
Epipharyngeal Abrasive Therapy (EAT) Has Potential as a Novel Method for Long COVID Treatment

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
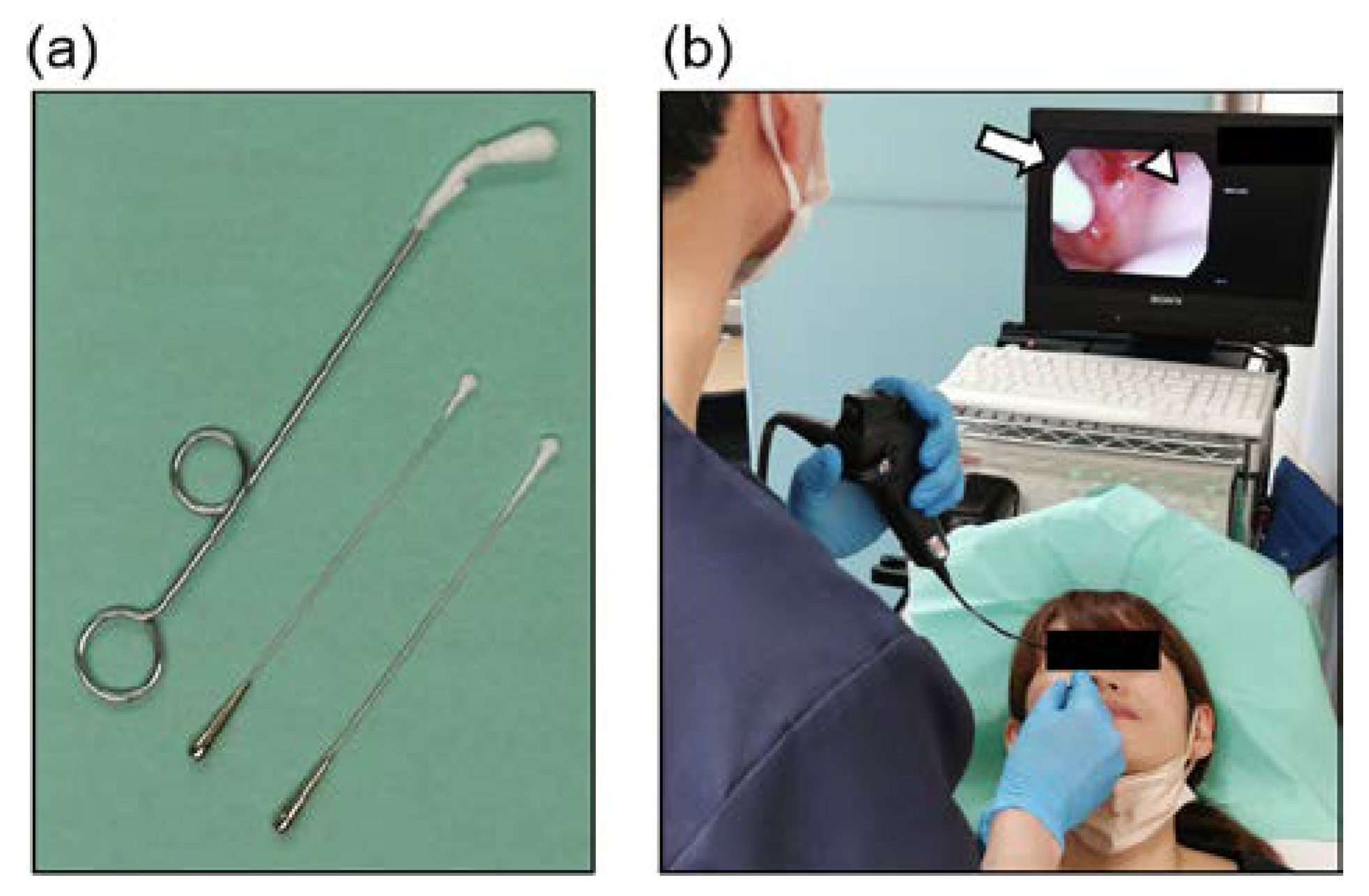
2.2. Epipharyngeal Abrasive Therapy (EAT)
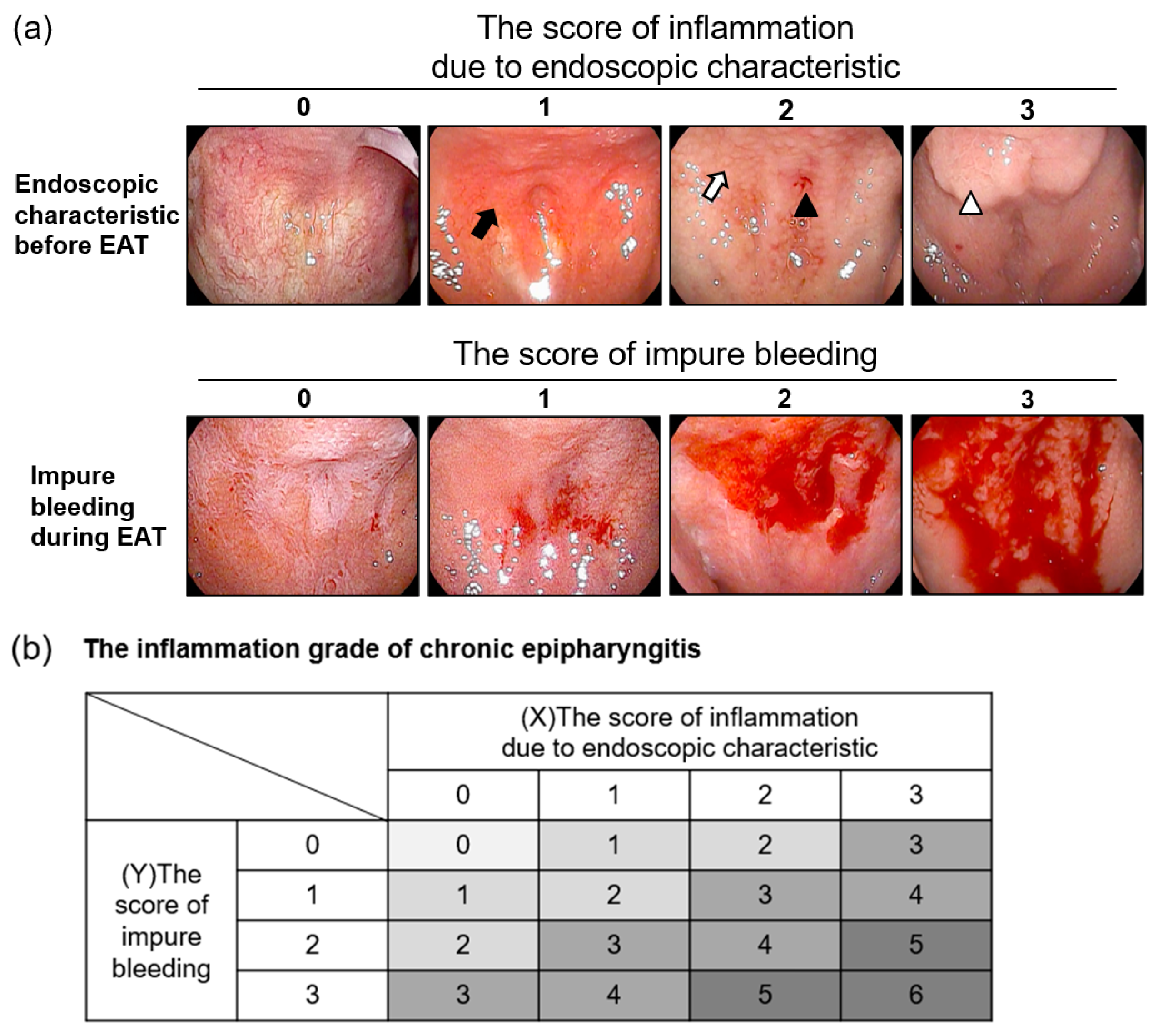
2.3. Diagnosis and Grading of Chronic Epipharyngitis
2.4. Efficacy Analysis of EAT for Chronic Epipharyngitis and Long COVID
3. Results
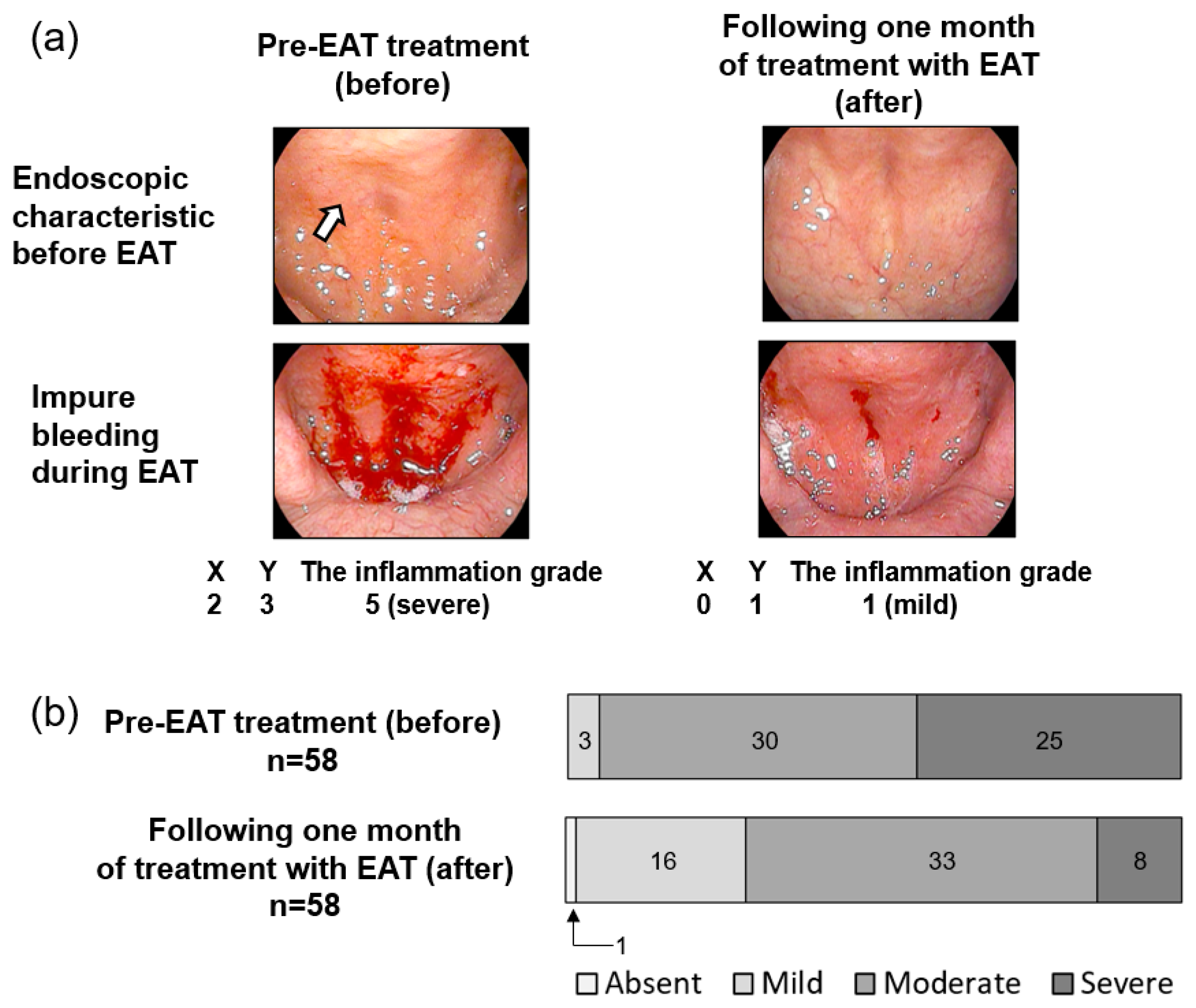
3.1. EAT Reduced Inflammation in the Epipharynx
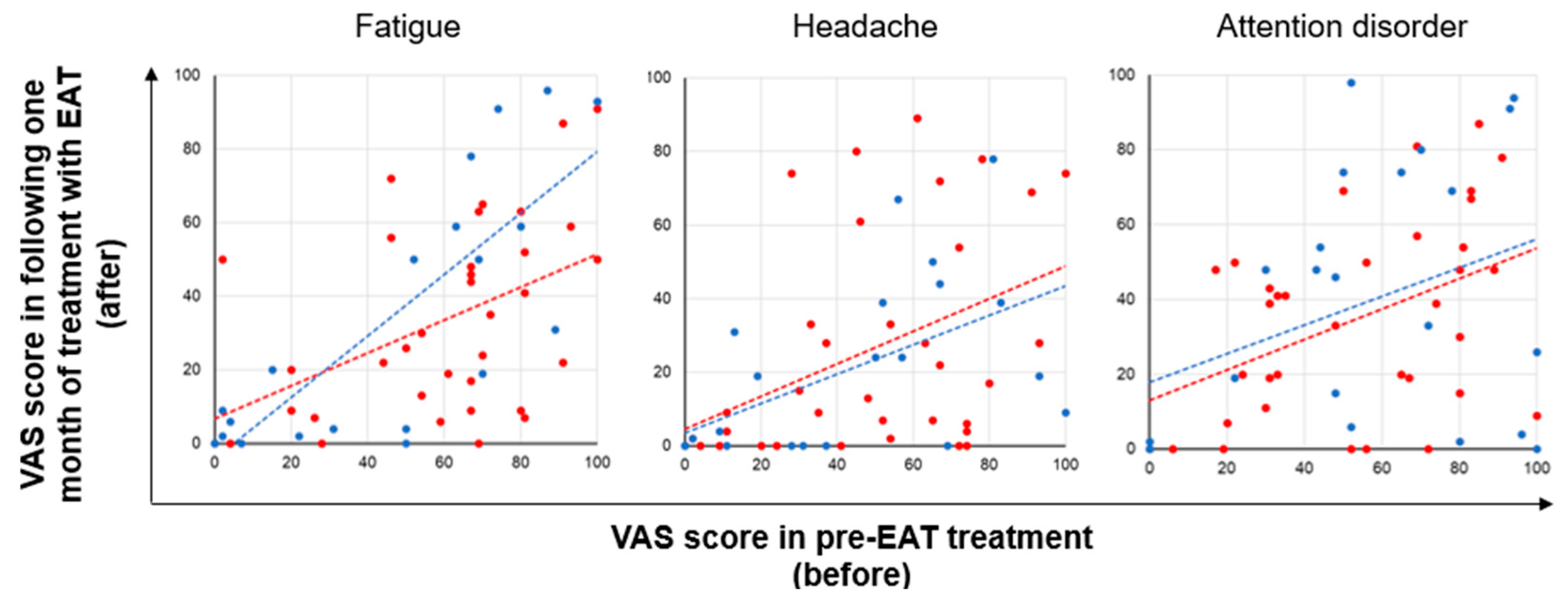
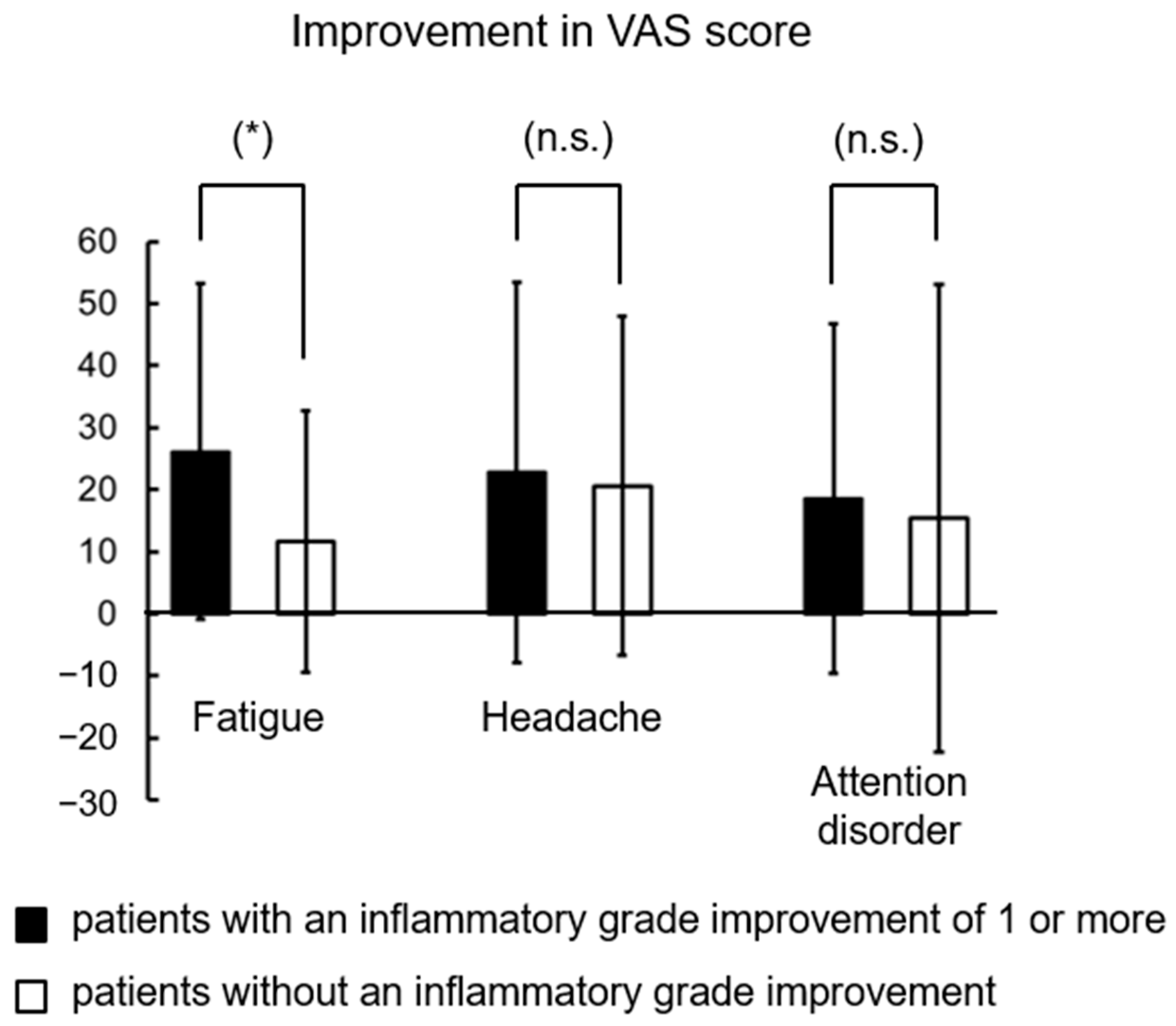
3.2. The Severity of Long COVID Symptoms Decreased Due to EAT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gorna, R.; MacDermott, N.; Rayner, C.; O’Hara, M.; Evans, S.; Agyen, L.; Nutland, W.; Rogers, N.; Hastie, C. Long COVID guidelines need to reflect lived experience. Lancet 2021, 397, 455–457. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Gubbi, S.; Koch, C.A. COVID-19 and chronic fatigue syndrome: An endocrine perspective. J. Clin. Transl. Endocrinol. 2022, 27, 100284. [Google Scholar] [CrossRef]
- Hennigs, J.K.; Oqueka, T.; Harbaum, L.; Klose, H. Organ-specific sequelae of COVID-19 in adults. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2022, 65, 462–470. [Google Scholar] [CrossRef]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Ceban, F.; Leber, A.; Jawad, M.Y.; Yu, M.; Lui, L.M.W.; Subramaniapillai, M.; Di Vincenzo, J.D.; Gill, H.; Rodrigues, N.B.; Cao, B.; et al. Registered clinical trials investigating treatment of long COVID: A scoping review and recommendations for research. Infect. Dis. 2022, 2043560. [Google Scholar] [CrossRef]
- Desgranges, F.; Tadini, E.; Munting, A.; Regina, J.; Filippidis, P.; Viala, B.; Karachalias, E.; Suttels, V.; Haefliger, D.; Kampouri, E.; et al. Post-COVID-19 Syndrome in Outpatients: A Cohort Study. J. Gen. Intern. Med. 2022, 1–10. [Google Scholar] [CrossRef]
- Nishi, K.; Yoshimoto, S.; Nishi, S.; Tsunoda, T.; Ohno, J.; Yoshimura, M.; Hiromatsu, K.; Yamano, T. Epipharyngeal Abrasive Therapy Down-regulates the Expression of SARS-CoV-2 Entry Factors ACE2 and TMPRSS2. In Vivo 2022, 36, 371–374. [Google Scholar] [CrossRef]
- Patarca, R. Cytokines and chronic fatigue syndrome. Ann. N. Y. Acad. Sci. 2001, 933, 185–200. [Google Scholar] [CrossRef]
- Hotta, O.; Oda, T. The epipharynx-kidney axis triggers glomerular vasculitis in immunoglobulin A nephropathy. Immunol. Res. 2019, 67, 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotta, O.; Ieiri, N.; Inoue, C.; Tanaka, A. Chronic epipharyngitis: A missing trigger in chronic fatigue syndrome. J. Transl. Sci. 2018, 4, 2–3. [Google Scholar] [CrossRef]
- Hotta, O.; Ieiri, N.; Nagai, M.; Tanaka, A.; Harabuchi, Y. Role of Palatine Tonsil and Epipharyngeal Lymphoid Tissue in the Development of Glomerular Active Lesions (Glomerular vasculitis) in Immunoglobulin A Nephropathy. Int. J. Mol. Sci. 2022, 23, 727. [Google Scholar] [CrossRef] [PubMed]
- Shin, I.; Hotta, O.; Tani, S. Epipharyngeal abrasive therapy in myalgic encephalomyelitis/chronic fatigue syndrome patients. Jpn. J. Clin. Med. 2021, 79, 989–994. [Google Scholar]
- Tanaka, A. Specifics of each method of endoscopic transnasal epipharyngeal abrasive therapy (E-TN-EAT) and endoscopic transoral epipharyngeal abrasive therapy (E-TO-EAT). Stomato-Pharyngol. 2020, 33, 5–16. [Google Scholar]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Mogitate, M.; Sasaki, Y.; Komiyama, A. Outcome of an outpatient specialty clinic for chronic epipharyngitis. Auris Nasus Larynx 2021, 48, 451–456. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 2021, 27, 895–906. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Iqbal, A.; Iqbal, K.; Arshad Ali, S.; Azim, D.; Farid, E.; Baig, M.D.; Bin Arif, T.; Raza, M. The COVID-19 Sequelae: A Cross-Sectional Evaluation of Post-recovery Symptoms and the Need for Rehabilitation of COVID-19 Survivors. Cureus 2021, 13, e13080. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Prins, J.B.; van der Meer, J.W.; Bleijenberg, G. Chronic fatigue syndrome. Lancet 2006, 367, 346–355. [Google Scholar] [CrossRef]
- Naess, H.; Sundal, E.; Myhr, K.M.; Nyland, H.I. Postinfectious and chronic fatigue syndromes: Clinical experience from a tertiary-referral centre in Norway. In Vivo 2010, 24, 185–188. [Google Scholar] [PubMed]
- Cortes Rivera, M.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Comprehensive Review. Diagnostics 2019, 9, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Swiahb, J.N.; Motiwala, M.A. Upper respiratory tract and otolaryngological manifestations of coronavirus disease 2019 (COVID-19): A systemic review. SAGE Open Med. 2021, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.L.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)-A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef] [PubMed]
- Simani, L.; Ramezani, M.; Darazam, I.A.; Sagharichi, M.; Aalipour, M.A.; Ghorbani, F.; Pakdaman, H. Prevalence and correlates of chronic fatigue syndrome and post-traumatic stress disorder after the outbreak of the COVID-19. J. Neurovirology 2021, 27, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Lu, L.; Fan, H. Global Trends and Research Hotspots in Long COVID: A Bibliometric Analysis. Int. J. Environ. Res. Public Health 2022, 19, 3742. [Google Scholar] [CrossRef]
- Robbins, T.; Gonevski, M.; Clark, C.; Baitule, S.; Sharma, K.; Magar, A.; Patel, K.; Sankar, S.; Kyrou, I.; Ali, A.; et al. Hyperbaric oxygen therapy for the treatment of long COVID: Early evaluation of a highly promising intervention. Clin. Med. 2021, 21, e629–e632. [Google Scholar] [CrossRef]
- Karosanidze, I.; Kiladze, U.; Kirtadze, N.; Giorgadze, M.; Amashukeli, N.; Parulava, N.; Iluridze, N.; Kikabidze, N.; Gudavadze, N.; Gelashvili, L.; et al. Efficacy of Adaptogens in Patients with Long COVID-19: A Randomized, Quadruple-Blind, Placebo-Controlled Trial. Pharmaceuticals 2022, 15, 345. [Google Scholar] [CrossRef]
- Vollbracht, C.; Kraft, K. Feasibility of Vitamin C in the Treatment of Post Viral Fatigue with Focus on Long COVID, Based on a Systematic Review of IV Vitamin C on Fatigue. Nutrients 2021, 13, 1154. [Google Scholar] [CrossRef] [PubMed]
- Hull, D.; Rennie, P.; Noronha, A.; Poore, C.; Harrington, N.; Fearnley, V.; Passàli, D. Effects of creating a non-specific, virus-hostile environment in the nasopharynx on symptoms and duration of common cold. Acta Otorhinolaryngol. Ital. 2007, 27, 73–77. [Google Scholar] [PubMed]
- Hilding, D.A. Literature review: The common cold. Ear Nose Throat J. 1994, 73, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Moneghetti, K.J.; Skhiri, M.; Contrepois, K.; Kobayashi, Y.; Maecker, H.; Davis, M.; Snyder, M.; Haddad, F.; Montoya, J.G. Value of Circulating Cytokine Profiling During Submaximal Exercise Testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Sci. Rep. 2018, 8, 2779. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.; Yang, Y.; Wang, D.; Li, C.; Qu, Y.; Guo, J.; Shi, T.; Bo, W.; Sun, Z.; Asakawa, T. The clinical value of cytokines in chronic fatigue syndrome. J. Transl. Med. 2019, 17, 213. [Google Scholar] [CrossRef] [PubMed]
- Hornig, M.; Montoya, J.G.; Klimas, N.G.; Levine, S.; Felsenstein, D.; Bateman, L.; Peterson, D.L.; Gottschalk, C.G.; Schultz, A.F.; Che, X.; et al. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. Sci. Adv. 2015, 1, e1400121. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; Twisk, F.N.; Johnson, C. Myalgic Encephalomyelitis (ME), Chronic Fatigue Syndrome (CFS), and Chronic Fatigue (CF) are distinguished accurately: Results of supervised learning techniques applied on clinical and inflammatory data. Psychiatry Res. 2012, 200, 754–760. [Google Scholar] [CrossRef]
- Hotta, O.; Inoue, C.; Tanaka, A.; Ieiri, N. Possible Mechanisms Underlying Epipharyngeal Abrasive Therapy (EAT) with ZnCl2 Solution for the Treatment of Autoimmune Diseases and Functional Somatic Syndrome. J. Antivir. Antiretrovir. 2017, 9, 81–86. [Google Scholar] [CrossRef]
- Hotta, O.; Tanaka, A.; Oda, T. Chronic epipharyngitis: A missing background of IgA nephropathy. Autoimmun. Rev. 2019, 18, 835–836. [Google Scholar] [CrossRef]
- Nishi, K.; Nishi, R.; Kimura, S.; Nishi, S.; Tanaka, H.; Yamano, T. Therapeutic effect of epipharyngeal abrasive therapy (EAT) on pharyngeal allergies. Stomato-Pharyngol. 2022, 35, 372–374. [Google Scholar]
- Maniaci, A.; Di Luca, M.; La Mantia, I.; Grillo, C.; Grillo, C.M.; Privitera, E.; Vicini, C.; Iannella, G.; Renna, C.; Bannò, V.; et al. Surgical Treatment for the Refractory Allergic Rhinitis: State of the Art. Allergies 2021, 1, 5. [Google Scholar] [CrossRef]
- Wise, S.K.; Lin, S.Y.; Toskala, E.; Orlandi, R.R.; Akdis, C.A.; Alt, J.A.; Azar, A.; Baroody, F.M.; Bachert, C.; Canonica, G.W.; et al. International Consensus Statement on Allergy and Rhinology: Allergic Rhinitis. Int. Forum Allergy Rhinol. 2018, 8, 108–352. [Google Scholar] [CrossRef] [PubMed]
- Koopman, F.A.; Chavan, S.S.; Miljko, S.; Grazio, S.; Sokolovic, S.; Schuurman, P.R.; Mehta, A.D.; Levine, Y.A.; Faltys, M.; Zitnik, R.; et al. Vagus nerve stimulation inhibits cytokine production and attenuates disease severity in rheumatoid arthritis. Proc. Natl. Acad. Sci. USA 2016, 113, 8284–8289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Qi, D.; Li, J.N.; Deng, X.Y.; Wang, D.X. Vagus nerve stimulation enhances the cholinergic anti-inflammatory pathway to reduce lung injury in acute respiratory distress syndrome via STAT3. Cell Death Discov. 2021, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Staats, P.; Giannakopoulos, G.; Blake, J.; Liebler, E.; Levy, R.M. The Use of Non-invasive Vagus Nerve Stimulation to Treat Respiratory Symptoms Associated with COVID-19: A Theoretical Hypothesis and Early Clinical Experience. Neuromodulation 2020, 23, 784–788. [Google Scholar] [CrossRef]
- Baptista, A.F.; Baltar, A.; Okano, A.H.; Moreira, A.; Campos, A.C.P.; Fernandes, A.M.; Brunoni, A.R.; Badran, B.W.; Tanaka, C.; de Andrade, D.C.; et al. Applications of Non-invasive Neuromodulation for the Management of Disorders Related to COVID-19. Front. Neurol 2020, 11, 573718. [Google Scholar] [CrossRef]
- Yuan, H.; Silberstein, S.D. Vagus Nerve Stimulation and Headache. Headache 2017, 57 (Suppl. S1), 29–33. [Google Scholar] [CrossRef] [Green Version]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-EAT Treatment (before) | Following One Month of Treatment with EAT (after) | Significance of Difference | Effect Sizes | |||||
|---|---|---|---|---|---|---|---|---|
| Parameters | Mean | Median | SD | Mean | Median | SD | p-Value a | Cohen’s d b |
| Inflammation grade | 4.69 | 1.13 | 3.57 | 1.31 | 5.4 × 10−7 * | −0.92 | ||
| VAS score for fatigue | 53.64 | 65 | 31.54 | 33.24 | 23 | 30.24 | 1.6 × 10−7 * | −0.66 |
| VAS score for headache | 45.48 | 49 | 30.05 | 23.57 | 11 | 27.38 | 5.7 × 10−7 * | −0.76 |
| VAS score for attention disorder | 53.43 | 52 | 29.79 | 36.12 | 36 | 29.66 | 1.6 × 10−4 * | −0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imai, K.; Yamano, T.; Nishi, S.; Nishi, R.; Nishi, T.; Tanaka, H.; Tsunoda, T.; Yoshimoto, S.; Tanaka, A.; Hiromatsu, K.; et al. Epipharyngeal Abrasive Therapy (EAT) Has Potential as a Novel Method for Long COVID Treatment. Viruses 2022, 14, 907. https://doi.org/10.3390/v14050907
Imai K, Yamano T, Nishi S, Nishi R, Nishi T, Tanaka H, Tsunoda T, Yoshimoto S, Tanaka A, Hiromatsu K, et al. Epipharyngeal Abrasive Therapy (EAT) Has Potential as a Novel Method for Long COVID Treatment. Viruses. 2022; 14(5):907. https://doi.org/10.3390/v14050907
Chicago/Turabian StyleImai, Kazuaki, Takafumi Yamano, Soichiro Nishi, Ryushiro Nishi, Tatsuro Nishi, Hiroaki Tanaka, Toshiyuki Tsunoda, Shohei Yoshimoto, Ayaki Tanaka, Kenji Hiromatsu, and et al. 2022. "Epipharyngeal Abrasive Therapy (EAT) Has Potential as a Novel Method for Long COVID Treatment" Viruses 14, no. 5: 907. https://doi.org/10.3390/v14050907