
Impact of Hepatitis B Virus Infection, Non-alcoholic Fatty Liver Disease, and Hepatitis C Virus Co-infection on Liver-Related Death among People Tested for Hepatitis B Virus in British Columbia: Results from a Large Longitudinal Population-Based Cohort Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Methods
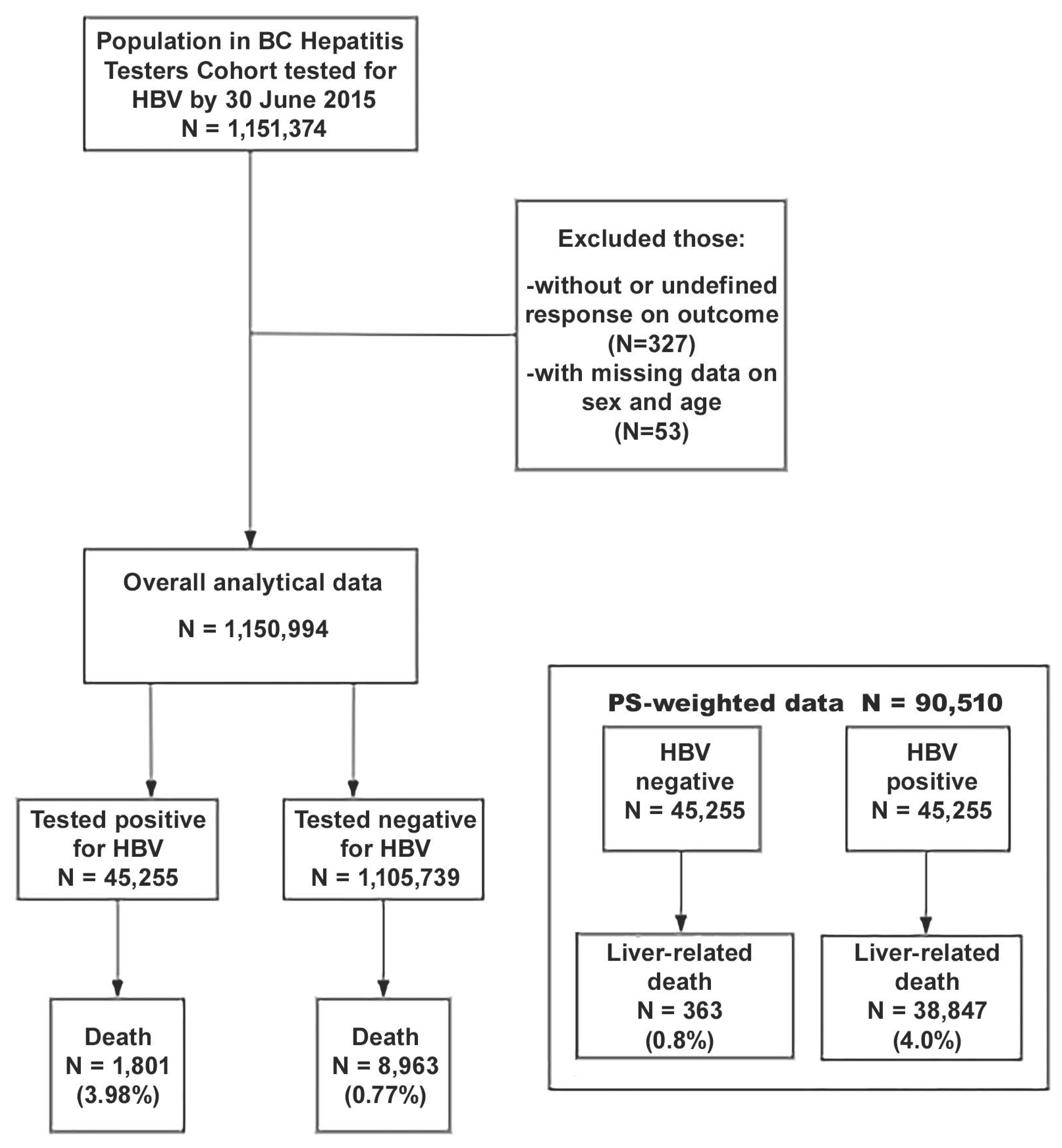
2.1. Data Source, Design, and Study Population
2.2. Outcome and Exposure
2.3. Potential Risk Factors
2.4. Statistical Analysis
3. Results
3.1. Study Participant’s Characteristics
3.2. Liver-Related Mortality Rate among Participants
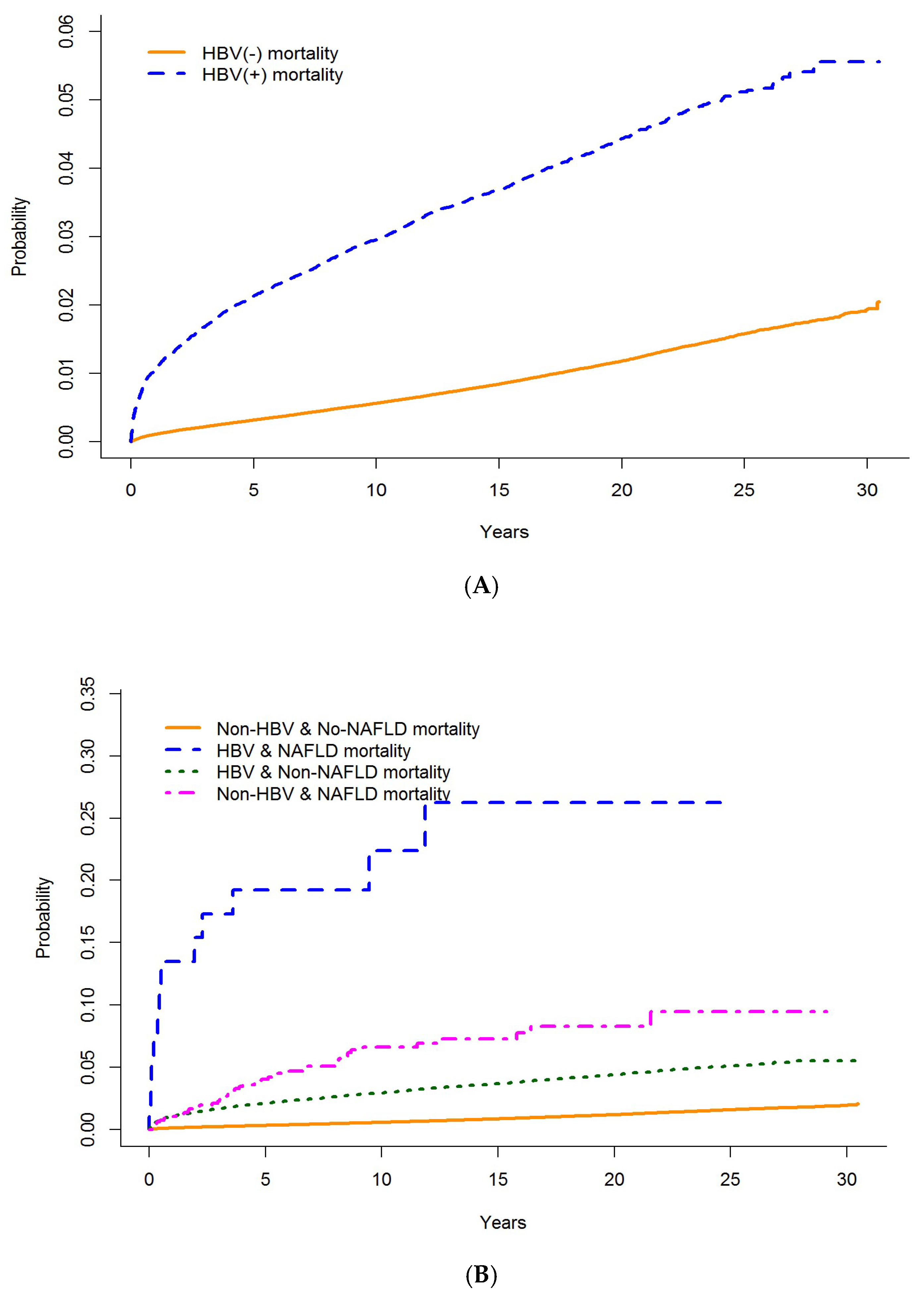
3.3. Effect of HBV Infection on Liver-Related Mortality
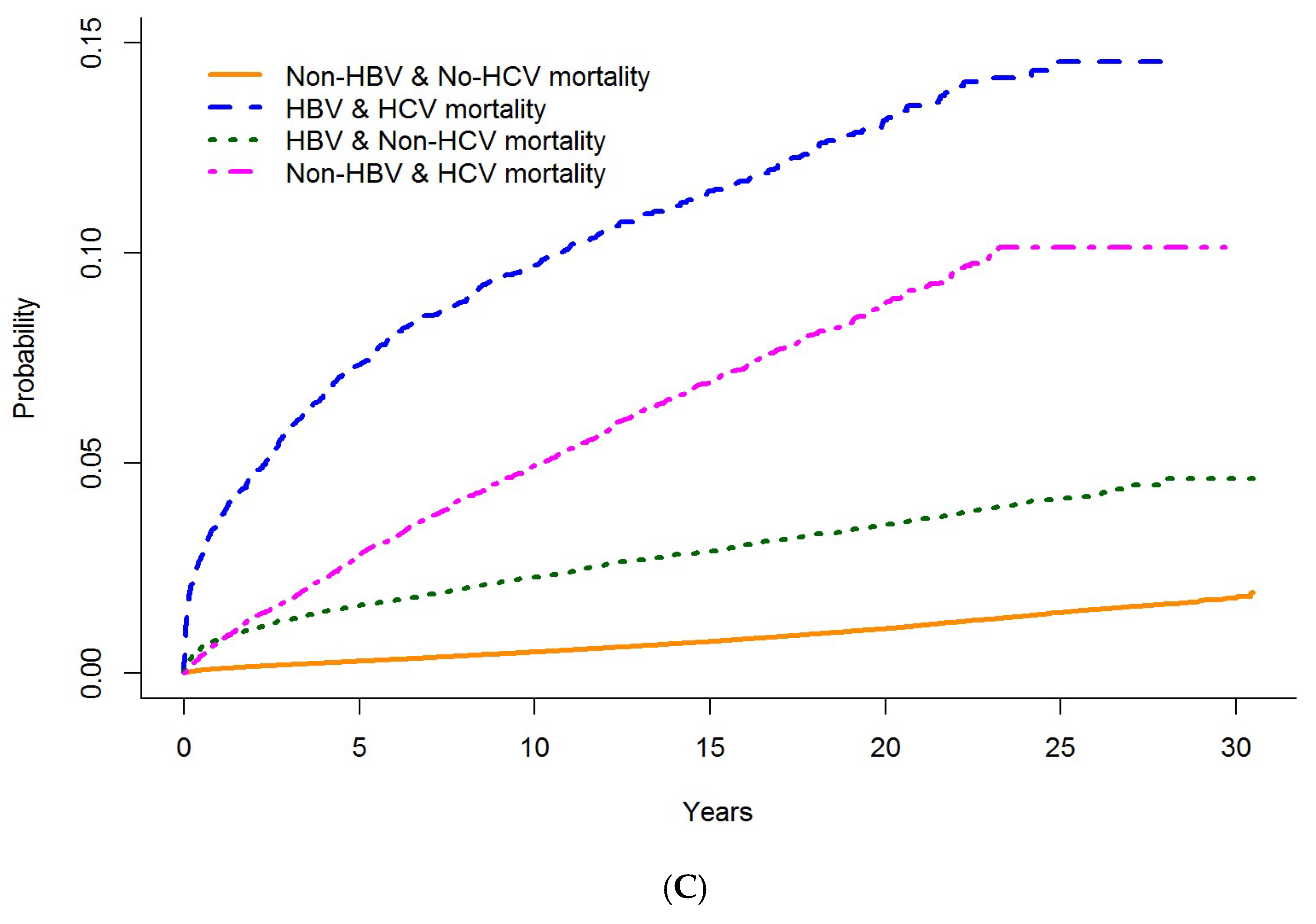
3.4. The Effect of NAFLD and HCV Infection in the HBV Liver-Related Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections; World Health Organization: Geneva, Switzerland, 2021; Volume 53, pp. 1689–1699. Available online: https://www.who.int/publications/i/item/9789240027077 (accessed on 20 September 2021).
- Fattovich, G.; Olivari, N.; Pasino, M.; D′Onofrio, M.; Martone, E.; Donato, F. Long-term outcome of chronic hepatitis B in Caucasian patients: Mortality after 25 years. Gut 2007, 57, 84–90. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Ventura-Cots, M.; Ballester-Ferré, M.P.; Ravi, S.; Bataller, R. Public health policies and alcohol-related liver disease. JHEP Rep. 2019, 1, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Myers, R.P.; Krajden, M.; Bilodeau, M.; Kaita, K.; Marotta, P.; Peltekian, K.; Ramji, A.; Estes, C.; Razavi, H.; Sherman, M. Burden of Disease and Cost of Chronic Hepatitis C Virus Infection in Canada. Can. J. Gastroenterol. Hepatol. 2014, 28, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Janjua, N.Z.; Wong, S.; Abdia, Y.; Jeong, D.; Buller-Taylor, T.; Adu, P.A.; Samji, H.; Wilton, J.; Pearce, M.; Butt, Z.A.; et al. Impact of direct-acting antivirals for HCV on mortality in a large population-based cohort study. J. Hepatol. 2021, 75, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Sherman, M.; Bilodeau, M.; Cooper, C.; Mackie, D.; Depew, W.; Villeneuve, J.-P. Liver Disease in Canada: A Crisis in the Making; Canadian Liver Foundation: Toronto, ON, Canada, 2013. [Google Scholar]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Centre for Communicable Diseases and Infection Control. Brief Report: Hepatitis B Infection in Canada; Public Health Agency of Canada: Ottawa, ON, Canada, 2011; pp. 1–13. Available online: http://www.phac-aspc.gc.ca/id-mi/hepatitisBCan-hepatiteBCan-eng.php (accessed on 19 November 2022).
- Binka, M.; Butt, Z.A.; Wong, S.; Chong, M.; A Buxton, J.; Chapinal, N.; Yu, A.; Alvarez, M.; Darvishian, M.; Wong, J.; et al. Differing profiles of people diagnosed with acute and chronic hepatitis B virus infection in British Columbia, Canada. World J. Gastroenterol. 2018, 24, 1216–1227. [Google Scholar] [CrossRef]
- Butt, Z.A.; Wong, S.; Rossi, C.; Binka, M.; Wong, J.; Yu, A.; Darvishian, M.; Alvarez, M.; Chapinal, N.; McKee, G.; et al. Concurrent Hepatitis C and B Virus and Human Immunodeficiency Virus Infections Are Associated With Higher Mortality Risk Illustrating the Impact of Syndemics on Health Outcomes. Open Forum Infect. Dis. 2020, 7, ofaa347. [Google Scholar] [CrossRef] [PubMed]
- Binka, M.; Butt, Z.A.; McKee, G.; Darvishian, M.; Cook, D.; Wong, S.; Yu, A.; Alvarez, M.; Samji, H.; Wong, J.; et al. Differences in risk factors for hepatitis B, hepatitis C, and human immunodeficiency virus infection by ethnicity: A large population-based cohort study in British Columbia, Canada. Int. J. Infect. Dis. 2021, 106, 246–253. [Google Scholar] [CrossRef]
- McKee, G.; Butt, Z.A.; Wong, S.; Salway, T.; Gilbert, M.; Wong, J.; Alvarez, M.; Chapinal, N.; Darvishian, M.; Tyndall, M.W.; et al. Syndemic Characterization of HCV, HBV, and HIV Co-infections in a Large Population Based Cohort Study. eClinicalMedicine 2018, 4–5, 99–108. [Google Scholar] [CrossRef]
- Ong, J.P.; Pitts, A.; Younossi, Z.M. Increased overall mortality and liver-related mortality in non-alcoholic fatty liver disease. J. Hepatol. 2008, 49, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, D.; Deutsch, M. The spectrum of HBV/HCV coinfection: Epidemiology, clinical characteristics, viralinteractions and management. Ann. Gastroenterol. 2015, 28, 221–228. [Google Scholar] [PubMed]
- Zhou, K.; Dodge, J.L.; Grab, J.; Poltavskiy, E.; Terrault, N.A. Mortality in Adults with Chronic Hepatitis B Infection in the United States: A Population-Based Study. Aliment Pharmacol. Ther. 2020, 52, 382–389. [Google Scholar] [CrossRef]
- Piselli, P.; Serraino, D.; Fusco, M.; Girardi, E.; Pirozzi, A.; Toffolutti, F.; Cimaglia, C.; Taborelli, M. Hepatitis C virus infection and risk of liver-related and non-liver-related deaths: A population-based cohort study in Naples, southern Italy. BMC Infect. Dis. 2021, 21, 667. [Google Scholar] [CrossRef]
- Hallager, S.; Ladelund, S.; Christensen, P.B.; Kjær, M.S.; Roege, B.T.; Grønbæk, K.E.; Belard, E.; Barfod, T.S.; Madsen, L.G.; Gerstoft, J.; et al. Liver-related morbidity and mortality in patients with chronic hepatitis C and cirrhosis with and without sustained virologic response. Clin. Epidemiol. 2017, 2017, 501–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brass, V.; Moradpour, D. New insights into hepatitis B and C virus co-infection. J. Hepatol. 2009, 51, 423–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thornton, A.C.; Jose, S.; Bhagani, S.; Chadwick, D.; Dunn, D.; Gilson, R.; Main, J.; Nelson, M.; Rodger, A.; Taylor, C.; et al. Hepatitis B, hepatitis C, and mortality among HIV-positive individuals. AIDS 2017, 31, 2525–2532. [Google Scholar] [CrossRef] [PubMed]
- Haflidadottir, S.; Jonasson, J.G.; Norland, H.; Einarsdottir, S.O.; Kleiner, D.E.; Lund, S.H.; Björnsson, E.S. Long term follow-up and liver-related death rate in patients with non-alcoholic and alcoholic related fatty liver disease. BMC Gastroenterol. 2014, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- Janjua, N.Z.; Kuo, M.; Chong, M.; Yu, A.; Alvarez, M.; Cook, D.; Armour, R.; Aiken, C.; Li, K.; Rizi, S.A.M.; et al. Assessing Hepatitis C Burden and Treatment Effectiveness through the British Columbia Hepatitis Testers Cohort (BC-HTC): Design and Characteristics of Linked and Unlinked Participants. PLoS ONE 2016, 11, e0150176. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). International Classification of Diseases: [9th] Ninth Revision Basic Tabulation List with Alphabetic Index; World Health Organization: Geneva, Switzerland, 1978. Available online: https://apps.who.int/iris/handle/10665/39473 (accessed on 18 October 2021).
- World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), 5th ed.; World Health Organization: Geneva, Switzerland, 2016; Volume 5. [Google Scholar]
- Zhang, Z. Survival analysis in the presence of competing risks. Ann. Transl. Med. 2017, 5, 47. [Google Scholar] [CrossRef]
- British Columbia Ministry of Health, British Columbia Medical Association. Hepatitis—Viral Hepatitis Testing; BC Guideline.ca; Government of British Columbia: Vancouver, BC, Canada, 2012; pp. 1–5.
- Yuen, M.F.; Tanaka, Y.; Fong, D.Y.T.; Fung, J.; Wong, D.K.H.; Yuen, J.C.H.; But, D.Y.K.; Chan, A.O.O.; Wong, B.C.Y.; Mizokami, M.; et al. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. J. Hepatol. 2009, 50, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Pandyarajan, V.; Govalan, R.; Yang, J.D. Risk Factors and Biomarkers for Chronic Hepatitis B Associated Hepatocellular Carcinoma. Int. J. Mol. Sci. 2021, 22, 479. [Google Scholar] [CrossRef] [PubMed]
- Lakha, F.; Gorman, D.R.; Mateos, P. Name analysis to classify populations by ethnicity in public health: Validation of Onomap in Scotland. Public Health 2011, 125, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.; Vernon, S.; Lawrence, G.; Wilson, S. Use of name recognition software, census data and multiple imputation to predict missing data on ethnicity: Application to cancer registry records. BMC Med Informatics Decis. Mak. 2012, 12, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pampalon, R.; Hamel, D.; Gamache, P.; Philibert, M.D.; Raymond, G. Simpson, A. An Area-based Material and Social Deprivation Index for Public Health in Québec and Canada. Can. J. Public Health 2012, 103 (Suppl. S2), 17–22. [Google Scholar] [CrossRef]
- Salway, T.; Butt, Z.A.; Wong, S.; Abdia, Y.; Balshaw, R.; Rich, A.J.; Ablona, A.; Wong, J.; Grennan, T.; Yu, A. A Computable Phenotype Model for Classification of Men Who Have Sex With Men Within a Large Linked Database of Laboratory, Surveillance, and Administrative Healthcare Records. Front Digit. Health 2020, 2, 547324. [Google Scholar] [CrossRef] [PubMed]
- Janjua, N.Z.; Islam, N.; Kuo, M.; Yu, A.; Wong, S.; Butt, Z.A.; Gilbert, M.; Buxton, J.; Chapinal, N.; Samji, H.; et al. Identifying injection drug use and estimating population size of people who inject drugs using healthcare administrative datasets. Int. J. Drug Policy 2018, 55, 31–39. [Google Scholar] [CrossRef] [PubMed]
- British Columbia Office of Provincial Health Officer. HIV Testing Guidelines for the Province of British Columbia; Office of the Provincial Health Officer: Victoria, BC, Canada, 2015; pp. 1–8.
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y. Balance diagnostics after propensity score matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef]
- Austin, P.C. A Tutorial and Case Study in Propensity Score Analysis: An Application to Estimating the Effect of In-Hospital Smoking Cessation Counseling on Mortality. Multivar. Behav. Res. 2011, 46, 119–151. [Google Scholar] [CrossRef]
- Desai, R.J.; Franklin, J.M. Alternative approaches for confounding adjustment in observational studies using weighting based on the propensity score: A primer for practitioners. BMJ 2019, 367, l5657. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Zhang, Z. Model building strategy for logistic regression: Purposeful selection. Ann. Transl. Med. 2016, 4, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Tedrow, K. Natural Language Processing with SAS®: Special Collection; SAS Institute Inc.: Cary, NC, USA, 2018; 473p, Available online: https://github.com/PacktPublishing/Natural-Language-Processing-with-TensorFlow (accessed on 8 December 2021).
- The R Development Core Team. R: A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2017; Volume 2, Available online: https://www.r-project.org/ (accessed on 19 November 2022).
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the Global Burden of Chronic Liver Diseases From 2012 to 2017: The Growing Impact of NAFLD. Hepatology 2020, 72, 1605–1616. [Google Scholar] [CrossRef]
- Golabi, P.; Paik, J.M.; Eberly, K.; de Avila, L.; Alqahtani, S.A.; Younossi, Z.M. Causes of death in patients with Non-alcoholic Fatty Liver Disease (NAFLD), alcoholic liver disease and chronic viral Hepatitis B and C. Ann. Hepatol. 2021, 27, 100556. [Google Scholar] [CrossRef]
- Aspinall, E.J.; Hutchinson, S.J.; Janjua, N.Z.; Grebely, J.; Yu, A.; Alavi, M.; Amin, J.; Goldberg, D.J.; Innes, H.; Law, M.; et al. Trends in mortality after diagnosis of hepatitis C virus infection: An international comparison and implications for monitoring the population impact of treatment. J. Hepatol. 2015, 62, 269–277. [Google Scholar] [CrossRef]
- Choi, H.S.J.; Brouwer, W.P.; Zanjir, W.M.; de Man, R.A.; Feld, J.J.; Hansen, B.E.; Janssen, H.L.A.; Patel, K. Nonalcoholic Steatohepatitis Is Associated With Liver-Related Outcomes and All-Cause Mortality in Chronic Hepatitis B. Hepatology 2020, 71, 539–548. [Google Scholar] [CrossRef]
- Peleg, N.; Issachar, A.; Arbib, O.S.; Cohen-Naftaly, M.; Braun, M.; Leshno, M.; Barsheshet, A.; Shlomai, A. Liver steatosis is a strong predictor of mortality and cancer in chronic hepatitis B regardless of viral load. JHEP Rep. 2019, 1, 9–16. [Google Scholar] [CrossRef]
- Thio, C.L.; Seaberg, E.C.; Skolasky, R., Jr.; Phair, J.; Visscher, B.; Muñoz, A.; Thomas, D.L. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 2002, 360, 1921–1926. [Google Scholar] [CrossRef]
- Alavi, M.; Grebely, J.; Hajarizadeh, B.; Amin, J.; Larney, S.; Law, M.G.; George, J.; Degenhardt, L.; Dore, G.J. Mortality trends among people with hepatitis B and C: A population-based linkage study, 1993-2012. BMC Infect. Dis. 2018, 18, 215. [Google Scholar] [CrossRef]
- Asrani, S.K.; Larson, J.J.; Yawn, B.; Therneau, T.M.; Kim, W.R. Underestimation of Liver-Related Mortality in the United States. Gastroenterology 2013, 145, 375–382.e2. [Google Scholar] [CrossRef]
- Amin, J.; Law, M.G.; Bartlett, M.; Kaldor, J.M.; Dore, G.J. Causes of death after diagnosis of hepatitis B or hepatitis C infection: A large community-based linkage study. Lancet 2006, 368, 938–945. [Google Scholar] [CrossRef]
- Kim, H.; Kisseleva, T.; Brenner, D.A. Aging and liver disease. Curr. Opin. Gastroenterol. 2015, 31, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Pham, A.; Cummings, M.; Lindeman, C.; Drummond, N.; Williamson, T. Recognizing misclassification bias in research and medical practice. Fam. Pract. 2019, 36, 804–807. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall Study Population | Inverse Probability of Treatment Weighted Dataset * | |||||
|---|---|---|---|---|---|---|
| Covariates | HBV Negative (n = 1,105,739) | HBV Positive (n = 45,255) | SMD | HBV Negative (n = 45,255) | HBV Positive (n = 45,255) | SMD |
| Sex (%) | 0.224 | 0.025 | ||||
| Female | 657,289 (55.8) | 20,236 (44.7) | 25,071 (55.4) | 24483 (54.1) | ||
| Male | 488,450 (44.2) | 25,019 (55.3) | 20,183 (44.6) | 20,772 (45.9) | ||
| Age group, years (%) | 0.331 | 0.033 | ||||
| <25 | 257,063 (23.2) | 6021 (13.3) | 10,318 (22.8) | 9820 (21.7) | ||
| 25–34 | 301,363 (27.3) | 10,634 (23.5) | 12,264 (27.1) | 12,174 (26.9) | ||
| 35–44 | 215,920 (19.5) | 12,128 (26.8) | 8960 (19.8) | 9413 (20.8) | ||
| 45–54 | 151,346 (13.7) | 8804 (19.5) | 6290 (13.9) | 6336 (14.0) | ||
| 55–64 | 96,763 (8.8) | 4677 (10.3) | 3982 (8.8) | 3439 (9.0) | ||
| ≥65 | 83,284 (7.5) | 2991 (6.6) | 3394 (7.5) | 3439 (7.6) | ||
| Birth group (%) | 0.496 | 0.055 | ||||
| <1945 | 117,235 (10.6) | 5523 (12.2) | 4842 (10.7) | 5250 (11.6) | ||
| 1945–1964 | 331,100 (29.9) | 21,107 (46.6) | 13,848 (30.6) | 14,572 (32.2) | ||
| 1965–1974 | 217,614 (19.7) | 10,183 (22.5) | 8960 (19.8) | 8870 (19.6) | ||
| ≥1975 | 439,790 (39.8) | 8442 (18.7) | 17,604 (38.9) | 16,563 (36.6) | ||
| Ethnicity (%) | 1.189 | 0.031 | ||||
| Other * | 867,680 (78.5) | 16,933 (37.4) | 34,756 (76.8) | 34,213 (75.6) | ||
| East Asian | 148,383 (13.4) | 26,827 (59.3) | 6924 (15.3) | 7377 (16.3) | ||
| South Asian | 89,676 (8.1) | 1495 (3.3) | 3575 (7.9) | 3666 (8.1) | ||
| Social deprivation (%) | 0.276 | 0.060 | ||||
| Most privileged (Q1) | 243,399 (22.0) | 6975 (15.4) | 8372 (18.5) | 8553 (18.9) | ||
| Q2 | 212,109 (19.2) | 6879 (15.2) | 8101 (17.9) | 8508 (18.8) | ||
| Q3 | 208,340 (18.8) | 8055 (17.8) | 7965 (17.6) | 7648 (16.9) | ||
| Q4 | 220,325 (19.9) | 9970 (22.0) | 9006 (19.9) | 8870 (19.6) | ||
| Most deprived (Q5) | 214,970 (19.4) | 12,654 (28.0) | 11,540 (25.5) | 11,812 (26.1) | ||
| Unknown | 6596 (0.6) | 722 (1.6) | 272 (0.6) | 272 (0.6) | ||
| Material deprivation (%) | 0.183 | 0.024 | ||||
| Most privileged (Q1) | 202,776 (18.3) | 10,326 (22.8) | 9820 (21.7) | 8553 (18.9) | ||
| Q2 | 196,770 (17.8) | 9053 (20.0) | 8598 (19.0) | 8508 (18.8) | ||
| Q3 | 194,886 (17.6) | 7663 (16.9) | 8508 (18.8) | 8644 (19.1) | ||
| Q4 | 221,654 (20.0) | 7650 (16.9) | 9051 (20.0) | 9187 (20.3) | ||
| Most deprived (Q5) | 283,057 (25.6) | 9841 (21.7) | 8960 (19.8) | 9866 (21.8) | ||
| Unknown | 6596 (0.6) | 722 (1.6) | 272 (0.6) | 272 (0.6) | ||
| Hepatitis C virus (yes) (%) | 15,906 (1.4) | 4139 (9.1) | 0.349 | 2869 (26.9) | 1665 (29.9) | 0.066 |
| HIV† (yes) (%) | 3961 (0.4) | 1318 (2.9) | 0.202 | 226 (0.5) | 272 (0.6) | 0.015 |
| Diabetes (yes) (%) | 63,917 (5.8) | 2493 (5.5) | 0.012 | 1655 (15.5) | 887 (15.9) | 0.011 |
| Chronic Kidney Disease (yes) (%) | 5342 (0.5) | 466 (1.0) | 0.063 | 226 (0.5) | 272 (0.6) | 0.010 |
| Hypertension (%) | 132,663 (12.0) | 4403 (9.7) | 0.073 | 5431 (12.0) | 4707 (10.4) | 0.049 |
| Cirrhosis (yes) (%) | 3490 (0.3) | 659 (1.5) | 0.105 | 226 (0.5) | 226 (0.5) | 0.022 |
| Decompensated cirrhosis (yes) (%) | 3576 (0.3) | 450 (1.0) | 0.083 | 181 (0.4) | 181 (0.4) | <0.001 |
| Gay, bisexual and other men who have sex with men (%) | 65,394 (5.9) | 4,013 (8.9) | 0.232 | 2761 (6.1) | 3620 (8.0) | 0.082 |
| History of injection drug use (%) | 28,814 (2.6) | 2318 (5.1) | 0.131 | 1222 (2.7) | 1222 (2.7) | 0.004 |
| Alcohol use disorder (%) | 39,599 (3.6) | 1953 (4.3) | 0.038 | 1629 (3.6) | 1448 (3.2) | 0.022 |
| Non-alcoholic fatty liver disease (%) | 668 (0.1) | 52 (0.1) | 0.018 | 45 (0.1) | 45 (0.1) | 0.003 |
| Overall Study Population | IPW-Dataset ATE ** | |||
|---|---|---|---|---|
| Covariates | asHR | 95%CI | asHR | 95%CI |
| HBV status | ||||
| Negative | Ref | Ref | ||
| Positive | 3.34 | (3.15, 3.53) | 3.24 | (2.99, 3.50) |
| Sex | ||||
| Female | Ref | |||
| Male | 1.52 | (0.21,10.91) | 1.99 | (1.75, 2.28) |
| Age, years | ||||
| <25 | Ref | |||
| 25–34 | 1.46 | (1.19, 1.79) | 1.34 | (0.68, 2.64) |
| 35–44 | 2.89 | (2.33, 3.57) | 2.3 | (1.18, 4.47) |
| 45–54 | 4.93 | (3.97,6.13) | 3.06 | (1.57, 5.97) |
| 55–64 | 7.34 | (5.87, 9.17) | 4.39 | (2.23, 8.66) |
| ≥65 | 10.32 | (8.20, 13.0) | 6.08 | (3.05, 12.09) |
| Birth group | ||||
| <1945 | Ref | |||
| 1945–1964 | 0.68 | (0.64, 0.73) | 0.49 | (0.41, 0.58) |
| 1965–1974 | 0.27 | (0.24, 0.31) | 0.23 | (0.16, 0.33) |
| ≥1975 | 0.12 | (0.10, 0.15) | 0.12 | (0.06, 0.24) |
| Ethnicity | ||||
| East Asian | Ref | |||
| South Asian | 1.24 | (1.11, 1.38) | 1.62 | (1.46, 1.78) |
| Other *** | 2.03 | (1.90, 2.16) | 0.93 | (0.70, 1.24) |
| Material deprivation | ||||
| Most privileged(Q1) | Ref | |||
| Q2 | 1.26 | (1.18, 1.35) | 1.13 | (0.92, 1.40) |
| Q3 | 1.26 | (1.18, 1.35) | 1.03 | (0.84, 1.27) |
| Q4 | 1.34 | (1.26, 1.43) | 1.21 | (0.99, 1.47) |
| Most deprived(Q5) | 1.49 | (1.40, 1.57) | 1.28 | (1.06, 1.54) |
| unknown | 1.46 | (1.20, 1.77) | 1.3 | (0.87, 1.95) |
| HCV status | ||||
| Negative | Ref | |||
| Positive | 3.68 | (3.45, 3.93) | 3.33 | (2.96, 3.76) |
| Diabetes | ||||
| No | Ref | |||
| Yes | 1.68 | (1.59, 1.77) | 1.86 | (1.58, 2.20) |
| Chronic Kidney Disease | ||||
| No | Ref | |||
| Yes | 1 | (0.84,1.18) | 0.99 | (0.67, 1.48) |
| Injection Drug Use | ||||
| No | Ref | |||
| Yes | 1.17 | (1.06,1.27) | 1.12 | (0.88, 1.41) |
| Alcohol use disorder | ||||
| No | Ref | |||
| Yes | 3.58 | (3.38, 3.80) | 2.56 | (2.13, 3.07) |
| Non-alcoholic fatty liver disease | ||||
| No | Ref | |||
| Yes | 4.31 | (3.32, 5.61) | 3.53 | (2.11, 5.91) |
| Overall Study Population | IPW-Dataset ** ATE | |||
|---|---|---|---|---|
| Covariates | asHR | 95%CI | asHR | 95%CI |
| HBV and NAFL status | ||||
| HBV Negative without NAFLD | Ref | Ref | ||
| HBV Negative with NAFLD | 4.49 | (3.35, 6.02) | 4.52 | (3.33, 6.12) |
| HBV positive without NAFLD | 3.35 | (3.16, 3.55) | 3.32 | (3.13, 3.53) |
| HBV positive with NAFLD | 12.5 | (7.08, 22.07) | 12.08 | (5.87, 24.89) |
| HBV and HCV status | ||||
| HBV Negative without HCV | Ref | |||
| HBV Negative with HCV | 4.69 | (4.37, 5.03) | 4.82 | (4.48, 5.19) |
| HBV positive without HCV | 4.36 | (4.09, 4.64) | 4.3 | (4.04, 4.57) |
| HBV positive with HCV | 8.4 | (7.62, 9.26) | 8.66 | (7.77, 9.64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makuza, J.D.; Jeong, D.; Binka, M.; Adu, P.A.; Cua, G.; Yu, A.; Velásquez García, H.A.; Alvarez, M.; Wong, S.; Bartlett, S.; et al. Impact of Hepatitis B Virus Infection, Non-alcoholic Fatty Liver Disease, and Hepatitis C Virus Co-infection on Liver-Related Death among People Tested for Hepatitis B Virus in British Columbia: Results from a Large Longitudinal Population-Based Cohort Study. Viruses 2022, 14, 2579. https://doi.org/10.3390/v14112579
Makuza JD, Jeong D, Binka M, Adu PA, Cua G, Yu A, Velásquez García HA, Alvarez M, Wong S, Bartlett S, et al. Impact of Hepatitis B Virus Infection, Non-alcoholic Fatty Liver Disease, and Hepatitis C Virus Co-infection on Liver-Related Death among People Tested for Hepatitis B Virus in British Columbia: Results from a Large Longitudinal Population-Based Cohort Study. Viruses. 2022; 14(11):2579. https://doi.org/10.3390/v14112579
Chicago/Turabian StyleMakuza, Jean Damascene, Dahn Jeong, Mawuena Binka, Prince Asumadu Adu, Georgine Cua, Amanda Yu, Héctor Alexander Velásquez García, Maria Alvarez, Stanley Wong, Sofia Bartlett, and et al. 2022. "Impact of Hepatitis B Virus Infection, Non-alcoholic Fatty Liver Disease, and Hepatitis C Virus Co-infection on Liver-Related Death among People Tested for Hepatitis B Virus in British Columbia: Results from a Large Longitudinal Population-Based Cohort Study" Viruses 14, no. 11: 2579. https://doi.org/10.3390/v14112579