
A Polymorphism in the TMPRSS2 Gene Increases the Risk of Death in Older Patients Hospitalized with COVID-19
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. DNA Extraction and Genotyping
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
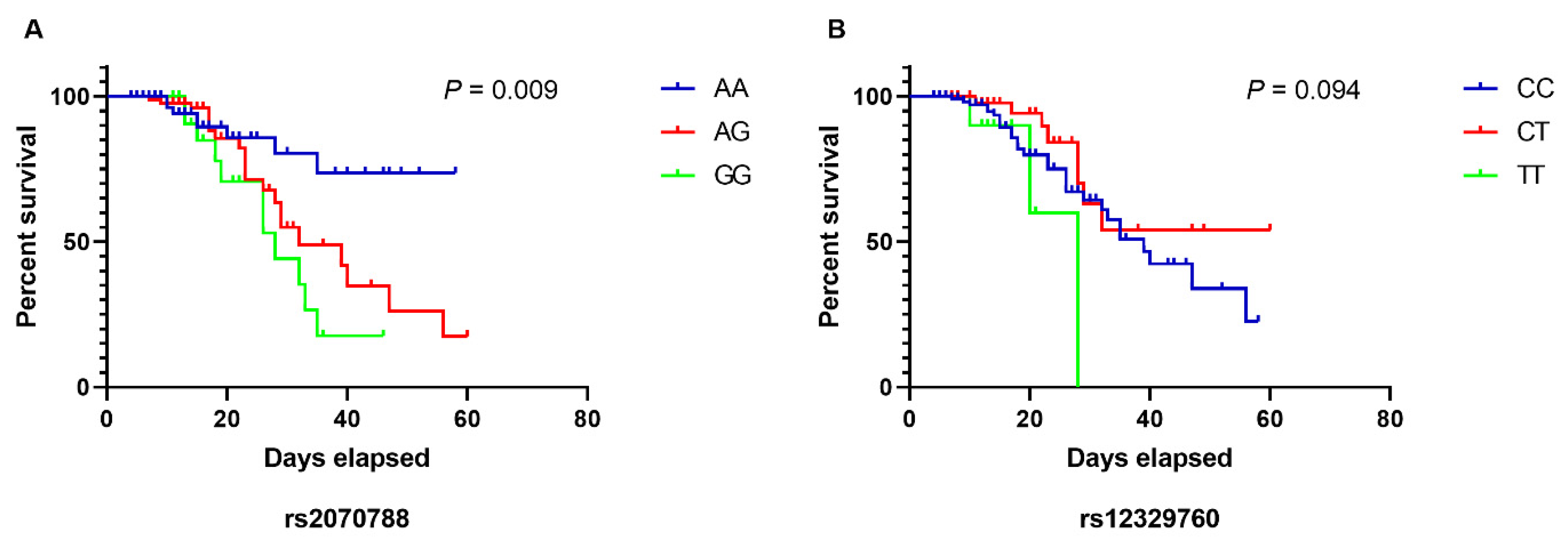
3.2. Influence of the TMPRSS2 Polymorphisms on the Risk of Death
3.3. Multivariable Analysis to Identify Predictors of Death in Older Individuals
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating Excess Mortality Due to the COVID-19 Pandemic: A Systematic Analysis of COVID-19-Related Mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, C.; Bhattacharya, M.; Sharma, A.R. Present Variants of Concern and Variants of Interest of Severe Acute Respiratory Syndrome Coronavirus 2: Their Significant Mutations in S-Glycoprotein, Infectivity, Re-Infectivity, Immune Escape and Vaccines Activity. Rev. Med. Virol. 2022, 32, e2270. [Google Scholar] [CrossRef]
- Lin, L.; Liu, Y.; Tang, X.; He, D. The Disease Severity and Clinical Outcomes of the SARS-CoV-2 Variants of Concern. Front. Public Health 2021, 9, 1929. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk Factors for Severe and Critically Ill COVID-19 Patients: A Review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-Related Risk Factors of COVID-19: A Systematic Review and Meta-Analysis of 42 Studies and 423,117 Patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Niemi, M.E.K.; Karjalainen, J.; Liao, R.G.; Neale, B.M.; Daly, M.; Ganna, A.; Pathak, G.A.; Andrews, S.J.; Kanai, M.; Veerapen, K.; et al. Mapping the Human Genetic Architecture of COVID-19. Nature 2021, 600, 472–477. [Google Scholar] [CrossRef]
- Pairo-Castineira, E.; Clohisey, S.; Klaric, L.; Bretherick, A.D.; Rawlik, K.; Pasko, D.; Walker, S.; Parkinson, N.; Fourman, M.H.; Russell, C.D.; et al. Genetic Mechanisms of Critical Illness in COVID-19. Nature 2020, 591, 92–98. [Google Scholar] [CrossRef]
- Shulla, A.; Heald-Sargent, T.; Subramanya, G.; Zhao, J.; Perlman, S.; Gallagher, T. A Transmembrane Serine Protease Is Linked to the Severe Acute Respiratory Syndrome Coronavirus Receptor and Activates Virus Entry. J. Virol. 2011, 85, 873–882. [Google Scholar] [CrossRef] [Green Version]
- Bertram, S.; Dijkman, R.; Habjan, M.; Heurich, A.; Gierer, S.; Glowacka, I.; Welsch, K.; Winkler, M.; Schneider, H.; Hofmann-Winkler, H.; et al. TMPRSS2 Activates the Human Coronavirus 229E for Cathepsin-Independent Host Cell Entry and Is Expressed in Viral Target Cells in the Respiratory Epithelium. J. Virol. 2013, 87, 6150–6160. [Google Scholar] [CrossRef]
- Matsuyama, S.; Nagata, N.; Shirato, K.; Kawase, M.; Takeda, M.; Taguchi, F. Efficient Activation of the Severe Acute Respiratory Syndrome Coronavirus Spike Protein by the Transmembrane Protease TMPRSS2. J. Virol. 2010, 84, 12658–12664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell Entry Mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef] [PubMed]
- Zipeto, D.; da Palmeira, J.F.; Argañaraz, G.A.; Argañaraz, E.R. ACE2/ADAM17/TMPRSS2 Interplay May Be the Main Risk Factor for COVID-19. Front. Immunol. 2020, 11, 2642. [Google Scholar] [CrossRef] [PubMed]
- Paoloni-Giacobino, A.; Chen, H.; Peitsch, M.C.; Rossier, C.; Antonarakis, S.E. Cloning of the TMPRSS2 Gene, Which Encodes a Novel Serine Protease with Transmembrane, LDLRA, and SRCR Domains and Maps to 21q22.3. Genomics 1997, 44, 309–320. [Google Scholar] [CrossRef]
- Cheng, Z.; Zhou, J.; To, K.K.W.; Chu, H.; Li, C.; Wang, D.; Yang, D.; Zheng, S.; Hao, K.; Bossé, Y.; et al. Identification of TMPRSS2 as a Susceptibility Gene for Severe 2009 Pandemic A(H1N1) Influenza and A(H7N9) Influenza. J. Infect. Dis. 2015, 212, 1214–1221. [Google Scholar] [CrossRef] [Green Version]
- Paniri, A.; Hosseini, M.M.; Akhavan-Niaki, H. First Comprehensive Computational Analysis of Functional Consequences of TMPRSS2 SNPs in Susceptibility to SARS-CoV-2 among Different Populations. J. Biomol. Struct. Dyn. 2020, 39, 3576–3593. [Google Scholar] [CrossRef]
- Barash, A.; Machluf, Y.; Ariel, I.; Dekel, Y. The Pursuit of COVID-19 Biomarkers: Putting the Spotlight on ACE2 and TMPRSS2 Regulatory Sequences. Front. Med. 2020, 7, 712. [Google Scholar] [CrossRef]
- Asselta, R.; Paraboschi, E.M.; Mantovani, A.; Duga, S. ACE2 and TMPRSS2 Variants and Expression as Candidates to Sex and Country Differences in COVID-19 Severity in Italy. Aging 2020, 12, 10087–10098. [Google Scholar] [CrossRef]
- Hou, Y.; Zhao, J.; Martin, W.; Kallianpur, A.; Chung, M.K.; Jehi, L.; Sharifi, N.; Erzurum, S.; Eng, C.; Cheng, F. New Insights into Genetic Susceptibility of COVID-19: An ACE2 and TMPRSS2 Polymorphism Analysis. BMC Med. 2020, 18, 216. [Google Scholar] [CrossRef]
- Irham, L.M.; Chou, W.H.; Calkins, M.J.; Adikusuma, W.; Hsieh, S.L.; Chang, W.C. Genetic Variants That Influence SARS-CoV-2 Receptor TMPRSS2 Expression among Population Cohorts from Multiple Continents. Biochem. Biophys. Res. Commun. 2020, 529, 263–269. [Google Scholar] [CrossRef] [PubMed]
- David, A.; Parkinson, N.; Peacock, T.P.; Pairo-Castineira, E.; Khanna, T.; Cobat, A.; Tenesa, A.; Sancho-Shimizu, V.; Casanova, J.L.; Abel, L.; et al. A Common TMPRSS2 Variant Has a Protective Effect against Severe COVID-19. Curr. Res. Transl. Med. 2022, 70, 103333. [Google Scholar] [CrossRef] [PubMed]
- Wulandari, L.; Hamidah, B.; Pakpahan, C.; Damayanti, N.S.; Kurniati, N.D.; Adiatmaja, C.O.; Wigianita, M.R.; Soedarsono; Husada, D.; Tinduh, D.; et al. Initial Study on TMPRSS2 p.Val160Met Genetic Variant in COVID-19 Patients. Hum. Genom. 2021, 15, 29. [Google Scholar] [CrossRef]
- Rokni, M.; Heidari Nia, M.; Sarhadi, M.; Mirinejad, S.; Sargazi, S.; Moudi, M.; Saravani, R.; Rahdar, S.; Kargar, M. Association of TMPRSS2 Gene Polymorphisms with COVID-19 Severity and Mortality: A Case-Control Study with Computational Analyses. Appl. Biochem. Biotechnol. 2022, 194, 3507–3526. [Google Scholar] [CrossRef]
- Schuler, B.A.; Habermann, A.C.; PLoSa, E.J.; Taylor, C.J.; Jetter, C.; Negretti, N.M.; Kapp, M.E.; Benjamin, J.T.; Gulleman, P.; Nichols, D.S.; et al. Age-Determined Expression of Priming Protease TMPRSS2 and Localization of SARS-CoV-2 in Lung Epithelium. J. Clin. Investig. 2021, 131, e140766. [Google Scholar] [CrossRef] [PubMed]
- Naslavsky, M.S.; Scliar, M.O.; Yamamoto, G.L.; Wang, J.Y.T.; Zverinova, S.; Karp, T.; Nunes, K.; Ceroni, J.R.M.; de Carvalho, D.L.; da Silva Simões, C.E.; et al. Whole-Genome Sequencing of 1,171 Elderly Admixed Individuals from Brazil. Nat. Commun. 2022, 13, 1004. [Google Scholar] [CrossRef]
- Auton, A.; Abecasis, G.R.; Altshuler, D.M.; Durbin, R.M.; Bentley, D.R.; Chakravarti, A.; Clark, A.G.; Donnelly, P.; Eichler, E.E.; Flicek, P.; et al. A Global Reference for Human Genetic Variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Akin, S.; Schriek, P.; Van Nieuwkoop, C.; Neuman, R.I.; Meynaar, I.; Van Helden, E.J.; El Bouazzaoui, H.; Baak, R.; Veuger, M.; Mairuhu, R.A.T.A.; et al. A Low Aldosterone/Renin Ratio and High Soluble ACE2 Associate with COVID-19 Severity. J. Hypertens. 2022, 40, 606–614. [Google Scholar] [CrossRef]
- Schönfelder, K.; Breuckmann, K.; Elsner, C.; Dittmer, U.; Fistera, D.; Herbstreit, F.; Risse, J.; Schmidt, K.; Sutharsan, S.; Taube, C.; et al. Transmembrane Serine Protease 2 Polymorphisms and Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Type 2 Infection: A German Case-Control Study. Front. Genet. 2021, 12, 667231. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W.; et al. A Crucial Role of Angiotensin Converting Enzyme 2 (ACE2) in SARS Coronavirus–Induced Lung Injury. Nat. Med. 2005, 11, 875. [Google Scholar] [CrossRef]
- Heurich, A.; Hofmann-Winkler, H.; Gierer, S.; Liepold, T.; Jahn, O.; Pöhlmann, S. TMPRSS2 and ADAM17 Cleave ACE2 Differentially and Only Proteolysis by TMPRSS2 Augments Entry Driven by the Severe Acute Respiratory Syndrome Coronavirus Spike Protein. J. Virol. 2014, 88, 1293–1307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 Entry into Cells. Nat. Rev. Mol. Cell Biol. 2021, 23, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Posadas-Sánchez, R.; Fragoso, J.M.; Sánchez-Muñoz, F.; Rojas-Velasco, G.; Ramírez-Bello, J.; López-Reyes, A.; Martínez-Gómez, L.E.; Sierra-Fernández, C.; Rodríguez-Reyna, T.; Regino-Zamarripa, N.E.; et al. Association of the Transmembrane Serine Protease-2 (TMPRSS2) Polymorphisms with COVID-19. Viruses 2022, 14, 1976. [Google Scholar] [CrossRef]
- Vitello, G.A.; Federico, C.; Bruno, F.; Vinci, M.; Musumeci, A.; Ragalmuto, A.; Sturiale, V.; Brancato, D.; Calì, F.; Saccone, S. Allelic Variations in the Human Genes TMPRSS2 and CCR5, and the Resistance to Viral Infection by SARS-CoV-2. Int. J. Mol. Sci. 2022, 23, 9171. [Google Scholar] [CrossRef]
- Monticelli, M.; Mele, B.H.; Benetti, E.; Fallerini, C.; Baldassarri, M.; Furini, S.; Frullanti, E.; Mari, F.; Andreotti, G.; Cubellis, M.V.; et al. Protective Role of a Tmprss2 Variant on Severe COVID-19 Outcome in Young Males and Elderly Women. Genes 2021, 12, 596. [Google Scholar] [CrossRef] [PubMed]
- Ravikanth, V.; Sasikala, M.; Naveen, V.; Latha, S.S.; Parsa, K.V.L.; Vijayasarathy, K.; Amanchy, R.; Avanthi, S.; Govardhan, B.; Rakesh, K.; et al. A Variant in TMPRSS2 Is Associated with Decreased Disease Severity in COVID-19. Meta Gene 2021, 29, 100930. [Google Scholar] [CrossRef]
- Abdelsattar, S.; Kasemy, Z.A.; Ewida, S.F.; Abo-Elsoud, R.A.A.; Zytoon, A.A.; Abdelaal, G.A.; Abdelgawad, A.S.; Khalil, F.O.; Kamel, H.F.M. ACE2 and TMPRSS2 SNPs as Determinants of Susceptibility to, and Severity of, a COVID-19 Infection. Br. J. Biomed. Sci. 2022, 79, 10238. [Google Scholar] [CrossRef]
- Sabino, E.C.; Buss, L.F.; Carvalho, M.P.S.; Prete, C.A.; Crispim, M.A.E.; Fraiji, N.A.; Pereira, R.H.M.; Parag, K.V.; da Silva Peixoto, P.; Kraemer, M.U.G.; et al. Resurgence of COVID-19 in Manaus, Brazil, despite High Seroprevalence. Lancet 2021, 397, 452–455. [Google Scholar] [CrossRef]
- The 1000 Genomes Project Consortium. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar]


{kind=link}
| Variables | Survived (n = 341) | Deceased (n = 61) | p Value |
|---|---|---|---|
| Age (mean ± SD) | 51.4 ± 14.3 | 60.4 ± 16.7 | 0.001 |
| Sex | |||
| Male (n, %) | 207 (60.7) | 38 (62.3) | 0.887 |
| Female (n, %) | 134 (39.3) | 23 (37.7) | |
| Comorbidities | |||
| Diabetes (n, %) | 92 (27.1) | 27 (44.3) | 0.009 |
| Hypertension (n, %) | 154 (45.3) | 37 (60.7) | 0.036 |
| Chronic heart disease (n, %) | 6 (1.8) | 5 (8.2) | 0.015 |
| Chronic kidney disease (n, %) | 5 (1.5) | 7 (11.5) | 0.001 |
| Chronic liver disease (n, %) | 0 (0.0) | 1 (1.6) | 0.152 |
| Malignancy (n, %) | 3 (0.9) | 1 (1.6) | 0.485 |
| Asthma (n, %) | 11 (3.2) | 1 (1.6) | 1.000 |
| COPD (n, %) | 12 (3.5) | 5 (8.2) | 0.156 |
| Rheumatic disease (n, %) | 3 (0.9) | 0 (0.0) | 1.000 |
| Obesity (n, %) | 78 (22.9) | 23 (37.7) | 0.024 |
| All (n = 402) | Older Individuals (n = 175) | |||||
|---|---|---|---|---|---|---|
| TMPRSS2 (rs2070788) | Survived (n = 341) | Deceased (n = 61) | p Value | Survived (n = 136) | Deceased (n = 39) | p Value |
| Alleles | n (%) | n (%) | n (%) | n (%) | ||
| A | 407 (59.6) | 59 (48.3) | 0.019 | 171 (62.8) | 36 (46.1) | 0.008 |
| G | 275 (40.3) | 63 (51.6) | 101 (37.1) | 42 (53.8) | ||
| Genotypes | n (%) | n (%) | n (%) | n (%) | ||
| AA | 128 (37.5) | 15 (24.6) | 51 (37.5) | 8 (20.5) | ||
| AG | 151 (44.3) | 29 (47.5) | 0.081 | 69 (50.7) | 20 (51.3) | 0.019 |
| GG | 62 (18.2) | 17 (27.9) | 16 (11.8) | 11 (28.2) | ||
| TMPRSS2 (rs12329760) | ||||||
| Alleles | n (%) | n (%) | n (%) | n (%) | ||
| C | 537 (78.7) | 102 (83.6) | 0.220 | 212 (77.9) | 64 (82.0) | 0.433 |
| T | 145 (21.2) | 20 (16.3) | 60 (22.0) | 14 (17.9) | ||
| Genotypes | n (%) | n (%) | n (%) | n (%) | ||
| CC | 213 (62.5) | 44 (72.1) | 84 (61.8) | 28 (71.8) | ||
| CT | 111 (32.6) | 14 (23.0) | 0.318 | 44 (32.4) | 8 (20.5) | 0.356 |
| TT | 17 (4.9) | 3 (5.0) | 8 (5.9) | 3 (7.7) | ||
| Variables | HR (95% CI) | p Value |
|---|---|---|
| TMPRSS2 (rs2070788) | ||
| AA | Reference | - |
| AG | 2.15 (0.93–4.97) | 0.073 |
| GG | 4.03 (1.49–10.84) | 0.006 |
| Comorbidities | ||
| Chronic heart disease | 3.19 (1.16–8.72) | 0.024 |
| Chronic kidney disease | 5.12 (2.10–12.46) | <0.0001 |
| Obesity | 2.08 (0.98–4.37) | 0.053 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Andrade, C.C.; Silva, A.T.P.; Vasconcelos, L.R.S.; Oliveira, P.R.S.; de Souza, C.D.F.; da Costa Armstrong, A.; do Carmo, R.F. A Polymorphism in the TMPRSS2 Gene Increases the Risk of Death in Older Patients Hospitalized with COVID-19. Viruses 2022, 14, 2557. https://doi.org/10.3390/v14112557
de Andrade CC, Silva ATP, Vasconcelos LRS, Oliveira PRS, de Souza CDF, da Costa Armstrong A, do Carmo RF. A Polymorphism in the TMPRSS2 Gene Increases the Risk of Death in Older Patients Hospitalized with COVID-19. Viruses. 2022; 14(11):2557. https://doi.org/10.3390/v14112557
Chicago/Turabian Stylede Andrade, Clara Caldeira, Ana Tércia Paulo Silva, Luydson Richardson Silva Vasconcelos, Pablo Rafael Silveira Oliveira, Carlos Dornels Freire de Souza, Anderson da Costa Armstrong, and Rodrigo Feliciano do Carmo. 2022. "A Polymorphism in the TMPRSS2 Gene Increases the Risk of Death in Older Patients Hospitalized with COVID-19" Viruses 14, no. 11: 2557. https://doi.org/10.3390/v14112557