV-2 Specific Immune Response and Inflammatory Profile in Advanced HIV-Infected Persons during a COVID-19 Outbreak. Viruses. 2022; 14(7):1575. https://doi.org/10.3390/v14071575
Chicago/Turabian StyleVergori, Alessandra, Antonio Boschini, Stefania Notari, Patrizia Lorenzini, Concetta Castilletti, Francesca Colavita, Giulia Matusali, Eleonora Tartaglia, Roberta Gagliardini, Andrea Boschi, and et al. 2022. "SARS-CoV-2 Specific Immune Response and Inflammatory Profile in Advanced HIV-Infected Persons during a COVID-19 Outbreak" Viruses 14, no. 7: 1575. https://doi.org/10.3390/v14071575