
Factors Associated with Significant Platelet Count Improvement in Thrombocytopenic Chronic Hepatitis C Patients Receiving Direct-Acting Antivirals

 , , , , , , , , , , , , , ,
, , , , , , , , , , , , , ,  , , , , ,
, , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
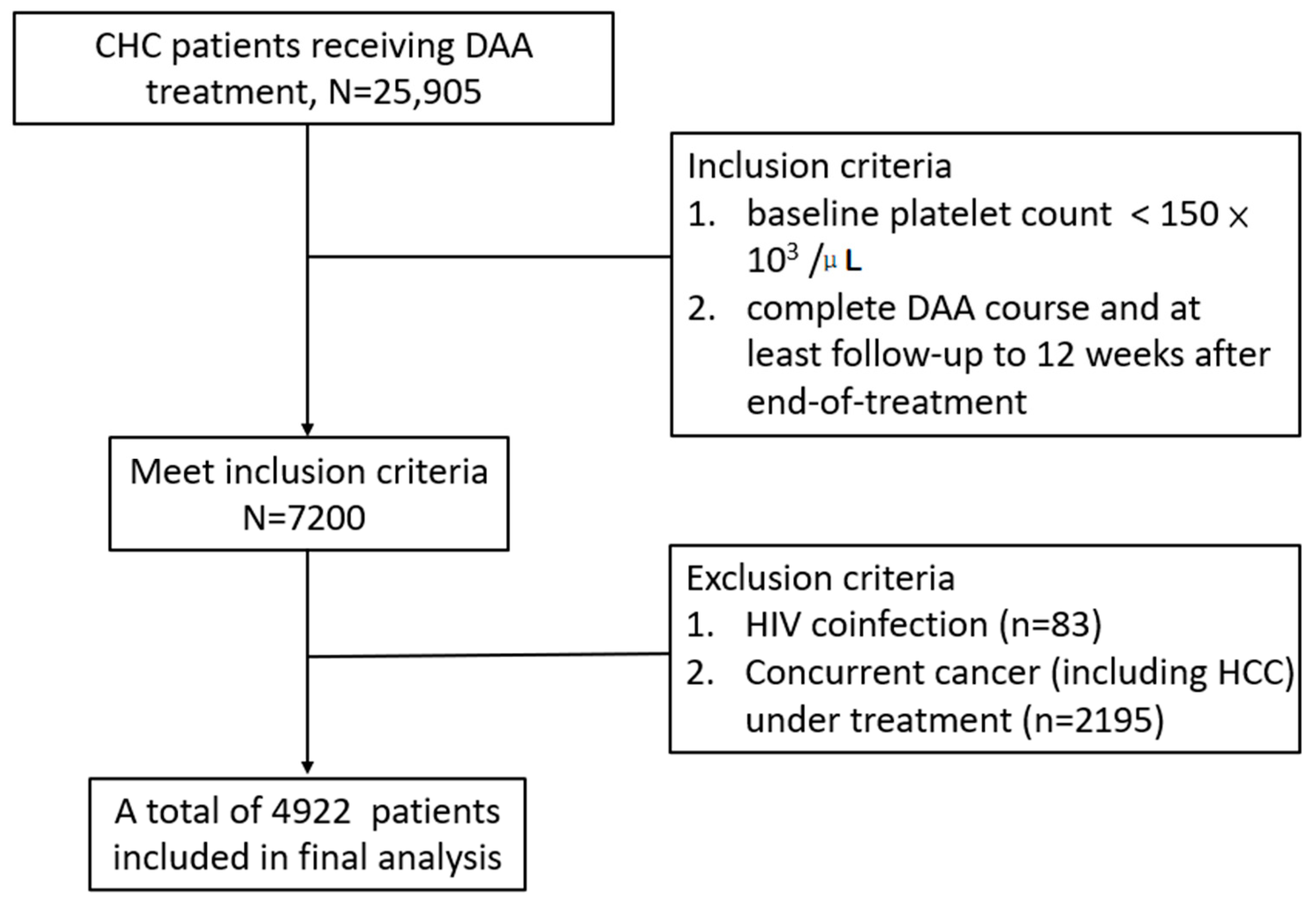
2.1. Patient Selection
2.2. Clinical and Laboratory Monitoring
2.3. Statistical and Data Analysis
3. Results
3.1. Baseline Characteristics of CHC Patients
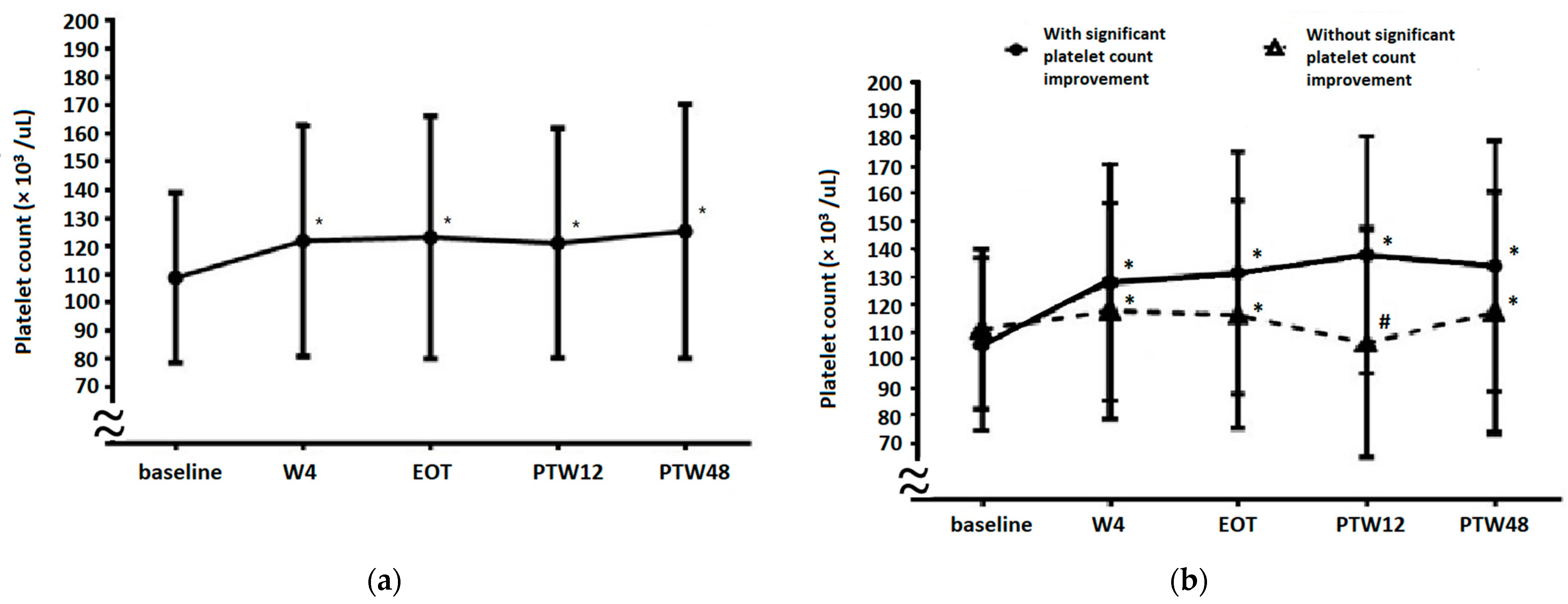
3.2. Platelet Count Evolution from Baseline to 48 Weeks after EOT (PTW48)
3.3. Factors Associated with Significant Platelet Count Improvement
3.4. Platelet Count Evolution in Patients with or without Significant Platelet Count Improvement
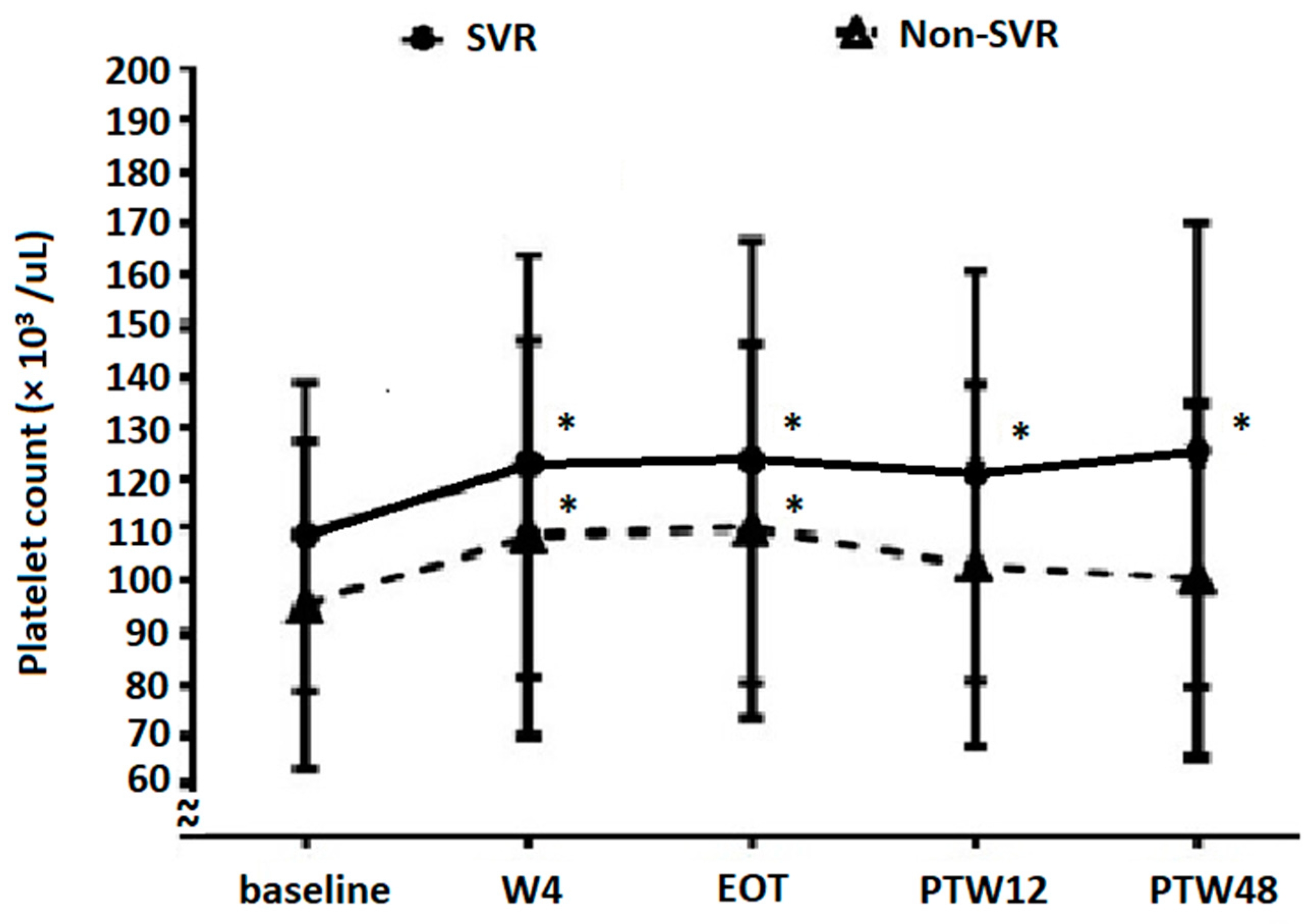
3.5. Platelet Count Evolution Based on DAA Treatment Response
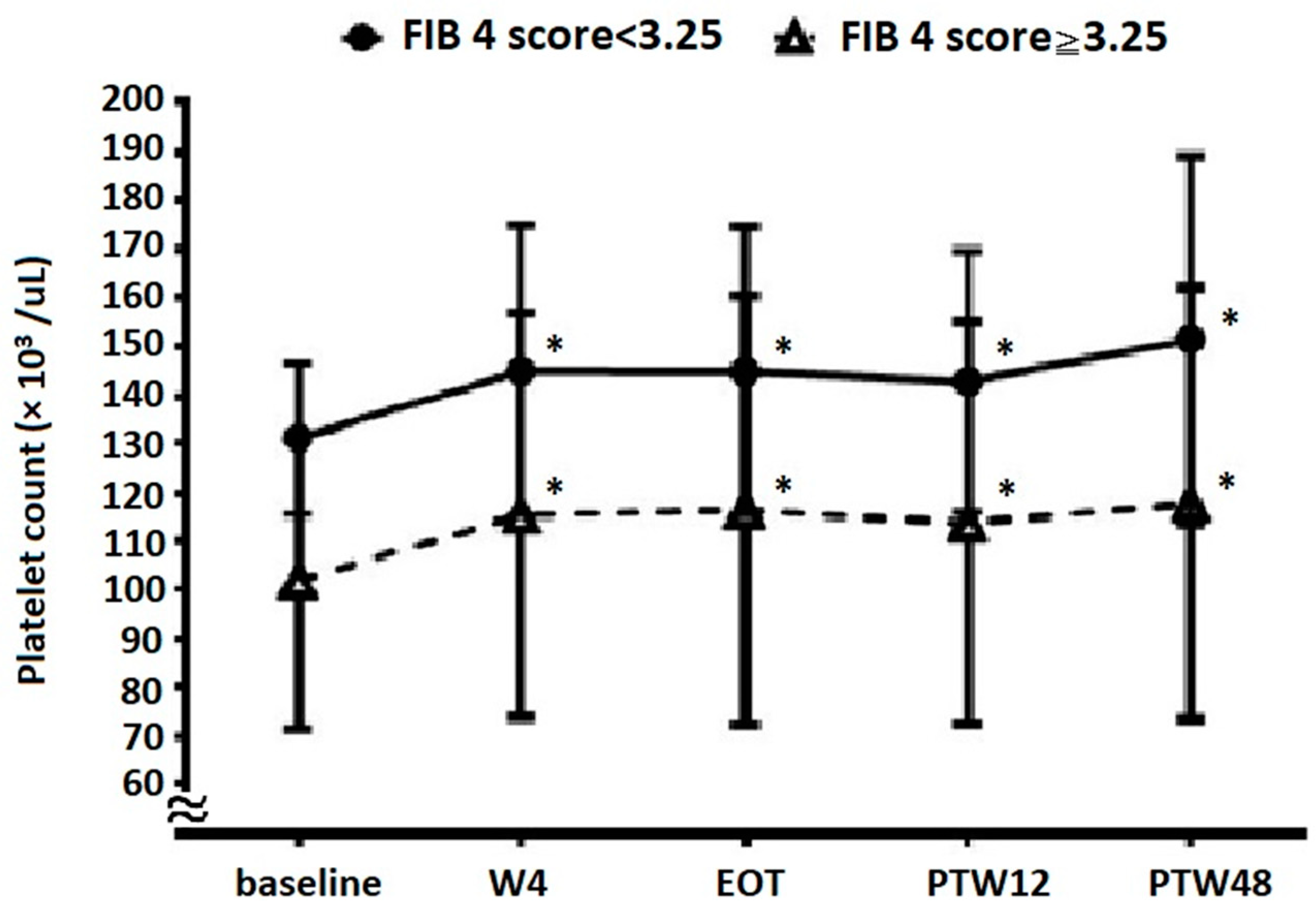
3.6. Platelet Count Evolution Based on Baseline Fibrosis Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Louie, K.S.; Micallef, J.M.; Pimenta, J.M.; Forssen, U.M. Prevalence of thrombocytopenia among patients with chronic hepatitis C: A systematic review. J. Viral Hepat. 2011, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.-Y.; Ho, C.-K.; Huang, J.-F.; Hsieh, M.-Y.; Hou, N.-J.; Lin, Z.-Y.; Chen, S.-C.; Wang, L.-Y.; Chang, W.-Y.; Yu, M.-L.; et al. Hepatitis C virus viremia and low platelet count: A study in a hepatitis B & C endemic area in Taiwan. J. Hepatol. 2010, 52, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Maruoka, D.; Imazeki, F.; Arai, M.; Kanda, T.; Fujiwara, K.; Yokosuka, O. Longitudinal changes of the laboratory data of chronic hepatitis C patients with sustained virological response on long-term follow-up. J. Viral Hepat. 2012, 19, e97–e104. [Google Scholar] [CrossRef] [PubMed]
- Van Der Meer, A.J.; Maan, R.; Veldt, B.J.; Feld, J.J.; Wedemeyer, H.; Dufour, J.-F.; Lammert, F.; Duarte-Rojo, A.; Manns, M.P.; Zeuzem, S.; et al. Improvement of platelets after SVR among patients with chronic HCV infection and advanced hepatic fibrosis. J. Gastroenterol. Hepatol. 2016, 31, 1168–1176. [Google Scholar] [CrossRef] [Green Version]
- Kee, K.-M.; Wang, J.-H.; Hung, C.-H.; Chen, C.-H.; Lee, C.-M.; Lu, S.-N. Improvement of thrombocytopenia in hepatitis C-related advanced fibrosis patients after sustained virological response. Dig. Dis. Sci. 2013, 58, 556–561. [Google Scholar] [CrossRef]
- Yeh, M.-L.; Huang, C.-I.; Huang, C.-F.; Hsieh, M.-H.; Hsieh, M.-Y.; Lin, Z.-Y.; Chen, S.-C.; Huang, J.-F.; Kuo, P.-L.; Kuo, H.-T.; et al. Post-treatment alpha fetoprotein and platelets predict hepatocellular carcinoma development in dual-infected hepatitis B and C patients after eradication of hepatitis C. Oncotarget 2018, 9, 12240–12249. [Google Scholar] [CrossRef] [Green Version]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Ghany, M.G.; Morgan, T.R.; AASLD-IDSA Hepatitis C Guidance Panel. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases-Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.-L.; Chen, P.-J.; Dai, C.-Y.; Hu, T.-H.; Huang, C.-F.; Huang, Y.-H.; Hung, C.-H.; Lin, C.-Y.; Liu, C.-H.; Liu, C.-J.; et al. Taiwan consensus statement on the management of hepatitis C: Part (I) general population. J. Formos. Med. Assoc. 2020, 119, 1019–1040. [Google Scholar] [CrossRef]
- Yu, M.-L.; Chen, P.-J.; Dai, C.-Y.; Hu, T.-H.; Huang, C.-F.; Huang, Y.-H.; Hung, C.-H.; Lin, C.-Y.; Liu, C.-H.; Liu, C.-J.; et al. Taiwan consensus statement on the management of hepatitis C: Part (II) special populations. J. Formos. Med. Assoc. 2020, 119, 1135–1157. [Google Scholar] [CrossRef]
- Honma, Y.; Shibata, M.; Hayashi, T.; Kusanaga, M.; Ogino, N.; Minami, S.; Kumei, S.; Oe, S.; Miyagawa, K.; Senju, M.; et al. Effect of direct-acting antivirals on platelet-associated immunoglobulin G and thrombocytopenia in hepatitis C virus-related chronic liver disease. Liver Int. 2019, 39, 1641–1651. [Google Scholar] [CrossRef]
- Sayyar, M.; Saidi, M.; Zapatka, S.; Deng, Y.; Ciarleglio, M.; Garcia-Tsao, G. Platelet count increases after viral elimination in chronic HCV, independent of the presence or absence of cirrhosis. Liver Int. 2019, 39, 2061–2065. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Tseng, C.W.; Tseng, K.C. Rapid platelet count improvement in chronic hepatitis C patients with thrombocytopenia receiving direct-acting antiviral agents. Medicine (Baltimore) 2020, 99, e20156. [Google Scholar] [CrossRef] [PubMed]
- Ishizu, Y.; Ishigami, M.; Hayashi, K.; Honda, T.; Kuzuya, T.; Ito, T.; Fujishiro, M. Rapid increase of platelet counts during antiviral therapy in patients with hepatitis C virus infection. Hepatol. Res. 2020, 50, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.C.; Ko, P.H.; Lee, C.C.; Tseng, C.W.; Tseng, K.C. Baseline thrombopoietin level is associated with platelet count improvement in thrombocytopenic chronic hepatitis C patients after successful direct-acting antiviral agent therapy. BMC Gastroenterol. 2021, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Calvaruso, V.; Craxi, A. Hepatic benefits of HCV cure. J. Hepatol. 2020, 73, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-F.; Yeh, M.-L.; Huang, C.-I.; Lin, Z.-Y.; Chen, S.-C.; Dai, C.-Y.; Huang, J.-F.; Yu, M.-L. Interference of hepatitis B virus dual infection in platelet count recovery in chronic hepatitis C patients with curative antiviral therapy. J. Gastroenterol. Hepatol. 2018, 33, 1108–1114. [Google Scholar] [CrossRef]
- Chen, C.; Huang, C.; Cheng, P.; Tseng, K.; Lo, C.; Kuo, H.; Huang, Y.; Tai, C.; Peng, C.; Bair, M.; et al. Factors associated with treatment failure of direct-acting antivirals for chronic hepatitis C: A real-world nationwide hepatitis C virus registry programme in Taiwan. Liver Int. 2021, 41, 1265–1277. [Google Scholar] [CrossRef]
- D’Amico, G.; Morabito, A.; D’Amico, M.; Pasta, L.; Malizia, G.; Rebora, P.; Valsecchi, M.G. New concepts on the clinical course and stratification of compensated and decompensated cirrhosis. Hepatol. Int. 2018, 12, 34–43. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Pawlotsky, J.-M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H. EASL Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck-Radosavljevic, M. Thrombocytopenia in chronic liver disease. Liver Int. 2017, 37, 778–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannini, E.; Borro, P.; Botta, F.; Fumagalli, A.; Malfatti, F.; Podestà, E.; Romagnoli, P.; Testa, E.; Chiarbonello, B.; Polegato, S.; et al. Serum thrombopoietin levels are linked to liver function in untreated patients with hepatitis C virus-related chronic hepatitis. J. Hepatol. 2002, 37, 572–577. [Google Scholar] [CrossRef]
- Bolognesi, M.; Merkel, C.; Sacerdoti, D.; Nava, V.; Gatta, A. Role of spleen enlargement in cirrhosis with portal hypertension. Dig. Liver Dis. 2002, 34, 144–150. [Google Scholar] [CrossRef]
- Jesri, A.; Okonofua, E.C.; Egan, B.M. Platelet and white blood cell counts are elevated in patients with the metabolic syndrome. J. Clin. Hypertens. (Greenwich) 2005, 7, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Lee, J.W.; Shim, J.Y.; Lee, Y.J. Relationship Between Platelet Count and Insulin Resistance in Korean Adolescents: A Nationwide Population-Based Study. Metab. Syndr. Relat. Disord. 2018, 16, 470–476. [Google Scholar] [CrossRef]
- Fuentes, E.; Fuentes, F.; Vilahur, G.; Badimon, L.; Palomo, I. Mechanisms of chronic state of inflammation as mediators that link obese adipose tissue and metabolic syndrome. Med. Inflamm. 2013, 2013, 136584. [Google Scholar] [CrossRef]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N.; et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef]
- Bhatta, S.; Singh, S.; Gautam, S.; Osti, B.P. Mean Platelet Volume and Platelet Count in Patients with Type 2 Diabetes Mellitus and Impaired Fasting Glucose. J. Nepal. Health Res. Counc. 2019, 16, 392–395. [Google Scholar] [CrossRef]
- Poordad, F.; Dieterich, D. Treating hepatitis C: Current standard of care and emerging direct-acting antiviral agents. J. Viral Hepat. 2012, 19, 449–464. [Google Scholar] [CrossRef]
- Aghemo, A.; Degasperi, E.; De Nicola, S.; Bono, P.; Orlandi, A.; D’Ambrosio, R.; Soffredini, R.; Perbellini, R.; Lunghi, G.; Colombo, M. Quantification of Core Antigen Monitors Efficacy of Direct-acting Antiviral Agents in Patients With Chronic Hepatitis C Virus Infection. Clin. Gastroenterol. Hepatol. 2016, 14, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Perpiñán, E.; Caro-Pérez, N.; García-González, N.; Gregori, J.; González, P.; Bartres, C.; Soria, M.E.; Perales, C.; Lens, S.; Mariño, Z.; et al. Hepatitis C virus early kinetics and resistance-associated substitution dynamics during antiviral therapy with direct-acting antivirals. J. Viral Hepat. 2018, 25, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, M.; Faleo, G.; Mohamed, A.M.F.; Morella, S.; Bruno, S.R.; Tundo, P.; Fiore, J.R.; Santantonio, T.A. Resistance Associated Mutations in HCV Patients Failing DAA Treatment. New Microbiol. 2021, 44, 12–18. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables Mean ± SD or n (%) | Total (n = 4922) | Patients with Significant Platelet Count Improvement # (n = 2230) | Patients without Significant Platelet Count Improvement # (n = 2692) | p Value |
|---|---|---|---|---|
| Baseline clinical characteristics | ||||
| Age (years) | 65.0 ± 10.7 | 64.6 ± 10.7 | 65.3 ± 10.6 | 0.023 |
| Male sex, n (%) | 2030 (41.2) | 941 (42.2) | 1089 (40.5) | 0.216 |
| HTN, n (%) | 3185 (64.7) | 1444 (64.8) | 1741 (64.7) | 0.953 |
| DM, n (%) | 1245 (25.3) | 598 (26.8) | 647 (24.0) | 0.025 |
| Cirrhosis, n (%) | 2051 (41.7) | 849 (38.1) | 1202 (44.7) | <0.0001 |
| Decompensated cirrhosis, n (%) | 270 (5.5) | 100 (4.5) | 170 (6.3) | 0.005 |
| History of variceal bleeding, n (%) | 92 (1.9) | 33 (1.5) | 59 (2.2) | 0.067 |
| HBV coinfection, n (%) | 361 (7.3) | 164 (7.3) | 197 (7.3) | 0.961 |
| Ascites, n (%) | 159 (3.2) | 55 (2.5) | 104 (3.9) | 0.006 |
| History of HE, n (%) | 10 (0.2) | 6 (0.3) | 4 (0.2) | 0.350 |
| Treatment experienced, n (%) | 1167 (23.7) | 519 (23.3) | 648 (24.1) | 0.512 |
| CKD, n (%) | 377 (7.7) | 179 (8.0) | 198 (7.4) | 0.378 |
| SVR12, n (%) | 4859 (98.7) | 2205 (98.9) | 2654 (98.6) | 0.367 |
| Baseline laboratory data | ||||
| Platelet count (103/μL) | 108.8 ± 30.0 | 105.7 ± 31.3 | 111.4 ± 28.6 | <0.0001 |
| AST (U/L) | 78.4 ± 57.6 | 78.9 ± 54.8 | 78.1 ± 59.9 | 0.615 |
| ALT (U/L) | 88.7 ± 74.1 | 90.1 ± 70.3 | 87.5 ± 77.2 | 0.214 |
| Total bilirubin (mg/dL) | 0.99 ± 0.54 | 0.96 ± 0.52 | 1.01 ± 0.56 | 0.003 |
| Albumin (g/dL) | 4.04 ± 0.45 | 4.05 ± 0.44 | 4.03 ± 0.46 | 0.299 |
| PT INR | 1.09 ± 0.34 | 1.09 ± 0.38 | 1.09 ± 0.31 | 0.807 |
| Creatinine (mg/dL) | 1.18 ± 1.62 | 1.24 ± 1.78 | 1.13 ± 1.47 | 0.025 |
| AFP (ng/mL) | 19.4 ± 114.2 | 21.4 ± 127.3 | 17.7 ± 102.0 | 0.272 |
| Variable | Single Variable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | p Value | |
| Baseline clinical characteristics | ||||
| Age | 0.99 (0.99, 1.00) | 0.023 | 0.99 (0.99, 1.00) | 0.01 |
| Male sex | 1.07 (0.96, 1.20) | 0.216 | 1.09 (0.72,2.15) | 0.171 |
| HTN | 1.00 (0.89, 1.12) | 0.953 | ||
| DM | 1.16 (1.01, 1.32) | 0.026 | 1.20 (1.06, 1.38) | 0.007 |
| Cirrhosis | 0.76 (0.68, 0.85) | <0.0001 | 0.66 (0.58, 0.75) | <0.0001 |
| Decompensated cirrhosis | 0.70 (0.54, 0.90) | 0.005 | 0.99 (0.62, 1.60) | 0.992 |
| History of variceal bleeding | 0.67 (0.44, 1.03) | 0.068 | 0.80 (0.46,1.39) | 0.438 |
| HBV coinfection | 1.01 (0.81, 1.25) | 0.961 | ||
| Ascites | 0.63 (0.45, 0.88) | 0.006 | 0.65 (0.38, 1.10) | 0.107 |
| History of HE | 1.81 (0.51, 6.43) | 0.357 | ||
| Treatment experienced | 0.96 (0.84, 1.09) | 0.512 | ||
| With CKD | 1.10 (0.89, 1.36) | 0.378 | ||
| With SVR12 | 1.26 (0.76, 2.10) | 0.368 | ||
| Baseline laboratory data | ||||
| Platelet count | 0.41 (0.31, 0.53) | <0.0001 | 0.99 (0.98, 0.99) | <0.0001 |
| Total bilirubin | 0.85 (0.76, 0.95) | 0.002 | 0.80 (0.71, 0.91) | 0.0003 |
| Albumin | 1.07 (0.94, 1.21) | 0.300 | ||
| PT INR | 1.02 (0.87, 1.21) | 0.804 | ||
| Creatinine | 1.04 (1.00, 1.08) | 0.026 | 1.02 (0.98, 1.06) | 0.261 |
| AFP | 1.00 (0.99, 1.00) | 0.261 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Chang, T.-S.; Chen, C.-H.; Cheng, P.-N.; Lo, C.-C.; Mo, L.-R.; Chen, C.-T.; Huang, C.-F.; Kuo, H.-T.; Huang, Y.-H.; et al. Factors Associated with Significant Platelet Count Improvement in Thrombocytopenic Chronic Hepatitis C Patients Receiving Direct-Acting Antivirals. Viruses 2022, 14, 333. https://doi.org/10.3390/v14020333
Chen Y-C, Chang T-S, Chen C-H, Cheng P-N, Lo C-C, Mo L-R, Chen C-T, Huang C-F, Kuo H-T, Huang Y-H, et al. Factors Associated with Significant Platelet Count Improvement in Thrombocytopenic Chronic Hepatitis C Patients Receiving Direct-Acting Antivirals. Viruses. 2022; 14(2):333. https://doi.org/10.3390/v14020333
Chicago/Turabian StyleChen, Yen-Chun, Te-Sheng Chang, Chien-Hung Chen, Pin-Nan Cheng, Ching-Chu Lo, Lein-Ray Mo, Chun-Ting Chen, Chung-Feng Huang, Hsing-Tao Kuo, Yi-Hsiang Huang, and et al. 2022. "Factors Associated with Significant Platelet Count Improvement in Thrombocytopenic Chronic Hepatitis C Patients Receiving Direct-Acting Antivirals" Viruses 14, no. 2: 333. https://doi.org/10.3390/v14020333