
Symptom-Based Predictive Model of COVID-19 Disease in Children

 ,
,  ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sampling
2.3. Data Sources and Setting
2.4. Case Definition
2.5. Recruitment Process
2.6. Ethical Considerations
2.7. Data Description
2.8. Pre-Processing
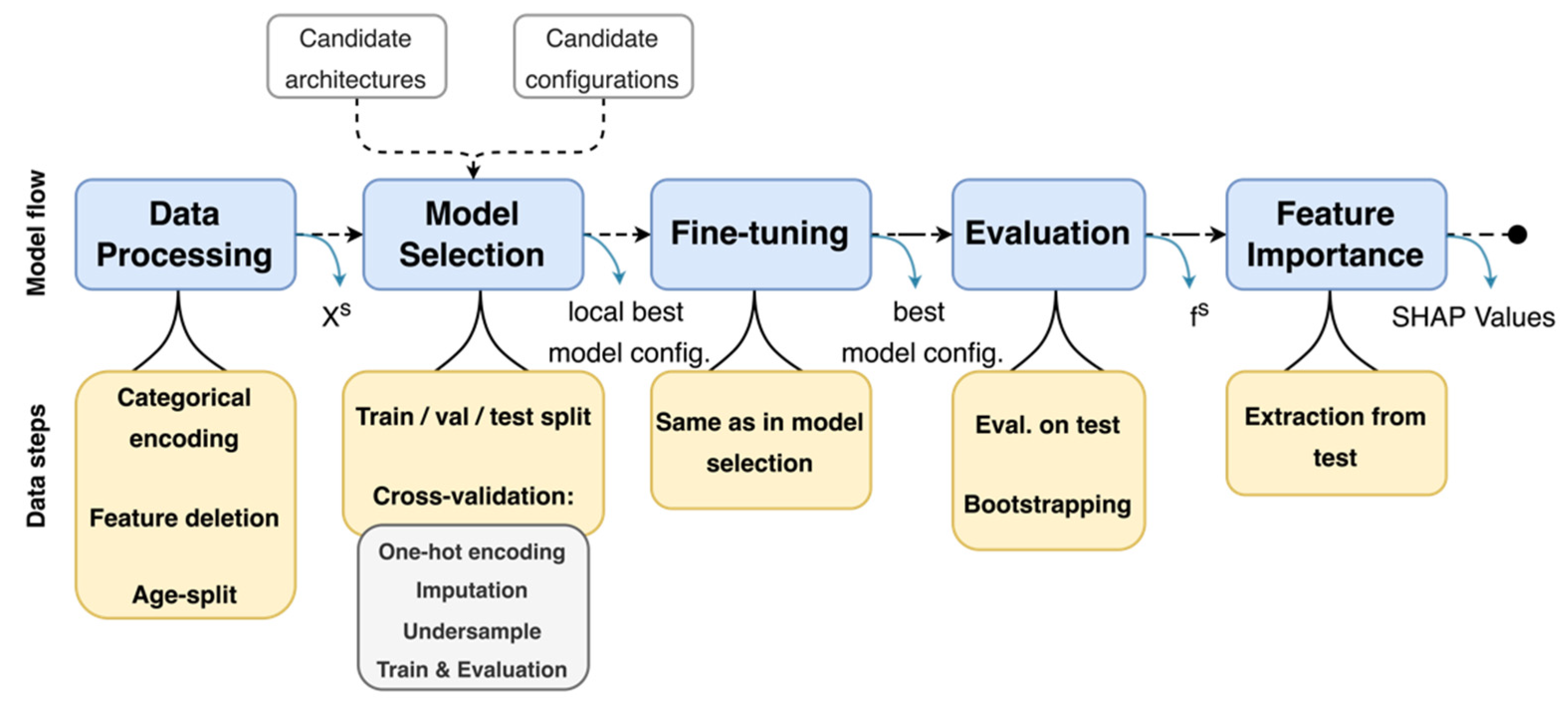
2.9. Methodology Implementation
2.10. Model Development
2.11. Feature Importance Extraction
3. Results
3.1. Data Description
3.2. Model Development
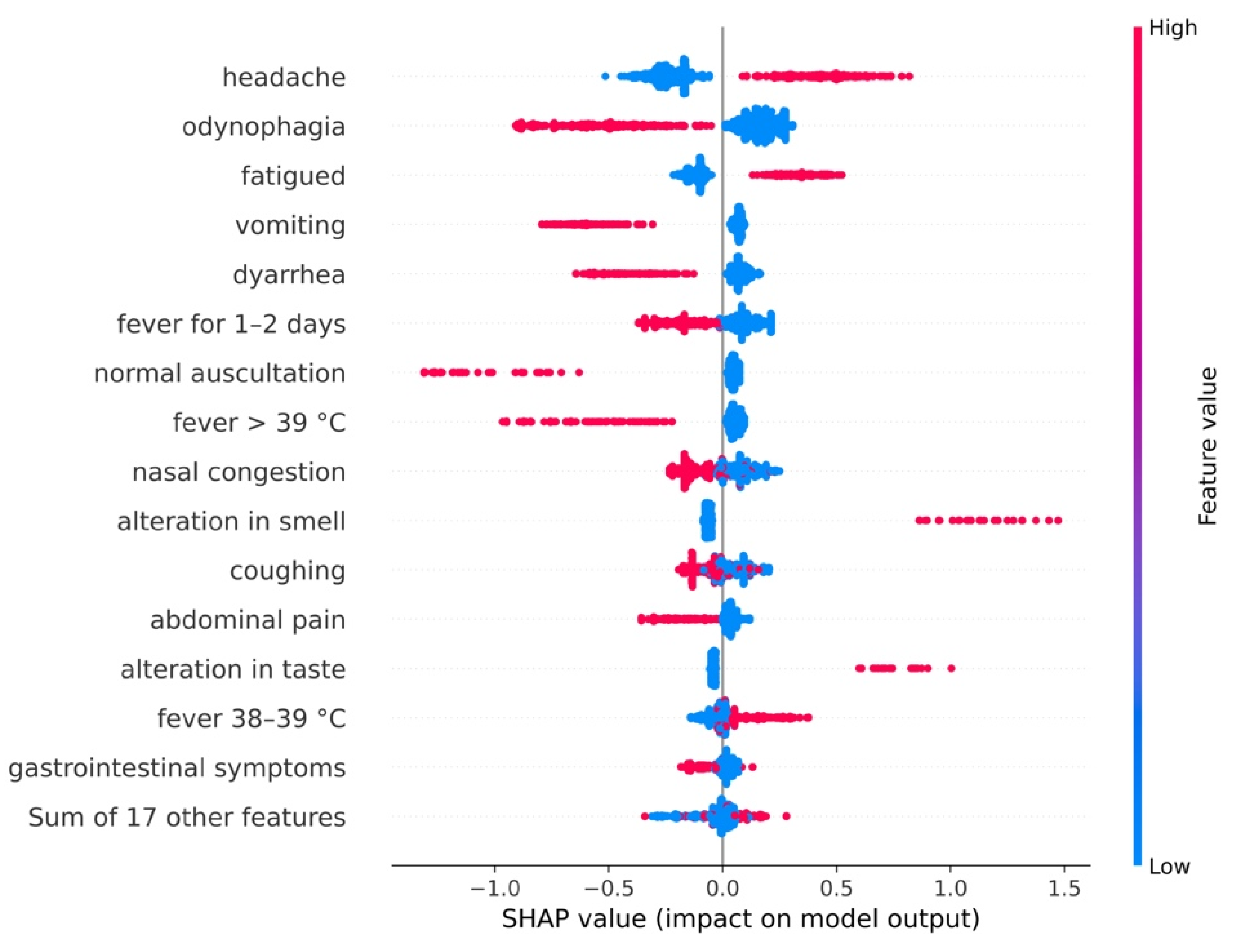
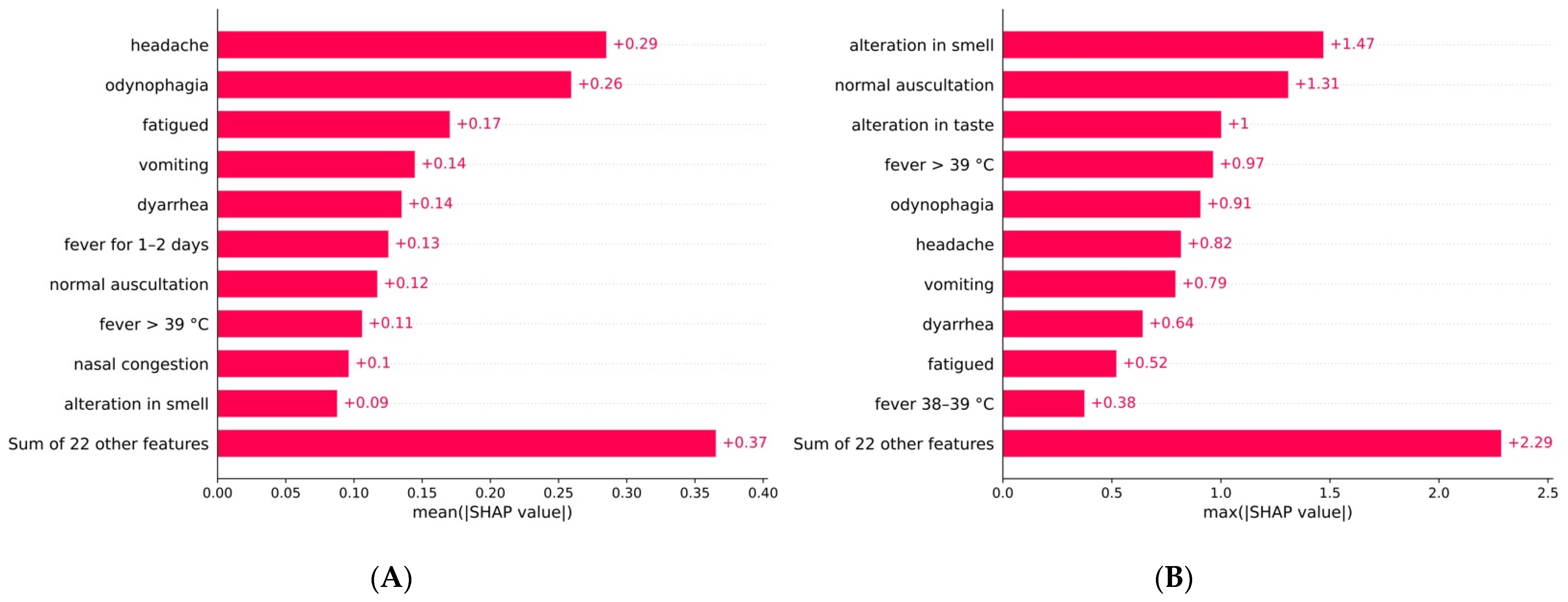
3.3. Feature Importance Extraction
3.3.1. General Model
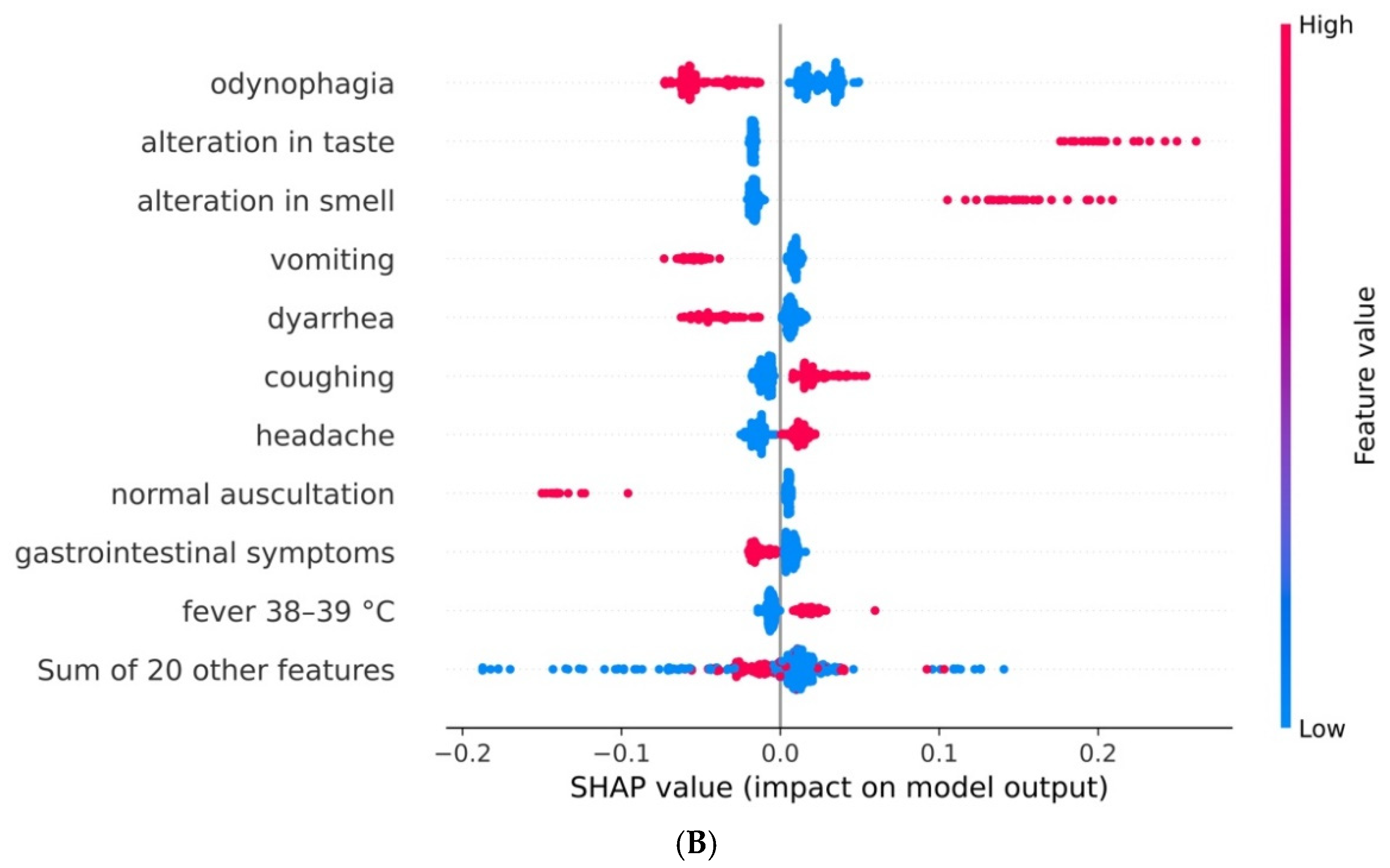
3.3.2. Model for Children by Age Range
4. Discussion
4.1. Main Results
4.2. Comparison with Prior Work
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Code Availability
References
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 15 October 2021).
- Dades Actualitzades SARS-CoV-2. Available online: https://aquas.gencat.cat/ca/actualitat/ultimes-dades-coronavirus (accessed on 1 October 2021).
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z. Epidemiological Characteristics of 2143 Pediatric Patients with 2019 Coronavirus Disease in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Soriano-Arandes, A.; Gatell, A.; Serrano, P. Household SARS-CoV-2 transmission and children: A network prospective study. Clin. Infect. Dis. 2021, 12, ciab228. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic. A Systematic Review. Ann. Intern Med. 2021, 174, 655–662. [Google Scholar] [CrossRef]
- Jernigan, J.A.; Low, D.E.; Hefland, R.F. Combining clinical and epidemiologic features for early recognition of SARS. Emerg Infect Dis. 2004, 10, 327–333. [Google Scholar] [CrossRef] [Green Version]
- Whiteside, T.; Kane, E.; Aljohani, B.; Alsamman, M.; Pourmand, A. Redesigning emergency department operations amidst a viral pandemic. Am. J. Emerg. Med. 2020, 38, 1448–1453. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Wang, M.; Song, H.; Shuo, G.; Zhou, Y.; Weimin, L.; Zhou, Y.; Li, M.; Song, X.; Zhou, Y.; et al. Development and utilization of an intelligent application for aiding COVID-19 diagnosis. MedRxiv 2020. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst. Rev. 2020, 7, CD013665. [Google Scholar] [CrossRef]
- Viner, R.M.; Ward, J.L.; Hudson, L.D.; Viner, R.M.; Ward, J.L.; Hudson, L.D.; Ashe, M.; Patel, S.V.; Hargreaves, D.; Whittaker, E. Systematic review of reviews of symptoms and signs of COVID-19 in children and adolescents. Arch. Dis. Child 2020, 106, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Tests Ràpids D’infeccions Respiratòries Pediàtriques. Available online: https://www.academia.cat/files/204-8709-FITXER/ProtocoltestsrapidsinfeccpeditriquesCatSalutDes20202.pdf (accessed on 17 November 2021).
- STROBE. Available online: https://www.strobe-statement.org (accessed on 17 November 2021).
- Perramon, A.; Soriano-Arandes, A.; Pino, D.; Lazcano, U.; Andrés, C.; Català, M.; Gatell, A.; Carulla, M.; Canadell, D.; Ricós, G.; et al. Schools as a Framework for COVID-19 Epidemiological Surveillance of Children in Catalonia, Spain: A Population-Based Study. Front. Pediatr. 2021, 9, 754744. [Google Scholar] [CrossRef]
- Analysis and Prediction of COVID-19 for EU-EFTA-UK and Other Countries. Available online: https://biocomsc.upc.edu/en/shared/20210521_report_233.pdf (accessed on 21 May 2021).
- SHAP. Available online: https://github.com/slundberg/shap (accessed on 20 March 2021).
- Shoer, S.; Karady, T.; Keshet, A.; Shilo, S.; Rossman, H.; Gavrieli, A.; Meir, T.; Lavon, A.; Kolobkov, D.; Kalka, I.; et al. A Prediction Model to Prioritize Individuals for a SARS-CoV-2 Test Built from National Symptom Surveys. Med 2021, 2, 196–208.e4. [Google Scholar] [CrossRef] [PubMed]
- Canas, L.S.; Sudre, C.H.; Capdevila Pujol, J.; Polidori, L.; Murray, B.; Molteni, E.; Graham, M.S.; Klaser, K.; Antonelli, M.; Berry, S.; et al. Early detection of COVID-19 in the UK using self-reported symptoms: A large-scale, prospective, epidemiological surveillance study. Lancet Digit. Health 2021, 3, e587–e598. [Google Scholar] [CrossRef]
- Gupta, R.K.; Harrison, E.M.; Ho, A.; Docherty, A.B.; Knight, S.R.; van Smeden, M.; Abubakar, I.; Lipman, M.; Quartagno, M.; Pius, R.; et al. Development and validation of the ISARIC 4C Deterioration model for adults hospitalised with COVID-19: A prospective cohort study. Lancet Respir. Med. 2021, 9, 349–359. [Google Scholar] [CrossRef]
- Wynants, L.; Sotgiu, G. Improving clinical management of COVID-19: The role of prediction models. Lancet Respir. Med. 2021, 9, 320–321. [Google Scholar] [CrossRef]
- Domínguez-Olmedo, J.L.; Gragera-Martínez, Á.; Mata, J.; Pachón Álvarez, V. Machine Learning Applied to Clinical Laboratory Data in Spain for COVID-19 Outcome Prediction: Model Development and Validation. J. Med. Internet. Res. 2021, 23, e26211. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Marks, M.; Samuels, T.H.A.; Luintel, A.; Rampling, T.; Chowdhury, H.; Quartagno, M.; Nair, A.; Lipman, M.; Abubakar, I.; et al. Systematic evaluation and external validation of 22 prognostic models among hospitalised adults with COVID-19: An observational cohort study. Eur. Respir. J. 2020, 56, 2003498. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Rodríguez, S.; Villaverde, S.; Sanz-Santaeufemia, F.J.; Grasa, C.; Soriano-Arandes, A.; Saavedra-Lozano, J.; Fumadó, V.; Epalza, C.; Serna-Pascual, M.; Alonso-Cadenas, J.A.; et al. A Bayesian Model to Predict COVID-19 Severity in Children. Pediatr. Infect. Dis. J. 2021, 40, e287–e293. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child. Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- King, J.A.; Whitten, T.A.; Bakal, J.A.; McAlister, F.A. Symptoms associated with a positive result for a swab for SARS-CoV-2 infection among children in Alberta. CMAJ 2021, 193, E1–E9. [Google Scholar] [CrossRef]
- Elliott, J.; Whitaker, M.; Bodinier, B.; Eales, O.; Riley, S.; Ward, H.; Cooke, G.; Darzi, A.; Chadeau-Hyam, M.; Elliott, P. Predictive symptoms for COVID-19 in the community: REACT-1 study of over 1 million people. PLoS Med. 2021, 18, e1003777. [Google Scholar] [CrossRef]
- Berger, A.; Nsoga, M.T.; Perez-Rodriguez, F.J.; Aad, Y.A.; Sattonnet-Roche, P.; Gayet-Ageron, A.; Jaksic, C.; Torriani, G.; Boehm, E.; Kronig, I.; et al. Diagnostic accuracy of two commercial SARS-CoV-2 antigen-detecting rapid tests at the point of care in community-based testing centers. PLoS ONE 2021, 16, e0248921. [Google Scholar] [CrossRef] [PubMed]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Chen, L.; Deng, J.; Murray, B.; Kerfoot, E.; Antonelli, M.S.; et al. Illness characteristics of COVID-19 in children infected with the SARS-CoV-2 Delta variant. medRxiv 2021. [Google Scholar] [CrossRef]
- Replication Package: Symptoms-Based Predictive Models of the COVID-19 Disease in Children. Available online: https://github.com/chus-chus/cov19-modeling (accessed on 16 November 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) | COVID-19 N (%) | No COVID-19 N (%) | p-Value |
|---|---|---|---|---|
| Sex (n = 4445) | ||||
| Male | 2461 (55.4) | 428 (55.9) | 2033 (55.3) | 0.78 |
| Female | 1984 (44.6) | 338 (44.1) | 1646 (44.7) | |
| Age (n = 4412) | ||||
| 0–5 | 1872 (42.4) | 315 (42.1) | 1557 (42.5) | 0.87 |
| 6–17 | 2540 (57.6) | 433 (57.9) | 2107 (57.5) | |
| Test performed (n = 4456) | ||||
| Yes | 4434 (99.5) | 764 (99.6) | 3670 (99.5) | 0.99 |
| No | 22 (0.5) | 3 (0.4) | 19 (0.5) | |
| PCR result (n = 840) | ||||
| Positive | 321 (38.2) | 321 (100.0) | 0 (0.0) | <0.001 |
| Negative | 519 (61.8) | 0 (0.0) | 494 (100.0) | |
| RDT result (n = 3916) | ||||
| Positive | 463 (11.8) | 463 (100.0) | 0 (0.0) | <0.001 |
| Negative | 3453 (88.2) | 0 (0.0) | 3453 (100.0) | |
| X-ray performed (n = 4328) | ||||
| Yes | 77 (1.8) | 15 (2.0) | 62 (1.7) | 0.54 |
| No | 4251 (98.2) | 731 (98.0) | 3520 (98.3) | |
| CT performed (n = 4263) | ||||
| Yes | 1 (0.02) | 1 (0.1) | 0 (0.0) | 0.17 |
| No | 4262 (99.98) | 730 (99.9) | 3532 (100.0) | |
| Use school bus (n = 3395) | ||||
| Yes | 121 (3.6) | 32 (5.5) | 89 (3.2) | 0.009 |
| No | 3274 (96.4) | 548 (94.5) | 2726 (96.8) | |
| Play sports (n = 3227) | ||||
| Yes | 376 (11.7) | 96 (17.1) | 280 (10.5) | <0.001 |
| No | 2851 (88.3) | 465 (82.9) | 2386 (89.5) | |
| Smokers at home (n = 4161) | ||||
| Yes | 1232 (29.6) | 197 (29.8) | 1035 (29.6) | 0.93 |
| No | 2929 (70.4) | 465 (70.2) | 2464 (70.4) | |
| Persons at home (n = 4230) | ||||
| ≤4 | 1360 (32.2) | 215 (29.9) | 1145 (32.6) | 0.17 |
| >4 | 2870 (67.8) | 503 (70.1) | 2367 (67.4) | |
| Suspected positive at home (n = 4456) | ||||
| Yes | 956 (21.4) | 494 (64.4) | 462 (12.5) | <0.001 |
| No | 3500 (78.6) | 273 (35.6) | 3227 (87.5) | |
| Confirmed positive at home (n = 4456) | ||||
| Yes | 548 (12.3) | 451 (58.8) | 97 (2.6) | <0.001 |
| No | 3908 (87.7) | 316 (41.2) | 3592 (97.4) | |
| Suspected positive at school (n = 4456) | ||||
| Yes | 338 (7.6) | 124 (16.2) | 214 (5.8) | <0.001 |
| No | 4118 (92.4) | 643 (83.8) | 3475 (94.2) | |
| Confirmed positive at school (n = 4456) | ||||
| Yes | 291 (6.5) | 125 (16.3) | 166 (4.5) | <0.001 |
| No | 4165 (93.5) | 642 (83.7) | 3523 (95.5) | |
| Co-viral infection (n = 2306) | ||||
| Yes | 14 (0.6) | 4 (2.3) | 10 (0.5) | 0.02 |
| No | 2292 (99.4) | 171 (97.7) | 2121 (99.5) | |
| Bacterial infection (n = 2363) | ||||
| Yes | 60 (2.5) | 11 (2.7) | 49 (2.5) | 0.73 |
| No | 2303 (97.5) | 390 (97.3) | 1913 (97.5) | |
| Comorbidities (n = 4456) | ||||
| Yes | 688 (15.4) | 129 (16.8) | 559 (15.2) | 0.25 |
| No | 3768 (84.6) | 638 (83.2) | 3130 (84.8) |
| Characteristic | Total N (%) | COVID-19 N (%) | No COVID-19 N (%) |
|---|---|---|---|
| Fever No 37.5 °C to <38 °C 38 °C to 39 °C >39 °C Unknown | 456 (43.51) 208 (19.85) 293 (29.96) 60 (5.73) 31 (2.96) | 219 (41.79) 122 (23.28) 141 (26.91) 22 (4.20) 20 (3.82) | 237 (45.23) 86 (16.41) 152 (29.01) 38 (7.25) 11 (2.10) |
| Cough No Yes Unknown | 574 (54.77) 441 (42.08) 33 (3.15) | 303 (57.82) 201 (38.36) 20 (3.82) | 271 (51.72) 240 (45.80) 13 (2.48) |
| Total days of fever None 1 or 2 days 3 to 7 days >7 days Unknown | 553 (52.77) 368 (35.11) 112 (10.69) 15 (1.43) - (-) | 279 (53.24) 188 (35.88) 48 (9.16) 9 (1.72) - (-) | 274 (52.29) 180 (34.35) 64 (12.21) 6 (1.15) - (-) |
| Auscultation Normal Pathological Unknown | 705 (67.27) 55 (5.25) 288 (27.48) | 351 (67.24) 2 (0.38) 169 (32.38) | 354 (67.56) 51 (9.73) 119 (22.71) |
| Auscultation type Normal Wheezing Crackles Both Unknown | 993 (94.75) 40 (3.82) 6 (0.57) 9 (0.86) - (-) | 520 (99.24) 4 (0.76) 0 (0) 0 (0) - (-) | 473 (90.44) 36 (6.88) 6 (1.15) 8 (1.53) - (-) |
| Dysphonia No Yes Unknown | 971 (92.65) 46 (4.39) 31 (2.96) | 486 (92.75) 18 (3.44) 20 (3.82) | 485 (92.56) 28 (5.34) 11 (2.10) |
| Respiratory sympt. No Yes Unknown | 954 (91.03) 56 (5.34) 38 (3.63) | 483 (92.18) 20 (3.82) 21 (4.01) | 471 (89.89) 36 (6.87) 17 (3.24) |
| Tachypnoea No Yes Unknown | 986 (94.08) 24 (2.29) 38 (3.63) | 497 (94.85) 2 (0.38) 25 (4.77) | 489 (93.32) 22 (4.20) 13 (2.48) |
| Odynophagia No Yes Unknown | 690 (65.84) 242 (23.09) 116 (11.07) | 359 (68.51) 114 (21.76) 51 (9.73) | 331 (63.17) 128 (24.43) 65 (12.40) |
| Congestion No Yes Unknown | 535 (51.05) 479 (45.71) 34 (3.24) | 285 (54.39) 216 (41.22) 23 (4.39) | 220 (44.53) 263 (53.24) 11 (2.23) |
| Fatigue No Yes Unknown | 692 (66.03) 277 (26.43) 79 (7.54) | 315 (60.11) 171 (32.63) 38 (7.25) | 377 (71.95) 106 (20.23) 41 (7.82) |
| Headache No Yes Unknown | 544 (51.91) 343 (32.73) 161 (15.36) | 225 (42.94) 232 (44.27) 67 (12.79) | 319 (60.88) 111 (21.18) 94 (17.94) |
| Conjunctivitis No Yes Unknown | 994 (94.85) 14 (1.34) 40 (3.82) | 488 (93.13) 9 (1.72) 27 (5.15) | 506 (96.56) 5 (0.95) 13 (2.48) |
| Gastro sympt. No Yes Unknown | 690 (65.84) 328 (31.3) 30 (2.86) | 350 (66.79) 154 (29.39) 20 (3.82) | 340 (64.89) 174 (33.21) 10 (1.91) |
| Abdominal sympt. No Yes Unknown | 833 (79.49) 200 (19.08) 15 (1.43) | 421 (80.34) 96 (18.32) 7 (1.34) | 412 (78.63) 104 (19.85) 8 (1.53) |
| Vomiting No Yes Unknown | 920 (87.79) 128 (12.21) - (-) | 479 (91.41) 45 (8.59) - (-) | 441 (84.16) 83 (15.84) - (-) |
| Diarrhoea No Yes Unknown | 879 (83.87) 168 (16.03) 1 (0.10) | 452 (86.26) 72 (13.74) 0 (0) | 427 (81.49) 96 (18.32) 1 (0.19) |
| Dermatologic No Yes Unknown | 980 (93.51) 28 (2.67) 40 (3.82) | 483 (92.18) 16 (3.05) 25 (4.77) | 497 (94.85) 12 (2.29) 15 (2.86) |
| Rash No Yes Unknown | 1032 (98.47) 16 (1.53) - (-) | 517 (98.66) 7 (1.34) - (-) | 515 (98.28) 9 (1.72) - (-) |
| Adenopathies No Yes Unknown | 726 (69.27) 10 (0.95) 312 (29.77) | 345 (65.84) 4 (0.76) 175 (33.40) | 381 (72.71) 6 (1.15) 137 (26.15) |
| Haemorrhages No Yes Unknown | 930 (88.74) 2 (0.19) 116 (11.07) | 456 (87.02) 1 (0.19) 67 (12.79) | 474 (90.46) 1 (0.19) 49 (9.35) |
| Irritability No Yes Unknown | 569 (54.29) 42 (4.01) 437 (41.70) | 292 (55.73) 22 (4.20) 210 (40.08) | 277 (52.86) 20 (3.82) 227 (43.32) |
| Neurological No Yes Unknown | 1010 (96.37) 6 (0.57) 32 (3.05) | 499 (95.23) 4 (0.76) 21 (4.01) | 511 (97.52) 2 (0.38) 11 (2.10) |
| Shock No Yes Unknown | 974 (92.94) 2 (0.29) 71 (6.78) | 489 (93.32) 0 (0) 35 (6.68) | 485 (92.56) 3 (0.57) 36 (6.87) |
| Absence of taste No Yes Unknown | 754 (71.95) 55 (5.25) 239 (22.81) | 386 (73.66) 49 (9.35) 89 (16.98) | 368 (70.23) 6 (1.15) 150 (28.63) |
| Absence of smell No Yes Unknown | 746 (71.18) 60 (5.73) 242 (23.09) | 380 (72.52) 55 (10.50) 89 (16.98) | 366 (69.85) 5 (0.95) 153 (29.20) |
| Architecture 1 | AUROC | Precision | Sensitivity | Specificity | F1 |
| XGB | 0.645 | 0.273 | 0.631 | 0.66 | 0.38 |
| RF | 0.644 | 0.278 | 0.607 | 0.680 | 0.381 |
| SVM | 0.627 | 0.289 | 0.507 | 0.747 | 0.367 |
| MLP | 0.567 | 0.253 | 0.496 | 0.637 | 0.264 |
| LR | 0.633 | 0.267 | 0.597 | 0.669 | 0.369 |
| Architecture 2 | AUROC | Precision | Sensitivity | Specificity | F1 |
| XGB | 0.577 | 0.141 | 0.558 | 0.596 | 0.225 |
| RF | 0.58 | 0.14 | 0.603 | 0.556 | 0.226 |
| SVM | 0.58 | 0.145 | 0.576 | 0.593 | 0.231 |
| MLP | 0.542 | 0.128 | 0.465 | 0.619 | 0.198 |
| LR | 0.564 | 0.134 | 0.562 | 0.567 | 0.216 |
| Architecture 3 | AUROC | Precision | Sensitivity | Specificity | F1 |
| XGB | 0.649 | 0.38 | 0.632 | 0.667 | 0.474 |
| RF | 0.652 | 0.377 | 0.663 | 0.641 | 0.479 |
| SVM | 0.651 | 0.378 | 0.653 | 0.65 | 0.477 |
| MLP | 0.596 | 0.33 | 0.588 | 0.605 | 0.419 |
| LR | 0.635 | 0.365 | 0.626 | 0.645 | 0.46 |
| Subset | Architecture | AUROC (95% CI) | Precision (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | F1 (95% CI) |
|---|---|---|---|---|---|---|
| All ages | XGB | 0.65 (0.62–0.67) | 0.66 (0.56–0.73) | 0.3 (0.27–0.33) | 0.65 (0.55–0.73) | 0.41 (0.38–0.43) |
| 0–5 year | RF | 0.63 (0.55–0.67) | 0.15 (0.13–0.19) | 0.65 (0.43–0.9) | 0.59 (0.38–0.74) | 0.25 (0.2–0.29) |
| 6–14 year | RF | 0.67 (0.64–0.69) | 0.36 (0.31–0.41) | 0.66 (0.56–0.75) | 0.68 (0.58–0.79) | 0.46 (0.43–0.49) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antoñanzas, J.M.; Perramon, A.; López, C.; Boneta, M.; Aguilera, C.; Capdevila, R.; Gatell, A.; Serrano, P.; Poblet, M.; Canadell, D.; et al. Symptom-Based Predictive Model of COVID-19 Disease in Children. Viruses 2022, 14, 63. https://doi.org/10.3390/v14010063
Antoñanzas JM, Perramon A, López C, Boneta M, Aguilera C, Capdevila R, Gatell A, Serrano P, Poblet M, Canadell D, et al. Symptom-Based Predictive Model of COVID-19 Disease in Children. Viruses. 2022; 14(1):63. https://doi.org/10.3390/v14010063
Chicago/Turabian StyleAntoñanzas, Jesús M., Aida Perramon, Cayetana López, Mireia Boneta, Cristina Aguilera, Ramon Capdevila, Anna Gatell, Pepe Serrano, Miriam Poblet, Dolors Canadell, and et al. 2022. "Symptom-Based Predictive Model of COVID-19 Disease in Children" Viruses 14, no. 1: 63. https://doi.org/10.3390/v14010063