
Evaluation of Screening Program and Phylogenetic Analysis of SARS-CoV-2 Infections among Hospital Healthcare Workers in Liège, Belgium

 , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Laboratory Assays
2.2. SARS-CoV-2 Sequencing and Phylogenetic Analysis
2.3. Statistical Analysis
3. Results
3.1. Characteristics of HCW Groups
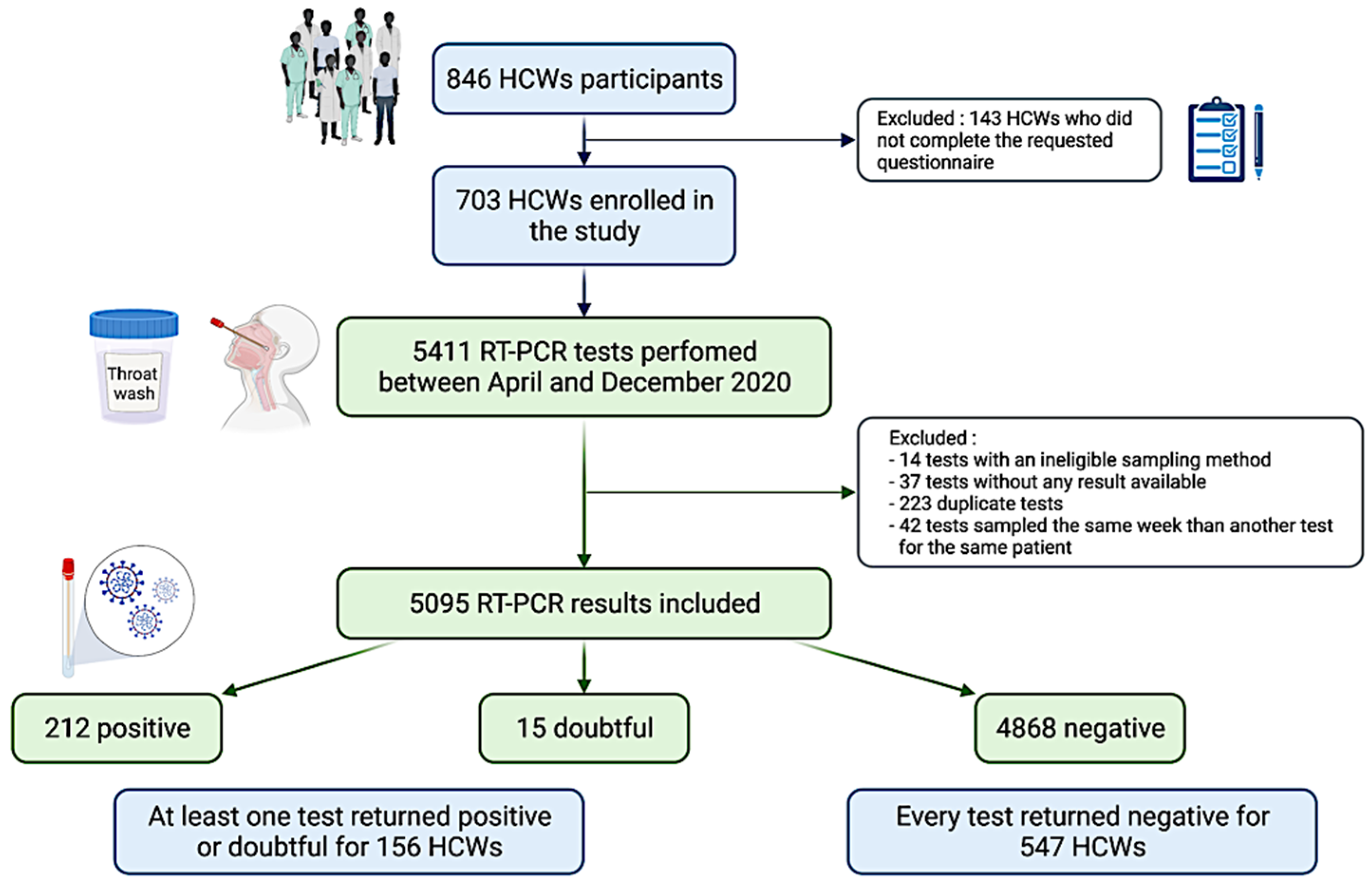
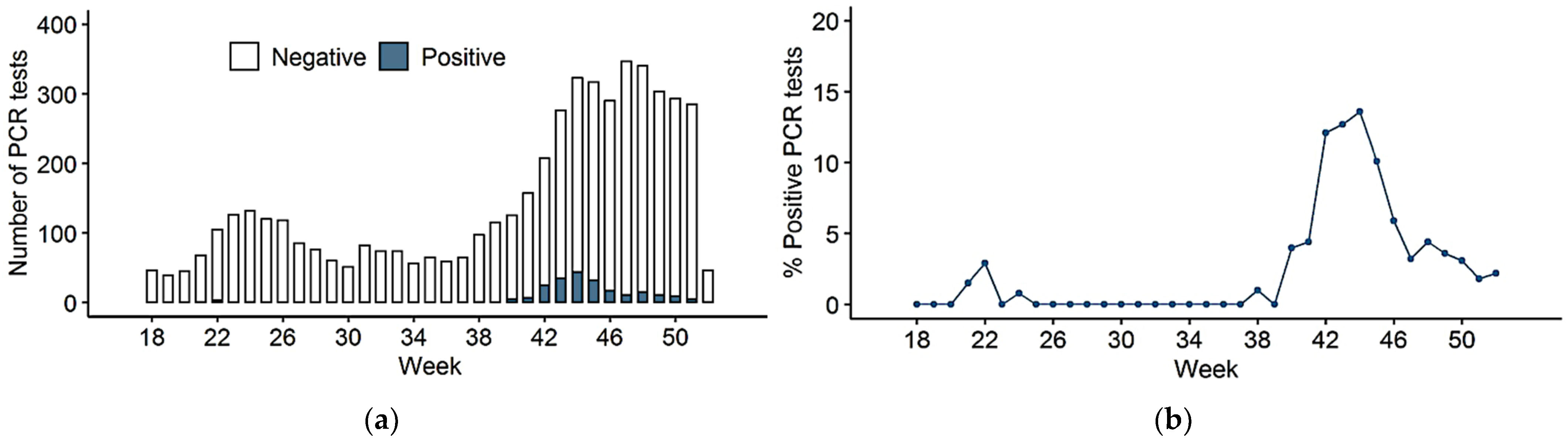
3.2. SARS-CoV-2 PCR Testing
3.3. Association of HCWs Role with SARS-CoV-2 Infection
3.4. Viral Sequencing and Phylogenetic Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lipsitch, M.; Swerdlow, D.L.; Finelli, L. Defining the epidemiology of COVID-19—Studies needed. N. Engl. J. Med. 2020, 382, 1194–1196. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Surveillance Frequently Asked Questions. Sciensano. Available online: https://covid19.sciensano.be/sites/default/files/Covid19/COVID-19_FAQ_ENG_final.pdf (accessed on 20 December 2021).
- Meurisse, M.; Lajot, A.; Dupont, Y.; Lesenfants, M.; Klamer, S.; Rebolledo, J.; Lernout, T.; Leroy, M.; Capron, A.; Van Bussel, J.; et al. One year of laboratory-based COVID-19 surveillance system in Belgium: Main indicators and performance of the laboratories. Arch. Belg. Public Health 2021, 79, 188. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 20, 1401–1408. [Google Scholar] [CrossRef]
- Li, R.; Xuyu, C.; Ying, W.; Wenwen, W.; Ling, Z.; Xiaodong, T. Risk Factors of Healthcare Workers with Coronavirus Disease 2019: A Retrospective Cohort Study in a Designated Hospital of Wuhan in China. Clin. Infect. Dis. 2020, 71, 2218–2221. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Joshi, A.D.; Guo, G.G.; Ma, W.; Mehta, R.S. Risk of COVID-19 among frontline healthcare workers and the general community: A prospective cohort study. Epidemiology 2020, 6, 20084111. [Google Scholar] [CrossRef]
- Lombardi, A.; Consonni, D.; Carugno, M.; Bozzi, G.; Mangioni, D.; Muscatello, A.; Castelli, V.; Palomba, E.; Cantù, A.P.; Ceriotti, F.; et al. Characteristics of 1573 healthcare workers who underwent nasopharyngeal swab testing for SARS-CoV-2 in Milan, 2020, Lombardy, Italy. Clin. Microbiol. Infect. 2020, 26, 1413.e9–1413.e13. [Google Scholar] [CrossRef]
- Mo, Y.; Eyre, D.W.; Lumley, S.F.; Walker, T.M.; Shaw, R.H.; O’Donnell, D.; Butcher, L.; Jeffery, K.; Donnelly, C.A.; Oxford COVID Infection Review Team; et al. Transmission of community- and hospital-acquired SARS-CoV-2 in hospital settings in the UK: A cohort study. PLoS Med. 2021, 18, e1003816. [Google Scholar] [CrossRef]
- Keeley, A.J.; Evans, C.; Colton, H.; Ankcorn, M.; Cope, A.; State, A.; Bennett, T.; Giri, P.; de Silva, T.I.; Raza, M. Roll-out of SARS-CoV-2 testing for healthcare workers at a large NHS Foundation Trust in the United Kingdom. Euro Surveill. Bull. Eur. Mal. Transm. 2020, 25, 2000433. [Google Scholar] [CrossRef]
- Lee, N.; Sung, J.J. Nosocomial Transmission of SARS. Curr. Infect. Dis. Rep. 2003, 5, 473–476. [Google Scholar] [CrossRef]
- Sikkema, R.S.; Pas, S.D.; Nieuwenhuijse, D.F.; O’Toole, Á.; Verweij, J.; Van der Linden, A.; Chestakova, I.; Schapendonk, C.; Pronk, M.; Lexmond, P.; et al. COVID-19 in health-care workers in three hospitals in the south of the Netherlands: A cross-sectional study. Lancet Infect. Dis. 2020, 20, 1273–1280. [Google Scholar] [CrossRef]
- Abbas, M.; Robalo Nunes, T.; Martischang, R.; Zingg, W.; Iten, A.; Pittet, D.; Harbarth, S. Nosocomial transmission and outbreaks of coronavirus disease 2019: The need to protect both patients and healthcare workers. Antimicrob. Resist. Infect. Control 2021, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Hunter, E.; Price, D.A.; Murphy, E.; Van der Loeff, I.S.; Baker, K.F.; Lendrem, D.; Lendrem, C.; Schmid, M.L.; Pareja-Cebrian, L.; Welch, A.; et al. Experience of COVID-19 screening of health-care workers in England. Lancet 2020, 395, e77–e78. [Google Scholar] [CrossRef]
- Ellingford, J.M.; George, R.; McDermott, J.H.; Ahmad, S.; Edgerley, J.J.; Gokhale, D.; Newman, W.G.; Ball, S.; Machin, N.; Black, G.C. Genomic and healthcare dynamics of nosocomial SARS-CoV-2 transmission. eLife 2021, 10, e65453. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Agnew, E.; Vynnycky, E.; Stimson, J.; Bhattacharya, A.; Rooney, C.; Warne, B.; Robotham, J. The impact of testing and infection prevention and control strategies on within-hospital transmission dynamics of COVID-19 in English hospitals. Philos. Trans. R. Soc. Lond. 2021, 376, 20200268. [Google Scholar] [CrossRef] [PubMed]
- Hanrath, A.T.; Schim van der Loeff, I.; Lendrem, D.W.; Baker, K.F.; Price, D.A.; McDowall, P.; McDowall, K.; Cook, S.; Towns, P.; Schwab, U.; et al. SARS-CoV-2 Testing of 11,884 Healthcare Workers at an Acute NHS Hospital Trust in England: A Retrospective Analysis. Front. Med. 2021, 8, 636160. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Lago, L.; Martínez-Lozano, H.; Pajares-Díaz, J.A.; Díaz-Gómez, A.; Machado, M.; Sola-Campoy, P.J.; Herranz, M.; Valerio, M.; Olmedo, M.; Suárez-González, J.; et al. Overlapping of Independent SARS-CoV-2 Nosocomial Transmissions in a Complex Outbreak. mSphere 2021, 6, e0038921. [Google Scholar] [CrossRef]
- Braun, K.M.; Moreno, G.K.; Buys, A.; Somsen, E.D.; Bobholz, M.; Accola, M.A.; Anderson, L.; Rehrauer, W.M.; Baker, D.A.; Safdar, N.; et al. Viral sequencing reveals US healthcare personnel rarely become infected with SARS-CoV-2 through patient contact. Clin. Infect. Dis. 2021, 73, e1329–e1336. [Google Scholar] [CrossRef]
- Lenggenhager, L.; Martischang, R.; Sauser, J.; Perez, M.; Vieux, L.; Graf, C.; Cordey, S.; Laubscher, F.; Nunes, T.R.; Zingg, W.; et al. Occupational and community risk of SARS-CoV-2 infection among employees of a long-term care facility: An observational study. Antimicrob. Resist. Infect. Control 2022, 11, 51. [Google Scholar] [CrossRef]
- Sikkens, J.J.; Buis, D.T.P.; Peters, E.; Dekker, M.; Schinkel, M.; Reijnders, T.; Schuurman, A.R.; de Brabander, J.; Lavell, A.; Maas, J.J.; et al. Serologic Surveillance and Phylogenetic Analysis of SARS-CoV-2 Infection Among Hospital Health Care Workers. JAMA Netw. Open 2021, 4, e2118554. [Google Scholar] [CrossRef]
- Leducq, V.; Jary, A.; Bridier-Nahmias, A.; Daniel, L.; Zafilaza, K.; Damond, F.; Goldstein, V.; Duval, A.; Blanquart, F.; Calvez, V.; et al. Nosocomial transmission clusters and lineage diversity characterized by SARS-CoV-2 genomes from two large hospitals in Paris, France, in 2020. Sci. Rep. 2022, 12, 1094. [Google Scholar] [CrossRef]
- Lucey, M.; Macori, G.; Mullane, N.; Sutton-Fitzpatrick, U.; Gonzalez, G.; Coughlan, S.; Purcell, A.; Fenelon, L.; Fanning, S.; Schaffer, K. Whole-genome Sequencing to Track Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Transmission in Nosocomial Outbreaks. Clin. Infect. Dis. 2021, 72, e727–e735. [Google Scholar] [CrossRef] [PubMed]
- Francis, R.V.; Billam, H.; Clarke, M.; Yates, C.; Tsoleridis, T.; Berry, L.; Mahida, N.; Irving, W.L.; Moore, C.; Holmes, N.; et al. The Impact of Real-Time Whole-Genome Sequencing in Controlling Healthcare-Associated SARS-CoV-2 Outbreaks. J. Infect. Dis. 2022, 225, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Borges, V.; Isidro, J.; Macedo, F.; Neves, J.; Silva, L.; Paiva, M.; Barata, J.; Catarino, J.; Ciobanu, L.; Duarte, S.; et al. Nosocomial Outbreak of SARS-CoV-2 in a “Non-COVID-19” Hospital Ward: Virus Genome Sequencing as a Key Tool to Understand Cryptic Transmission. Viruses 2021, 13, 604. [Google Scholar] [CrossRef] [PubMed]
- MacCannell, T.; Batson, J.; Bonin, B.; Astha, K.C.; Quenelle, R.; Strong, B.; Lin, W.; Rudman, S.L.; Dynerman, D.; Ayscue, P.; et al. Genomic Epidemiology and Transmission Dynamics of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Congregate Healthcare Facilities in Santa Clara County, California. Clin. Infect. Dis. 2022, 74, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Meredith, L.W.; Hamilton, W.L.; Warne, B.; Houldcroft, C.J.; Hosmillo, M.; Jahun, A.S.; Curran, M.D.; Parmar, S.; Caller, L.G.; Caddy, S.L.; et al. Rapid implementation of SARSCoV-2 sequencing to investigate cases of health-care associated COVID-19: A prospective genomic surveillance study. Lancet Infect. Dis. 2020, 20, 1263–1271. [Google Scholar] [CrossRef]
- Korth, J.; Wilde, B.; Dolff, S.; Frisch, J.; Jahn, M.; Krawczyk, A.; Trilling, M.; Schipper, L.; Cordes, S.; Ross, B.; et al. SARS-CoV-2 Seroprevalence in Healthcare Workers in Germany: A Follow-Up Study. Int. J. Environ. Res. Public Health 2021, 18, 4540. [Google Scholar] [CrossRef]
- Jacob, J.T.; Baker, J.M.; Fridkin, S.K.; Lopman, B.A.; Steinberg, J.P.; Christenson, R.H.; King, B.; Leekha, S.; O’Hara, L.M.; Rock, P.; et al. Risk Factors Associated With SARS-CoV-2 Seropositivity Among US Health Care Personnel. JAMA Netw. Open 2021, 4, e211283. [Google Scholar] [CrossRef]
- Nygren, D.; Norén, J.; De Marinis, Y.; Holmberg, A.; Fraenkel, C.J.; Rasmussen, M. Association between SARS-CoV-2 and exposure risks in health care workers and university employees—A cross-sectional study. Infect. Dis. 2021, 53, 460–468. [Google Scholar] [CrossRef]
- Wilkins, J.T.; Gray, E.L.; Wallia, A.; Hirschhorn, L.R.; Zembower, T.R.; Ho, J.; Kalume, N.; Agbo, O.; Zhu, A.; Rasmussen-Torvik, L.J.; et al. Seroprevalence and Correlates of SARS-CoV-2 Antibodies in Health Care Workers in Chicago. Open Forum Infect. Dis. 2020, 8, ofaa582. [Google Scholar] [CrossRef]
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shang, K.; Xia, C.; Wang, S.; et al. Coronavirus Disease 2019 (COVID-2019) Infection Among Health Care Workers and Implications for Prevention Measures in a Tertiary Hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef]
- Eyre, D.W.; Lumley, S.F.; O’Donnell, D.; Campbell, M.; Sims, E.; Lawson, E.; Warren, F.; James, T.; Cox, S.; Howarth, A.; et al. Differential occupational risks to healthcare workers from SARS-CoV-2 observed during a prospective observational study. eLife 2020, 9, e60675. [Google Scholar] [CrossRef] [PubMed]
- Kahlert, C.R.; Persi, R.; Güsewell, S.; Egger, T.; Leal-Neto, O.B.; Sumer, J.; Flury, D.; Brucher, A.; Lemmenmeier, E.; Möller, J.C.; et al. Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers—A multicentre cross-sectional study. Clin. Microbiol. Infect. 2020, 27, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- Rudberg, A.S.; Havervall, S.; Månberg, A.; Jernbom Falk, A.; Aguilera, K.; Ng, H.; Gabrielsson, L.; Salomonsson, A.C.; Hanke, L.; Murrell, B.; et al. SARS-CoV-2 exposure, symptoms and seroprevalence in healthcare workers in Sweden. Nat. Commun. 2020, 11, 5064. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systemat-ic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef]
- Steensels, D.; Oris, E.; Coninx, L.; Nuyens, D.; Delforge, M.L.; Vermeersch, P.; Heylen, L. Hospital-Wide SARS-CoV-2 Antibody Screening in 3056 Staff in a Tertiary Center in Belgium. JAMA 2020, 324, 195–197. [Google Scholar] [CrossRef]
- Jafari, Y.; Yin, M.; Lim, C.; Pople, D.; Evans, S.; Stimson, J.; Pham, T.M.; LSHTM CMMID COVID-19 Working Group; Read, J.M.; Robotham, J.V.; et al. Effectiveness of infection prevention and control interventions, excluding personal protective equipment, to prevent nosocomial transmission of SARS-CoV-2: A systematic review and call for action. Infect. Prev. Pract. 2021, 4, 100192. [Google Scholar] [CrossRef]
- COVID-19: Occupational Health and Safety for Health Workers, Interim Guidance. 2 February 2021. Available online: https://hlh.who.int/docs/librariesprovider4/hlh-documents/covid-19---occupational-health-and-safety-for-health-workers.pdf?sfvrsn=581e60c6_5 (accessed on 20 December 2021).
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife 2020, 9, e58728. [Google Scholar] [CrossRef]
- Kasper, M.R.; Geibe, J.R.; Sears, C.L.; Riegodedios, A.J.; Luse, T.; von Thun, A.M.; McGinnis, M.B.; Olson, N.; Houskamp, D.; Fenequito, R.; et al. An Outbreak of Covid-19 on an Aircraft Carrier. N. Engl. J. Med. 2020, 383, 2417–2426. [Google Scholar] [CrossRef]
- Defêche, J.; Azarzar, S.; Mesdagh, A.; Dellot, P.; Tytgat, A.; Bureau, F.; Gillet, L.; Belhadj, Y.; Bontems, S.; Hayette, M.P.; et al. In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2. Pathogens 2021, 10, 1362. [Google Scholar] [CrossRef]
- Huynen, P.; Grégoire, C.; Gofflot, S.; Seidel, L.; Maes, N.; Vranken, L.; Delcour, S.; Moutschen, M.; Hayette, M.P.; Kolh, P.; et al. Long-term longitudinal evaluation of the prevalence of SARS-CoV-2 antibodies in healthcare and university workers. Sci. Rep. 2022, 12, 5156. [Google Scholar] [CrossRef]
- Freed, N.E.; Vlková, M.; Faisal, M.B.; Silander, O.K. Rapid and inexpensive whole-genome sequencing of SARS-CoV-2 using 1200 bp tiled amplicons and Oxford Nanopore Rapid Barcoding. Biol. Methods Protoc. 2020, 5, bpaa014. [Google Scholar] [CrossRef] [PubMed]
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, R.A. Next strain: Real-time tracking of pathogen evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [CrossRef] [PubMed]
- Minh, B.Q.; Schmidt, H.A.; Chernomor, O.; Schrempf, D.; Woodhams, M.D.; von Haeseler, A.; Lanfear, R. IQ-TREE 2: New Models and Efficient Methods for Phylogenetic Inference in the Genomic Era. Mol. Biol. Evol. 2020, 37, 1530–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavaré, S. Some probabilistic and statistical problems in the analysis of DNA sequences. In Lectures on Mathematics in the Life Sciences; The American Mathematical Society: Providence, RI, USA, 1986; Volume 17, pp. 57–86. [Google Scholar]
- Yang, Z. A space-time process model for the evolution of DNA sequences. Genetics 1995, 139, 993–1005. [Google Scholar] [CrossRef] [PubMed]
- Sagulenko, P.; Puller, V.; Neher, R.A. TreeTime: Maximum-likelihood phylodynamic analysis. Virus Evol. 2018, 4, vex042. [Google Scholar] [CrossRef] [PubMed]
- Dellicour, S.; Durkin, K.; Hong, S.L.; Vanmechelen, B.; Martí-Carreras, J.; Gill, M.S. A Phylodynamic Workflow to Rapidly Gain Insights into the Dispersal History and Dynamics of SARS-CoV-2 Lineages. Mol. Biol. Evol. 2021, 38, 1608–1613. [Google Scholar] [CrossRef] [PubMed]
- Bollen, N.; Artesi, M.; Durkin, K.; Hong, S.L.; Potter, B.; Boujemla, B.; Vanmechelen, B.; Martí-Carreras, J.; Wawina-Bokalanga, T.; Meex, C.; et al. Exploiting genomic surveillance to map the spatio-temporal dispersal of SARS-CoV-2 spike mutations in Belgium across 2020. Sci. Rep. 2021, 11, 18580. [Google Scholar] [CrossRef] [PubMed]
- Lemey, P.; Rambaut, A.; Drummond, A.J.; Suchard, M.A. Bayesian phylogeography finds its roots. PLoS Comput. Biol. 2009, 5, e1000520. [Google Scholar] [CrossRef] [Green Version]
- Suchard, M.A.; Lemey, P.; Baele, G.; Ayres, D.L.; Drummond, A.J.; Rambaut, A. Bayesian phylogenetic and phylodynamic data integration using BEAST 1.10. Virus Evol. 2018, 4, vey016. [Google Scholar] [CrossRef] [Green Version]
- Rambaut, A.; Drummond, A.J.; Xie, D.; Baele, G.; Suchard, M.A. Posterior Summarization in Bayesian Phylogenetics Using Tracer 1.7. Syst. Biol. 2018, 67, 901–904. [Google Scholar] [CrossRef] [Green Version]
- Biorender. Available online: https://app.biorender.com/ (accessed on 23 February 2022).
- Martischang, R.; Iten, A.; Arm, I.; Abbas, M.; Meyer, B.; Yerly, S.; Eckerle, I.; Pralong, J.; Sauser, J.; Suard, J.C.; et al. Severe acute respiratory coronavirus virus 2 (SARS-CoV-2) seroconversion and occupational exposure of employees at a Swiss university hospital: A large longitudinal cohort study. Infect. Control Hosp. Epidemiol. 2021, 43, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.M.; Nelson, K.N.; Overton, E.; Lopman, B.A.; Lash, T.L.; Photakis, M.; Jacob, J.T.; Roback, J.; Fridkin, S.K.; Steinberg, J.P. Quantification of occupational and community risk factors for SARS-CoV-2 seropositivity among healthcare workers in a large U.S. healthcare system. Preprint. medRxiv 2020, 2020, 20222877. [Google Scholar] [CrossRef]
- Modenese, A.; Casolari, L.; Rossi, G.; Della Vecchia, E.; Glieca, F.; D’Elia, C.; Garavini, D.; Righi, E.; Mariani, S.; Venturelli, L.; et al. Factors Associated with SARS-CoV-2 Infection Risk among Healthcare Workers of an Italian University Hospital. Healthcare 2021, 9, 1495. [Google Scholar] [CrossRef] [PubMed]
- McEllistrem, M.C.; Clancy, C.J.; Buehrle, D.J.; Singh, N.; Lucas, A.; Sirianni, V.; Decker, B.K. SARS-CoV-2 is associated with high viral loads in asymptomatic and recently symptomatic healthcare workers. PLoS ONE 2021, 16, e0248347. [Google Scholar] [CrossRef]
- Paltansing, S.; Sikkema, R.S.; De Man, S.J.; Koopmans, M.; Oude Munnink, B.B.; De Man, P. Transmission of SARS-CoV-2 among healthcare workers and patients in a teaching hospital in the Netherlands confirmed by whole-genome sequencing. J. Hosp. Infect. 2021, 110, 178–183. [Google Scholar] [CrossRef]
- He, X.; Lau, E.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Schwartz, N.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Public Health–Seattle and King County, EvergreenHealth, and CDC COVID-19 Investigation Team. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef]
- Migisha, R.; Ario, A.R.; Kwesiga, B.; Bulage, L.; Kadobera, D.; Kabwama, S.N.; Katana, E.; Ndyabakira, A.; Wadunde, I.; Byaruhanga, A.; et al. Risk perception and psychological state of healthcare workers in referral hospitals during the early phase of the COVID-19 pandemic, Uganda. BMC Psychol. 2021, 9, 195. [Google Scholar] [CrossRef]
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.; Sham, P.C.; Chua, S.E.; Wong, J.G. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Canadian journal of psychiatry. Rev. Can. Psychiatr. 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Jones, N.K.; Rivett, L.; Sparkes, D.; Forrest, S.; Sridhar, S.; Young, J.; Pereira-Dias, J.; Cormie, C.; Gill, H.; Reynolds, N.; et al. Effective control of SARS-CoV-2 transmission between healthcare workers during a period of diminished community prevalence of COVID-19. eLife 2020, 9, e59391. [Google Scholar] [CrossRef]
- Grassly, N.C.; Pons-Salort, M.; Parker, E.P.K. Role of Testing in COVID-19 Control. London, United Kingdom: Imperial College. 2020. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2020-04-23-COVID19-Report-16.pdf (accessed on 20 December 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Data Available (n = 703) | Results 1 |
|---|---|---|
| Demographics | ||
| Age (years) | 703 | 41.4 ± 11.3 |
| Female Gender | 703 | 560 (79.7) |
| Height (cm) | 661 | 168 ± 9 |
| Weight (kg) | 659 | 68.7 ± 13.5 |
| BMI (kg/m2) | 659 | 24.3 ± 4.2 |
| Smokers | 661 | 75 (11.3) |
| Comorbidities | ||
| Diabetes mellitus | 661 | 25 (3.8) |
| Hypertension | 661 | 48 (7.3) |
| Heart failure/coronary artery disease | 661 | 6 (0.9) |
| Stroke | 661 | 1 (0.1) |
| Liver failure/cirrhosis | 661 | 1 (0.1) |
| Renal Failure | 661 | 1 (0.1) |
| Chronic lung disease | 661 | 3 (0.4) |
| Asthma | 661 | 70 (10.6) |
| Autoimmune disease | 661 | 50 (7.6) |
| Immunodeficiency | 661 | 6 (0.9) |
| Hematological cancer | 661 | 3 (0.4) |
| Non hematological cancer | 661 | 18 (2.7) |
| Organ or cell transplantation | 661 | 0 (0.0) |
| Taking medication | 661 | 438 (66.3) |
| Staff role | ||
| Administrative staff | 701 | 155 (22.1) |
| Laboratory staff | 701 | 139 (19.8 |
| Handling respiratory samples | 701 | 45 (6.4) |
| Physicians | 701 | 76 (10.8) |
| Paramedics | 701 | 120 (17.1) |
| Nurses | 701 | 164 (23.4) |
| Research scientists | 701 | 10 (1.4) |
| Technicians | 701 | 37 (5.3) |
| In contact with patients | 703 | 395 (56.2) |
| Characteristics | n | Number of Weeks of Participation 1 | Comparison (Coef. ± SE, p-Value) |
|---|---|---|---|
| Age (years) | |||
| 20–29 | 139 | 9 (3–21) | 0.058 ± 0.036, p = 0.11 |
| 30–39 | 208 | 10 (5–26) | |
| 40–49 | 177 | 11 (5–25) | |
| ≥50 | 179 | 12 (6–26) | |
| Gender | |||
| Female | 560 | 11 (5–25) | 2.1 ± 1.0, p = 0.033 |
| Male (reference) | 143 | 9 (4–21) | |
| Staff role | |||
| Administrative staff (reference) | 155 | 8 (4–24) | - |
| Laboratory staff | 139 | 10 (5–22) | 0.82 ± 1.2, p = 0.49 |
| Physicians | 76 | 12 (4–25) | 1.3 ± 1.4, p = 0.35 |
| Paramedics | 120 | 8 (5–15) | −1.7 ± 1.2, 0.17 |
| Nurses | 164 | 24 (8–30) | 7.1 ± 1.1, p < 0.0001 |
| Research scientists | 10 | 5 (1–16) | −5.3 ± 3.4, p = 0.12 |
| Technicians | 37 | 7 (2–21) | −1.1 ± 1.9, p = 0.55 |
| In contact with patients | |||
| Yes | 395 | 13 (5–27) | 3.6 ± 0.81, p < 0.0001 |
| No (reference) | 308 | 8 (5–21) | - |
| Characteristics | All Negative RT-PCR Results (n= 547) | At Least One Positive RT-PCR Result (n = 156) | Logistic Regression Models | |||
|---|---|---|---|---|---|---|
| n Non Missing | Result 1 | n Non Missing | Result 1 | OR (95% CI) | p-Value | |
| Demographics | ||||||
| Age (years) | 547 | 41.4 ± 11.4 | 156 | 41.7 ± 11.2 | 1.0 (0.99–1.02) | 0.79 |
| Gender, women | 547 | 432 (79.0) | 156 | 128 (82.0) | 0.82 (0.52–1.3) | 0.40 |
| Heigth (cm) | 514 | 168 ± 9 | 147 | 168 ± 9 | 1.0 (0.98–1.02) | 0.91 |
| Weigth (kg) | 512 | 68.6 ± 13.7 | 147 | 69.3 ± 13.0 | 1.0 (0.99–1.02) | 0.59 |
| BMI (kg/m2) | 512 | 24.3 ± 4.2 | 147 | 24.6 ± 4.3 | 1.0 (0.97–1.1) | 0.51 |
| Smoking | 514 | 64 (12.4) | 147 | 11 (7.5) | 0.57 (0.29–1.1) | 0.098 |
| Comorbidities | ||||||
| Diabetes mellitus | 514 | 21 (4.1) | 147 | 4 (2.7) | 0.66 (0.22–2.0) | 0.45 |
| Hypertension | 514 | 37 (7.2) | 147 | 11 (7.5) | 1.0 (0.52–2.1) | 0.91 |
| Heart failure/coronary artery disease | 514 | 5 (1.0) | 147 | 1 (0.7) | 0.70 (0.10–6.0) | 0.74 |
| Stroke | 514 | 0 (0.0) | 147 | 1 (0.7) | - | - |
| Liver failure/cirrhosis | 514 | 1 (0.2) | 147 | 0 (0.0) | - | - |
| Renal failure | 514 | 1 (0.2) | 147 | 0 (0.0) | - | - |
| Chronic lung disease | 514 | 3 (0.6) | 147 | 0 (0.0) | - | - |
| Asthma | 514 | 52 (10.1) | 147 | 18 (12.2) | 1.2 (0.70–2.2) | 0.46 |
| Autoimmune disease | 514 | 43 (8.4) | 147 | 7 (4.8) | 0.55 (0.24–1.2) | 0.15 |
| Immunodeficiency | 514 | 5 (1.0) | 147 | 1 (0.7) | 0.70 (0.10–6.0) | 0.74 |
| Hematological cancer | 514 | 3 (0.6) | 147 | 0 (0.0) | - | - |
| Non hematological cancer | 514 | 14 (2.7) | 147 | 4 (2.7) | 1.0 (0.32–3.1) | 1.0 |
| Staff role | 545 | 156 | ||||
| Control group: administrative staff and research scientists | 137 (25.1) | 28 (18.0) | - | - | ||
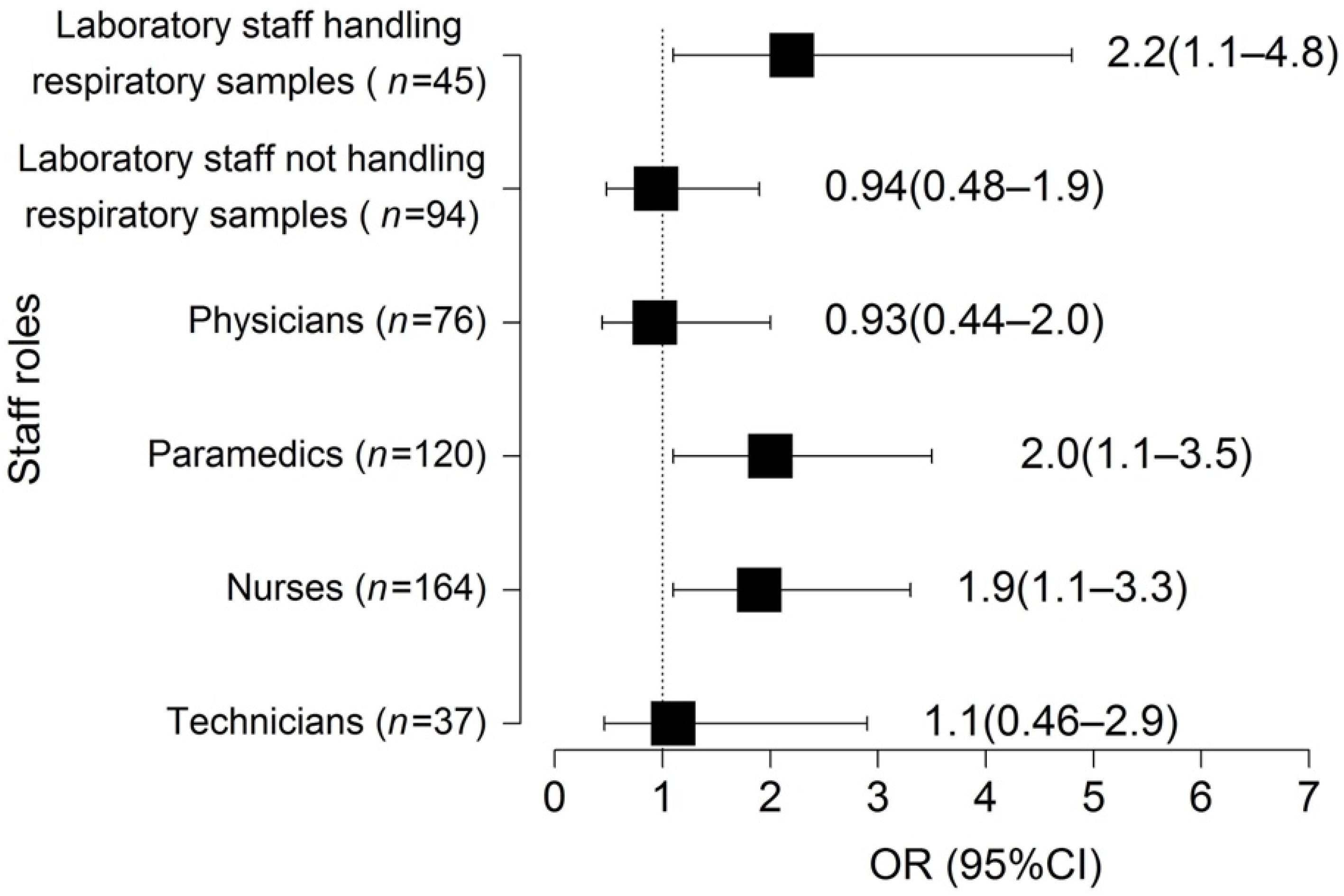
| Laboratory staff handling respiratory samples | 31 (5.7) | 14 (9.0) | 2.2 (1.1–4.8) | 0.0035 | ||
| Laboratory staff not handling respiratory samples | 79 (14.5) | 15 (9.6) | 0.94 (0.48–1.9) | 0.87 | ||
| Physicians | 64 (11.7) | 12 (7.7) | 0.93 (0.44–2.0) | 0.85 | ||
| Paramedics | 86 (15.8) | 34 (21.8) | 2.0 (1.1–3.5) | 0.020 | ||
| Nurses | 118 (21.7) | 46 (29.5) | 1.9 (1.1–3.3) | 0.015 | ||
| Technicians | 30 (5.5) | 7 (4.5) | 1.1 (0.46–2.9) | 0.75 | ||
| In contact with patients | 547 | 296 (54.1) | 156 | 99 (63.5) | 1.5 (1.02–2.1) | 0.039 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Moussaoui, M.; Maes, N.; Hong, S.L.; Lambert, N.; Gofflot, S.; Dellot, P.; Belhadj, Y.; Huynen, P.; Hayette, M.-P.; Meex, C.; et al. Evaluation of Screening Program and Phylogenetic Analysis of SARS-CoV-2 Infections among Hospital Healthcare Workers in Liège, Belgium. Viruses 2022, 14, 1302. https://doi.org/10.3390/v14061302
El Moussaoui M, Maes N, Hong SL, Lambert N, Gofflot S, Dellot P, Belhadj Y, Huynen P, Hayette M-P, Meex C, et al. Evaluation of Screening Program and Phylogenetic Analysis of SARS-CoV-2 Infections among Hospital Healthcare Workers in Liège, Belgium. Viruses. 2022; 14(6):1302. https://doi.org/10.3390/v14061302
Chicago/Turabian StyleEl Moussaoui, Majdouline, Nathalie Maes, Samuel L. Hong, Nicolas Lambert, Stéphanie Gofflot, Patricia Dellot, Yasmine Belhadj, Pascale Huynen, Marie-Pierre Hayette, Cécile Meex, and et al. 2022. "Evaluation of Screening Program and Phylogenetic Analysis of SARS-CoV-2 Infections among Hospital Healthcare Workers in Liège, Belgium" Viruses 14, no. 6: 1302. https://doi.org/10.3390/v14061302