
Epidemiology and Clinical Manifestation of West Nile Virus Infections of Equines in Hungary, 2007–2020
 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Sample Collection
2.3. PCR Analysis and Definition of Lineage
2.4. Data Analysis
3. Results
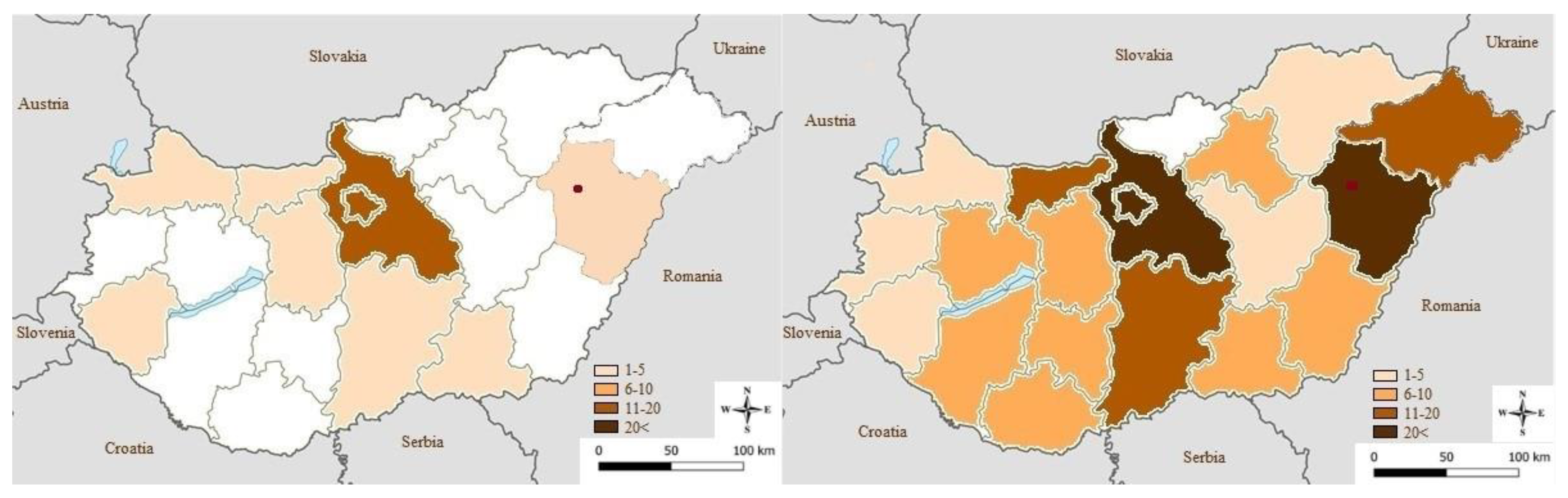
3.1. Geographical Distribution
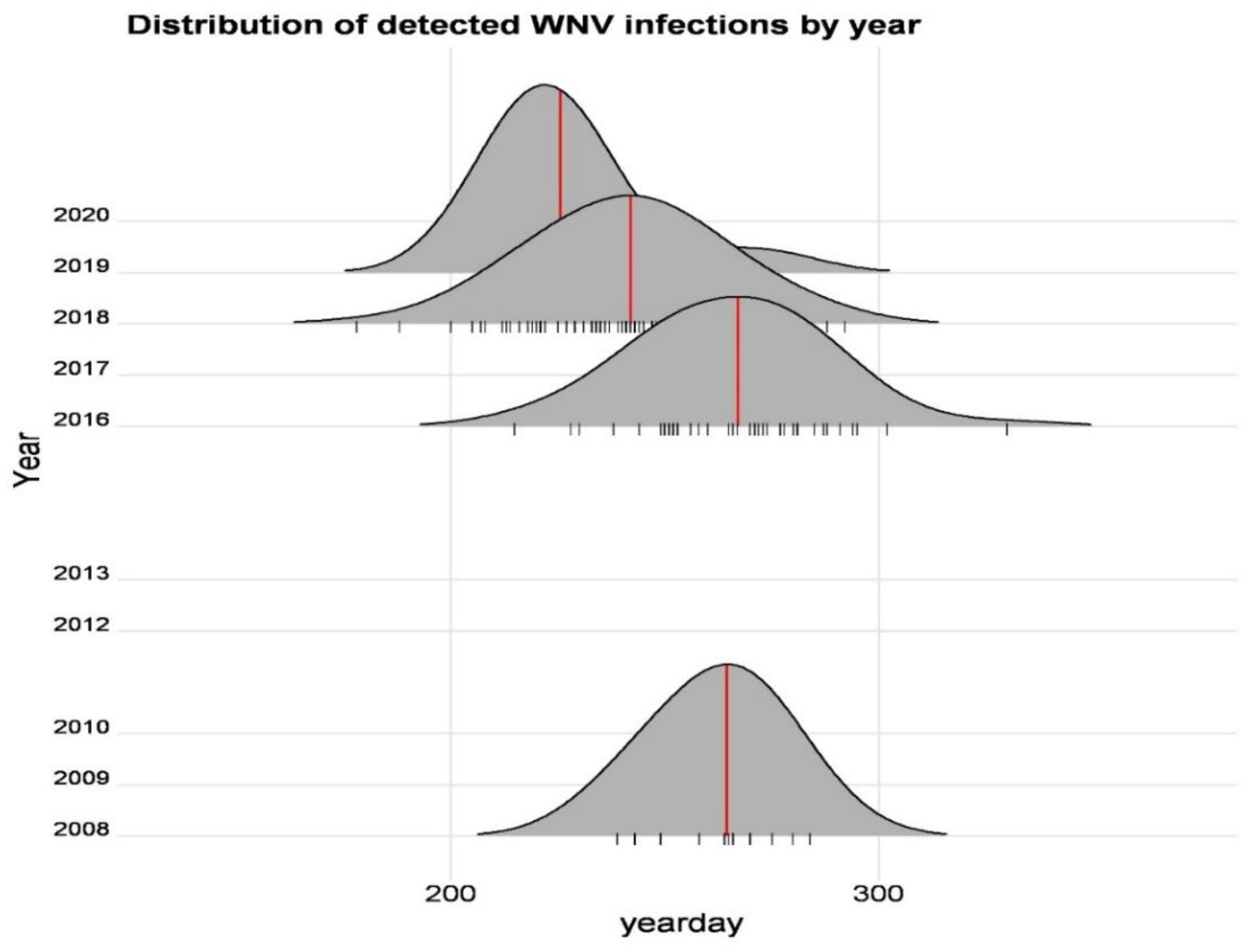
3.2. Temporary Distribution
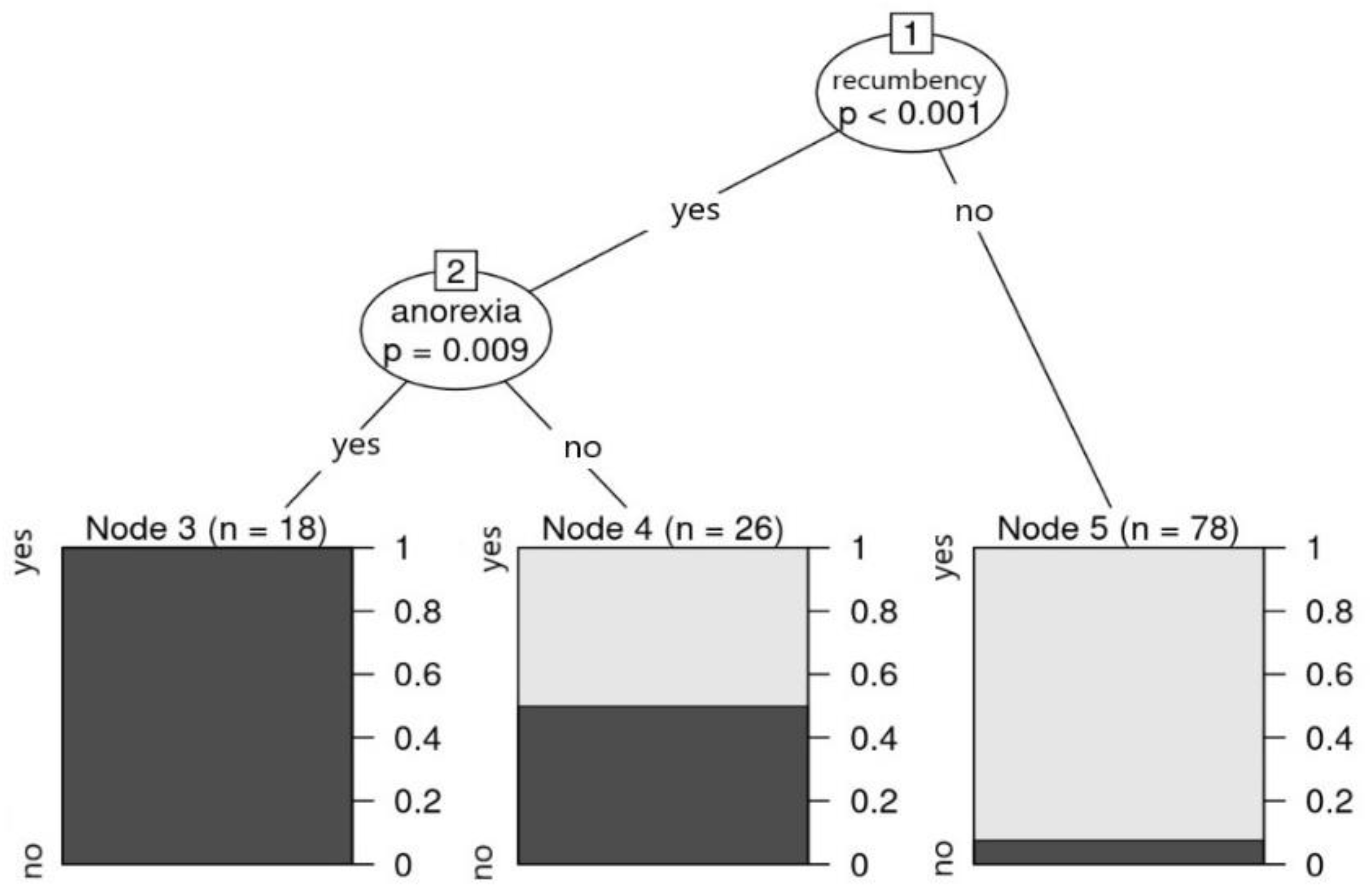
3.3. Clinical Data
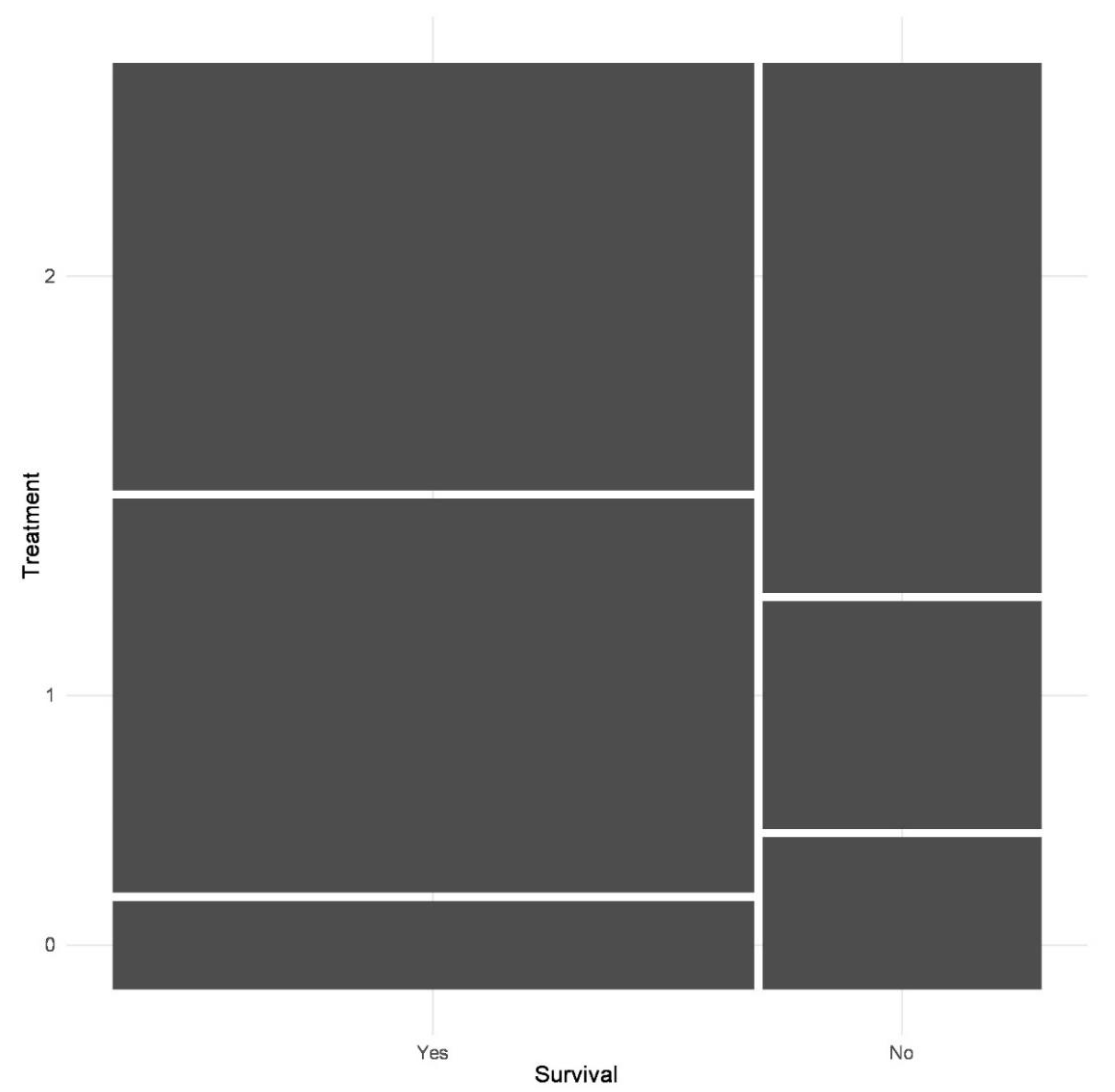
3.4. Treatment
4. Discussion
5. Conclusions
6. Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bakonyi, T.; Hubálek, Z.; Rudolf, I.; Nowotny, N. Novel Flavivirus or New Lineage of West Nile Virus, Central Europe. Emerg. Infect. Dis. 2005, 11, 225–231. [Google Scholar] [CrossRef]
- Bakonyi, T.; Ferenczi, E.; Erdélyi, K.; Kutasi, O.; Csörgő, T.; Seidel, B.; Weissenböck, H.; Brugger, K.; Bán, E.; Nowotny, N. Explosive spread of a neuroinvasive lineage 2 West Nile virus in Central Europe, 2008/2009. Veter-Microbiol. 2013, 165, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Ciota, A.T.; Kramer, L.D. Vector-Virus Interactions and Transmission Dynamics of West Nile Virus. Viruses 2013, 5, 3021–3047. [Google Scholar] [CrossRef] [PubMed]
- Mancini, G.; Montarsi, F.; Calzolari, M.; Capelli, G.; Dottori, M.; Ravagnan, S.; Lelli, D.; Chiari, M.; Santilli, A.; Quaglia, M.; et al. Mosquito species involved in the circulation of West Nile and Usutu viruses in Italy. Vet. Ital. 2017, 53, 97–110. [Google Scholar] [PubMed]
- DeFelice, N.B.; Schneider, Z.D.; Little, E.; Barker, C.; Caillouët, K.A.; Campbell, S.R.; Damian, D.; Irwin, P.; Jones, H.M.P.; Townsend, J.; et al. Use of temperature to improve West Nile virus forecasts. PLoS Comput. Biol. 2018, 14, e1006047. [Google Scholar] [CrossRef] [Green Version]
- Hubálek, Z.; Halouzka, J. West Nile Fever–a Reemerging Mosquito-Borne Viral Disease in Europe. Emerg. Infect. Dis. 1999, 5, 643–650. [Google Scholar] [CrossRef]
- Bakonyi, T.; Ivanics, É.; Erdélyi, K.; Ursu, K.; Ferenczi, E.; Weissenböck, H.; Nowotny, N. Lineage 1 and 2 Strains of Encephalitic West Nile Virus, Central Europe. Emerg. Infect. Dis. 2006, 12, 618–623. [Google Scholar] [CrossRef]
- Calistri, P.; Giovannini, A.; Hubalek, Z.; Ionescu, A.; Monaco, F.; Savini, G.; Lelli, R. Epidemiology of West Nile in Europe and in the Mediterranean Basin~!2009-11-17~!2009-12-11~!2010-04-22~! Open Virol. J. 2010, 4, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Chancey, C.; Grinev, A.; Volkova, E.; Rios, M. The Global Ecology and Epidemiology of West Nile Virus. BioMed Res. Int. 2015, 2015, 376230. [Google Scholar] [CrossRef] [Green Version]
- Kutasi, O.; Bakonyi, T.; Lecollinet, S.; Biksi, I.; Ferenczi, E.; Bahuon, C.; Sardi, S.; Zientara, S.; Szenci, O. Equine Encephalomyelitis Outbreak Caused by a Genetic Lineage 2 West Nile Virus in Hungary. J. Veter-Intern. Med. 2010, 25, 586–591. [Google Scholar] [CrossRef]
- Bouzalas, I.G.; Diakakis, N.; Chaintoutis, S.C.; Brellou, G.D.; Papanastassopoulou, M.; Danis, K.; Vlemmas, I.; Seuberlich, T.; Dovas, C.I. Emergence of Equine West Nile Encephalitis in Central Macedonia, Greece, 2010. Transbound. Emerg. Dis. 2016, 63, e219–e227. [Google Scholar] [CrossRef] [PubMed]
- Hernã¡ndez-Triana, L.M.; Jeffries, C.L.; Mansfield, K.L.; Carnell, G.; Fooks, A.R.; Johnson, N. Emergence of West Nile Virus Lineage 2 in Europe: A Review on the Introduction and Spread of a Mosquito-Borne Disease. Front. Public Health 2014, 2, 271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savini, G.; Capelli, G.; Monaco, F.; Polci, A.; Russo, F.; Di Gennaro, A.; Marini, V.; Teodori, L.; Montarsi, F.; Pinoni, C.; et al. Evidence of West Nile virus lineage 2 circulation in Northern Italy. Veter-Microbiol. 2012, 158, 267–273. [Google Scholar] [CrossRef] [PubMed]
- de Heus, P.; Kolodziejek, J.; Camp, J.V.; Dimmel, K.; Bagó, Z.; Hubálek, Z.; van den Hoven, R.; Cavalleri, J.-M.V.; Nowotny, N. Emergence of West Nile virus lineage 2 in Europe: Characteristics of the first seven cases of West Nile neuroinvasive disease in horses in Austria. Transbound. Emerg. Dis. 2020, 67, 1189–1197. [Google Scholar] [CrossRef] [Green Version]
- Beck, C.; Goffart, I.L.; Franke, F.; Gonzalez, G.; Dumarest, M.; Lowenski, S.; Blanchard, Y.; Lucas, P.; Lamballerie, X.; Grard, G.; et al. Contrasted Epidemiological Patterns of West Nile Virus Lineages 1 and 2 Infections in France from 2015 to 2019. Pathogens 2020, 9, 908. [Google Scholar] [CrossRef]
- Ziegler, U.; Lühken, R.; Keller, M.; Cadar, D.; van der Grinten, E.; Michel, F.; Albrecht, K.; Eiden, M.; Rinder, M.; Lachmann, L.; et al. West Nile virus epizootic in Germany, 2018. Antivir. Res. 2018, 162, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Bakonyi, T.; Haussig, J.M. West Nile virus keeps on moving up in Europe. Eurosurveillance 2020, 25, 2001938. [Google Scholar] [CrossRef]
- ECDC. Historical Data by Year-West Nile Fever Seasonal Surveillance. Available online: https://www.ecdc.europa.eu/en/west-nile-fever/surveillance-and-disease-data/historical (accessed on 21 December 2021).
- Popescu, C.P.; Florescu, S.A.; Ruta, S.M. West Nile virus in Central Europe—Pandora’s box is wide open! Travel Med. Infect. Dis. 2020, 37, 101864. [Google Scholar] [CrossRef]
- Vlaskamp, D.R.; Thijsen, S.F.; Reimerink, J.; Hilkens, P.; Bouvy, W.H.; E Bantjes, S.; Vlaminckx, B.J.; Zaaijer, H.; Kerkhof, H.H.V.D.; Raven, S.F.; et al. First autochthonous human West Nile virus infections in the Netherlands, July to August 2020. Eurosurveillance 2020, 25, 2001904. [Google Scholar] [CrossRef]
- Joó, K.; Bakonyi, T.; Szenci, O.; Sárdi, S.; Ferenczi, E.; Barna, M.; Malik, P.; Hubalek, Z.; Fehér, O.; Kutasi, O. Comparison of assays for the detection of West Nile virus antibodies in equine serum after natural infection or vaccination. Veter- Immunol. Immunopathol. 2017, 183, 1–6. [Google Scholar] [CrossRef]
- Fehér, O.; Bakonyi, T.; Barna, M.; Nagy, A.; Takács, M.; Szenci, O.; Joó, K.; Sárdi, S.; Korbacska-Kutasi, O. Serum neutralising antibody titres against a lineage 2 neuroinvasive West Nile Virus strain in response to vaccination with an inactivated lineage 1 vaccine in a European endemic area. Veter-Immunol. Immunopathol. 2020, 227, 110087. [Google Scholar] [CrossRef] [PubMed]
- Petersen, L.R.; Roehrig, J.T. West Nile Virus: A Reemerging Global Pathogen. Emerg. Infect. Dis. 2001, 7, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Porter, R.S.; Leblond, A.; Lecollinet, S.; Tritz, P.; Cantile, C.; Kutasi, O.; Zientara, S.; Pradier, S.; Van Galen, G.; Speybroek, N.; et al. Clinical Diagnosis of West Nile Fever in Equids by Classification and Regression Tree (CART) Analysis and Comparative Study of Clinical Appearance in Three European Countries. Transbound. Emerg. Dis. 2011, 58, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Sejvar, J.J. Clinical Manifestations and Outcomes of West Nile Virus Infection. Viruses 2014, 6, 606–623. [Google Scholar] [CrossRef] [Green Version]
- Murgue, B.; Murri, S.; Zientara, S.; Durand, B.; Durand, J.-P.; Zeller, H. West Nile Outbreak in Horses in Southern France, 2000: The Return after 35 Years. Emerg. Infect. Dis. 2001, 7, 692–696. [Google Scholar] [CrossRef]
- Porter, M.B.; Long, M.T.; Getman, L.M.; Giguère, S.; MacKay, R.J.; Lester, G.D.; Alleman, A.R.; Wamsley, H.L.; Franklin, R.P.; Jacks, S.; et al. West Nile Virus encephalomyelitis in horses: 46 cases (2001). J. Am. Veter-Med. Assoc. 2003, 222, 1241–1247. [Google Scholar] [CrossRef]
- Salazar, P.; Traub-Dargatz, J.L.; Morley, P.S.; Wilmot, D.D.; Steffen, D.J.; Cunningham, W.E.; Salman, M.D. Outcome of equids with clinical signs of West Nile virus infection and factors associated with death. J. Am. Veter-Med. Assoc. 2004, 225, 267–274. [Google Scholar] [CrossRef]
- Snook, C.S.; Hyman, S.S.; Del Piero, F.; Palmer, J.E.; Ostlund, E.N.; Barr, B.S.; Desrochers, A.M.; Reilly, L.K. West Nile virus encephalomyelitis in eight horses. J. Am. Veter-Med. Assoc. 2001, 218, 1576–1579. [Google Scholar] [CrossRef]
- Venter, M.; Human, S.; Zaayman, D.; Gerdes, G.H.; Williams, J.H.; Steyl, J.; Leman, P.A.; Paweska, J.T.; Setzkorn, H.; Rous, G.; et al. Lineage 2 West Nile Virus as Cause of Fatal Neurologic Disease in Horses, South Africa. Emerg. Infect. Dis. 2009, 15, 877–884. [Google Scholar] [CrossRef]
- Ward, M.P.; Schuermann, J.A.; Highfield, L.D.; Murray, K.O. Characteristics of an outbreak of West Nile virus encephalomyelitis in a previously uninfected population of horses. Veter-Microbiol. 2006, 118, 255–259. [Google Scholar] [CrossRef]
- Bertram, F.-M.; Thompson, P.N.; Venter, M. Epidemiology and Clinical Presentation of West Nile Virus Infection in Horses in South Africa, 2016–2017. Pathogens 2020, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Snyman, J.; Koekemoer, O.; van Schalkwyk, A.; van Vuren, P.J.; Snyman, L.; Williams, J.; Venter, M. Epidemiology and Genomic Analysis of Equine Encephalosis Virus Detected in Horses with Clinical Signs in South Africa, 2010–2017. Viruses 2021, 13, 398. [Google Scholar] [CrossRef] [PubMed]
- Venter, M.; Pretorius, M.; Fuller, J.A.; Botha, E.; Rakgotho, M.; Stivaktas, V.; Weyer, C.; Romito, M.; Williams, J. West Nile Virus Lineage 2 in Horses and Other Animals with Neurologic Disease, South Africa, 2008–2015. Emerg. Infect. Dis. 2017, 23, 2060–2064. [Google Scholar] [CrossRef]
- El Garch, H.; Minke, J.; Rehder, J.; Richard, S.; Toulemonde, C.E.; Dinic, S.; Andreoni, C.; Audonnet, J.; Nordgren, R.; Juillard, V. A West Nile virus (WNV) recombinant canarypox virus vaccine elicits WNV-specific neutralizing antibodies and cell-mediated immune responses in the horse. Veter-Immunol. Immunopathol. 2008, 123, 230–239. [Google Scholar] [CrossRef]
- OIE Terrestrial Manual. 2018. Chapter 2.1.24. Available online: http://www.oie.int/fileadmin/Home/eng/Health_standards/tahm/2.01.24_WEST_NILE.pdf (accessed on 10 December 2021).
- Beck, C.; Lowenski, S.; Durand, B.; Bahuon, C.; Zientara, S.; Lecollinet, S. Improved reliability of serological tools for the diagnosis of West Nile fever in horses within Europe. PLoS Negl. Trop. Dis. 2017, 11, e0005936. [Google Scholar] [CrossRef]
- Pérez-Ramírez, E.; Cano-Gómez, C.; Llorente, F.; Vodica, A.; Veljović, L.; Toklikishvilli, N.; Sherifi, K.; Sghaier, S.; Omani, A.; Kustura, A.; et al. Evaluation of West Nile Virus Diagnostic Capacities in Veterinary Laboratories of the Mediterranean and Black Sea Regions. Pathogens 2020, 9, 1038. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.B.; Long, M.; Gosche, D.G.; Schott, H.M.; Hines, M.T.; Rossano, M.; Sellon, D.C. Immunoglobulin M–Capture Enzyme-Linked Immunosorbent Assay Testing of Cerebrospinal Fluid and Serum from Horses Exposed to West Nile Virus by Vaccination or Natural Infection. J. Vet. Intern. Med. 2004, 18, 866. [Google Scholar]
- Breiman, L.; Friedman, J.; Olshen, R.A.; Stone, C.J. Classification and Decision Trees, 1st ed.; Routledge: Belmont, Wadsworth, 1984. [Google Scholar] [CrossRef]
- De’ath, G.; Fabricius, K.E. Classification and Regression Trees: A Powerful yet Simple Technique for Ecological Data Analys. Ecology 2000, 81, 3178–3192. [Google Scholar] [CrossRef]
- Trájer, A.; Bede-Fazekas, Á.; Bobvos, J.; Paldy, A. Seasonality and geographical occurrence of West Nile fever and distribution of Asian tiger mosquito. Időjárás. Q. J. Hung. Meteorol. Serv. 2014, 118, 19–40. [Google Scholar]
- Szentpáli-Gavallér, K.; Antal, L.; Tóth, M.; Kemenesi, G.; Soltész, Z.; Dán, Á.; Erdélyi, K.; Bányai, K.; Bálint, Á.; Jakab, F.; et al. Monitoring of West Nile Virus in Mosquitoes Between 2011–2012 in Hungary. Vector-Borne Zoonotic Dis. 2014, 14, 648–655. [Google Scholar] [CrossRef] [Green Version]
- Zana, B.; Erdélyi, K.; Nagy, A.; Mezei, E.; Nagy, O.; Takács, M.; Bakonyi, T.; Forgách, P.; Korbacska-Kutasi, O.; Fehér, O.; et al. Multi-Approach Investigation Regarding the West Nile Virus Situation in Hungary, 2018. Viruses 2020, 12, 123. [Google Scholar] [CrossRef] [PubMed]
- Lecollinet, S.; Pronost, S.; Coulpier, M.; Beck, C.; Gonzalez, G.; Leblond, A.; Tritz, P. Viral Equine Encephalitis, a Growing Threat to the Horse Population in Europe? Viruses 2019, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikkema, R.S.; Schrama, M.; Berg, T.V.D.; Morren, J.; Munger, E.; Krol, L.; van der Beek, J.G.; Blom, R.; Chestakova, I.; van der Linden, A.; et al. Detection of West Nile virus in a common whitethroat (Curruca communis) and Culex mosquitoes in the Netherlands, 2020. Eurosurveillance 2020, 25, 2001704. [Google Scholar] [CrossRef] [PubMed]
- Nagy, A.; Bán, E.; Nagy, O.; Ferenczi, E.; Farkas, Á.; Bányai, K.; Farkas, S.; Takács, M. Detection and sequencing of West Nile virus RNA from human urine and serum samples during the 2014 seasonal period. Arch. Virol. 2016, 161, 1797–1806. [Google Scholar] [CrossRef]
- Paz, S.; Semenza, J.C. Environmental Drivers of West Nile Fever Epidemiology in Europe and Western Asia—A Review. Int. J. Environ. Res. Public Health 2013, 10, 3543–3562. [Google Scholar] [CrossRef] [Green Version]
- Soltész, Z.; Erdélyi, K.; Bakonyi, T.; Barna, M.; Szentpáli-Gavallér, K.; Solt, S.; Horváth, É.; Palatitz, P.; Kotymán, L.; Dán, Á.; et al. West Nile virus host-vector-pathogen interactions in a colonial raptor. Parasites Vectors 2017, 10, 449. [Google Scholar] [CrossRef] [Green Version]
- Swaddle, J.P.; Calos, S.E. Increased Avian Diversity Is Associated with Lower Incidence of Human West Nile Infection: Observation of the Dilution Effect. PLoS ONE 2008, 3, e2488. [Google Scholar] [CrossRef] [Green Version]
- Weese, J.S.; Baird, J.D.; DeLay, J.; Kenney, D.G.; Staempfli, H.R.; Viel, L.; Parent, J.; Smith-Maxie, L.; Poma, R. West Nile virus encephalomyelitis in horses in Ontario: 28 cases. Can. Vet. J. = La Rev. Vet. Can. 2003, 44, 469–473. [Google Scholar]
- Ostlund, E.N.; Crom, R.L.; Pedersen, D.D.; Johnson, D.J.; Williams, W.O.; Schmitt, B.J. Equine West Nile Encephalitis, United States. Emerg. Infect. Dis. 2001, 7, 665–669. [Google Scholar] [CrossRef]
- Wang, H.; Siddharthan, V.; Hall, J.O.; Morrey, J.D. Autonomic Nervous Dysfunction in Hamsters Infected with West Nile Virus. PLoS ONE 2011, 6, e19575. [Google Scholar] [CrossRef] [Green Version]
- Bowen, R.A.; Nordgren, R.; Minke, J.M.; Siger, L.; Rouge, M.M.; Johnson, J.; Karaca, K. Pathogenesis of west nile virus infection in dogs treated with glucocorticoids. Am. J. Trop. Med. Hyg. 2006, 74, 670–673. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | 2007 | 2008 | 2010 | 2012 | 2013 | 2016 | 2017 | 2018 | 2019 | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Examined number of horses (n) | 2 | 16 | 2 | 1 | 4 | 19 | 2 | 72 | 6 | 124 |
| Percentage of cases according to year (%) | 1.6 | 12.9 | 1.6 | 0.8 | 3.2 | 15.3 | 1.6 | 58.1 | 4.8 | 100 |
| Year | 2007 | 2008 | 2009 | 2010 | 2012 | 2013 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 2 | 18 | 1 | 2 | 1 | 4 | 47 | 3 | 109 | 10 | 1 |
| mean (week) | 44 | 38 | 33 | 30 | 40 | 36 | 38 | 35 | 35 | 32 | 38 |
| median (day) | 306.5 | 264.5 | 229 | 213 | 275 | 244 | 267 | 253 | 242 | 225 | 261 |
| first case (day) | 306 | 239 | 229 | 213 | 275 | 213 | 215 | 219 | 178 | 214 | 261 |
| last case (day) | 307 | 284 | 229 | 213 | 275 | 289 | 330 | 253 | 292 | 271 | 261 |
| Clinical Sign | Total Number (n) | Total Percentage (%) | 2008 (n; %) | 2016 (n; %) | 2018 (n; %) | |||
|---|---|---|---|---|---|---|---|---|
| ataxia | 101 | 81.5% | 11/15 | 73.3% | 15/19 | 78.9% | 60/70 | 83.3% |
| lethargy/depression | 77 | 62.1% | 11/14 | 78.6% | 10/19 | 52.6% | 45/72 | 62.5% |
| paresis/weakness | 77 | 62.1% | 10/11 | 90.9% | 8/19 | 42.1% | 47/72 | 65.3% |
| behavior change | 54 | 43.5% | 9/12 | 75.0% | 11/19 | 57.8% | 20/72 | 27.8% |
| anorexia | 51 | 41.1% | 6/14 | 42.9% | 7/19 | 36.8% | 29/72 | 40.3% |
| hyperthermia | 50 | 40.3% | 3/15 | 20.0% | 8/19 | 42.1% | 31/72 | 43.1% |
| muscle fasciculation | 47 | 37.9% | 8/12 | 66.7% | 5/19 | 26.3% | 30/72 | 41.7% |
| recumbence | 44 | 35.5% | 7/12 | 58.3% | 7/19 | 36.8% | 27/72 | 37.5% |
| hyperesthesia | 44 | 35.5% | 5/11 | 45.5% | 6/19 | 31.6% | 27/72 | 37.5% |
| n. facialis paralysis | 25 | 20.2% | 8/13 | 61.5% | 3/19 | 15.7% | 8/71 | 11.3% |
| colic | 21 | 16.9% | 2/15 | 13.3% | 6/19 | 31.6% | 10/72 | 13.9% |
| limb paralysis | 16 | 12.9% | 3/11 | 27.3% | 2/19 | 10.5% | 10/72 | 13.9% |
| lameness | 15 | 12.1% | 0/16 | 0.0% | 8/19 | 42.1% | 4/72 | 5.6% |
| dysphagia | 9 | 7.3% | 1/15 | 6.7% | 1/19 | 5.3% | 4/72 | 5.6% |
| nystagmus | 4 | 3.2% | 0/14 | 0.0% | 0/19 | 0.0% | 2/72 | 2.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fehér, O.E.; Fehérvári, P.; Tolnai, C.H.; Forgách, P.; Malik, P.; Jerzsele, Á.; Wagenhoffer, Z.; Szenci, O.; Korbacska-Kutasi, O. Epidemiology and Clinical Manifestation of West Nile Virus Infections of Equines in Hungary, 2007–2020. Viruses 2022, 14, 2551. https://doi.org/10.3390/v14112551
Fehér OE, Fehérvári P, Tolnai CH, Forgách P, Malik P, Jerzsele Á, Wagenhoffer Z, Szenci O, Korbacska-Kutasi O. Epidemiology and Clinical Manifestation of West Nile Virus Infections of Equines in Hungary, 2007–2020. Viruses. 2022; 14(11):2551. https://doi.org/10.3390/v14112551
Chicago/Turabian StyleFehér, Orsolya Eszter, Péter Fehérvári, Csenge Hanna Tolnai, Petra Forgách, Péter Malik, Ákos Jerzsele, Zsombor Wagenhoffer, Otto Szenci, and Orsolya Korbacska-Kutasi. 2022. "Epidemiology and Clinical Manifestation of West Nile Virus Infections of Equines in Hungary, 2007–2020" Viruses 14, no. 11: 2551. https://doi.org/10.3390/v14112551