
Comparison of Antigen Tests and qPCR in Rapid Diagnostics of Infections Caused by SARS-CoV-2 Virus

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory Tests
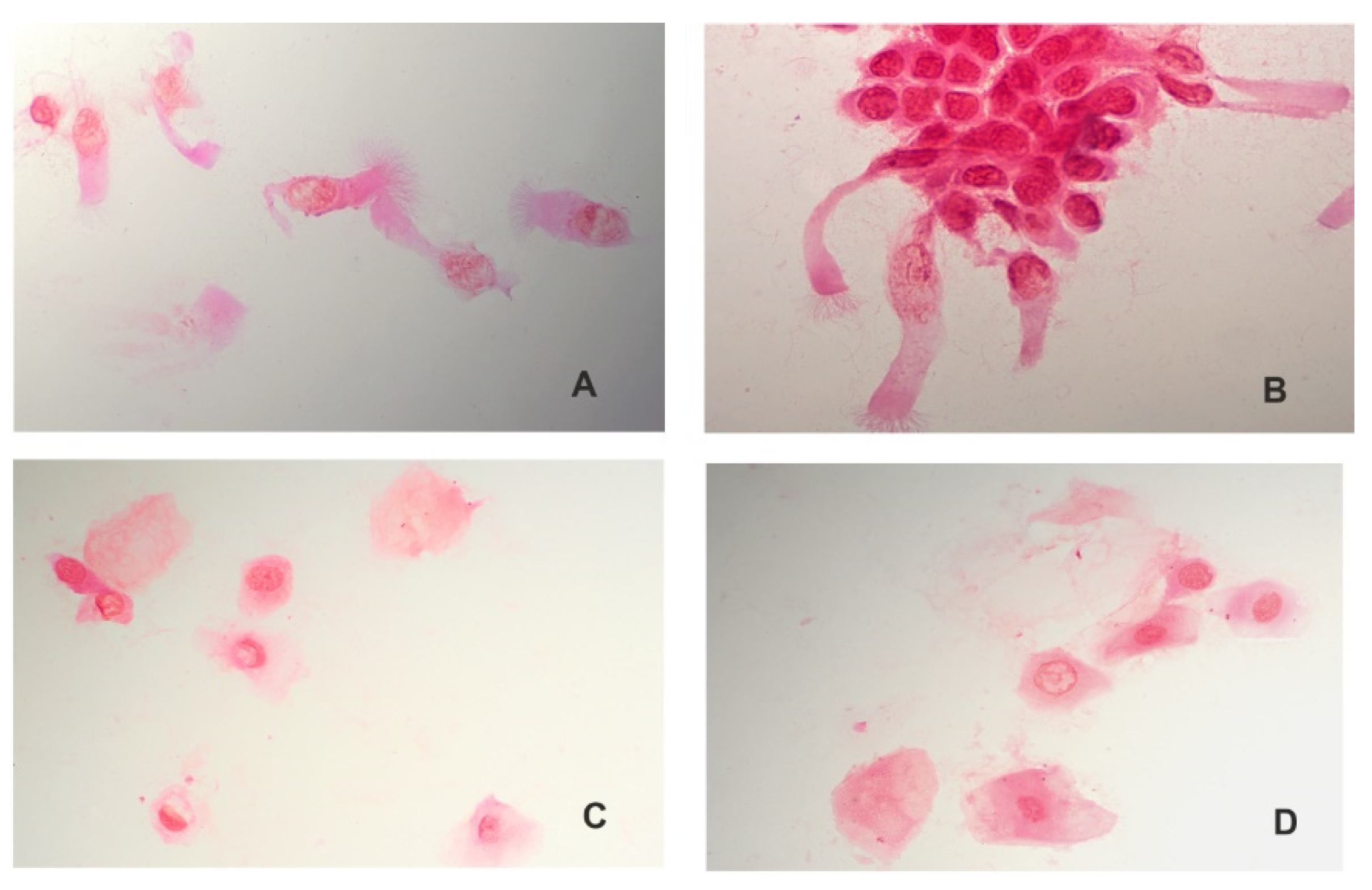
2.3. Microscopic Analysis
2.4. qPCR
2.5. SARS-CoV-2 Virus Antigen Detection
2.6. Statistical Analysis
3. Results
3.1. Microscopic Analysis
3.2. Humasis COVID-19 Ag Test and Vitassay qPCR SARS-CoV-2 Kit Results
3.3. Positive qPCR Results
3.4. Negative qPCR Results
3.5. Positive Results in the Antigen Test and Negative Results in the qPCR Test
4. Discussion
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van der Hoek, L.; Pyrc, K.; Jebbink, M.F.; Vermeulen-Oost, W.; Berkhout, R.J.; Wolthers, K.C.; Wertheim-van Dillen, P.M.; Kaandorp, J.; Spaargaren, J.; Berkhout, B. Identification of a new human coronavirus. Nat. Med. 2004, 10, 368–373. [Google Scholar] [CrossRef]
- Tyrrell, D.A.; Bynoe, M.L. Cultivation of a novel type of common-cold virus in organ cultures. Br. Med. J. 1965, 1, 1467–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamre, D.; Procknow, J.J. A new virus isolated from the human respiratory tract. Proc. Soc. Exp. Biol. Med. 1966, 121, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.C.; Lau, S.K.; Chu, C.M.; Chan, K.H.; Tsoi, H.W.; Huang, Y.; Wong, B.H.; Poon, R.W.; Cai, J.J.; Luk, W.K.; et al. Characterization and complete genome sequence of a novel coronavirus, coronavirus HKU1, from patients with pneumonia. J. Virol. 2005, 79, 884–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groot, R.J.; Baker, S.C.; Baric, R.S.; Brown, C.S.; Drosten, C.; Enjuanes, L.; Fouchier, R.A.; Galiano, M.; Gorbalenya, A.E.; Memish, Z.A.; et al. Middle East respiratory syndrome coronavirus (MERS-CoV): Announcement of the Coronavirus Study Group. J. Virol. 2013, 87, 7790–7792. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Shi, Z.; Yu, M.; Ren, W.; Smith, C.; Epstein, J.H.; Wang, H.; Crameri, G.; Hu, Z.; Zhang, H.; et al. Bats are natural reservoirs of SARS-like coronaviruses. Science 2005, 310, 676–679. [Google Scholar] [CrossRef]
- Memish, Z.A.; Perlman, S.; Van Kerkhove, M.D.; Zumla, A. Middle East respiratory syndrome. Lancet 2020, 395, 1063–1077. [Google Scholar] [CrossRef]
- Singh, S.K. Middle East Respiratory Syndrome Virus Pathogenesis. Semin. Respir. Crit. Care Med. 2016, 37, 572–577. [Google Scholar] [CrossRef] [Green Version]
- Senga, M.; Arabi, Y.M.; Fowler, R.A. Clinical spectrum of the Middle East respiratory syndrome coronavirus (MERS-CoV). J. Infect. Public Health 2017, 10, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.M.; Moon, S.Y.; Yang, H.I.; Kim, K.S. Understanding Viral Infection Mechanisms and Patient Symptoms for the Development of COVID-19 Therapeutics. Int. J. Mol. Sci. 2021, 22, 1737. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Laboratory Testing for Coronavirus Disease 2019 (COVID-19) in Suspected Human Cases: Interim Guidance. World Health Organization. 2020. Available online: https://apps.who.int/iris/handle/10665/331329 (accessed on 17 July 2021).
- Safiabadi Tali, S.H.; LeBlanc, J.J.; Sadiq, Z.; Oyewunmi, O.D.; Camargo, C.; Nikpour, B.; Armanfard, N.; Sagan, S.M.; Jahanshahi-Anbuhi, S. Tools and Techniques for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)/COVID-19 Detection. Clin. Microbiol. Rev. 2021, 34, e00228-20. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, Overview of Testing for SARS-CoV-2 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html (accessed on 17 July 2021).
- The Foundation for Innovative Diagnostics. FIND. SARS-CoV-2 Diagnostic Pipeline. Available online: www.finddx.org/covid-19/pipeline/ (accessed on 8 December 2021).
- World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection. World Health Organization. 2021. Available online: https://apps.who.int/iris/handle/10665/345948 (accessed on 22 December 2021).
- Turcato, G.; Zaboli, A.; Pfeifer, N.; Sibilio, S.; Tezza, G.; Bonora, A.; Ciccariello, L.; Ausserhofer, D. Rapid antigen test to identify COVID-19 infected patients with and without symptoms admitted to the Emergency Department. Am. J. Emerg. Med. 2021, 51, 92–97, Advance online publication. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Orris, S.; Freeman, T.; Freeman, M.C.; Adam, M.; Axe, M.; Gribschaw, J.; Suyama, J.; Hoberman, A.; Wells, A. Performance of SARS-CoV-2 antigen testing in symptomatic and asymptomatic adults: A single-center evaluation. BMC Infect. Dis. 2021, 21, 1071. [Google Scholar] [CrossRef]
- Sungnak, W.; Huang, N.; Bécavin, C.; Berg, M.; Queen, R.; Litvinukova, M.; Talavera-López, C.; Maatz, H.; Reichart, D.; Sampaziotis, F.; et al. HCA Lung Biological Network. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat. Med. 2020, 26, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Available online: www.aotm.gov.pl/media/2021/05/Diagnostyka-COVID-19-%E2%80%93-Aktualizacja-Zalecen-wersja-2.1-27-maja-2021-r..pdf (accessed on 30 November 2021).
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [Green Version]
- Chaimayo, C.; Kaewnaphan, B.; Tanlieng, N.; Athipanyasilp, N.; Sirijatuphat, R.; Chayakulkeeree, M.; Angkasekwinai, N.; Sutthent, R.; Puangpunngam, N.; Tharmviboonsri, T.; et al. Rapid SARS-CoV-2 antigen detection assay in comparison with real-time RT-PCR assay for laboratory diagnosis of COVID-19 in Thailand. Virol. J. 2020, 17, 177. [Google Scholar] [CrossRef]
- Porte, L.; Legarraga, P.; Vollrath, V.; Aguilera, X.; Munita, J.M.; Araos, R.; Pizarro, G.; Vial, P.; Iruretagoyena, M.; Dittrich, S.; et al. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int. J. Infect. Dis. 2020, 99, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Linares, M.; Pérez-Tanoira, R.; Carrero, A.; Romanyk, J.; Pérez-García, F.; Gómez-Herruz, P.; Arroyo, T.; Cuadros, J. Panbio antigen rapid test is reliable to diagnose SARS-CoV-2 infection in the first 7 days after the onset of symptoms. J. Clin. Virol. 2020, 133, 104659. [Google Scholar] [CrossRef]
- Xiao, A.T.; Tong, Y.X.; Zhang, S. Profile of RT-PCR for SARS-CoV-2: A Preliminary Study from 56 COVID-19 Patients. Clin. Infect. Dis. 2020, 71, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.W.; Imöhl, M.; Kleines, M. Comparison of the SARS-CoV-2 Rapid antigen test to the real star SARS-CoV-2 RT PCR kit. J. Virol. Methods 2021, 288, 114024. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Test Result | qPCR Test | |||
|---|---|---|---|---|
| Positive | Negative | Total | ||
| Humasis COVID-19 Ag Test | Positive | 43 | 2 | 45 |
| Negative | 4 | 140 | 144 | |
| Total | 47 | 142 | 189 | |
| qPCR Test | ORF 1ab Gene Ct Values | N Gene Ct Values | Humasis COVID-19 Ag Test |
|---|---|---|---|
| Positive | 29.95 | 37.87 | Positive |
| Positive | 15.16 | 21.04 | Positive |
| Positive | 11.49 | 15.56 | Positive |
| Positive | 18.97 | 23.89 | Positive |
| Positive | 11.46 | 15.55 | Positive |
| Positive | 19.60 | 17.90 | Positive |
| Positive | 26.62 | 23.42 | Positive |
| Positive | 24.55 | 39.46 | Positive |
| Positive | 22.97 | 23.93 | Positive |
| Positive | 16.65 | 24.20 | Positive |
| Positive | 31.72 | 32.95 | Positive |
| Positive | 18.47 | 23.72 | Positive |
| Positive | 21.44 | 22.39 | Positive |
| Positive | 20.84 | 21.07 | Positive |
| Positive | 15.64 | 28.48 | Positive |
| Positive | 18.47 | 23.72 | Positive |
| Positive | 21.22 | 21.89 | Positive |
| Positive | 17.72 | 22.90 | Positive |
| Positive | 23.93 | 23.73 | Positive |
| Positive | 16.16 | 19.84 | Positive |
| Positive | 22.19 | 21.38 | Positive |
| Positive | 24.08 | 24.27 | Positive |
| Positive | 30.46 | 24.29 | Positive |
| Positive | 28.04 | 31.07 | Positive |
| Positive | 33.37 | 31.03 | Positive |
| Positive | 30.42 | 24.90 | Positive |
| Positive | 28.31 | 28.11 | Positive |
| Positive | 24.89 | 25.65 | Positive |
| Positive | 24.05 | 26.11 | Positive |
| Positive | 14.35 | 16.64 | Positive |
| Positive | 18.57 | 24.37 | Positive |
| Positive | 22.89 | 24.54 | Positive |
| Positive | 11.95 | 11.56 | Positive |
| Positive | 11.12 | 17.83 | Positive |
| Positive | 22.24 | 24.65 | Positive |
| Positive | 29.76 | 28.20 | Positive |
| Positive | 28.78 | 26.06 | Positive |
| Positive | 17.72 | 22.90 | Positive |
| Positive | 18.37 | 17.48 | Positive |
| Positive | 22.12 | 23.76 | Positive |
| Positive | 19.81 | 24.99 | Positive |
| Positive | 27.25 | 24.35 | Positive |
| Positive | 23.10 | 24.27 | Positive |
| Positive | 31.80 | 23.90 | Negative |
| Positive | 32.81 | 31.02 | Negative |
| Positive | 35.10 | 33.21 | Negative |
| Positive | 34.20 | 33.61 | Negative |
| Value | 95% CI | |
|---|---|---|
| Sensitivity | 91.49% | 79.62–97.63% |
| Specificity | 97.90% | 93.99–99.57% |
| PPV | 93.48% | 82.10–98.63% |
| NPV | 97.22% | 93.04–99.24% |
| LR+ | 43.61 | 14.19–134.07 |
| LR- | 0.09 | 0.03–0.22 |
| Accuracy | 96.32% | 92.56–98.51% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klajmon, A.; Olechowska-Jarząb, A.; Salamon, D.; Sroka-Oleksiak, A.; Brzychczy-Włoch, M.; Gosiewski, T. Comparison of Antigen Tests and qPCR in Rapid Diagnostics of Infections Caused by SARS-CoV-2 Virus. Viruses 2022, 14, 17. https://doi.org/10.3390/v14010017
Klajmon A, Olechowska-Jarząb A, Salamon D, Sroka-Oleksiak A, Brzychczy-Włoch M, Gosiewski T. Comparison of Antigen Tests and qPCR in Rapid Diagnostics of Infections Caused by SARS-CoV-2 Virus. Viruses. 2022; 14(1):17. https://doi.org/10.3390/v14010017
Chicago/Turabian StyleKlajmon, Adrianna, Aldona Olechowska-Jarząb, Dominika Salamon, Agnieszka Sroka-Oleksiak, Monika Brzychczy-Włoch, and Tomasz Gosiewski. 2022. "Comparison of Antigen Tests and qPCR in Rapid Diagnostics of Infections Caused by SARS-CoV-2 Virus" Viruses 14, no. 1: 17. https://doi.org/10.3390/v14010017