
Comparative Study of Vaccinated and Unvaccinated Hospitalised Patients: A Retrospective Population Study of 500 Hospitalised Patients with SARS-CoV-2 Infection in a Spanish Population of 220,000 Inhabitants
 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Age and Comorbidities
3.2. Chest Radiograph upon Admission
3.3. Oxygen Supplementation
3.4. Laboratory Results
3.5. Treatments
3.6. COVID-19 Severity: ICU Admission, Classification at Hospital Discharge, and In-Hospital Mortality
3.7. One-Month Mortality
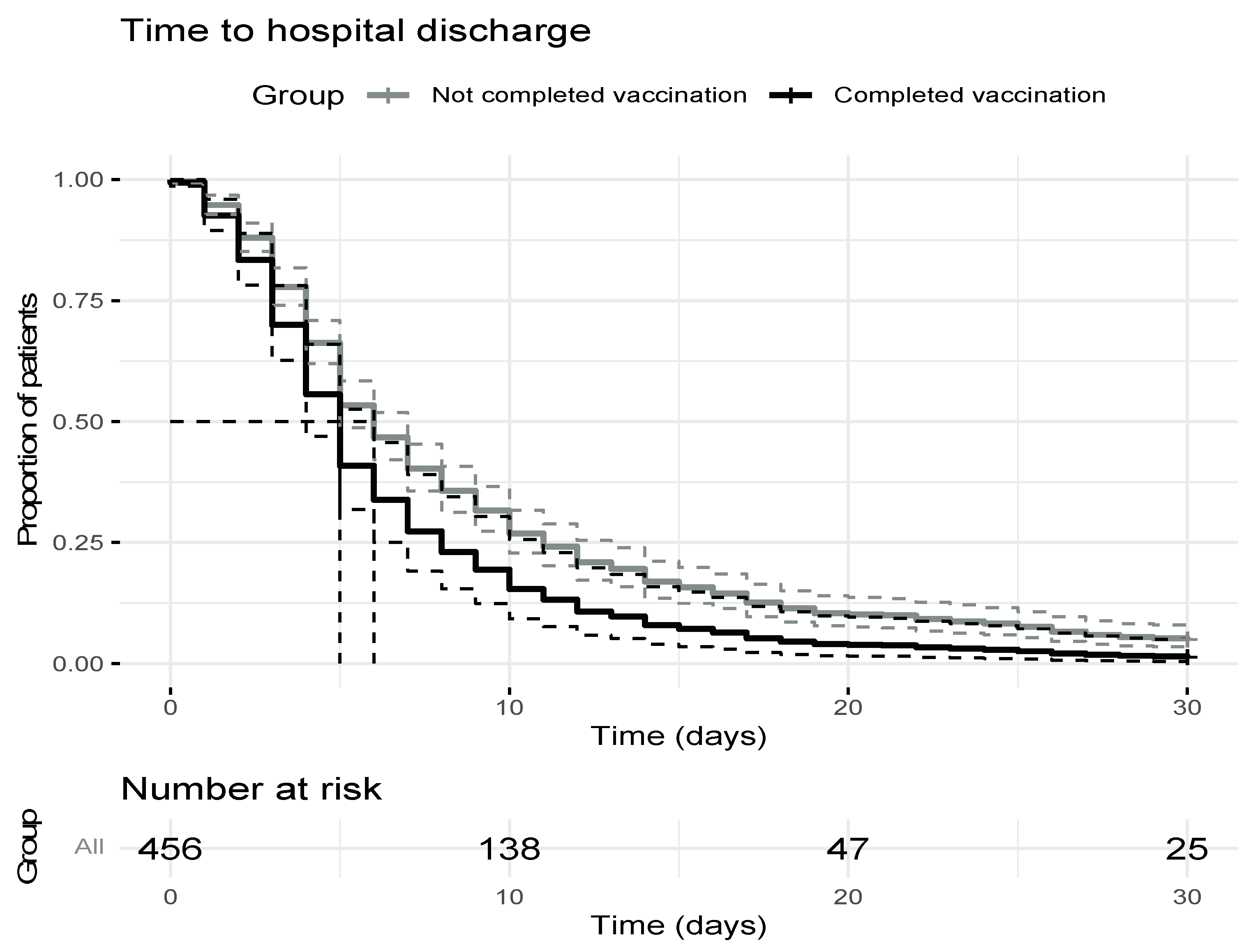
3.8. Length of Hospital Stay
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://COVID19.who.int (accessed on 12 July 2022).
- Health Concierge, Community of Madrid. COVID-19 Surveillance Epidemiological Report. Available online: https://www.comunidad.madrid/sites/default/files/doc/sanidad/epid/informe_epidemiologico_semanal.pdf (accessed on 12 July 2022). (In Spanish).
- Spanish Statistical Office. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=2881&L=0 (accessed on 12 July 2022). (In Spanish).
- Fuenlabrada City Council. Numerical Summary by Nationality. Available online: https://www.aytofuenlabrada.es/recursos/doc/SC/Estadisticas_y_territorio/20644_2512512021141528.pdf (accessed on 20 November 2021). (In Spanish).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111, Erratum in Lancet 2021, 397, 98. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Government of Spain. COVID-19 Vaccination Strategy. Available online: https://www.vacunacovid.gob.es/ (accessed on 15 October 2021). (In Spanish).
- The Spanish Agency for Medication and Healthcare Products. Available online: https://www.aemps.gob.es/la-aemps/ultima-informacion-de-la-aemps-acerca-del-covid%e2%80%9119/vacunas-contra-la-covid%e2%80%9119/informacion-de-vacunas-autorizadas/ (accessed on 28 September 2021). (In Spanish).
- Spanish Ministry of Health. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/vacunaCovid19.htm (accessed on 23 October 2021). (In Spanish).
- Haas, E.J.; McLaughlin, J.M.; Khan, F.; Angulo, F.J.; Anis, E.; Lipsitch, M.; Singer, S.R.; Mircus, G.; Brooks, N.; Smaja, M.; et al. Infections, hospitalisations, and deaths averted via a nationwide vaccination campaign using the Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine in Israel: A retrospective surveillance study. Lancet Infect. Dis. 2021, 22, 357–366. [Google Scholar] [CrossRef]
- Taylor, C.A.; Patel, K.; Pham, H.; Whitaker, M.; Anglin, O.; Kambhampati, A.K.; Milucky, J.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; et al. Severity of Disease Among Adults Hospitalized with Laboratory-Confirmed COVID-19 Before and During the Period of SARS-CoV-2 B.1.617.2 (Delta) Predominance—COVID-NET, 14 States, January–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Olivier, E.; Sophie, A.; Maeva, L.; Jean-François, F.; Jocelyn, M.; Emilia, F.; Sophie, B.; Cécile, J.; Gabrielle, C.; Audrey, F.; et al. Impact of vaccination on the symptoms of hospitalised patients with SARS-CoV-2 delta variant (B.1.617.1) infection. Clin. Microbiol. Infect. 2022, in press. [Google Scholar] [CrossRef]
- Moreira, A.C.; Teles, M.J.; Silva, T.; Bento, C.M.; Alves, I.S.; Pereira, L.; Guimarães, J.T.; Porto, G.; Oliveira, P.; Gomes, M.S. Iron Related Biomarkers Predict Disease Severity in a Cohort of Portuguese Adult Patients during COVID-19 Acute Infection. Viruses 2021, 13, 2482. [Google Scholar] [CrossRef] [PubMed]
- Alhasan, K.A.; Shalaby, M.A.; Temsah, M.-H.; Aljamaan, F.; Shagal, R.; AlFaadhel, T.; Alomi, M.; AlMatham, K.; AlHerbish, A.J.; Raina, R.; et al. Factors That Influence Mortality in Critically Ill Patients with SARS-CoV-2 Infection: A Multicenter Study in the Kingdom of Saudi Arabia. Healthcare 2021, 9, 1608. [Google Scholar] [CrossRef] [PubMed]
- Bilgir, F.; Çalik, Ş.; Demir, I.; Akan, Ö.Y.I.L.; Bilgir, O. The effects of lung involvement, clinical and laboratory parameters on outcome in elderly patients with coronavirus disease 2019. Blood Coagul. Fibrinolysis 2022, 3, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Pya, Y.; Bekbossynova, M.; Gaipov, A.; Lesbekov, T.; Kapyshev, T.; Kuanyshbek, A.; Tauekelova, A.; Litvinova, L.; Sailybayeva, A.; Vakhrushev, I.; et al. Mortality predictors of hospitalized patients with COVID-19: Retrospective cohort study from Nur-Sultan, Kazakhstan. PLoS ONE 2021, 16, e0261272. [Google Scholar] [CrossRef] [PubMed]
- Brosh-Nissimov, T.; Orenbuch-Harroch, E.; Chowers, M.; Elbaz, M.; Nesher, L.; Stein, M.; Maor, Y.; Cohen, R.; Hussein, K.; Weinberger, M.; et al. BNT162b2 vaccine breakthrough: Clinical characteristics of 152 fully vaccinated hospitalized COVID-19 patients in Israel. Clin. Microbiol. Infect. 2021, 27, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Muthukrishnan, J.; Vardhan, V.; Mangalesh, S.; Koley, M.; Shankar, S.; Yadav, A.K.; Khera, A. Vaccination status and COVID-19 related mortality: A hospital based cross sectional study. Med. J. Armed Forces India 2021, 77 (Suppl. S2), S278–S282. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
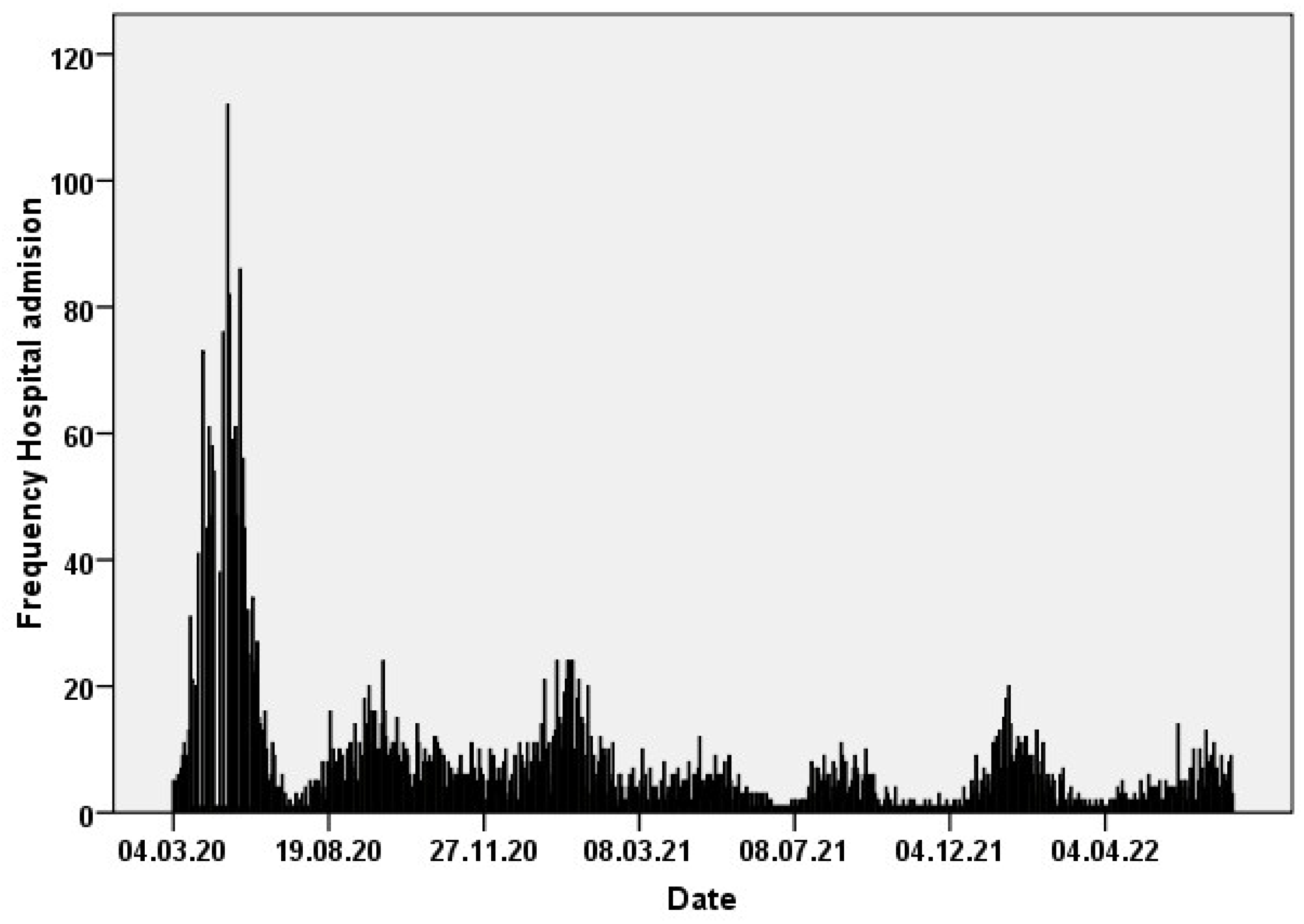
| Waves | Hospital Admissions | Mean Age, (SD) Years | ICU (%) | Deaths in Hospital (%) | Deaths in Patients >70 Years (%) | Date |
|---|---|---|---|---|---|---|
| First | 1586 | 63 (14.9) | 85 (5.4) | 154/1570 (9.8) | 108/499 (21) | 4 March 2020 to 14 July 2020 |
| Second | 915 | 60 (17.6) | 76 (8.3) | 77/910 (8.5) | 46/253 (18.1) | 15 July 2020 to 25 November 2020 |
| Third | 853 | 65 (16.6) | 75 (8.8) | 90/833 (10.8) | 62/305 (20.3) | 26 November 2020 to 28 February 2021 |
| Fourth | 306 | 61 (14.6) | 44 (14.7) | 16/306 (5.2) | 14/85 (16.4) | 1 March 2021 to 30 June 2021 |
| Fifth | 194 | 56 (20.1) | 23 (11.5) | 11/194 (5.6) | 10/51 (19.6) | 1 July 2021 to 27 September 2021 |
| Sixth | 538 | 66.5 (17.4) | 34 (6.3) | 34/538 (6.3) | 23/191 (12) | 1 October 2021 to 4 April 2022 |
| Seventh | 344 | 74.5 (14.8) | 5 (2) | 16/344 (4.3) | 14/166 (8.4) | 6 April 2022 to 4 July 2022 |
| Total | 4736 | |||||
| Variable | No.of Patients | Not Vaccinated | Vaccinated | p Value | |||
|---|---|---|---|---|---|---|---|
| Vaccination | 500 | 423 | 84.6% | 77 | 15.4% | <0.01 | |
| Age (years) | 500 | 423 | 55 (43–67) | 77 | 76 (67–87) | <0.01 | |
| Age | Under 40 years | 75 | 75/423 | 17.7% | 0/77 | 0% | <0.01 |
| 41–50 | 94 | 93/423 | 22% | 1/77 | 1.3% | ||
| 51–60 | 94 | 88/423 | 20.8% | 6/77 | 7.8% | ||
| 61–70 | 101 | 84/423 | 19.9% | 17/77 | 22.1% | ||
| 71–80 | 79 | 60/423 | 14.4% | 19/77 | 24.7% | ||
| Over 80 | 57 | 23/423 | 5.4% | 34/77 | 44.2% | ||
| Sex (M/F) | 500 (272/228) | 423 (236/137) | 55.8%/44.2% | 77 (36/41) | 46.8%/53.2% | 0.17 | |
| BMI (kg/m2) | 368 | 328 | 29.3 (26.6–33.2) | 60 | 28.8 (25.4–33.1) | 0.26 | |
| Charlson scale | 476 | 400 | 0 (0–1) | 76 | 2 (0.25–3) | <0.01 | |
| Hypertension | 211/497 | 154/420 | 36.7% | 57/77 | 74% | <0.01 | |
| Diabetes | 88/498 | 56/421 | 13.3% | 32/77 | 41.6% | <0.01 | |
| Ischemic cardiopathy | 26/497 | 13/421 | 3.1% | 13/76 | 15.3% | <0.01 | |
| Heart failure | 27/496 | 17/419 | 4.1% | 10/77 | 13% | <0.01 | |
| Smoker | 29/500 | 24/423 | 5.7% | 5/77 | 6.5% | 0.96 | |
| COPD | 41/500 | 32/423 | 7.6% | 9/77 | 11.7% | 0.25 | |
| Haematological disease | 30/495 | 22/418 | 5.2% | 9/77 | 11.6% | 0.20 | |
| Oncological disease | 28/492 | 20/415 | 4.8% | 8/77 | 10% | 0.23 | |
| Autoimmune disease | 16/498 | 15/421 | 3.6% | 1/77 | 1.3% | 0.48 | |
| HIV | 1/492 | 1/460 | 0.2% | 0/77 | 0% | 0.66 | |
| Dementia | 24/496 | 9/419 | 2.1% | 15/77 | 19.5% | <0.01 | |
| Nursing home | 17/486 | 9/413 | 2.2% | 8/77 | 15% | <0.01 | |
| Variable | No. of Patients | Not Vaccinated | Vaccinated | p Value | ||
|---|---|---|---|---|---|---|
| Initial chest radiography | ||||||
| No pneumonia | 81/451 | 51/376 | 13.6% | 30/75 | 40% | <0.01 |
| Unilateral pneumonia | 79/451 | 66/376 | 17.6% | 13/75 | 17.5% | |
| Bilateral pneumonia | 291/451 | 259/376 | 68.9% | 32/75 | 42.7% | |
| Severity | ||||||
| Mild (without pneumonia) | 69/490 | 43/415 | 10.4% | 26/75 | 34.7% | <0.01 |
| Moderate (pneumonia without severe symptoms) | 184/490 | 163/415 | 39.3% | 21/75 | 26% | |
| Severe (Tachipnea, saturation under 93% or more than 50% affected lungs) | 237/490 | 209/415 | 50.4% | 28/75 | 37.3% | |
| Highest oxygen requirements | ||||||
| Not oxygen | 77/492 | 66/416 | 15.9% | 11/76 | 14.3% | 0.23 |
| Low flow oxygen | 260/492 | 216/416 | 51.9% | 44/76 | 57.9% | |
| VM 28% | 2/492 | 1/416 | 0.2% | 1/76 | 1.3% | |
| VM 31% | 5/492 | 5/416 | 1.2% | 0 | 0% | |
| VM 35% | 34/492 | 26/416 | 6.3% | 8/76 | 10.5% | |
| VM 50% | 91/492 | 83/416 | 20% | 8/78 | 10.5% | |
| NRBM 100% | 23/492 | 19/416 | 4.6% | 4/76 | 5.3% | |
| Analytical findings | ||||||
| Highest CRP (mg/mL) | 490 | 415 | 9 (3.8–13) | 75 | 10.2 (3.8–17.2) | 0.38 |
| Highest IL6 (pg/mL) in hospital | 372 | 317 | 38.4 (12–104) | 55 | 40 (6.7–65) | 0.88 |
| Highest IL6 (pg/mL) pretreatment with tocilizumab | 271 | 229 | 26.4 (8.4–59.5) | 42 | 14.9 (5.3–54.6) | 0.20 |
| Lowest lymphocyte (value/mcL) | 492 | 416 | 875 (650–1210) | 76 | 930 (572–1320) | 0.43 |
| DD (mg/dL) | 486 | 411 | 925 (565–1625) | 75 | 879 (437–2287) | 0.71 |
| LDH (mg/dL) | 487 | 412 | 323 (257–412) | 75 | 313 (229–436) | 0.83 |
| Highest ferritin (ng/dL) | 460 | 391 | 700 (336–1268) | 69 | 351 (144–739) | <0.01 |
| Treatments | Total Patients | Not Vaccinated (%) | Vaccinated (%) | p Value |
|---|---|---|---|---|
| Remdesivir | 7/500 | 5/423 (1.2) | 2/77 (2.6) | 0.29 |
| Tocilizumab | 228/500 | 202/423 (47.8) | 26/77 (33.8) | 0.025 |
| Imatinib | 15/500 | 15/423 (3.5) | 0/77 (0.0) | 0.093 |
| Baricitinib | 59/500 | 49/423 (11.6) | 10/77 (10.0) | 0.72 |
| Anakinra | 5/500 | 5/423 (1.18) | 0/77 (0.0) | 1 |
| LMWH | 478/500 | 404/423 (95.5) | 74/77 (96.1) | 1 |
| Corticosteroids | 450/500 | 384/423 (90.8) | 66/77 (85.7) | 0.17 |
| Variable | No. of Patients | Not Vaccinated | Vaccinated | p Value | ||
|---|---|---|---|---|---|---|
| Hospital stay (days) | 483 | 407 | 6 (4–11) | 76 | 6 (4–12) | 0.63 |
| ICU stay (days) | 67 | 63 | 17.8 (7–26) | 4 | 17 (4–18) | 0.26 |
| ICU admission | 67/500 | 63/423 | 14.9% | 4/77 | 6% | 0.018 |
| Under 40 y | 12/75 | 12/75 | 16% | 0/0 | 0% | |
| 41–50 y | 12/94 | 12/93 | 12.9% | 0/1 | 0% | |
| 51–60 y | 9/94 | 8/88 | 9% | 1/6 | 16.6% | |
| 61–70 y | 18/101 | 18/84 | 21.4% | 0/17 | 0% | |
| 71–80 y | 14/79 | 12/60 | 20% | 2/19 | 10.5% | |
| Over 80 y | 2/57 | 1/23 | 4.3% | 1/34 | 2.9% | |
| Death in hospital | 27/500 | 17/423 | 4% | 10/77 | 13% | <0.01 |
| Under 40 y | 0/75 | 0/75 | 0% | 0/0 | 0% | <0.01 |
| 41–50 | 0/94 | 0/93 | 0% | 0/1 | 0% | |
| 51–60 | 0/94 | 0/88 | 0% | 0/6 | 0% | |
| 61–70 | 3/101 | 3/84 | 3.5% | 0/17 | 0% | |
| 71–80 | 11/79 | 8/60 | 13.3% | 3/19 | 15.7% | |
| Over 80 years | 13/57 | 6/23 | 26% | 7/34 | 20.5% | |
| Death one month after discharge | 33/500 | 22/418 | 5.3% | 11/77 | 14.3% | <0.01 |
| Under 40 y | 0/75 | 0/75 | 0% | 0/0 | 0% | |
| 41–50 y | 0/94 | 0/93 | 0% | 0/1 | 0% | |
| 51–60 y | 1/94 | 1/88 | 1.1% | 0/6 | 0% | |
| 61–70 y | 4/101 | 3/84 | 3.5% | 1/17 | 5.8% | |
| 71–80 y | 13/79 | 10/60 | 16.6% | 3/19 | 15.7% | |
| Over 80 y | 15/57 | 8/23 | 34.7% | 7/34 | 20.5% | |
| Risk of Death in the First 30 Days of Admission | Univariant Analysis | Multivariant Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | IC 2.5% | IC 97.5% | p Value | HR | IC 2.5% | IC 97.5% | p Value | |
| Completed Vaccination (ref = no) | 3.38 | 1.57 | 7.30 | <0.01 | ||||
| Age (years) | 1.10 | 1.06 | 1.14 | <0.01 | 1.10 | 1.06 | 1.14 | <0.01 |
| Charlson (ref = ≤ 1) | 4.51 | 2.11 | 9.65 | <0.01 | ||||
| Hypertension (ref = no) | 2.07 | 0.93 | 4.61 | 0.08 | ||||
| Heart failure (ref = no) | 3.11 | 1.17 | 8.23 | <0.03 | ||||
| Haematological disease (ref = no) | 3.46 | 1.46 | 8.23 | <0.01 | 2.99 | 1.26 | 7.11 | <0.02 |
| Dementia | 5.45 | 2.29 | 12.95 | <0.01 | ||||
| Risk of being discharged alive in the first 30 days of admission | Univariant analysis | Multivariant analysis | ||||||
| HR | IC 2.5% | IC 97.5% | p Valor | HR | IC 2.5% | IC 97.5% | p Value | |
| Completed Vaccination (ref = no) | 0.98 | 0.76 | 1.28 | 0.90 | 1.42 | 1.05 | 1.91 | <0.025 |
| Age(years) | 0.985 | 0.98 | 0.99 | <0.01 | 0.98 | 0.97 | 0.99 | <0.01 |
| Hypertension (ref = no) | 0.80 | 0.66 | 0.97 | 0.03 | ||||
| Haematological disease (ref = no) | 0.64 | 0.42 | 1.0 | 0.051 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Giardin, J.M.; Rivilla, M.; Mesa, N.; Morales, A.; Rivas, L.; Izquierdo, A.; Escribá, A.; San Martín, J.V.; Bernal-Bello, D.; Madroñal, E.; et al. Comparative Study of Vaccinated and Unvaccinated Hospitalised Patients: A Retrospective Population Study of 500 Hospitalised Patients with SARS-CoV-2 Infection in a Spanish Population of 220,000 Inhabitants. Viruses 2022, 14, 2284. https://doi.org/10.3390/v14102284
Ruiz-Giardin JM, Rivilla M, Mesa N, Morales A, Rivas L, Izquierdo A, Escribá A, San Martín JV, Bernal-Bello D, Madroñal E, et al. Comparative Study of Vaccinated and Unvaccinated Hospitalised Patients: A Retrospective Population Study of 500 Hospitalised Patients with SARS-CoV-2 Infection in a Spanish Population of 220,000 Inhabitants. Viruses. 2022; 14(10):2284. https://doi.org/10.3390/v14102284
Chicago/Turabian StyleRuiz-Giardin, José M., Marta Rivilla, Nieves Mesa, Alejandro Morales, Luis Rivas, Aída Izquierdo, Almudena Escribá, Juan V. San Martín, David Bernal-Bello, Elena Madroñal, and et al. 2022. "Comparative Study of Vaccinated and Unvaccinated Hospitalised Patients: A Retrospective Population Study of 500 Hospitalised Patients with SARS-CoV-2 Infection in a Spanish Population of 220,000 Inhabitants" Viruses 14, no. 10: 2284. https://doi.org/10.3390/v14102284