
Modeling the Transmission of the SARS-CoV-2 Delta Variant in a Partially Vaccinated Population


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Derivation of the Mathematical Model of a Partially-Vaccinated Population of the United States
2.3. Estimation of Parameters Related to an Imperfect Vaccine
2.4. Estimation of the Function to Predict Vaccination in the following Months
2.5. Estimation of the Parameters of the Outbreak of the Delta Virus in the US
2.6. Estimation of the Control Reproduction Number
2.7. Local Sensitivity Analysis of the Parameters of the Mathematical Model
2.8. Global Sensitivity Analysis of the Mathematical Model
3. Results
3.1. Modeling the SARS-CoV-2 Delta Variant Spread in a Partially Vaccinated Population
3.2. Spread of the Delta Variant under Different Transmission and Vaccination Rates
3.3. Vaccine Effectiveness and New Infections in Vaccinated vs. Unvaccinated Individuals
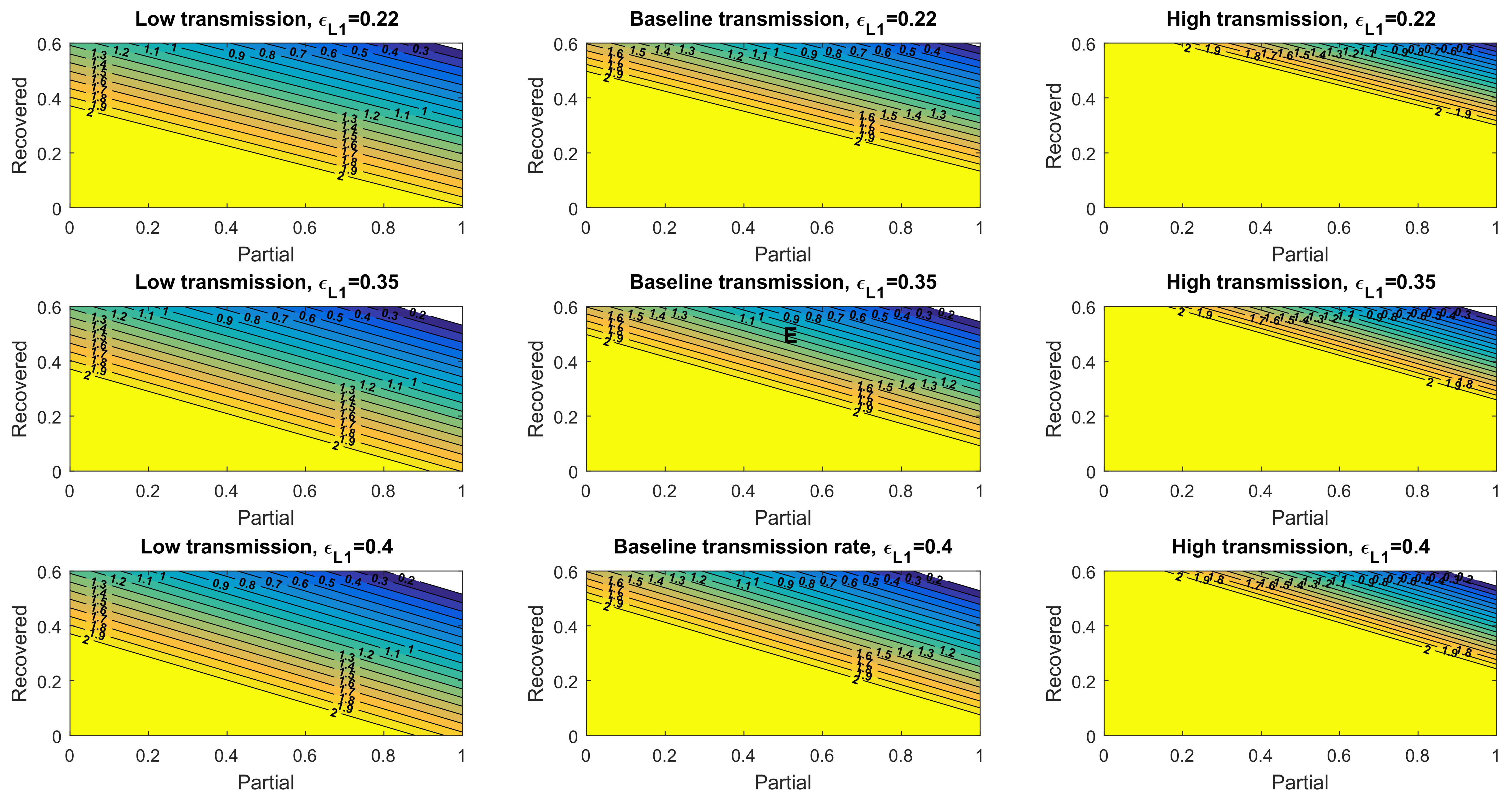
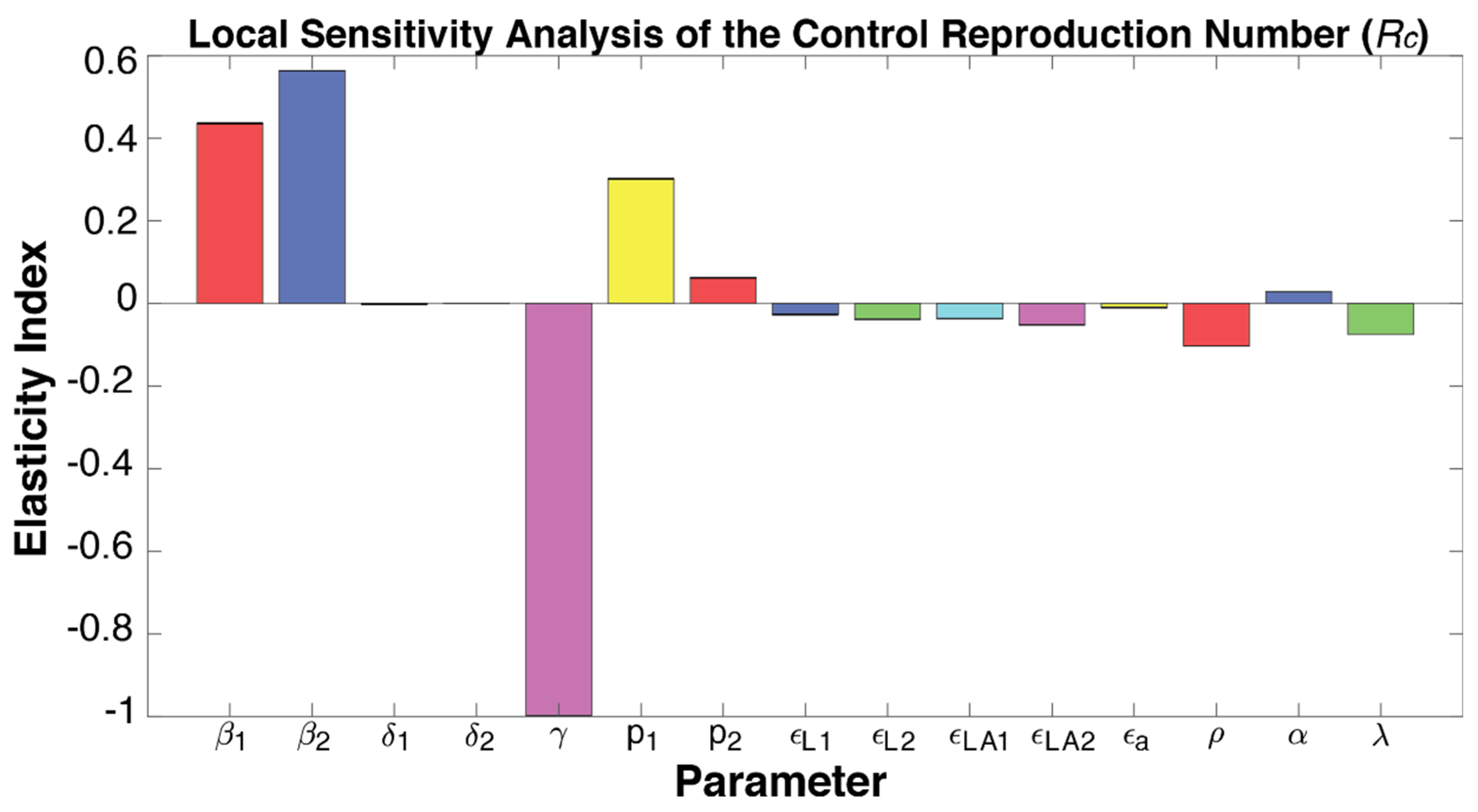
3.4. The Control Reproduction Number Mediated by Natural and Vaccine-Induced Immunity
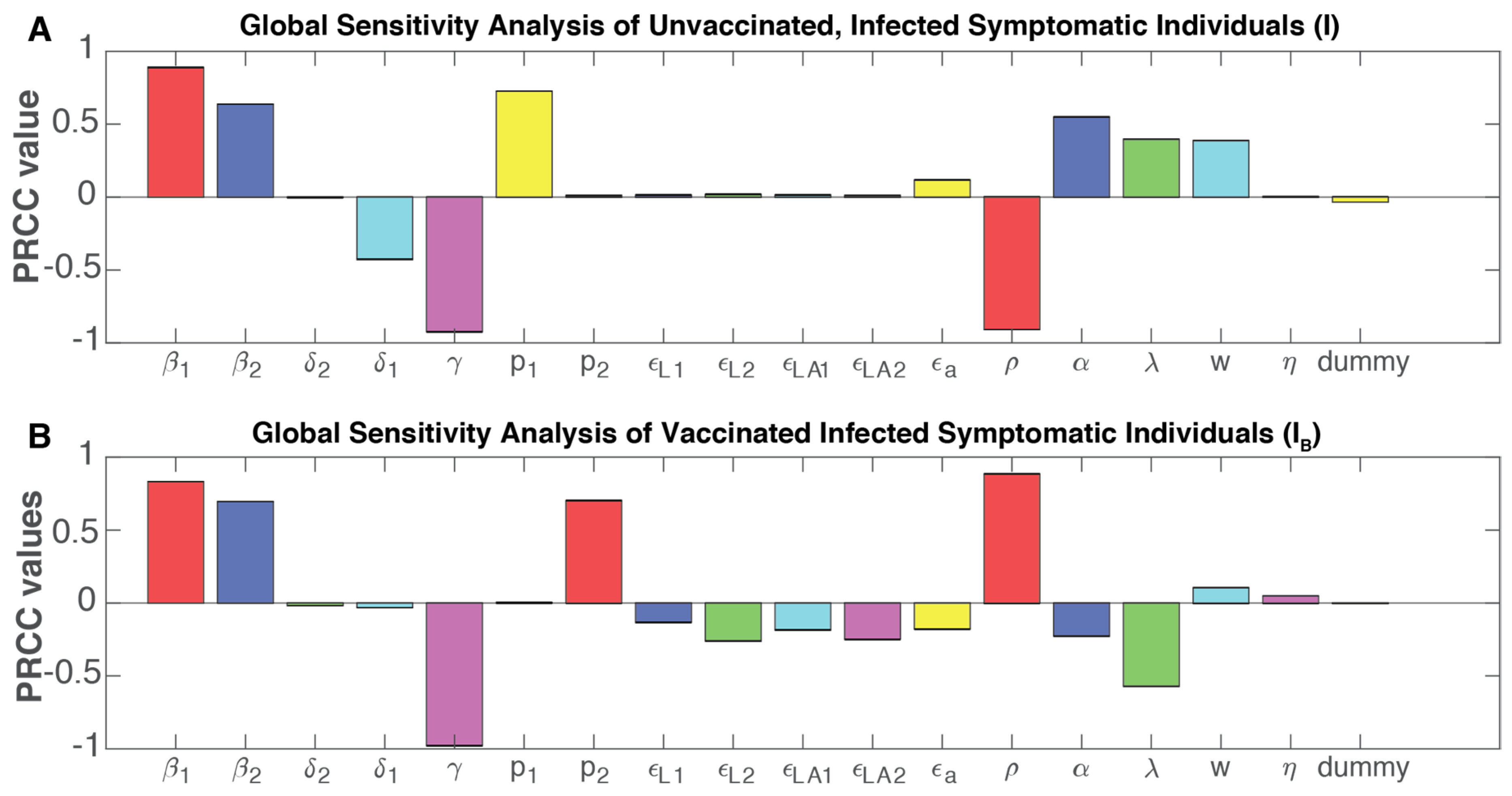
3.5. Sensitivity Analyses of Model Parameters Affecting the Pandemic Trajectories
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Mathematical Model with Asymptomatic Individuals and Vaccination
Appendix A.2. Control Reproduction Number with a Disease-Free Equilibrium
Appendix A.3. Control Reproduction Number for the Delta Variant
References
- Dong, E.; Du, H.; Gardner, L. An Interactive Web-Based Dashboard to Track COVID-19 in Real Time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the Effectiveness of Worldwide COVID-19 Government Interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Perra, N. Non-Pharmaceutical Interventions during the COVID-19 Pandemic: A Review. Phys. Rep. 2021, 913, 1–52. [Google Scholar] [CrossRef] [PubMed]
- IHME COVID-19 Forecasting Team. Modeling COVID-19 Scenarios for the United States. Nat. Med. 2021, 27, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Gondim, J.A.M. Preventing Epidemics by Wearing Masks: An Application to COVID-19. Chaos Solitons Fractals 2021, 143, 110599. [Google Scholar] [CrossRef]
- Perkins, T.A.; España, G. Optimal Control of the COVID-19 Pandemic with Non-Pharmaceutical Interventions. Bull. Math. Biol. 2020, 82, 118. [Google Scholar] [CrossRef] [PubMed]
- Ngonghala, C.N.; Iboi, E.A.; Gumel, A.B. Could Masks Curtail the Post-Lockdown Resurgence of COVID-19 in the US? Math. Biosci. 2020, 329, 108452. [Google Scholar] [CrossRef]
- Childs, M.L.; Kain, M.P.; Kirk, D.; Harris, M.; Couper, L.; Nova, N.; Delwel, I.; Ritchie, J.; Mordecai, E.A. The Impact of Long-Term Non-Pharmaceutical Interventions on COVID-19 Epidemic Dynamics and Control. medRxiv Preprint 2020. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Humer, E.; Probst, T. Comparing Mental Health During the COVID-19 Lockdown and 6 Months After the Lockdown in Austria: A Longitudinal Study. Front. Psychiatry 2021, 12, 625973. [Google Scholar] [CrossRef]
- Callaway, E. What Pfizer’s Landmark COVID Vaccine Results Mean for the Pandemic. Nature 2020. [Google Scholar] [CrossRef]
- Wang, W.; Wu, Q.; Yang, J.; Dong, K.; Chen, X.; Bai, X.; Chen, X.; Chen, Z.; Viboud, C.; Ajelli, M.; et al. Global, Regional, and National Estimates of Target Population Sizes for COVID-19 Vaccination: Descriptive Study. BMJ 2020, 371, m4704. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Hodcroft, E.B. Genetic Variants of SARS-CoV-2—What Do They Mean? JAMA 2021, 325, 529–531. [Google Scholar] [CrossRef]
- Panovska-Griffiths, J. Can Mathematical Modelling Solve the Current COVID-19 Crisis? BMC Public Health 2020, 20, 551. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Parra, G.; Martínez-Rodríguez, D.; Villanueva-Micó, R.J. Impact of a New SARS-CoV-2 Variant on the Population: A Mathematical Modeling Approach. Math. Comput. Appl. 2021, 26, 25. [Google Scholar] [CrossRef]
- Elbe, S.; Buckland-Merrett, G. Data, Disease and Diplomacy: GISAID’s Innovative Contribution to Global Health. Glob. Chall. 2017, 1, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Eurosurveillance Editorial Team. Eurosurveillance editorial team Updated Rapid Risk Assessment from ECDC on the Risk Related to the Spread of New SARS-CoV-2 Variants of Concern in the EU/EEA—First Update. Eurosurveillance 2021, 26. [Google Scholar]
- Callaway, E. Delta Coronavirus Variant: Scientists Brace for Impact. Nature 2021, 595, 17–18. [Google Scholar] [CrossRef]
- World Health Organization. Thirteenth Meeting of the WHO Advisory Committee on Variola Virus Research (2011: Geneva, Switzerland). In WHO Advisory Committee on Variola Virus Research: Report of the Thirteenth Meeting; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- CDC COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/ (accessed on 11 November 2021).
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A Global Database of COVID-19 Vaccinations. Nat. Hum. Behav 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.; Eikenberry, S.E.; Gumel, A.B. Will Vaccine-Derived Protective Immunity Curtail COVID-19 Variants in the US? Infect. Dis. Model. 2021, 6, 1110–1134. [Google Scholar] [CrossRef]
- Gumel, A.B.; Iboi, E.A.; Ngonghala, C.N.; Ngwa, G.A. Toward Achieving a Vaccine-Derived Herd Immunity Threshold for COVID-19 in the U.S. Front. Public Health 2021, 9, 709369. [Google Scholar] [CrossRef]
- Pérez, Á.G.C.; Oluyori, D.A. An Extended SEIARD Model for COVID-19 Vaccination in Mexico: Analysis and Forecast. Math. Appl. Sci. Eng. 2021, 2, 219–309. [Google Scholar] [CrossRef]
- Magpantay, F.M.G. Vaccine Impact in Homogeneous and Age-Structured Models. J. Math. Biol. 2017, 75, 1591–1617. [Google Scholar] [CrossRef]
- Arora, P.; Sidarovich, A.; Krüger, N.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.-S.; Winkler, M.S.; Schulz, S.; Jäck, H.-M.; et al. B.1.617.2 Enters and Fuses Lung Cells with Increased Efficiency and Evades Antibodies Induced by Infection and Vaccination. Cell Rep. 2021, 37, 109825. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced Sensitivity of SARS-CoV-2 Variant Delta to Antibody Neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Haw, D.; Wang, H.; Eales, O.; Walters, C.; Ainslie, K.; Atchison, C.; Fronterre, C.; Diggle, P.; Page, A.; et al. REACT-1 Round 13 Final Report: Exponential Growth, High Prevalence of SARS-CoV-2 and Vaccine Effectiveness Associated with Delta Variant in England during May to July 2021. medRxiv 2021. [Google Scholar] [CrossRef]
- Halloran, M.E.; Haber, M.; Longini, I.M., Jr. Interpretation and Estimation of Vaccine Efficacy under Heterogeneity. Am. J. Epidemiol. 1992, 136, 328–343. [Google Scholar] [CrossRef]
- Wang, X. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2021, 384, 1577–1578. [Google Scholar] [PubMed]
- Allen, H.; Vusirikala, A.; Flannagan, J.; Twohig, K.A.; Zaidi, A.; Chudasama, D.; Lamagni, T.; COVID-19 Genomics UK (COG-UK Consortium). Household Transmission of COVID-19 Cases Associated with SARS-CoV-2 Delta Variant (B.1.617.2): National Case-Control Study. Lancet Reg. Health Eur. 2021, 12, 100252. [Google Scholar] [CrossRef]
- Caccavo, D. Chinese and Italian COVID-19 Outbreaks Can Be Correctly Described by a Modified SIRD Model. medRxiv 2020. [Google Scholar] [CrossRef]
- Avila-Ponce de León, U.; Pérez, Á.G.C.; Avila-Vales, E. An SEIARD Epidemic Model for COVID-19 in Mexico: Mathematical Analysis and State-Level Forecast. Chaos Solitons Fractals 2020, 140, 110165. [Google Scholar] [CrossRef]
- Rodrigues, H.S.; Monteiro, M.T.T.; Torres, D.F.M. Sensitivity Analysis in a Dengue Epidemiological Model. Conf. Pap. Math. 2013, 2013, 1–7. [Google Scholar] [CrossRef]
- Marino, S.; Hogue, I.B.; Ray, C.J.; Kirschner, D.E. A Methodology for Performing Global Uncertainty and Sensitivity Analysis in Systems Biology. J. Theor. Biol. 2008, 254, 178–196. [Google Scholar] [CrossRef]
- Amaral, F.; Casaca, W.; Oishi, C.M.; Cuminato, J.A. Simulating Immunization Campaigns and Vaccine Protection Against COVID-19 Pandemic in Brazil. IEEE Access 2021, 9, 126011–126022. [Google Scholar] [CrossRef]
- Matrajt, L.; Janes, H.; Schiffer, J.T.; Dimitrov, D. Quantifying the Impact of Lifting Community Nonpharmaceutical Interventions for COVID-19 During Vaccination Rollout in the United States. Open Forum. Infect. Dis. 2021, 8, ofab341. [Google Scholar] [CrossRef] [PubMed]
- Matrajt, L.; Eaton, J.; Leung, T.; Dimitrov, D.; Schiffer, J.T.; Swan, D.A.; Janes, H. Optimizing Vaccine Allocation for COVID-19 Vaccines Shows the Potential Role of Single-Dose Vaccination. Nat. Commun. 2021, 12, 3449. [Google Scholar] [CrossRef]
- Moline, H.L.; Whitaker, M.; Deng, L.; Rhodes, J.C.; Milucky, J.; Pham, H.; Patel, K.; Anglin, O.; Reingold, A.; Chai, S.J.; et al. Effectiveness of COVID-19 Vaccines in Preventing Hospitalization Among Adults Aged ≥65 Years—COVID-NET, 13 States, February-April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1088–1093. [Google Scholar] [CrossRef]
- Office of the Commissioner Comirnaty and Pfizer-BioNTech COVID-19 Vaccine. Available online: https://www.fda.gov/media/144413/download (accessed on 15 November 2021).
- Britton, T.; Ball, F.; Trapman, P. A Mathematical Model Reveals the Influence of Population Heterogeneity on Herd Immunity to SARS-CoV-2. Science 2020, 369, 846–849. [Google Scholar] [CrossRef]
- Saad-Roy, C.M.; Wagner, C.E.; Baker, R.E.; Morris, S.E.; Farrar, J.; Graham, A.L.; Levin, S.A.; Metcalf, C.J.E.; Grenfell, B.T. Immuno-Epidemiological Life-History and the Dynamics of SARS-CoV-2 over the next Five Years. medRxiv 2020. [Google Scholar] [CrossRef]
- El Guerche-Séblain, C.; Chakir, L.; Nageshwaran, G.; Harris, R.C.; Sevoz-Couche, C.; Vitoux, O.; Vanhems, P. Experience from Five Asia-Pacific Countries during the First Wave of the COVID-19 Pandemic: Mitigation Strategies and Epidemiology Outcomes. Travel Med. Infect. Dis. 2021, 44, 102171. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.G.; Wilson, N.; Anglemyer, A. Successful Elimination of COVID-19 Transmission in New Zealand. N. Engl. J. Med. 2020, 383, e56. [Google Scholar] [CrossRef]
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and Non-Pharmaceutical Interventions for COVID-19: A Mathematical Modelling Study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Giordano, G.; Colaneri, M.; Di Filippo, A.; Blanchini, F.; Bolzern, P.; De Nicolao, G.; Sacchi, P.; Colaneri, P.; Bruno, R. Modeling Vaccination Rollouts, SARS-CoV-2 Variants and the Requirement for Non-Pharmaceutical Interventions in Italy. Nat. Med. 2021, 27, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Viana, J.; van Dorp, C.H.; Nunes, A.; Gomes, M.C.; van Boven, M.; Kretzschmar, M.E.; Veldhoen, M.; Rozhnova, G. Controlling the Pandemic during the SARS-CoV-2 Vaccination Rollout. Nat. Commun. 2021, 12, 3674. [Google Scholar] [CrossRef]
- Chen, J.; Vullikanti, A.; Santos, J.; Venkatramanan, S.; Hoops, S.; Mortveit, H.; Lewis, B.; You, W.; Eubank, S.; Marathe, M.; et al. Epidemiological and Economic Impact of COVID-19 in the US. Sci. Rep. 2021, 11, 20451. [Google Scholar] [CrossRef]
- Radfar, A.; Ferreira, M.M.; Sosa, J.P.; Filip, I. Emergent Crisis of COVID-19 Pandemic: Mental Health Challenges and Opportunities. Front. Psychiatry 2021, 12, 631008. [Google Scholar] [CrossRef]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.S.; Andreae, M.O.; Pöschl, U.; Su, H. Face Masks Effectively Limit the Probability of SARS-CoV-2 Transmission. Science 2021, 372, 1439–1443. [Google Scholar] [CrossRef]
- Head, J.R.; Andrejko, K.L.; Remais, J.V. Model-Based Assessment of SARS-CoV-2 Delta Variant Transmission Dynamics within Partially Vaccinated K-12 School Populations. medRxiv 2021. [Google Scholar] [CrossRef]
- Kharazian, N.A.; G Magpantay, F.M. The Honeymoon Period after Mass Vaccination. Math. Biosci. Eng. 2020, 18, 354–372. [Google Scholar] [CrossRef]
- Swan, D.A.; Goyal, A.; Bracis, C.; Moore, M.; Krantz, E.; Brown, E.; Cardozo-Ojeda, F.; Reeves, D.B.; Gao, F.; Gilbert, P.B.; et al. Mathematical Modeling of Vaccines That Prevent SARS-CoV-2 Transmission. Viruses 2021, 13, 1921. [Google Scholar] [CrossRef] [PubMed]
- Marquioni, V.M.; de Aguiar, M.A.M. Modeling Neutral Viral Mutations in the Spread of SARS-CoV-2 Epidemics. PLoS ONE 2021, 16, e0255438. [Google Scholar] [CrossRef]
- Tada, T.; Zhou, H.; Dcosta, B.M.; Samanovic, M.I.; Mulligan, M.J.; Landau, N.R. SARS-CoV-2 Lambda Variant Remains Susceptible to Neutralization by mRNA Vaccine-Elicited Antibodies and Convalescent Serum. bioRxiv 2021. [Google Scholar] [CrossRef]
- Kimura, I.; Kosugi, Y.; Wu, J.; Yamasoba, D.; Butlertanaka, E.P.; Tanaka, Y.L.; Liu, Y.; Shirakawa, K.; Kazuma, Y.; Nomura, R.; et al. SARS-CoV-2 Lambda Variant Exhibits Higher Infectivity and Immune Resistance. bioRxiv 2021. [Google Scholar] [CrossRef]
- McCallum, M.; Bassi, J.; De Marco, A.; Chen, A.; Walls, A.C.; Di Iulio, J.; Tortorici, M.A.; Navarro, M.-J.; Silacci-Fregni, C.; Saliba, C.; et al. SARS-CoV-2 Immune Evasion by the B.1.427/B.1.429 Variant of Concern. Science 2021, 373, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Arora, P.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Sidarovich, A.; Winkler, M.S.; Schulz, S.; Jäck, H.-M.; Stankov, M.V.; Behrens, G.M.N.; et al. Delta Variant (B.1.617.2) Sublineages Do Not Show Increased Neutralization Resistance. Cell. Mol. Immunol. 2021, 18, 2557–2559. [Google Scholar] [CrossRef] [PubMed]
- Grubaugh, N.D.; Hodcroft, E.B.; Fauver, J.R.; Phelan, A.L.; Cevik, M. Public Health Actions to Control New SARS-CoV-2 Variants. Cell 2021, 184, 1127–1132. [Google Scholar] [CrossRef]
- Muller, C.P. Do Asymptomatic Carriers of SARS-COV-2 Transmit the Virus? Lancet Reg. Health Eur. 2021, 4, 100082. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, P.; Zimmer, J.; Schulz, J.; Glod, F.; Veiber, L.; Mombaerts, L.; Rodrigues, B.; Aalto, A.; Pastore, J.; Snoeck, C.J.; et al. SARS-CoV-2 Transmission Risk from Asymptomatic Carriers: Results from a Mass Screening Programme in Luxembourg. Lancet Reg. Health Eur. 2021, 4, 100056. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avila-Ponce de León, U.; Avila-Vales, E.; Huang, K.-l. Modeling the Transmission of the SARS-CoV-2 Delta Variant in a Partially Vaccinated Population. Viruses 2022, 14, 158. https://doi.org/10.3390/v14010158
Avila-Ponce de León U, Avila-Vales E, Huang K-l. Modeling the Transmission of the SARS-CoV-2 Delta Variant in a Partially Vaccinated Population. Viruses. 2022; 14(1):158. https://doi.org/10.3390/v14010158
Chicago/Turabian StyleAvila-Ponce de León, Ugo, Eric Avila-Vales, and Kuan-lin Huang. 2022. "Modeling the Transmission of the SARS-CoV-2 Delta Variant in a Partially Vaccinated Population" Viruses 14, no. 1: 158. https://doi.org/10.3390/v14010158