
Association between SARS-CoV-2 Seroprevalence in Nursing Home Staff and Resident COVID-19 Cases and Mortality: A Cross-Sectional Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jordan, R.E.; Adab, P.; Cheng, K.K. Covid-19: Risk Factors for Severe Disease and Death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [Green Version]
- Comas-Herrera, A.; Zalakaín, J.; Lemmon, E.; Henderson, D.; Litwin, C.; Hsu, A.T.; Schmidt, A.E.; Arling, G.; Kruse, F.; Fernández, J.-L. Mortality Associated with COVID-19 in Care Homes: International Evidence; International Long-Term Care Policy Network; CPEC-LSE—Care Policy and Evaluation Centre: London, UK, 2021. [Google Scholar]
- Décès Liés au COVID-19 en Suisse et en Comparaison Internationale; Federal Office of Public Health: Bern, Switzerland, 2021.
- Bagchi, S.; Mak, J.; Li, Q.; Sheriff, E.; Mungai, E.; Anttila, A.; Soe, M.M.; Edwards, J.R.; Benin, A.L.; Pollock, D.A.; et al. Rates of COVID-19 among Residents and Staff Members in Nursing Homes—United States, May 25–November 22, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.J.; Barreiro, P.; San Román, J.; del Mar Carretero, M.; Sanz, J.C.; Pérez-Abeledo, M.; Ramos, B.; Viñuela-Prieto, J.M.; Canora, J.; Martínez-Peromingo, F.J.; et al. The Demography and Characteristics of SARS-CoV-2 Seropositive Residents and Staff of Nursing Homes for Older Adults in the Community of Madrid: The SeroSOS Study. Age Ageing 2021, 50, 1038–1047. [Google Scholar] [CrossRef] [PubMed]
- Abbas, M.; Robalo Nunes, T.; Cori, A.; Cordey, S.; Laubscher, F.; Baggio, S.; Jombart, T.; Iten, A.; Vieux, L.; Teixeira, D.; et al. Explosive Nosocomial Outbreak of SARS-CoV-2 in a Rehabilitation Clinic: The Limits of Genomics for Outbreak Reconstruction. J. Hosp. Infect. 2021, 117, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Kittang, B.R.; von Hofacker, S.; Solheim, S.P.; Krüger, K.; Løland, K.K.; Jansen, K. Outbreak of COVID-19 at Three Nursing Homes in Bergen. Tidsskr. Den. Nor. Laegeforening Tidsskr. Prakt. Med. Ny Raekke 2020, 140, 405. [Google Scholar] [CrossRef]
- Bayle, C.; Cantin, D.; Vidal, J.-S.; Sourdeau, E.; Slama, L.; Dumesges, N.; Trombert, S.; Ayllon, S.; Nguyen, J.-M.; Slama, D.; et al. Asymptomatic SARS COV-2 Carriers among Nursing Home Staff: A Source of Contamination for Residents? Infect. Dis. Now 2021, 51, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Rowland, T.A.J.; Whitaker, H.; Jeffery-Smith, A.; Lang, N.; Sendall, K.; McLaren, R.; Brown, K.E.; Ramsay, M.; Ladhani, S.N.; Zambon, M. Seropositivity and Risk Factors for SARS-CoV-2 Infection in Staff Working in Care Homes during the COVID-19 Pandemic. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Stringhini, S.; Zaballa, M.-E.; Pullen, N.; de Mestral, C.; Perez-Saez, J.; Dumont, R.; Picazio, A.; Pennacchio, F.; Dibner, Y.; Yerly, S.; et al. Large Variation in Anti-SARS-CoV-2 Antibody Prevalence among Essential Workers in Geneva, Switzerland. Nat. Commun. 2021, 12, 3455. [Google Scholar] [CrossRef] [PubMed]
- Richard, A.; Wisniak, A.; Perez-Saez, J.; Garrison-Desany, H.; Petrovic, D.; Piumatti, G.; Baysson, H.; Picazio, A.; Pennacchio, F.; Ridder, D.D.; et al. Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies, Risk Factors for Infection and Associated Symptoms in Geneva, Switzerland: A Population-Based Study. medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Nursing Home Data. Available online: https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg/ (accessed on 14 July 2021).
- Stacey, K.; Ghiglione, D.; Solomon, E.; Abboud, L. Vaccine Scepticism among Medics Sparks Alarm in Europe and US. Financial Times, 7 January 2021. [Google Scholar]
- COVID-19. Point Épidémiologique Hebdomadaire n° 68 du 17 juin 2021; Santé Publique France: Saint-Maurice, France, 2021; p. 41.
- Nouveau Coronavirus (COVID-19) Critères de Suspicion, de Prélèvement D’échantillons et de Déclaration Etat: 16.04.2020; Federal Office of Public Health: Bern, Switzerland, 2020.
- Gorges, R.J.; Konetzka, R.T. Staffing Levels and COVID-19 Cases and Outbreaks in U.S. Nursing Homes. J. Am. Geriatr. Soc. 2020, 68, 2462–2466. [Google Scholar] [CrossRef] [PubMed]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; Ridder, D.D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies in Geneva, Switzerland (SEROCoV-POP): A Population-Based Study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Domi, M.; Leitson, M.; Gifford, D.; Nicolaou, A.; Sreenivas, K.; Bishnoi, C. The BNT162b2 Vaccine Is Associated with Lower New COVID-19 Cases in Nursing Home Residents and Staff. J. Am. Geriatr. Soc. 2021, 69, 2079–2089. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Sample | Range by Nursing Home | Median (IQR) by Nursing Home | |
|---|---|---|---|
| Nursing homes (N = 25) | |||
| Number of beds | 2317 | 48–235 | 80 (60–92) |
| Occupation rate (%) | 96.9% | 77.1–100% | 98.6% (96.6–99.7) |
| Staff (N = 3167) | |||
| Participating staff (n) | 1071 | 12–126 | 39 (20–50) |
| Participation rate (%) | 33.8% | 16.0–61.3% | 32.2% (20.8–45.9) |
| Seropositive staff (n) | 154 | 0–22 | 3 (1–8) |
| Staff seroprevalence (%) | 14.4% | 0.0–31.4% | 12.5% (4.4–20.5) |
| PCR-confirmed COVID-19 cases (n) | 5 | 0–1 | 0 (0–0) |
| % staff with PCR-confirmed COVID-19 | 0.16% | 0.0–1.4% | 0.0% (0.0–0.0) |
| Residents | |||
| PCR-confirmed COVID-19 cases (n) | 229 | 0–83 | 5 (0–12) |
| Cumulative incidence of COVID-19 cases * | 0.56 | 0.00–2.15 | 0.36 (0.00–0.69) |
| Number of COVID-19 hospitalizations | 25 | 0–7 | 0 (0–2) |
| Cumulative incidence of hospitalizations | 0.06 | 0.00–0.21 | 0.00 (0.00–0.10) |
| Number of COVID-19 deaths † | 89 | 0–33 | 1 (0–4) |
| Cumulative incidence of deaths *† | 0.22 | 0.00–0.85 | 0.07 (0.00–0.19) |
| Outcome | Correlation | Quasi-Poisson Regression 1 |
|---|---|---|
| Spearman’s coefficient (95% CI) | Incidence rate ratio (95% CI) | |
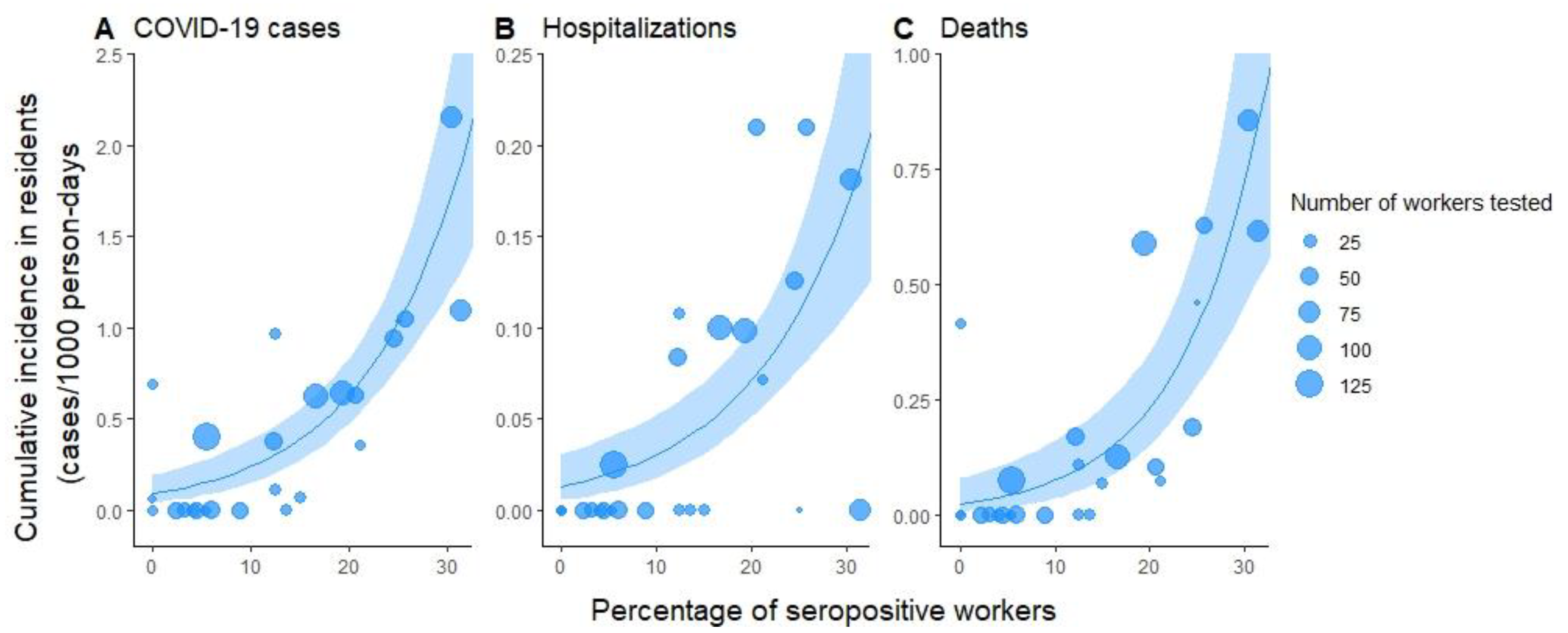
| COVID-19 cases | 0.72 (0.45–0.87) * | 1.10 (1.07–1.14) * |
| Hospitalizations | 0.59 (0.25–0.80) ** | 1.09 (1.05–1.13) * |
| Deaths | 0.71 (0.44–0.86) * | 1.12 (1.07–1.18) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wisniak, A.; Menon, L.K.; Dumont, R.; Pullen, N.; Regard, S.; Dubos, R.; Zaballa, M.-E.; Baysson, H.; Courvoisier, D.; Kaiser, L.; et al. Association between SARS-CoV-2 Seroprevalence in Nursing Home Staff and Resident COVID-19 Cases and Mortality: A Cross-Sectional Study. Viruses 2022, 14, 43. https://doi.org/10.3390/v14010043
Wisniak A, Menon LK, Dumont R, Pullen N, Regard S, Dubos R, Zaballa M-E, Baysson H, Courvoisier D, Kaiser L, et al. Association between SARS-CoV-2 Seroprevalence in Nursing Home Staff and Resident COVID-19 Cases and Mortality: A Cross-Sectional Study. Viruses. 2022; 14(1):43. https://doi.org/10.3390/v14010043
Chicago/Turabian StyleWisniak, Ania, Lakshmi Krishna Menon, Roxane Dumont, Nick Pullen, Simon Regard, Richard Dubos, María-Eugenia Zaballa, Hélène Baysson, Delphine Courvoisier, Laurent Kaiser, and et al. 2022. "Association between SARS-CoV-2 Seroprevalence in Nursing Home Staff and Resident COVID-19 Cases and Mortality: A Cross-Sectional Study" Viruses 14, no. 1: 43. https://doi.org/10.3390/v14010043