
Effect of Previous COVID-19 Vaccination on Humoral Immunity 3 Months after SARS-CoV-2 Omicron Infection and Booster Effect of a Fourth COVID-19 Vaccination 2 Months after SARS-CoV-2 Omicron Infection
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
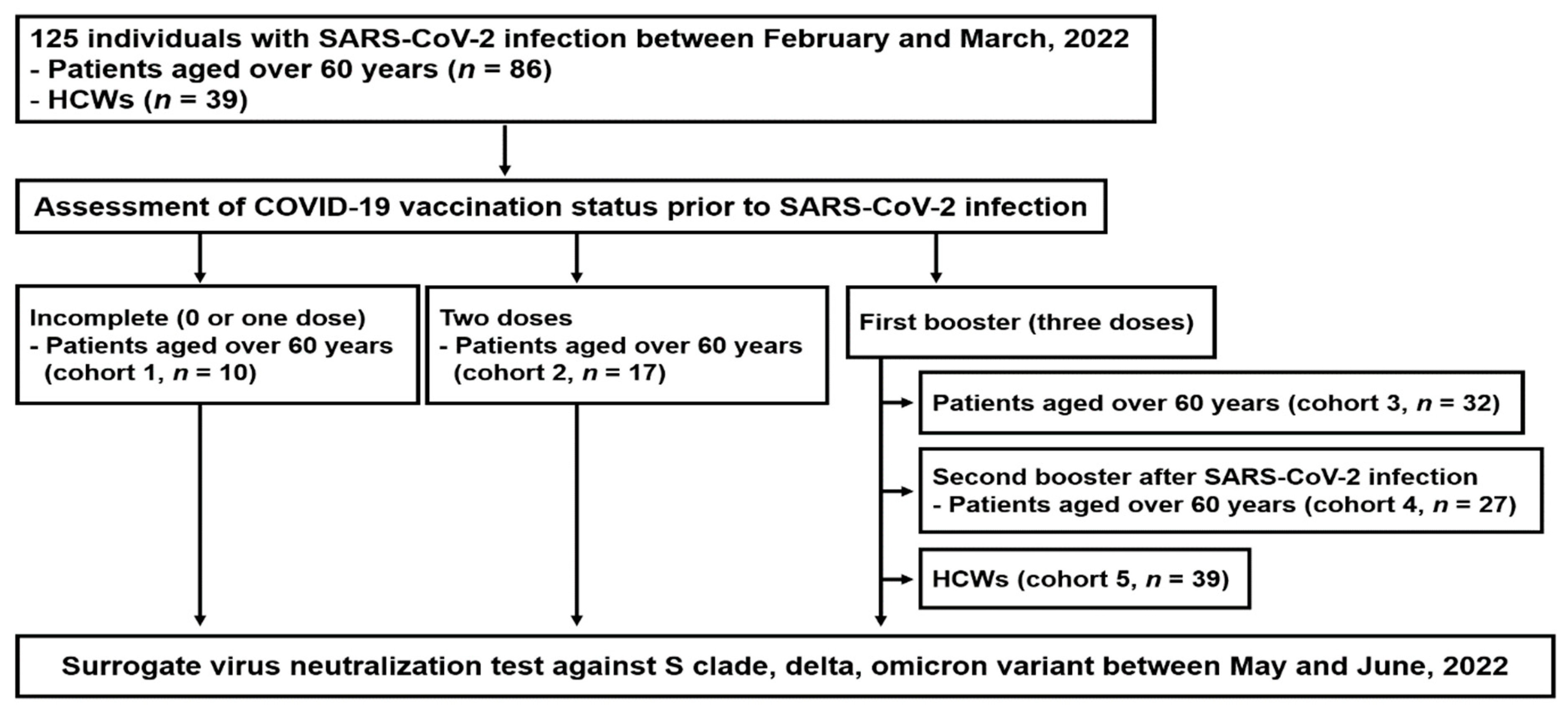
2.1. Study Population and Clinical Data Collection
2.2. Surrogate sVNT
2.3. Statistical Analysis
3. Results
3.1. Enrollment and Baseline Characteristics
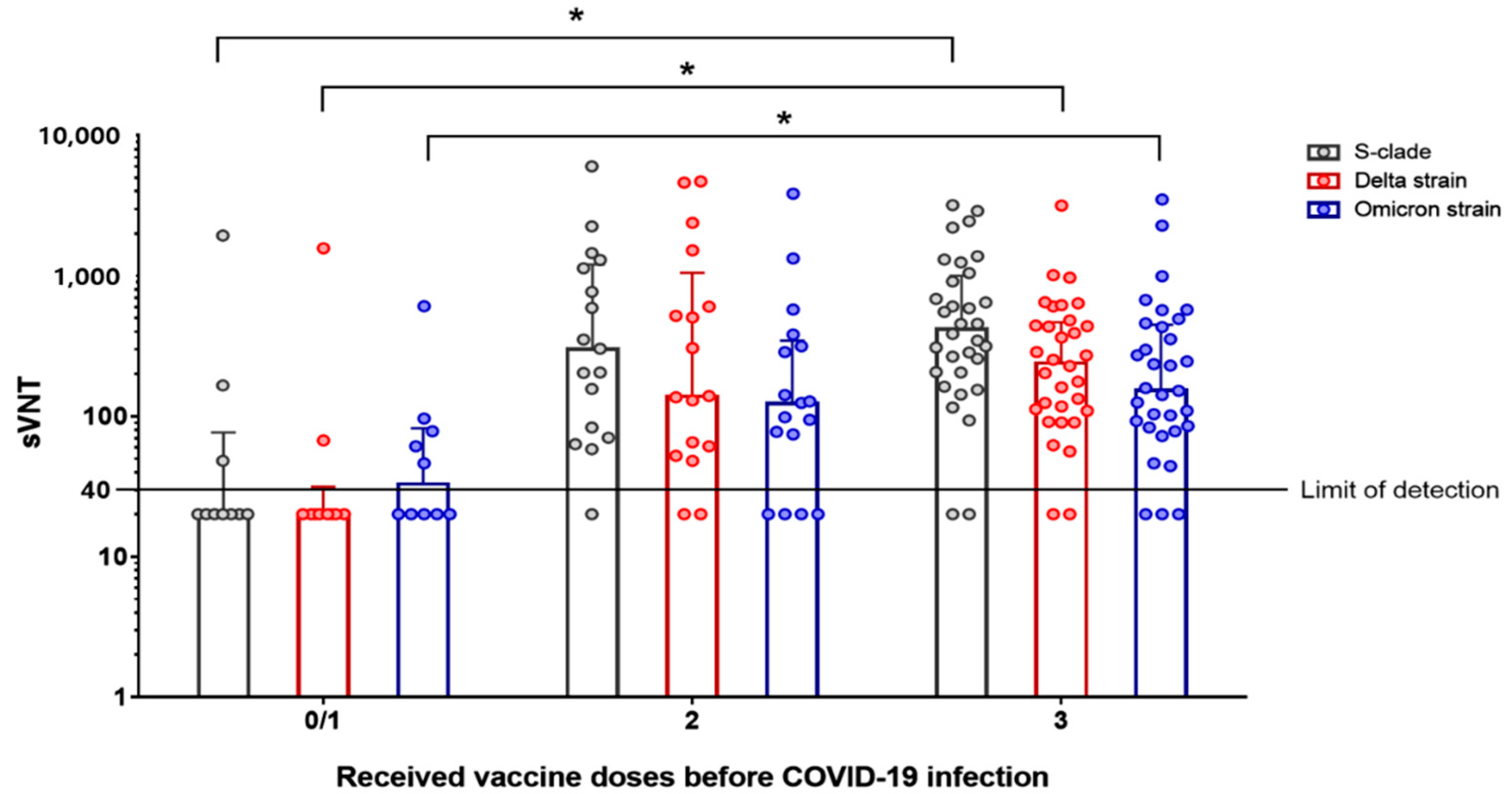
3.2. Surrogate sVNT Results According to Vaccination Status before Omicron Variant Infection
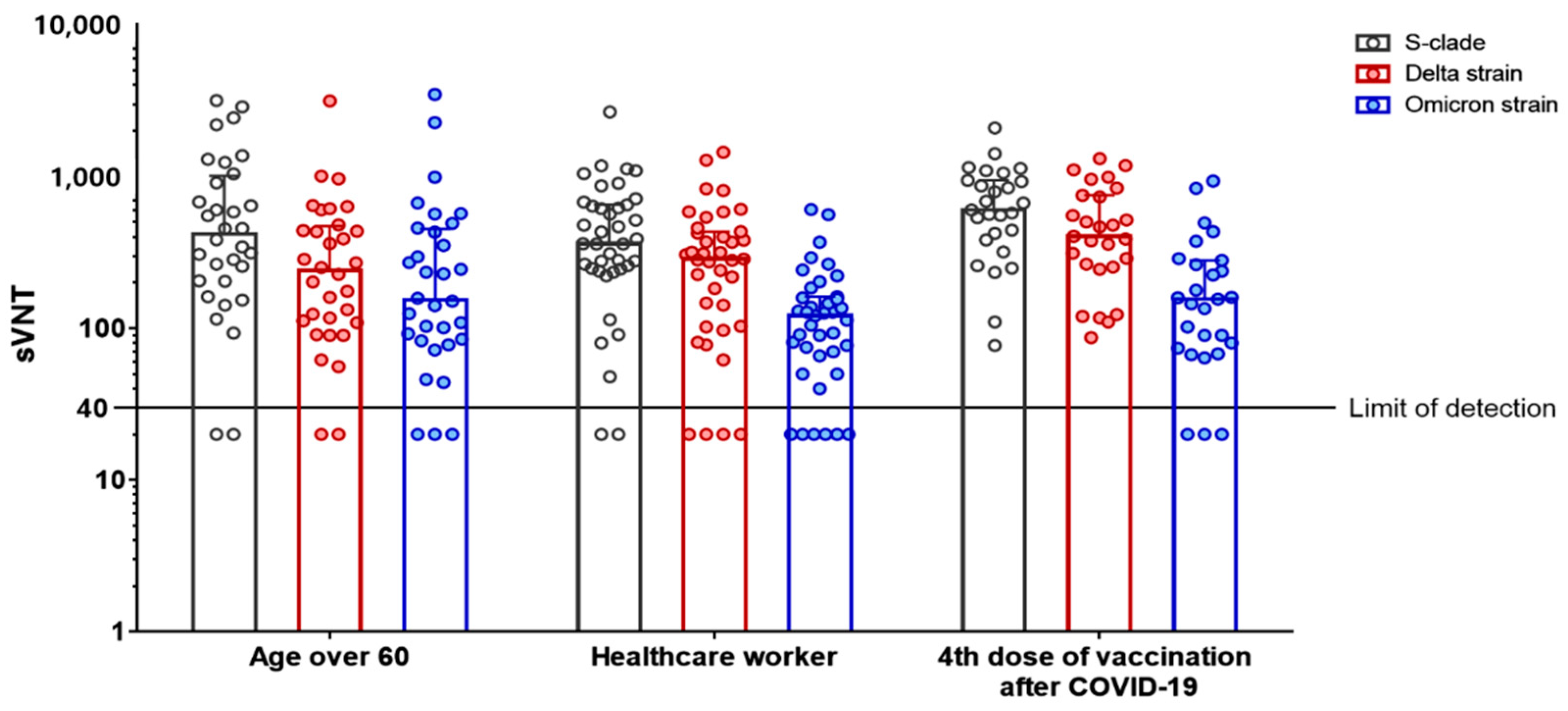
3.3. Surrogate sVNT Results after a Second Booster Vaccination (Fourth Dose) following Omicron Variant Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 10 August 2022).
- Pulliam, J.R.C.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science 2022, 376, eabn4947. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron variant from previous SARS-CoV-2 infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef]
- Hachmann, N.P.; Miller, J.; Collier, A.Y.; Ventura, J.D.; Yu, J.; Rowe, M.; Bondzie, E.A.; Powers, O.; Surve, N.; Hall, K.; et al. Neutralization escape by SARS-CoV-2 omicron subvariants BA.2.12.1, BA.4, and BA.5. N. Engl. J. Med. 2022, 387, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Qu, P.; Faraone, J.; Evans, J.P.; Zou, X.; Zheng, Y.M.; Carlin, C.; Bednash, J.S.; Lozanski, G.; Mallampalli, R.K.; Saif, L.J.; et al. Neutralization of the SARS-CoV-2 Omicron BA.4/5 and BA.2.12.1 subvariants. N. Engl. J. Med. 2022, 386, 2526–2528. [Google Scholar] [CrossRef]
- Wang, Q.; Guo, Y.; Iketani, S.; Nair, M.S.; Li, Z.; Mohri, H.; Wang, M.; Yu, J.; Bowen, A.D.; Chang, J.Y.; et al. Antibody evasion by SARS-CoV-2 Omicron subvariants BA.2.12.1, BA.4 and BA.5. Nature 2022, 608, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Outcomes of SARS-CoV-2 reinfection. Research Square. 2022. [Google Scholar] [CrossRef]
- Sneller, M.C.; Liang, C.J.; Marques, A.R.; Chung, J.Y.; Shanbhag, S.M.; Fontana, J.R.; Raza, H.; Okeke, O.; Dewar, R.L.; Higgins, B.P.; et al. A longitudinal study of COVID-19 sequelae and immunity: Baseline findings. Ann. Intern. Med. 2022, 175, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: https://covid.cdc.gov/covid-data-tracker/#demographics (accessed on 10 August 2022).
- Heesakkers, H.; van der Hoeven, J.G.; Corsten, S.; Janssen, I.; Ewalds, E.; Simons, K.S.; Westerhof, B.; Rettig, T.C.D.; Jacobs, C.; van Santen, S.; et al. Clinical outcomes among patients with 1-year survival following intensive care unit treatment for COVID-19. JAMA 2022, 327, 559–565. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a fourth dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef]
- Muhsen, K.; Maimon, N.; Mizrahi, A.Y.; Boltyansky, B.; Bodenheimer, O.; Diamant, Z.H.; Gaon, L.; Cohen, D.; Dagan, R. Association of receipt of the fourth BNT162b2 dose with omicron infection and COVID-19 hospitalizations among residents of long-term care facilities. JAMA Intern. Med. 2022, 182, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and waning of natural and hybrid immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: A retrospective, total population cohort study in Sweden. Lancet Infect. Dis. 2022, 22, 781–790. [Google Scholar] [CrossRef]
- Hammerman, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Peretz, A.; Netzer, D.; Yaron, S.; Arbel, R. Effectiveness of the BNT162b2 Vaccine after Recovery from Covid-19. N. Engl. J. Med. 2022, 386, 1221–1229. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of previous infection and vaccination on symptomatic Omicron infections. N. Engl. J. Med. 2022, 387, 21–34. [Google Scholar] [CrossRef] [PubMed]
- US Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html (accessed on 10 August 2022).
- World Health Organization. Coronavirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines (accessed on 10 August 2022).
- European Centre for Disease Prevention and Control. Overview of the Implementation of COVID-19 Vaccination Strategies and Deployment Plans in the EU/EEA; European Center for Disease Prevention and Control: Stockholm, Sweden, 2022. [Google Scholar]
- COVID Information Center Israel Ministry of Health. Vaccines. Available online: https://corona.health.gov.il/en/vaccine-for-covid (accessed on 10 August 2022).
- Korea Disease Control and Prevention Agency (KDCA). Outbreak report of COVID-19 during designation of class 1 infectious disease in the Republic of Korea (20 January 2020–24 April 2022). In Public Health Weekly Report (PHWR); Korea Disease Control and Prevention Agency (KDCA): Cheongju, Korea, 2022. [Google Scholar]
- Korea Centers for Disease Control & Prevention. Central Disease Control Headquarters Press Release. 11 August 2022. Available online: http://ncov.mohw.go.kr/tcmBoardView.do?brdId=3&brdGubun=31&dataGubun=&ncvContSeq=6812&contSeq=6812&board_id=312&gubun=ALL (accessed on 10 August 2022).
- Korea Centers for Disease Control & Prevention. Central Disease Control Headquarters Press Release. 13 December 2021. Available online: http://ncov.mohw.go.kr/en/tcmBoardView.do?brdId=12&brdGubun=125&dataGubun=&ncvContSeq=368863&contSeq=368863&board_id=1365&gubun= (accessed on 10 August 2022).
- Perera, R.A.; Mok, C.K.; Tsang, O.T.; Lv, H.; Ko, R.L.; Wu, N.C.; Yuan, M.; Leung, W.S.; Chan, J.M.; Chik, T.S.; et al. Serological assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Eurosurveillance 2020, 25, 2000421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suryawanshi, R.K.; Chen, I.P.; Ma, T.; Syed, A.M.; Brazer, N.; Saldhi, P.; Simoneau, C.R.; Ciling, A.; Khalid, M.M.; Sreekumar, B.; et al. Limited cross-variant immunity from SARS-CoV-2 Omicron without vaccination. Nature 2022, 607, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Medits, I.; Springer, D.N.; Graninger, M.; Camp, J.V.; Höltl, E.; Aberle, S.W.; Traugott, M.T.; Hoepler, W.; Deutsch, J.; Lammel, O.; et al. Different neutralization profiles after primary SARS-CoV-2 Omicron BA.1 and BA.2 infections. Front. Immunol. 2022, 13, 946318. [Google Scholar] [CrossRef]
- Carreño, J.M.; Alshammary, H.; Tcheou, J.; Singh, G.; Raskin, A.J.; Kawabata, H.; Sominsky, L.A.; Clark, J.J.; Adelsberg, D.C.; Bielak, D.A.; et al. Activity of convalescent and vaccine serum against SARS-CoV-2 Omicron. Nature 2022, 602, 682–688. [Google Scholar] [CrossRef]
- Rössler, A.; Knabl, L.; von Laer, D.; Kimpel, J. Neutralization profile after recovery from SARS-CoV-2 Omicron infection. N. Engl. J. Med. 2022, 386, 1764–1766. [Google Scholar] [CrossRef]
- Nevejan, L.; Cuypers, L.; Laenen, L.; Van Loo, L.; Vermeulen, F.; Wollants, E.; Van Hecke, I.; Desmet, S.; Lagrou, K.; Maes, P.; et al. Early SARS-CoV-2 reinfections within 60 days and implications for retesting policies. Emerg. Infect. Dis. 2022, 28, 1729–1731. [Google Scholar] [CrossRef] [PubMed]
- Helfand, M.; Fiordalisi, C.; Wiedrick, J.; Ramsey, K.L.; Armstrong, C.; Gean, E.; Winchell, K.; Arkhipova-Jenkins, I. Risk for reinfection after SARS-CoV-2: A living, rapid review for American College of Physicians Practice Points on the role of the antibody response in conferring immunity following SARS-CoV-2 infection. Ann. Intern. Med. 2022, 175, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.H.; Michlmayr, D.; Gubbels, S.M.; Mølbak, K.; Ethelberg, S. Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: A population-level observational study. Lancet 2021, 397, 1204–1212. [Google Scholar] [CrossRef]
- Zhong, D.; Xiao, S.; Debes, A.K.; Egbert, E.R.; Caturegli, P.; Colantuoni, E.; Milstone, A.M. Durability of antibody levels after vaccination with mRNA SARS-CoV-2 vaccine in individuals with or without prior infection. JAMA 2021, 326, 2524–2526. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir. Med. 2021, 9, 712–720. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control & Prevention. Central Disease Control Headquarters Press Release. 12 May 2022. Available online: http://ncov.mohw.go.kr/tcmBoardView.do?brdId=3&brdGubun=31&dataGubun=&ncvContSeq=6635&contSeq=6635&board_id=312&gubun=BDJ (accessed on 10 August 2022).
- Munro, A.P.S.; Feng, S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; et al. Safety, immunogenicity, and reactogenicity of BNT162b2 and mRNA-1273 COVID-19 vaccines given as fourth-dose boosters following two doses of ChAdOx1 nCoV-19 or BNT162b2 and a third dose of BNT162b2 (COV-BOOST): A multicentre, blinded, phase 2, randomised trial. Lancet Infect. Dis. 2022, 22, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Parry, H.; Bruton, R.; Stephens, C.; Bentley, C.; Brown, K.; Amirthalingam, G.; Hallis, B.; Otter, A.; Zuo, J.; Moss, P. Extended interval BNT162b2 vaccination enhances peak antibody generation. NPJ Vaccines 2022, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.H.; Liu, X.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Effect of priming interval on reactogenicity, peak immunological response, and waning after homologous and heterologous COVID-19 vaccine schedules: Exploratory analyses of Com-COV, a randomised control trial. Lancet Respir. Med. 2022, 10, 1049–1060. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a fourth dose of Covid-19 mRNA vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Cohen, M.J.; Oster, Y.; Moses, A.E.; Spitzer, A.; Benenson, S. Association of receiving a fourth dose of the BNT162b vaccine with SARS-CoV-2 infection among health care workers in Israel. JAMA Netw. Open 2022, 5, e2224657. [Google Scholar] [CrossRef]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.Y.; Chan, Y.H.L.; et al. Efficacy of covid-19 vaccines in immunocompromised patients: Systemic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Freund, T.; Peleg, H.; Paran, D.; Levartovsky, D.; Kaufman, I.; Broyde, A.; Elalouf, O.; Polachek, A.; et al. Immunogenicity induced by two and three doses of the BNT162b2 mRNA vaccine in patients with autoimmune inflammatory rheumatic diseases and immunocompetent controls: A longitudinal multicentre study. Ann. Rheum. Dis. 2022, 81, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; Lam, E.C.; Astudillo, M.G.; Yang, D.; Miller, T.E.; Feldman, J.; Hauser, B.M.; Caradonna, T.M.; Clayton, K.L.; Nitido, A.D.; et al. COVID-19 neutralizing antibodies predict disease severity and survival. Cell 2021, 184, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.B.; Jarlhelt, I.; Perez-Alos, L.; Landsy, L.H.; Loftager, M.; Rosbjerg, A.; Helgstrand, C.; Bjelke, J.R.; Egebjerg, T.; Jardine, J.G.; et al. SARS-CoV-2 antibody response are correlated to disease severity in COVID-19 convalescent individuals. J. Immunol. 2021, 206, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Masia, M.; Fernandez-Gonzalez, M.; Telenti, G.; Agullo, V.; Garcia, J.A.; Padilla, S.; Garcia-Abellan, J.; Galiana, A.; Gonzalo-Jimenez, N.; Gutierrez, F. Durable antibody response one year after hospitalization for COVID-19: A longitudinal cohort study. J. Autoimmun. 2021, 123, 102703. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.K.; Kim, M.; Hong, J.; Kim, G.; Lee, S.; Chang, E.; Choe, P.G.; Kim, N.J.; Kim, I.S.; Seo, J.Y.; et al. Distinct immune response at 1 year post-COVID-19 according to disease severity. Front. Immunol. 2022, 13, 830433. [Google Scholar] [CrossRef]
- Herzberg, J.; Vollmer, T.; Fischer, B.; Becher, H.; Becker, A.K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. SARS-CoV-2 antibody response in health care workers after vaccination or natural infection in a longitudinal observational study. Vaccine 2022, 40, 206–212. [Google Scholar] [CrossRef]
- Morgiel, E.; Szmyrka, M.; Madej, M.; Sebastian, A.; Sokolik, R.; Andrasiak, I.; Chodyra, M.; Walas-Antoszek, M.; Korman, L.; Swierkot, J. Complete (humoral and cellular) response to vaccination against COVID-19 in a group of healthcare workers- assessment of factors affecting immunogenicity. Vaccines 2022, 10, 710. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. A bivalent omicron-containing booster vaccine against Covid-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Aged ≥ 60 Years | |||||
|---|---|---|---|---|---|
| Variables | Incomplete vaccination a (n = 10) | 2nd Vaccination (n = 17) | 3rd Vaccination (n = 32) | 4th Vaccinationafter COVID-19 (n = 27) | Healthcare Worker (n = 39) |
| Age, years | 67.5 (62.8–68.3) | 66.0 (63.0–68.5) | 65.5 (63.0–67.0) | 65.0 (63.0–68.0) | 30.0 (27.0–37.0) |
| Sex, male | 4 (40.0) | 7 (41.2) | 17 (53.1) | 17 (63.0) | 10 (25.6) |
| Primary vaccination before SARS-CoV-2 infection | |||||
| Two doses of mRNA vaccine b | NA | 6 (35.3) | 4 (12.5) | 0 | 6 (15.4) |
| Interval between 1st and 2nd doses, days | NA | 38.0 (30.0–42.0) | 21.5 (21.0–31.8) | NA | 24.5 (21.0–28.5) |
| Two doses of ChAdOx1-S | NA | 11 (64.7) | 25 (78.1) | 26 (96.3) | 30 (76.9) |
| Interval between 1st and 2nd doses, days | NA | 77.0 (77.0–77.0) | 77.0 (77.0–77.0) | 77.0 (77.0–77.0) | 84.0 (81.8–85.3) |
| Heterologous vaccination c | NA | 0 | 3 (9.4) | 1 (3.7) | 3 (7.7) |
| Interval between 1st and 2nd doses, days | NA | NA | 77.0 (77.0–77.0) | 77 | 77.0 (74.0–80.0) |
| 3rd vaccination before SARS-CoV-2 infection | |||||
| mRNA vaccine d | NA | NA | 32 (100.0) | 27 (100.0) | 39 (100.0) |
| Interval between 2nd and 3rd doses, days | NA | NA | 118.0 (107.0–130.5) | 119.0 (105.0–121.0) | 175.0 (169.0–192.0) |
| Homologous booster | NA | NA | 4 (12.5) | 0 | 6 (15.4) |
| Heterologous booster e | NA | NA | 28 (87.5) | 27 (100.0) | 33 (84.6) |
| 4th vaccination after SARS-CoV-2 infection | |||||
| Time interval from SARS-CoV-2, days | NA | NA | NA | 60.0 (55.0–67.0) | NA |
| mRNA vaccine f | NA | NA | NA | 24 (88.9) | NA |
| Interval between 3rd and 4th doses, days | NA | NA | NA | 137.0 (130.0–150.3) | NA |
| Nuvaxovid vaccine | NA | NA | NA | 3 (11.1) | NA |
| Interval between 3rd and 4th doses, days | NA | NA | NA | 137.0 (130.0–149.5) | NA |
| Sampling interval, days | |||||
| From SARS-CoV-2 infection | 87.5 (85.5–93.5) | 94.0 (87.5–99.0) | 84.0 (83.0–87.8) | 86.0 (84.0–90.0) | 81.0 (78.0–84.0) |
| From 4th vaccination | NA | NA | NA | 28.0 (22.0–32.0) | NA |
| Variables | Incomplete Vaccination a (n = 10) | 2nd Vaccination (n = 17) | 3rd Vaccination (n = 32) | p Value b | p Value c |
|---|---|---|---|---|---|
| Serologic test | |||||
| S clade, sVNT50 | |||||
| Detectable antibody titer d | 3 (30.0) | 16 (94.1) | 30 (93.8) | <0.001 | >0.99 |
| Antibody titer | 20.0 (20.0–77.3) | 302.0 (76.5–1210.5) | 418.5 (204.5–1008.5) | <0.001 | 0.50 |
| Delta variant, sVNT50 | |||||
| Detectable antibody titer d | 2 (20.0) | 15 (88.2) | 30 (93.8) | <0.001 | 0.60 |
| Antibody titer | 20.0 (20.0–31.8) | 139.0 (56.5–1058.5) | 239.5 (109.8–470.3) | <0.001 | 0.93 |
| Omicron variant, sVNT50 | |||||
| Detectable antibody titer d | 5 (50.0) | 13 (76.5) | 29 (90.6) | 0.01 | 0.22 |
| Antibody titer | 33.0 (20.0–82.5) | 124.0 (47.0–347.5) | 154.5 (83.5–451.0) | 0.003 | 0.44 |
| Variables | 3rd Vaccination (n = 32) | Healthcare Worker (n = 39) | 4th Vaccination after COVID-19 (n = 27) | p Value a | p Value b |
|---|---|---|---|---|---|
| Serologic test | |||||
| S clade, sVNT50 | |||||
| Detectable antibody titer c | 30 (93.8) | 37 (94.9) | 27 (100.0) | 0.50 | 0.51 |
| Antibody titer | 418.5 (204.5–1008.5) | 362.0 (246.0–652.0) | 603.0 (383.0–945.0) | 0.25 | 0.03 |
| Delta variant, sVNT50 | |||||
| Detectable antibody titer c | 30 (93.8) | 35 (89.7) | 27 (100.0) | 0.50 | 0.14 |
| Antibody titer | 239.5 (109.8–470.3) | 287.0 (103.0–433.0) | 405.0 (253.0–753.0) | 0.03 | 0.03 |
| Omicron variant, sVNT50 | |||||
| Detectable antibody titer c | 29 (90.6) | 33 (84.6) | 24 (88.9) | >0.99 | 0.73 |
| Antibody titer | 154.5 (83.5–451.0) | 121.0 (66.0–162.0) | 156.0 (74.0–281.0) | 0.49 | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Seo, H.; Kim, H.-W.; Kim, D.; Kwon, H.-J.; Kim, Y.-K. Effect of Previous COVID-19 Vaccination on Humoral Immunity 3 Months after SARS-CoV-2 Omicron Infection and Booster Effect of a Fourth COVID-19 Vaccination 2 Months after SARS-CoV-2 Omicron Infection. Viruses 2022, 14, 2458. https://doi.org/10.3390/v14112458
Kim J, Seo H, Kim H-W, Kim D, Kwon H-J, Kim Y-K. Effect of Previous COVID-19 Vaccination on Humoral Immunity 3 Months after SARS-CoV-2 Omicron Infection and Booster Effect of a Fourth COVID-19 Vaccination 2 Months after SARS-CoV-2 Omicron Infection. Viruses. 2022; 14(11):2458. https://doi.org/10.3390/v14112458
Chicago/Turabian StyleKim, Jinsoo, Hyeonji Seo, Han-Wool Kim, Dongbum Kim, Hyung-Joo Kwon, and Yong-Kyun Kim. 2022. "Effect of Previous COVID-19 Vaccination on Humoral Immunity 3 Months after SARS-CoV-2 Omicron Infection and Booster Effect of a Fourth COVID-19 Vaccination 2 Months after SARS-CoV-2 Omicron Infection" Viruses 14, no. 11: 2458. https://doi.org/10.3390/v14112458