
Point-of-Care Tests for Rapid Detection of Porcine Epidemic Diarrhea Virus: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection and Data Extraction
2.3. Data Analysis
3. Results
3.1. Literature Search
3.2. Characteristics and Quality Assessment
3.3. Diagnostic Performance of POCTs for PEDV
3.4. Heterogeneity Exploration
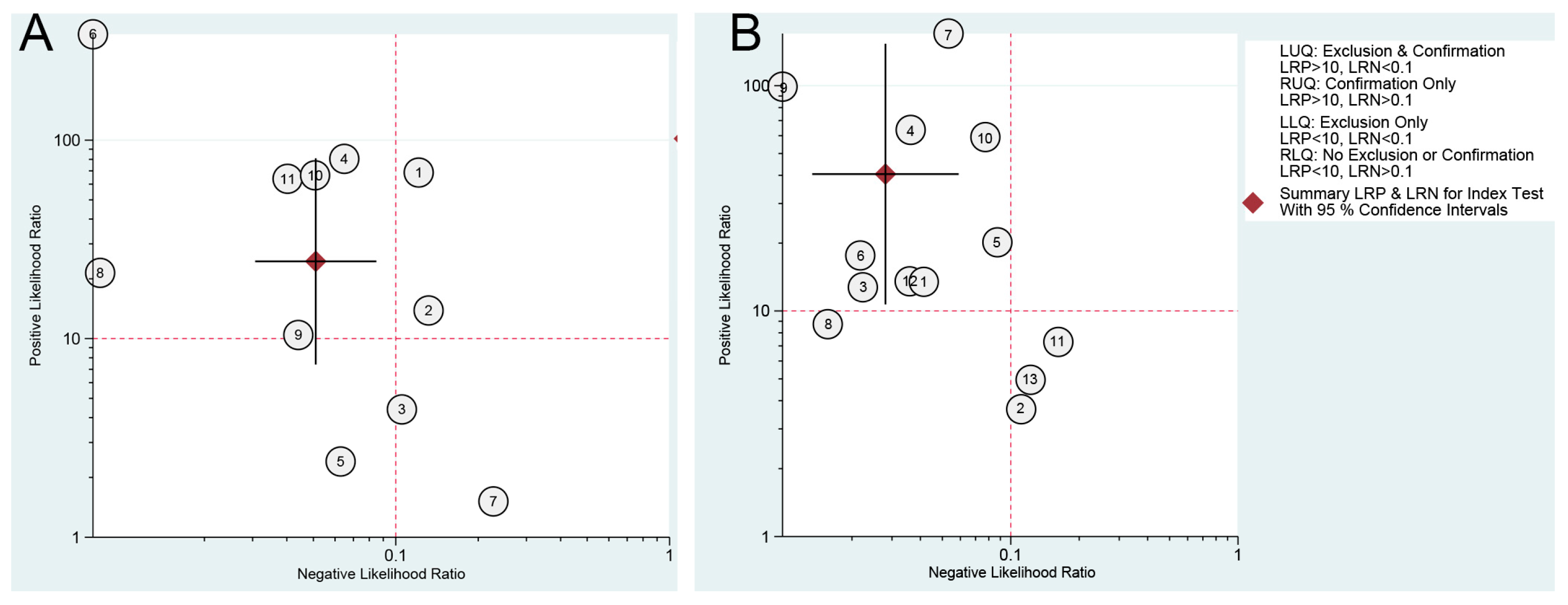
3.5. Clinical Utility
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turlewicz-Podbielska, H.; Pomorska-Mól, M. Porcine coronaviruses: Overview of the state of the art. Virol. Sin. 2021, 36, 833–851. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Ji, J.; Chen, X.; Bi, Y.; Li, J.; Wang, Q.; Hu, T.; Song, H.; Zhao, R.; Chen, Y.; et al. Identification of novel bat coronaviruses sheds light on the evolutionary origins of SARS-CoV-2 and related viruses. Cell 2021, 184, 4380–4391. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.C.; Zhang, J.X.; Zhang, S.Y.; Wang, P.; Fan, X.H.; Li, L.F.; Li, G.; Dong, B.Q.; Liu, W.; Cheung, C.L.; et al. Prevalence and genetic diversity of coronaviruses in bats from China. J. Virol. 2006, 80, 7481–7490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepin, K.M.; Miller, R.S.; Wilber, M.Q. A framework for surveillance of emerging pathogens at the human-animal interface: Pigs and coronaviruses as a case study. Prev. Vet. Med. 2021, 188, 105281. [Google Scholar] [CrossRef]
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.K.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Qiao, S.; Yang, Y.; Guo, J.; Xie, S.; Zhou, E.; Zhang, G. Genome sequencing and analysis of a novel recombinant porcine epidemic diarrhea virus strain from Henan, China. Virus Genes 2016, 52, 91–98. [Google Scholar] [CrossRef]
- Pascual-Iglesias, A.; Sanchez, C.M.; Penzes, Z.; Sola, I.; Enjuanes, L.; Zuniga, S. Recombinant chimeric transmissible gastroenteritis virus (TGEV)—Porcine epidemic diarrhea virus (PEDV) virus provides protection against virulent PEDV. Viruses 2019, 11, 682–699. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Nguyen, V.G.; Huynh, T.M.; Park, Y.H.; Park, B.K.; Chung, H.C. Molecular characterization of porcine epidemic diarrhea virus and Its new genetic classification based on the nucleocapsid gene. Viruses 2020, 12, 1562–1576. [Google Scholar] [CrossRef]
- Garcia-Hernandez, M.E.; Trujillo-Ortega, M.E.; Alcaraz-Estrada, S.L.; Lozano-Aguirre-Beltran, L.; Sandoval-Jaime, C.; Taboada-Ramirez, B.I.; Sarmiento-Silva, R.E. Molecular detection and characterization of porcine epidemic diarrhea virus and porcine Aichivirus C coinfection in Mexico. Viruses 2021, 13, 738–749. [Google Scholar] [CrossRef]
- Lu, Y.; Huang, W.; Zhong, L.; Qin, Y.; Liu, X.; Yang, C.; Wang, R.; Su, X.; Du, C.; Mi, X.; et al. Comparative characterization and pathogenicity of a novel porcine epidemic diarrhea virus (PEDV) with a naturally occurring truncated ORF3 gene coinfected with PEDVs possessing an intact ORF3 gene in piglets. Viruses 2021, 13, 1562–1576. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, 7647–7671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Chartrand, C.; Leeflang, M.M.G.; Minion, J.; Brewer, T.; Pai, M. Accuracy of rapid influenza diagnostic tests: A meta-analysis. Ann. Intern. Med. 2012, 156, 500–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef]
- Hellmich, M.; Lehmacher, W. A ruler for interpreting diagnostic test results. Methods. Inf. Med. 2005, 44, 124–126. [Google Scholar]
- Leeflang, M.M.G.; Deeks, J.J.; Gatsonis, C.; Bossuyt, P.M.M.; Cochrane Diagnostic Test Accuracy Working Group. Systematic reviews of diagnostic test accuracy. Ann. Intern. Med. 2008, 149, 889–897. [Google Scholar] [CrossRef]
- Zou, S.; Wu, L.; Li, G.; Wang, J.; Cao, D.; Xu, T.; Jia, A.; Tang, Y. Development of an accurate lateral flow immunoassay for PEDV detection in swine fecal samples with a filter pad design. Anim. Dis. 2021, 1, 27–38. [Google Scholar] [CrossRef]
- Wang, H.; Zhao, X.; Yan, R.; Xie, C.; Liu, G.; Ma, Z.; Wang, S.; Fang, D. Establishment of a time-resolved fluorescence immunochromatographic assay for detection of PEDV. Chin. J. Prev. Vet. Med. 2021, 43, 40–45. [Google Scholar]
- Liu, J.; Gao, R.; Shi, H.; Cong, G.; Chen, J.; Zhang, X.; Da, S.; Cao, L.; Wang, X.; Zhang, J.; et al. Development of a rapid immunochromatographic strip test for the detection of porcine epidemic diarrhea virus specific SIgA in colostrum. J. Virol. Methods 2020, 279, 113855–113860. [Google Scholar] [CrossRef]
- Liu, J.; Shi, H.; Cong, G.; Chen, J.; Zhang, X.; Da, S.; Cao, L.; Wang, X.; Zhang, J.; Ji, Z.; et al. Development of a rapid and sensitive europium (III) chelate microparticle-based lateral flow test strip for the detection and epidemiological surveillance of porcine epidemic diarrhea virus. Arch. Virol. 2020, 165, 1049–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, F.; Jin, Z.; Zou, S.; Chen, C.; Song, Q.; Deng, S.; Xiao, W.; Zhang, X.; Jia, A.; Tang, Y. EuNPs-mAb fluorescent probe based immunochromatographic strip for rapid and sensitive detection of porcine epidemic diarrhea virus. Talanta 2020, 214, 120865. [Google Scholar] [CrossRef]
- Zhang, Y.; Huiqin, W.; Mm, P.; Ruiyi, L.; Nanhang, H. Establishment and clinical application detection the antigen of porcine of immunochromatography for epidemic diarrhea virus. Chin. J. Vet. Med. 2020, 56, 19–23. [Google Scholar]
- Bian, H.; Xu, F.; Jia, Y.; Wang, L.; Deng, S.; Jia, A.; Tang, Y. A new immunochromatographic assay for on-site detection of porcine epidemic diarrhea virus based on monoclonal antibodies prepared by using cell surface fluorescence immunosorbent assay. BMC Vet. Res. 2019, 15, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Xu, F.; Bian, H.; Wang, J.; Jia, A.; Tang, Y.; Jia, X. Preparation of monoclonal antibodies against porcine epidemic diarrhea virus and establishment of colloidal gold immunochromatographic assay. Chin. J. Prev. Vet. Med. 2019, 41, 924–928. [Google Scholar]
- Li, R.; Tian, X.; Yu, Y.; Qiao, S.; Wang, Z.; Ma, J. Development of a rapid immunochromatographic assay for detection of antibodies against porcine epidemic diarrhea virus. Pol. J. Vet. Sci. 2018, 21, 139–147. [Google Scholar]
- Lyoo, K.-S.; Yeom, M.; Kim, J.; Kim, D.; Ha, G.; Na, W.; van Le, P.; Song, D. Development of rapid immunochromatographic strip test for the detection of porcine epidemic diarrhoea virus. Vet. Rec. 2017, 181, 596. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.K.; Lim, S.-I.; Cho, I.-S.; Cheong, K.-M.; Lee, E.-J.; Lee, S.-O.; Kim, J.-B.; Kim, J.-H.; Jeong, D.-S.; An, B.-H.; et al. A novel diagnostic approach to detecting porcine epidemic diarrhea virus: The lateral immunochromatography assay. J. Virol. Methods 2015, 225, 4–8. [Google Scholar] [CrossRef]
- Kim, J.-K.; Kim, H.-R.; Kim, D.-Y.; Kim, J.-M.; Kwon, N.-Y.; Park, J.-H.; Park, J.-Y.; Kim, S.-H.; Lee, K.-K.; Lee, C.; et al. A simple colorimetric detection of porcine epidemic diarrhea virus by reverse transcription loop-mediated isothermal amplification assay using hydroxynaphthol blue metal indicator. J. Virol. Methods 2021, 298, 114289–114296. [Google Scholar] [CrossRef]
- El-Tholoth, M.; Bai, H.; Mauk, M.G.; Saif, L.; Bau, H.H. A portable, 3D printed, microfluidic device for multiplexed, real time, molecular detection of the porcine epidemic diarrhea virus, transmissible gastroenteritis virus, and porcine deltacoronavirus at the point of need. Lab. Chip. 2021, 21, 1118–1130. [Google Scholar] [CrossRef]
- Li, G.; Wu, M.; Li, J.; Cai, W.; Xie, Y.; Si, G.; Xiao, L.; Cong, F.; He, D. Rapid detection of porcine deltacoronavirus and porcine epidemic diarrhea virus using the duplex recombinase polymerase amplification method. J. Virol. Methods 2021, 292, 114096–114103. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Liang, Y.; Li, Y.; Liu, Q.; Zhang, W.; Yin, D.; Song, X.; Shao, Y.; Tu, J.; Qi, K. Reverse transcription-enzymatic recombinase amplification coupled with CRISPR-Cas12a for rapid detection and differentiation of PEDV wild-type strains and attenuated vaccine strains. Anal. Bioanal. Chem. 2021, 413, 7521–7529. [Google Scholar] [CrossRef] [PubMed]
- Di, Y.; Tan, F.; Qin, S.; Yu, X.; Cui, W.; Jiang, Y.; Wang, L.; Tang, L.; Zhou, H.; Wang, X.; et al. Establishment and application of RT-LAMP rapid detection assay for porcine epidemic diarrhea virus. Chin. J. Prev. Vet. Med. 2021, 43, 832–837. [Google Scholar]
- Wang, Z.; Li, X.; Shang, Y.; Wu, J.; Dong, Z.; Cao, X.; Liu, Y.; Lan, X. Rapid differentiation of PEDV wild-type strains and classical attenuated vaccine strains by fluorescent probe-based reverse transcription recombinase polymerase amplification assay. BMC Vet. Res. 2020, 16, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Chen, Y.; Fang, X.; Liu, Y.; Du, M.; Lu, X.; Li, Q.; Sun, Y.; Ma, J.; Lan, T. Microfluidic-RT-LAMP chip for the point-of-care detection of emerging and re-emerging enteric coronaviruses in swine. Anal. Chim. Acta. 2020, 1125, 57–65. [Google Scholar] [CrossRef]
- Wang, X.; Xu, X.; Hu, W.; Zuo, K.; Li, Z.; Kan, Y.; Yao, L.; Ji, J.; Bi, Y. Visual detection of porcine epidemic diarrhea virus using a novel reverse transcription polymerase spiral reaction method. BMC Vet. Res. 2019, 15, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Mai, T.N.; van Nguyen, D.; Yamazaki, W.; Okabayashi, T.; Mitoma, S.; Notsu, K.; Sakai, Y.; Yamaguchi, R.; Norimine, J.; Sekiguchi, S. Development of pooled testing system for porcine epidemic diarrhoea using real-time fluorescent reverse-transcription loop-mediated isothermal amplification assay. BMC Vet. Res. 2018, 14, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhang, R.; Wang, J.; Han, Q.; Liu, L.; Li, Y.; Yuan, W. Real-time reverse transcription recombinase polymerase amplification assay for rapid detection of porcine epidemic diarrhea virus. J. Virol. Methods 2018, 253, 49–52. [Google Scholar] [CrossRef]
- Wang, F.-X.; Yuan, D.-Y.; Jin, Y.-N.; Hu, L.; Sun, Z.-Y.; He, Q.; Zhao, S.-H.; Zhan, S.-B.; Wen, Y.-J. Reverse transcription cross-priming amplification-nucleic acid test strip for papid detection of porcine epidemic diarrhea virus. Sci. Rep. 2016, 6, 24702–24708. [Google Scholar] [CrossRef] [Green Version]
- Gou, H.; Deng, J.; Wang, J.; Pei, J.; Liu, W.; Zhao, M.; Chen, J. Rapid and sensitive detection of porcine epidemic diarrhea virus by reverse transcription loop-mediated isothermal amplification combined with a vertical flow visualization strip. Mol. Cell. Probes. 2015, 29, 48–53. [Google Scholar] [CrossRef]
- Yu, X.; Shi, L.; Lv, X.; Yao, W.; Cao, M.; Yu, H.; Wang, X.; Zheng, S. Development of a real-time reverse transcription loop-mediated isothermal amplification method for the rapid detection of porcine epidemic diarrhea virus. Virol. J. 2015, 12, 76–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Nardo, F.A.-O.; Chiarello, M.A.-O.; Cavalera, S.A.-O.X.; Baggiani, C.A.-O.; Anfossi, L.A.-O. Ten years of lateral flow immunoassay technique applications: Trends, challenges and future perspectives. Sensors 2021, 21, 5185–5217. [Google Scholar] [CrossRef]
- Munafò, M.R.; Flint, J. Meta-analysis of genetic association studies. Trends. Genet. 2004, 20, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol. 2006, 6, 31. [Google Scholar] [CrossRef] [PubMed]
- Moses, L.E.; Shapiro, D.; Littenberg, B. Combining independent studies of a diagnostic test into a summary ROC curve: Data-analytic approaches and some additional considerations. Stat. Med. 1993, 12, 1293–1316. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Saif, L.J.; Wang, Q. Porcine epidemic diarrhea virus (PEDV): An update on etiology, transmission, pathogenesis, and prevention and control. Virus. Res. 2020, 286, 198045–198096. [Google Scholar] [CrossRef]
- Niederwerder, M.C.; Nietfeld, J.C.; Bai, J.; Peddireddi, L.; Breazeale, B.; Anderson, J.; Kerrigan, M.A.; An, B.; Oberst, R.D.; Crawford, K.; et al. Tissue localization, shedding, virus carriage, antibody response, and aerosol transmission of Porcine epidemic diarrhea virus following inoculation of 4-week-old feeder pigs. J. Vet. Diagn. Investig. 2016, 28, 671–678. [Google Scholar] [CrossRef] [Green Version]
- Yuan, W.; Li, Y.; Li, P.; Song, Q.; Li, L.; Sun, J. Development of a nanoparticle-assisted PCR assay for detection of porcine epidemic diarrhea virus. J. Virol. Methods 2015, 220, 18–20. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, Y.; Byrum, B. Development and evaluation of a duplex real-time RT-PCR for detection and differentiation of virulent and variant strains of porcine epidemic diarrhea viruses from the United States. J. Virol. Methods 2014, 207, 154–157. [Google Scholar] [CrossRef]
- Zhao, P.-D.; Bai, J.; Jiang, P.; Tang, T.-S.; Li, Y.; Tan, C.; Shi, X. Development of a multiplex TaqMan probe-based real-time PCR for discrimination of variant and classical porcine epidemic diarrhea virus. J. Virol. Methods 2014, 206, 150–155. [Google Scholar] [CrossRef]
- Liu, F.X.; Cui, J.Q.; Park, H.; Chan, K.W.; Leung, T.; Tang, B.Z.; Yao, S. Isothermal background-free nucleic acid quantification by a one-pot Cas13a assay using droplet microfluidics. Anal. Chem. 2022, 94, 5883–5892. [Google Scholar] [CrossRef] [PubMed]
- Sekhon, S.S.; Nguyen, P.-L.; Ahn, J.-Y.; Lee, K.-A.; Lee, L.; Kim, S.Y.; Yoon, H.; Park, J.; Ko, J.H.; Kim, Y.-H. Porcine epidemic diarrhea (PED) infection, diagnosis and vaccination: A mini review. Toxicol. Environ. Health. Sci. 2016, 8, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Naveen, K.P.; Bhat, A.I. Reverse transcriptase loop-mediated isothermal amplification and reverse transcriptase recombinase amplification assays for rapid and sensitive detection of cardamom vein clearing virus. 3 Biotech 2020, 10, 250. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (First Author, Year) | Country | Sample Type | Sample Size | Reference Standard | TP | FP | FN | TN |
|---|---|---|---|---|---|---|---|---|
| ICA-based POCTs | ||||||||
| Zou, 2021 [18] | China | feces | 108 | RT-PCR | 62 | 0 | 8 | 38 |
| Wang, 2021 [19] | China | rectal swab | 160 | real-time RT-PCR | 71 | 5 | 10 | 74 |
| Liu, 2020a [20] | China | colostrum | 63 | ELISA | 51 | 4 | 2 | 6 |
| Liu, 2020b [21] | China | rectal swab | 923 | RT-PCR | 63 | 2 | 0 | 858 |
| Xu, 2020 [22] | China | feces | 60 | RT-PCR | 33 | 5 | 3 | 19 |
| Zhang, 2020 [23] | China | feces | 80 | RT-PCR | 36 | 0 | 2 | 42 |
| Bian, 2019 [24] | China | feces | 27 | RT-PCR | 20 | 3 | 2 | 2 |
| Jia, 2019 [25] | China | feces | 115 | RT-PCR | 62 | 2 | 0 | 51 |
| Li, 2018 [26] | China | serum | 201 | ELISA | 120 | 7 | 5 | 69 |
| Lyoo, 2017 [27] | Korea | rectal swab | 130 | real-time RT-PCR | 57 | 1 | 3 | 69 |
| Kim, 2015 [28] | Korea | feces | 493 | real-time RT-PCR | 218 | 4 | 9 | 262 |
| NAIA-based POCTs | ||||||||
| Kim, 2021 [29] | Korea | feces and intestine | 149 | real-time RT-PCR | 95 | 4 | 2 | 48 |
| El-Tholoth, 2021 [30] | Egypt | rectal swabs | 11 | real-time RT-PCR | 5 | 0 | 0 | 6 |
| Li, 2021 [31] | China | feces and intestine | 45 | real-time RT-PCR | 13 | 0 | 0 | 32 |
| Yang, 2021 [32] | China | feces and intestine | 15 | real-time RT-PCR | 5 | 0 | 0 | 10 |
| Di, 2021 [33] | China | feces and lymph nodes | 60 | RT-PCR | 12 | 3 | 0 | 45 |
| Wang, 2020 [34] | China | not stated | 80 | real-time RT-PCR | 71 | 0 | 1 | 8 |
| Zhou, 2020 [35] | China | feces and intestine | 173 | real-time RT-PCR | 80 | 0 | 4 | 89 |
| Wang, 2019 [36] | China | not stated | 65 | RT-PCR | 35 | 3 | 0 | 27 |
| Mai, 2018 [37] | Japan | feces | 99 | RT-PCR | 50 | 0 | 0 | 49 |
| Wang, 2018 [38] | China | intestine | 76 | real-time RT-PCR | 42 | 0 | 3 | 31 |
| Wang, 2016 [39] | China | feces | 41 | RT-PCR | 6 | 4 | 1 | 30 |
| Gou, 2015 [40] | China | not stated | 20 | RT-PCR | 14 | 0 | 0 | 6 |
| Yu, 2015 [41] | China | feces and intestine | 52 | real-time RT-PCR | 27 | 4 | 3 | 18 |
| Sensitivity (95% CI) | Specificity (95% CI) | PLR (95% CI) | NLR (95% CI) | DOR (95% CI) | AUC (95% CI) | |
|---|---|---|---|---|---|---|
| ICA-based POCTs | 0.95 | 0.96 | 24.5 | 0.05 | 480 | 0.98 |
| (0.92–0.97) | (0.88–0.99) | (7.4–81.0) | (0.03–0.08) | (111–2074) | (0.96–0.99) | |
| NAIA-based POCTs | 0.97 | 0.98 | 42.4 | 0.03 | 1517 | 0.99 |
| (0.94–0.99) | (0.91–0.99) | (10.9–164.9) | (0.01–0.06) | (290–7943) | (0.98–1.00) |
| Parameter | Category | No. of Studies | Sensitivity | Specificity | LRT Chi-Square | P (Joint Model) | ||
|---|---|---|---|---|---|---|---|---|
| Pooled Value (95% CI) | p1 | Pooled Value (95% CI) | p2 | |||||
| ICA-based POCTs | ||||||||
| Sample type | Feces | 6 | 0.95 (0.91–0.98) | 0.00 | 0.96 (0.90–1.00) | 0.56 | 0.21 | 0.90 |
| Other a | 5 | 0.96 (0.92–0.99) | 0.96 (0.90–1.00) | |||||
| Sample size | ≥100 | 7 | 0.96 (0.93–0.98) | 0.05 | 0.98 (0.96–1.00) | 0.02 | 5.12 | 0.08 |
| <100 | 4 | 0.94 (0.89–0.99) | 0.82 (0.60–1.00) | |||||
| Reference standard | ELISA | 2 | 0.96 (0.92–1.00) | 0.19 | 0.81 (0.46–1.00) | 0.21 | 3.95 | 0.14 |
| Other b | 9 | 0.94 (0.92–0.97) | 0.97 (0.94–1.00) | |||||
| NAIA-based POCTs | ||||||||
| Sample type | Feces | 8 | 0.97 (0.94–0.99) | 0.10 | 0.97 (0.93–1.00) | 0.44 | 0.59 | 0.74 |
| Other c | 5 | 0.98 (0.95–1.00) | 0.98 (0.94–1.00) | |||||
| Sample size | ≥100 | 2 | 0.97 (0.93–1.00) | 0.18 | 0.98 (0.94–1.00) | 0.13 | 0.18 | 0.91 |
| <100 | 11 | 0.98 (0.95–1.00) | 0.97 (0.93–1.00) | |||||
| Reference standard | Real-time RT-PCR | 8 | 0.96 (0.94–0.99) | 0.26 | 0.98 (0.96–1.00) | 0.07 | 3.85 | 0.15 |
| RT-PCR | 5 | 0.99 (0.97–1.00) | 0.96 (0.90–1.00) | |||||
| Assaytype | RT-LAMP | 7 | 0.97 (0.95–1.00) | 0.19 | 0.98 (0.94–1.00) | 0.42 | 0.02 | 0.99 |
| RT-RPA | 6 | 0.97 (0.95–1.00) | 0.98 (0.94–1.00) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, R.; Tian, X.; Pang, J.; Li, L.; Yuan, J.; Tian, Z.; Wang, Z. Point-of-Care Tests for Rapid Detection of Porcine Epidemic Diarrhea Virus: A Systematic Review and Meta-Analysis. Viruses 2022, 14, 1355. https://doi.org/10.3390/v14071355
Li R, Tian X, Pang J, Li L, Yuan J, Tian Z, Wang Z. Point-of-Care Tests for Rapid Detection of Porcine Epidemic Diarrhea Virus: A Systematic Review and Meta-Analysis. Viruses. 2022; 14(7):1355. https://doi.org/10.3390/v14071355
Chicago/Turabian StyleLi, Renfeng, Xiangqin Tian, Junzeng Pang, Linyue Li, Jiakang Yuan, Zhuangzhuang Tian, and Ziliang Wang. 2022. "Point-of-Care Tests for Rapid Detection of Porcine Epidemic Diarrhea Virus: A Systematic Review and Meta-Analysis" Viruses 14, no. 7: 1355. https://doi.org/10.3390/v14071355