
Application and Impact of Antiviral Therapy for Patients with HBV-Related Hepatocellular Carcinoma Receiving Sorafenib and Lenvatinib Treatment
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. Patient Assessment
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
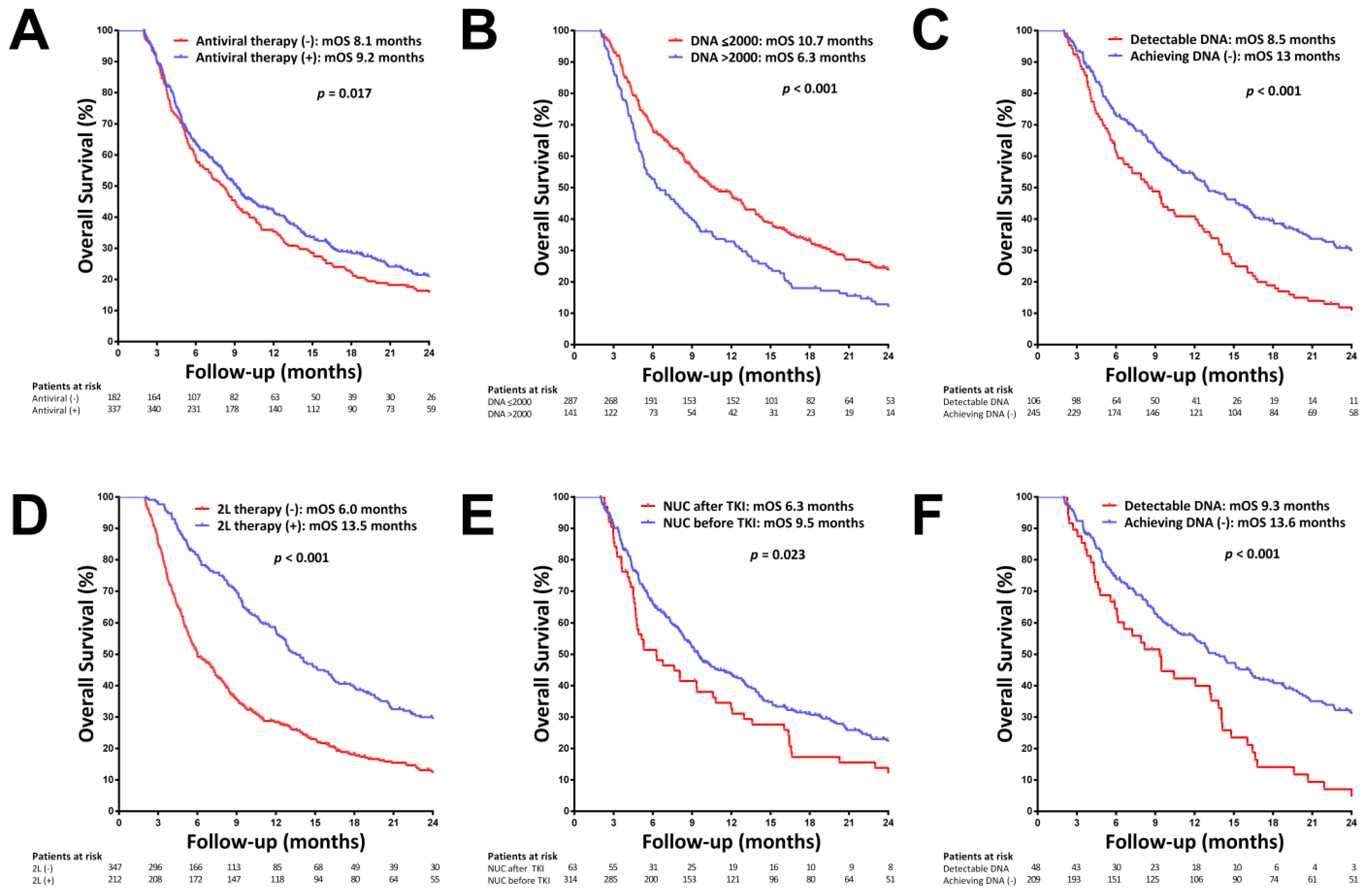
3.2. Main Outcomes in Patients with and without NUC Therapy
3.3. Secular Trends in Overall Survival and NUC Therapy Uptake from 2012–2022
3.4. Factors Associated with Overall Survival
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vogel, A.; Meyer, T.; Sapisochin, G.; Salem, R.; Saborowski, A. Hepatocellular carcinoma. Lancet 2022, 400, 1345–1362. [Google Scholar] [CrossRef]
- Wu, J.C.; Huang, Y.H.; Chau, G.Y.; Su, C.W.; Lai, C.R.; Lee, P.C.; Huo, T.I.; Sheen, I.J.; Lee, S.D.; Lui, W.Y. Risk factors for early and late recurrence in hepatitis B-related hepatocellular carcinoma. J. Hepatol. 2009, 51, 890–897. [Google Scholar] [CrossRef]
- Lee, I.C.; Lei, H.J.; Chau, G.Y.; Yeh, Y.C.; Wu, C.J.; Su, C.W.; Huo, T.I.; Chao, Y.; Lin, H.C.; Hou, M.C.; et al. Predictors of long-term recurrence and survival after resection of HBV-related hepatocellular carcinoma: The role of HBsAg. Am. J. Cancer Res. 2021, 11, 3711–3725. [Google Scholar] [PubMed]
- Wong, G.L.; Tse, Y.K.; Chan, H.L.; Yip, T.C.; Tsoi, K.K.; Wong, V.W. Oral nucleos(t)ide analogues reduce recurrence and death in chronic hepatitis B-related hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2016, 43, 802–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.C.; Chau, G.Y.; Yeh, Y.C.; Chao, Y.; Huo, T.I.; Su, C.W.; Lin, H.C.; Hou, M.C.; Huang, Y.H. Risk of recurrence in chronic hepatitis B patients developing hepatocellular carcinoma with antiviral secondary prevention failure. PLoS ONE 2017, 12, e0188552. [Google Scholar]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fabrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Han, J.; Kim, G.M.; Han, K.H.; Choi, H.J. Hepatitis B viral load predicts survival in hepatocellular carcinoma patients treated with sorafenib. J. Gastroenterol. Hepatol. 2015, 30, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Gao, H.; Huang, J.; Wang, H.; Zhou, Z.; Zhang, Y.; Li, S.; Chen, M. Antiviral therapy in the improvement of survival of patients with hepatitis B virus-related hepatocellular carcinoma treated with sorafenib. J. Gastroenterol. Hepatol. 2015, 30, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wen, F.; Li, J.; Zhang, P.; Yan, W.; Hao, P.; Xia, F.; Bi, F.; Li, Q. A high baseline HBV load and antiviral therapy affect the survival of patients with advanced HBV-related HCC treated with sorafenib. Liver Int. 2015, 35, 2147–2154. [Google Scholar] [CrossRef]
- Wang, H.W.; Chuang, P.H.; Su, W.P.; Kao, J.T.; Hsu, W.F.; Lin, C.C.; Huang, G.T.; Lin, J.T.; Lai, H.C.; Peng, C.Y. On-Treatment Albumin-Bilirubin Grade: Predictor of Response and Outcome of Sorafenib-Regorafenib Sequential Therapy in Patients with Unresectable Hepatocellular Carcinoma. Cancers 2021, 13, 3758. [Google Scholar] [CrossRef] [PubMed]
- Uchikawa, S.; Kawaoka, T.; Ando, Y.; Yamaoka, K.; Kosaka, Y.; Suehiro, Y.; Fujii, Y.; Morio, K.; Nakahara, T.; Murakami, E.; et al. Trends in Hepatic Functional Reserve of Patients with Hepatocellular Carcinoma Treated with Tyrosine Kinase Inhibitors. Oncology 2020, 98, 727–733. [Google Scholar] [CrossRef]
- Lee, I.C.; Chao, Y.; Li, C.P.; Su, C.W.; Lan, K.H.; Lin, H.C.; Hou, M.C.; Huang, Y.H. Risk of renal events during tenofovir disoproxil fumarate and entecavir antiviral prophylaxis in HBsAg-positive cancer patients undergoing chemotherapy. J. Viral Hepat. 2018, 25, 1599–1607. [Google Scholar] [CrossRef]
- Lee, I.C.; Lan, K.H.; Su, C.W.; Li, C.P.; Chao, Y.; Lin, H.C.; Hou, M.C.; Huang, Y.H. Efficacy and Renal Safety of Prophylactic Tenofovir Alafenamide for HBV-Infected Cancer Patients Undergoing Chemotherapy. Int. J. Mol. Sci. 2022, 23, 11335. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Tampaki, M.; Lok, A.S.; Papatheodoridis, G.V. Risk of HBV reactivation during therapies for HCC: A systematic review. Hepatology 2022, 75, 1257–1274. [Google Scholar] [CrossRef]
- Bruix, J.; Chan, S.L.; Galle, P.R.; Rimassa, L.; Sangro, B. Systemic treatment of hepatocellular carcinoma: An EASL position paper. J. Hepatol. 2021, 75, 960–974. [Google Scholar] [CrossRef]
- Lee, I.C.; Chen, Y.T.; Chao, Y.; Huo, T.I.; Li, C.P.; Su, C.W.; Lin, H.C.; Lee, F.Y.; Huang, Y.H. Determinants of survival after sorafenib failure in patients with BCLC-C hepatocellular carcinoma in real-world practice. Medicine 2015, 94, e688. [Google Scholar] [CrossRef]
- Lee, I.C.; Chao, Y.; Lee, P.C.; Chen, S.C.; Chi, C.T.; Wu, C.J.; Wu, K.C.; Hou, M.C.; Huang, Y.H. Determinants of Survival and Post-Progression Outcomes by Sorafenib-Regorafenib Sequencing for Unresectable Hepatocellular Carcinoma. Cancers 2022, 14, 2014. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.C.; Chen, Y.T.; Chao, Y.; Huo, T.I.; Li, C.P.; Su, C.W.; Lee, M.H.; Hou, M.C.; Lee, F.Y.; Lin, H.C.; et al. Validation of the albumin-bilirubin grade-based integrated model as a predictor for sorafenib-failed hepatocellular carcinoma. Liver Int. 2018, 38, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.W.; Lee, P.C.; Chao, Y.; Su, C.W.; Lee, I.C.; Lan, K.H.; Chu, C.J.; Hung, Y.P.; Chen, S.C.; Hou, M.C.; et al. Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma. Ther. Adv. Med. Oncol. 2022, 14, 17588359221099401. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.J.; Lee, P.C.; Hung, Y.W.; Lee, C.J.; Chi, C.T.; Lee, I.C.; Hou, M.C.; Huang, Y.H. Lenvatinib plus pembrolizumab for systemic therapy-naive and -experienced unresectable hepatocellular carcinoma. Cancer Immunol. Immunother. 2022, 71, 2631–2643. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Lee, I.C.; Hung, Y.W.; Liu, C.A.; Lee, R.C.; Su, C.W.; Huo, T.I.; Li, C.P.; Chao, Y.; Lin, H.C.; Hou, M.C.; et al. A new ALBI-based model to predict survival after transarterial chemoembolization for BCLC stage B hepatocellular carcinoma. Liver Int. 2019, 39, 1704–1712. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [Green Version]
- Tovoli, F.; Ielasi, L.; Casadei-Gardini, A.; Granito, A.; Foschi, F.G.; Rovesti, G.; Negrini, G.; Orsi, G.; Renzulli, M.; Piscaglia, F. Management of adverse events with tailored sorafenib dosing prolongs survival of hepatocellular carcinoma patients. J. Hepatol. 2019, 71, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Hui, V.W.; Chan, S.L.; Wong, V.W.; Liang, L.Y.; Yip, T.C.; Lai, J.C.; Yuen, B.W.; Luk, H.W.; Tse, Y.K.; Lee, H.W.; et al. Increasing antiviral treatment uptake improves survival in patients with HBV-related HCC. JHEP Rep. 2020, 2, 100152. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.H.; Lu, S.N.; Chen, Y.Y.; Kee, K.M.; Yen, Y.H.; Hung, C.H.; Hu, T.H.; Chen, C.H.; Wang, J.H. Real-World Lenvatinib Versus Sorafenib in Patients with Advanced Hepatocellular Carcinoma: A Propensity Score Matching Analysis. Front. Oncol. 2021, 11, 737767. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Yang, S.S.; Lien, H.C.; Peng, Y.C.; Ko, C.W.; Lee, T.Y. Efficacy of Lenvatinib and Sorafenib in the Real-World First-Line Treatment of Advanced-Stage Hepatocellular Carcinoma in a Taiwanese Population. J. Clin. Med. 2022, 11, 1444. [Google Scholar] [CrossRef] [PubMed]
- Hung, Y.W.; Lee, I.C.; Chi, C.T.; Lee, R.C.; Liu, C.A.; Chiu, N.C.; Hwang, H.E.; Chao, Y.; Hou, M.C.; Huang, Y.H. Redefining Tumor Burden in Patients with Intermediate-Stage Hepatocellular Carcinoma: The Seven-Eleven Criteria. Liver Cancer 2021, 10, 629–640. [Google Scholar] [CrossRef]
- Schemmer, P.; Burra, P.; Hu, R.H.; Huber, C.M.; Loinaz, C.; Machida, K.; Vogel, A.; Samuel, D. State of the art treatment of hepatitis B virus hepatocellular carcinoma and the role of hepatitis B surface antigen post-liver transplantation and resection. Liver Int. 2022, 42, 288–298. [Google Scholar] [CrossRef]
- Kuo, Y.H.; Huang, T.H.; Wang, J.H.; Chen, Y.Y.; Tsai, M.C.; Chen, Y.H.; Lu, S.N.; Hu, T.H.; Chen, C.H.; Hung, C.H. Well-Controlled Viremia Predicts the Outcome of Hepatocellular Carcinoma in Chronic Viral Hepatitis Patients Treated with Sorafenib. Cancers 2022, 14, 3971. [Google Scholar] [CrossRef]
- Lee, I.C.; Yang, S.S.; Lee, C.J.; Su, C.W.; Wang, Y.J.; Lan, K.H.; Lin, H.C.; Hou, M.C.; Peng, C.Y.; Huang, Y.H. Incidence and Predictors of HBsAg Loss After Peginterferon Therapy in HBeAg-Negative Chronic Hepatitis B: A Multicenter, Long-term Follow-up Study. J. Infect. Dis. 2018, 218, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.C.; Su, C.W.; Lan, K.H.; Wang, Y.J.; Lee, K.C.; Lin, H.C.; Hou, M.C.; Huang, Y.H. Virological and immunological predictors of long term outcomes of peginterferon alfa-2a therapy for HBeAg-negative chronic hepatitis B. J. Formos. Med. Assoc. 2021, 120, 1676–1685. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| With NUC Therapy (n = 377) | Without NUC Therapy (n = 182) | p | |
|---|---|---|---|
| Age (years) | 62.2 ± 12.5 | 63.3 ± 13.2 | 0.318 |
| Sex (male), n (%) | 319 (84.6) | 158 (86.8) | 0.575 |
| HCC treatment: Sorafenib/lenvatinib, n (%) | 340/37 (90.2/9.8) | 178/4 (97.8/2.2) | 0.002 |
| BCLC stage B/C, n (%) | 331 (87.8) | 176 (96.7) | 0.001 |
| Portal vein invasion, n (%) | 210 (55.7) | 111 (61) | 0.274 |
| Vp4 | 62 (16.4) | 26 (14.3) | 0.594 |
| Extrahepatic metastasis, n (%) | 197 (52.3) | 106 (58.2) | 0.215 |
| Child-Pugh class A/B, n (%) | 38 (10.1) | 25 (13.7) | 0.255 |
| ALBI score | −2.47 ± 0.49 | −2.48 ± 0.44 | 0.896 |
| ALBI grade 1/2/3, n (%) | 160/211/6 (42.4/56/1.6) | 75/105/2 (41.2/57.7/1.1) | 0.875 |
| HBV DNA (Log IU/mL) * | 2.72 ± 2 | 3.08 ± 1.99 | 0.013 |
| Undetectable HBV DNA, n (%) * | 161 (47.9) | 27 (29.3) | 0.002 |
| HBV DNA < 2000 IU/mL, n (%) * | 230 (68.5) | 57 (62) | 0.294 |
| NUC type: LMV/ADV/ETV/TDF/TAF, n (%) | 6/3/305/31/32 (1.6/0.8/80.9/8.2/8.5) | - | |
| NUC therapy before TKI, n (%) | 314 (83.3) | - | |
| Bilirubin (mg/dL) | 1.04 ± 1.24 | 0.93 ± 0.51 | 0.387 |
| Albumin (g/dL) | 3.80 ± 0.51 | 3.80 ± 0.46 | 0.695 |
| ALT (U/L) | 52 ± 48 | 52 ± 50 | 0.956 |
| AST (U/L) | 72 ± 68 | 68 ± 56 | 0.766 |
| Platelet (109/L) | 173 ± 95 | 179 ± 100 | 0.496 |
| AFP (ng/mL) | 269 (16–4766) | 1153 (19–8682) | 0.028 |
| With NUC Therapy (n = 377) | Without NUC Therapy (n = 182) | p | |
|---|---|---|---|
| Follow-up period (months) | 14.1 (2–103.3) | 11.9 (2–61.2) | 0.442 |
| Duration of Sorafenic/Lenvatinib treatment (days) | 86 (59–145) | 73.5 (56–131.5) | 0.156 |
| Disease progression, n (%) | 159 (87.4) | 332 (88.1) | 0.921 |
| Progression-free survival (months) | 2.6 (2.2–2.9) | 2.4 (2.0–2.8) | 0.914 |
| Second-line systemic therapy, n (%) | 156 (41.4) | 56 (30.8) | 0.020 |
| Death, n (%) | 306 (81.2) | 170 (93.4) | <0.001 |
| Overall survival (months) | 9.2 (8.0–10.4) | 8.1 (6.4–9.7) | 0.017 |
| Virological response, n (%) * | 209 (81.3) | - | - |
| HBV reactivation, n (%) | - | 12 (6.6) | - |
| HBV reactivation-related death, n (%) | - | 2 (16.7) | - |
| Univariate | Multivariate Model I † | Multivariate Model II † | |||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| Baseline factors | |||||||
| Age (years) | >60 vs. ≤60 | 0.889 (0.741–1.066) | 0.205 | ||||
| Sex | Female vs. male | 1.035 (0.802–1.337) | 0.792 | ||||
| BCLC stage | C vs. B | 2.678 (1.803–3.979) | <0.001 | 1.971 (1.273–3.052) | 0.002 | 1.695 (1.077–2.666) | 0.023 |
| Portal vein invasion | Yes vs. no | 1.633 (1.356–1.967) | <0.001 | NS | NS | ||
| Vp4 | Yes vs. no | 1.412 (1.106–1.804) | 0.006 | NS | NS | ||
| Extrahepatic metastasis | Yes vs. no | 1.128 (0.941–1.351) | 0.193 | ||||
| AFP (ng/mL) | >400 vs. ≤400 | 1.659 (1.384–1.988) | <0.001 | 1.374 (1.374–1.109) | 0.004 | NS | |
| HBV DNA (IU/mL) | >20 vs. ≤20 | 1.442 (1.168–1.779) | 0.001 | NS | NS | ||
| >2000 vs. ≤2000 | 1.486 (1.195–1.847) | <0.001 | 1.309 (1.049–1.634) | 0.017 | NS | ||
| NUC therapy | Yes vs. no | 0.796 (0.660–0.961) | 0.018 | NS | NS | ||
| ALBI grade | 2–3 vs. 1 | 1.874 (1.554–2.260) | <0.001 | 1.609 (1.298–1.996) | <0.001 | 1.688 (1.285–2.217) | <0.001 |
| ALT (U/L) | >40 vs. ≤40 | 1.280 (1.069–1.533) | 0.007 | NS | NS | ||
| AST (U/L) | >40 vs. ≤40 | 1.562 (1.291–1.889) | <0.001 | NS | NS | ||
| Platelet count (109/L) | >150 vs. ≤150 | 0.971 (0.811–1.163) | 0.752 | ||||
| On-treatment factors | |||||||
| Achieving undetectable HBV DNA | Yes vs. no | 0.533 (0.432–0.709) | <0.001 | 0.609 (0.442–0.839) | 0.002 | ||
| Second-line therapy | Yes vs. no | 0.523 (0.433–0.632) | <0.001 | 0.630 (0.481–0.824) | 0.001 | ||
| Univariate | Multivariate Model I † | Multivariate Model II † | |||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| Baseline factors | |||||||
| Age (years) | >60 vs. ≤60 | 0.872 (0.696–1.094) | 0.236 | ||||
| Sex | Female vs. male | 0.901 (0.662–1.228) | 0.510 | ||||
| BCLC stage | C vs. B | 2.544 (1.663–3.894) | <0.001 | 1.936 (1.233–3.041) | 0.004 | 1.842 (1.149–2.953) | 0.011 |
| Portal vein invasion | Yes vs. no | 1.623 (1.290–2.043) | <0.001 | NS | NS | ||
| Vp4 | Yes vs. no | 1.423 (1.052–1.926) | 0.022 | NS | NS | ||
| Extrahepatic metastasis | Yes vs. no | 1.224 (0.977–1.533) | 0.079 | NS | NS | ||
| AFP (ng/mL) | >400 vs. ≤400 | 1.778 (1.418–2.229) | <0.001 | 1.439 (1.127–1.837) | 0.004 | 1.382 (1.033–1.849) | 0.030 |
| HBV DNA (IU/mL) | >20 vs. ≤20 | 1.593 (1.254–2.024) | <0.001 | NS | NS | ||
| >2000 vs. ≤2000 | 1.508 (1.173–1.938) | 0.001 | NS | NS | |||
| NUC starting time | Before TKI vs. After TKI | 0.715 (0.535–0.957) | 0.024 | 0.711 (0.521–0.971) | 0.032 | NS | |
| ALBI grade | 2–3 vs. 1 | 1.940 (1.534–2.452) | <0.001 | 1.655 (1.294–2.118) | <0.001 | 1.648 (1.239–2.193) | 0.001 |
| ALT (U/L) | >40 vs. ≤40 | 1.267 (1.012–1.586) | 0.039 | NS | NS | ||
| AST (U/L) | >40 vs. ≤40 | 1.480 (1.168–1.874) | 0.001 | NS | NS | ||
| Platelet count (109/L) | >150 vs. ≤150 | 0.992 (0.792–1.241) | 0.942 | ||||
| On-treatment factors | |||||||
| Achieving undetectable HBV DNA | Yes vs. no | 0.496 (0.353–0.697) | <0.001 | 0.580 (0.411–0.817) | 0.002 | ||
| Second-line therapy | Yes vs. no | 0.586 (0.465–0.737) | <0.001 | 0.620 (0.468–0.822) | 0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.-C.; Lee, P.-C.; Chao, Y.; Chi, C.-T.; Wu, C.-J.; Hung, Y.-P.; Su, C.-W.; Hou, M.-C.; Huang, Y.-H. Application and Impact of Antiviral Therapy for Patients with HBV-Related Hepatocellular Carcinoma Receiving Sorafenib and Lenvatinib Treatment. Viruses 2022, 14, 2355. https://doi.org/10.3390/v14112355
Lee I-C, Lee P-C, Chao Y, Chi C-T, Wu C-J, Hung Y-P, Su C-W, Hou M-C, Huang Y-H. Application and Impact of Antiviral Therapy for Patients with HBV-Related Hepatocellular Carcinoma Receiving Sorafenib and Lenvatinib Treatment. Viruses. 2022; 14(11):2355. https://doi.org/10.3390/v14112355
Chicago/Turabian StyleLee, I-Cheng, Pei-Chang Lee, Yee Chao, Chen-Ta Chi, Chi-Jung Wu, Yi-Ping Hung, Chien-Wei Su, Ming-Chih Hou, and Yi-Hsiang Huang. 2022. "Application and Impact of Antiviral Therapy for Patients with HBV-Related Hepatocellular Carcinoma Receiving Sorafenib and Lenvatinib Treatment" Viruses 14, no. 11: 2355. https://doi.org/10.3390/v14112355